
Abstract
Untethered mobile microrobots have the potential to transform medicine radically. Their small size and wireless mobility can enable access to and navigation in confined, small, hard-to-reach, and sensitive inner body sites, where they can provide new ways of minimally invasive interventions and targeted diagnosis and therapy down to the cellular length scales with high precision and repeatability. The exponential recent progress of the field at the preclinical level raises anticipations for their near-future clinical prospects. To pave the way for this transformation to happen, however, the formerly proposed microrobotic system designs need a comprehensive review by including essential aspects that a microrobot needs to function properly and safely in given in vivo conditions of a targeted medical problem. The present review provides a translational perspective on medical microrobotics research with an application-oriented, integrative design approach. The blueprint of a medical microrobot needs to take account of microrobot shape, material composition, manufacturing technique, permeation of biological barriers, deployment strategy, actuation and control methods, medical imaging modality, and the execution of the prescribed medical tasks altogether at the same time. The incorporation of functional information pertaining each such element to the physical design of the microrobot is highly dependent on the specific clinical application scenario. We discuss the complexity of the challenges ahead and the potential directions to overcome them. We also throw light on the potential regulatory aspects of medical microrobots toward their bench-to-bedside translation. Such a multifaceted undertaking entails multidisciplinary involvement of engineers, materials scientists, biologists and medical doctors, and bringing their focus on specific medical problems where microrobots could make a disruptive or radical impact.
Export citation and abstract BibTeX RIS

Original content from this work may be used under the terms of the Creative Commons Attribution 3.0 licence. Any further distribution of this work must maintain attribution to the author(s) and the title of the work, journal citation and DOI.
Introduction
The past decades have witnessed an eruption in the development of robotic systems for healthcare. Devices and platforms for robotic surgery [1], compliant soft robots for wearable and assistive devices [2, 3], and pill-size capsule endoscopes for gastrointestinal delivery [4] are among the notable examples that underpin a progressive trend toward minimally invasive, patient-centered, precise, and personalized medical solutions. In the same strain, untethered mobile microrobots smaller than 1 mm can substantially advance the scope of minimally invasive medical procedures and targeted therapies [5–10]. They can do so by navigating in confined, small, hard-to-reach, and sensitive inner body sites to perform local and targeted diagnostic and therapeutic medical operations with high precision and repeatability.
*What is a microrobot?
A mobile microrobot is a sub-millimeter scale untethered, or cordless, machine with partly or fully self-contained capabilities for locomotion, sensing, and functional operations [10]. Due to its small size, locomotion mechanics and physical interactions of a mobile microrobot are dominated by surface area-related forces, and the contribution of volumetric (e.g. inertial) forces are usually negligibly small. Fluid flows around a moving microrobot are mostly steady and laminar, which is described by the Stokes flow where Reynolds number, the ratio of the inertial to viscous forces, is much smaller than 1. Microrobots may contain functional components, such as microactuators, microsensors, and reservoirs for diagnostic and therapeutic agents to carry out specific functions for a given medical task, such as microsurgery, cargo transport, and local heating. To power such functions, microrobots may harness the chemical energy in its microenvironment or use wireless power delivery routes, such as external magnetic or acoustic fields. Real-time feedback and control mechanisms regulating the interactions among functional components and between the microrobot and the outer environment are central to achieve safe, robust, and precise medical functions. At comparable length scales, the innate functioning of cells, such as bacteria, algae, neutrophils, trypanosomes, or multicellular microorganisms, such as, volvox colonies and yeasts can provide a rich source of inspiration to create similarly performing robust synthetic robot designs. Alternatively, microorganisms themselves can provide the locomotion, sensing, and control behaviors in a biohybrid microrobot design. The interested readers are directed to read further text dedicated to the design principles of microrobots [5–13]. To avoid confusion and concentrate primarily on the translational prospects, the present review considers all sub-millimeter scale untethered robot designs cited herein a microrobot.
Medical microrobotics research initially concentrated on the principles of microscopic locomotion methods and their dynamic interactions with their surrounding fluids and surfaces [11]. Recent advances in design, fabrication, actuation, and control methods of microrobots have played a pivotal role in achieving many locomotion modes. Swimming has been the most commonly studied locomotion mode, where a plenty of self-propelled [12–18] or remotely actuated [19–25] microswimmers and micromotors [26] have been reported with in vitro [14, 16–18, 20, 22, 24], ex vivo [23], and in vivo [15, 19, 21] experimental results towards medical applications. Incorporation of functional capabilities using biocompatible and responsive materials to these microswimmers paved the way for unveiling their biomedical potential [7]. Despite a number of proof-of-concept studies to this end, however, a promising microrobot* with minimally required capabilities targeting a well-defined medical problem has not been available yet. This is because the formerly proposed microrobot designs lack a comprehensive design approach that can realistically address the requirements of their targeted clinical applications. The design of a medical microrobot should consider the entire clinical scenario from the point of entry to the mechanisms of safe and functional operation and to the disposal after the operation is complete, and all aspects must be encoded in the physical design of the microrobot simultaneously.
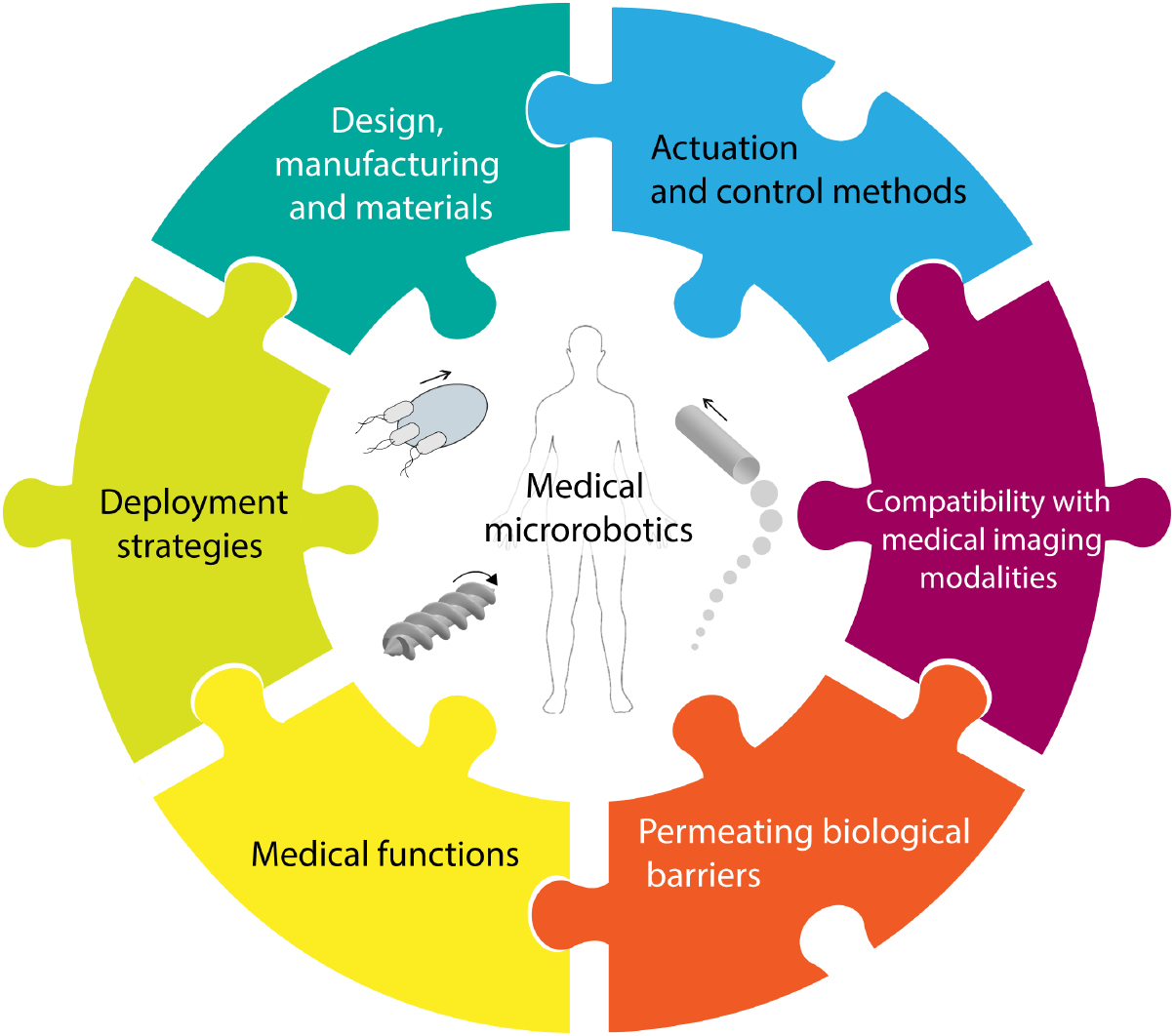
This review aims to stimulate discussions by providing a translational perspective on the medical microrobotics research. We suggest that the design of a medical microrobotic system should assume an application-specific, integrated approach, where microrobot's 3D body shape, material composition, manufacturing technique, permeation of biological barriers, deployment strategy, actuation and control methods, medical imaging modality, and the execution of the prescribed medical tasks are considered altogether (figure 1). Each of the essential aspects conceptualized in figure 1 contains particular information and a special design consideration, which must be incorporated into the physical design of the microrobot. The interpretation of this is growing complexity and a large network of coupled interactions among physical parameters. This is a nontrivial task to accomplish. Here we use the lessons that we have learned from the existing in vitro and in vivo studies and discuss the potential pitfalls of microrobots to design more complete systems towards their successful clinical translation. Nevertheless, lessons learned in one context do not always translate into others. Because the physical design of a microrobot is more sophisticated than those of passive particles, the proof-of-concept developments in one type of design is usually not suitable for integration with another so as to impart the microrobot with multiple capabilities. The modular design approach does not seem to work efficiently for microrobotics. There are various reasons behind this, mostly created by the lack of suitable materials and inflexible manufacturing techniques to accommodate adequate sophistication in the physical design of a microrobot. The variations and complexity of biological environments in health and disease states also put high demands on the expected performance of the microrobot. These conditions are rarely captured in the existing in vitro and ex vivo testbeds, and the disease model animals have not been systematically used with microrobots so far.

Figure 1. Essentials of a microrobot to function in vivo. Design of an untethered microscopic mobile machine with medical interventional capabilities should assume an integrated approach where design 3D body shape, material composition, manufacturing technique, deployment strategy, actuation and control methods, imaging modality, permeation of biological barriers, and the execution of the prescribed medical tasks need to be considered altogether. Each of these essential aspects contains a special design consideration, which must be reflected at the physical design of the microrobot. The growing complexity and a big network of interactions among physical parameters necessitate an application-oriented design; the entire clinical scenario from the way of administration to the mechanism of action and to the disposal must be well-known and well-organized.
Download figure:
Standard image High-resolution imageGiven the multidimensional complexity of challenges ahead, this review may not be able to impart a perfect ability to predict what could work. Researchers should nonetheless adapt a more integrative approach and foster it to the greatest extent possible. Strategies that will ensure coupling of essential aspects will create higher impact than the limited scopes of individual proof-of-concept studies. This thinking should also grow with more realistic preclinical tests by considering regulatory aspects to qualify the bench-to-bedside translation of microrobots. This new understanding requires fostering collaborative research with the involvement of engineers, materials scientists, biologists, and healthcare providers, and bringing their focus on well-defined medical problems where microrobots can make a transformative high impact.
Medical functions of a microrobot
A medical microrobot should bear one of the following qualities to create a transforming impact in medicine: (1) improving the diagnostic or therapeutic capabilities of the current state-of-the-art, (2) offering a safer, less invasive, or implantable alternative in particular for patients with special conditions, or (3) enabling previously unthinkable or impossible new diagnostic or therapeutic capabilities. The first step in the design of a microrobotic system is to define the specific medical problem. Each medical scenario has its unique conditions: the type of the tissue the microrobot will interact with and its sensitivity, the type of pathology and its severity, the size of the target area, how to reach there and obtain imaging feedback during the operation, the properties of the body fluid (e.g. non-Newtonian fluid property, fluid heterogeneity) to operate in, the presence of a fluidic flow or other body motions (e.g. breathing, peristalsis, arterial pulsation) in that environment, the immunogenic activity and other potential biological barriers, etc. Once the full picture of the medical problem and its constituents are captured, the physical design should follow. Depending on the medical scenario, microrobots may have components designed to move and function autonomously in response to the pathological signals in their environment or to be teleoperated by a healthcare provider directly using external stimuli or forces. These robots may operate as a single entity, teams [23, 27–29], or swarms [23, 30], performing parallel and distributed tasks. The medical operation of a microrobot should also include a contingency plan in case the pathological conditions evolve and microrobots fail to respond in time. As the level of autonomy and competence of microrobots increases, the role and responsibility given to the microrobots may overlap with the healthcare providers, which could trigger new ethical questions. A master switch or fail-safe strategies may be needed that would contain the situation in case the execution of the given medical task fails or adverse effects are observed.
This section aims to recapitulate potential diagnostic and therapeutic capabilities that can be imparted to a microrobot. We put a particular emphasis on the design pillars of a microrobotic system that will operate in the body in the following sections.
Targeted cargo delivery
Targeted cargo delivery is one of the most important medical applications where microrobots could revolutionize the gold standards of medical procedures [31]. Active navigation of highly concentrated diagnostic and therapeutic agents to the site of action can surpass the limited delivery and distribution efficiencies offered by the systemic routes and local diffusion [23]. Thus, it would be possible to minimize the effects of systemic toxicity and increase the overall efficacy of single-dose administration [32]. A microrobot should possess the following capabilities to be effective and safe in targeted cargo delivery strategies: (1) Positional control: The microrobot should be able to actively carry and steer concentrated cargo, e.g. drugs [22, 24, 33], imaging contrast agents [24], siRNA [34], cells [35, 36], vaccine [37], etc, and (2) minimize the off-target distribution by keeping the cargo during its voyage until reaching the target site; (3) Temporal control: The therapeutic release should be programmable and triggered via environmental [24] or externally controlled [22] stimuli so that the microrobot can provide a fine-tuned and sustained therapeutic window. Based on these requirements, actuation and control strategies, microrobot's material composition, cargo release strategy, and biodegradability become key concepts in a delivery microrobot. The right body shape and porosity in the material can achieve concentrated cargo loading. Porous hydrogel networks in a microrobot can very effectively sequester high amounts of diagnostic and therapeutic cargos [24]. After accomplishment of the task, the microrobot should degrade fully in a reasonable time frame in the given physiological microenvironment to prevent foreign body reaction [21, 24]. Autonomous release of diagnostic and therapeutic cargo types with programmable kinetics based on the environmental sensing of local cues, e.g. disease markers, can enable microrobotic diagnosis and therapy in the form of an orderly executed and programmable operation [24]. Alternatively, microrobots might be externally triggered using light to release cargo in controlled temporal patterns [22].
Microrobot-aided physical surgery
Endoscopy or robot-assisted surgery have markedly reduced centi/decimeter-size incisions to millimeter-size key holes, lowered post-operative patient morbidity, shortened recovery times, and decreased downsides caused by radical surgeries [1]. Remote microscopic manipulation will likely to expand the concept of minimally invasive surgery to very small, localized, and controlled physical damage as a curative treatment model [38]. Microrobots can drill through a blood clot in the circulatory system or can open up obstructions in the ductal and urinary systems with the aim of restoring the normal flow conditions [39–41]. Beyond luminal manipulations, sub-millimeter fenestrations or incisions can be carried out by functionalized robots. Fine mechanical resection of malignant tumors in sensitive places, such as the central nervous system (CNS), can have a high medical impact. In the process of hard drilling, a soft carrier compartment of the microrobots could locally release degrading enzymes or medications to eliminate the debris left behind. Microrobots could also serve as semi- or permanent implants in the luminal organs or in obstructive surgeries to keep the lumens open. In some obstructions, the microrobots may be needed to keep dormant in the body until they are needed in a local revision surgery. Remote control and steering could drastically help in the design and placement of new types of reconfigurable stents in the luminal organs and in the circulatory system. In such long-term applications, the durability and biocompatibility of microrobots should be carefully assessed. For such physical surgery operations to be accomplished in tissues, highly precise force and position control strategies and spatial navigation with high dexterity are essential. Besides, remote actuation systems should enable enough penetration force to execute the function, and be cost-effective for hospitals ideally to gain widespread clinical adoption. Towards drilling-based medical microrobot operations, model wireless corkscrew structures [42–44], magnetic hammers [45], and microscopic sharp tipped needles [46] have been proposed. A main challenge in the development of microscopic drillers is the wireless delivery of adequate power as the driller size gets smaller. New material compositions and manufacturing techniques are necessary to further miniaturize the microrobots for microrobot-assisted surgery and to ensure their safety. Because these microrobots will likely be made from hard non-biodegradable materials, their retrieval following the operation needs a viable solution. Moreover, such physical surgeries should be incorporated with delivering specific cargos, such as chemical drugs or immunotherapy agents, by the given microrobot design to make sure that any possibly remaining disease source after the surgery would be fully removed by such cargo release function.
Remote tissue heating
Clinical hyperthermia is a therapeutic method used particularly for cancer [47–49]. Microrobots may be able to produce directed local heat under radio waves of high frequency, magnetic fields, and high intensity focused ultrasound to destroy cancer cells in small and hard-to-reach cancerous lesions where resection is deemed dangerous [50–53]. In such a treatment, the microrobot should be able to generate hyperthermia in the selective therapeutic window typically between 40 °C–44 °C, where the exact values depend on the physiological characteristics, such as local perfusion variations [54]. The microrobot may need to contain a sensory feedback mechanism to monitor the temperature rise in the surrounding healthy tissues and influence the decision to continue to the heating cycle in an optimized and feedback-controlled pattern. Advantages of the hyperthermia are not limited with direct cell and tissue destruction; it may also enhance the sensitivity of cancer cells to chemotherapy, radiotherapy, and immunotherapy [47, 51, 55]. Remote heating could be also used for blood coagulation to stop bleeding in tiny and sensitive parts in the human body. Typically, local temperature values around 42 °C for brief periods can be sufficient to stop the bleeding through coagulation. Higher local temperatures around 60 °C–90 °C can be used for thermal ablation and above 200 °C for local micro/milliscale cauterization [56].
Micro-biopsy
Conducting a biopsy is a gold standard for the diagnosis of many diseases, provides valuable information of the pathology at the time of intervention and guides for preparing an effective therapy method. A microscopic biopsy robot would have the potential to decrease the discomfort of the patient during the procedure and hence would broaden its utilization as a monitoring tool to assess the prognosis of the disease. Wireless prototypes of shape memory alloys [57], chemically responsive grippers [58], and thermo-responsive grippers [29, 59] have been proposed to mimic the incisional biopsy ex vivo. To collect the biopsy sample with microrobots, a robust control over the collection of the specimen is a must. The microrobots should be able to produce high forces to detach cell samples from the suspected tissue lesion. Specimen taken via a microrobot must also be representative enough for pathologic investigation and diagnosis, so these systems must be able to retrieve or encapsulate at least biomarkers or a population of cells. To this end, biopsy sizes should range from around 10 micron to 1 mm [60]. Their deployment and retrieval strategies must be well-defined. Following the collection of the specimen, robots must follow the shortest possible path to bring the specimen back with no contamination for evaluation ex vivo, or be equipped with remote sensing for carrying out in vivo diagnostic or prognostic tests [5]. Biopsy microrobots should preserve the integrity of the specimen and not lose it during the retrieval. Reducing the representative specimen size and shortening the retrieval path or in situ evaluation methods can significantly minimize the risk of spreading of cancer cells.
Remote sensing and healthcare monitoring
A microrobot functioning as an implantable mobile sensor may trace desired biochemical markers and transmit this spatiotemporal information to the outside world wirelessly. This information can be evaluated using medical imaging tools or in the form of biochemical signals as byproducts produced by microrobots [61]. This can enable continuous monitoring of health and early awareness in case of an emerging disease [62]. Shape-changing polymers, nanoparticles, and featured surfaces have been shown as implantable biosensor candidates responding to endogenous signals [63, 64]. For example, durability for long period of time and close proximity to the target tissues facilitate in vivo nucleic acid detection instead of time-consuming conventional methods [65].
Medical models and testbeds for microrobots
For gaining mechanistic insight into the behaviors of microrobots in complex physiological and pathological environments, biomimetic in vitro disease models [66], tissue and organ phantoms [67, 68], freshly acquired ex vivo tissues and organs, and live animal models are needed. For cargo delivery and controlled release applications, existing tissue engineered disease models could be adapted for proof-of-concept investigations [69]. Hydrogels of biomaterials with tailorable mechanical properties can be used as in vitro testbeds to optimize microrobot-aided operation. Successful prototypes can be tested in live tissues and organs of small animals to show the preclinical feasibility of the proposed new concepts before going forward with large animals. Such in vivo testbeds are also essential to understand and control bleeding tendencies of the tissues during a microrobotic medical operation. Highly vascularized liver, lungs, and spleen might serve as promising candidates to this purpose. Disease states can put high demands on the expected performance of microrobots, which is not easy to recapitulate in the available in vitro and ex vivo testbeds. Animal disease models have not been used with microrobots so far. Tests inside an animal disease model will also be beneficial for additional microrobotic tasks, such as feedback from the microenvironment and communication with the operator. Such tests, however, should always be conducted with extreme care to minimize the use of animals. To this end, the development of new types of high quality realistic tissue and organ phantoms could help tremendously [70].
Biological barriers against the functioning of microrobots
The in vivo journey of a microrobot from the point of deployment to the target site of action is full of perils. A microrobot needs to overcome biological barriers to reach the target site. The complexity of the biological barriers and the potential mechanisms to overcome them depend in large on the site of administration, the associated target tissue, and the desired function. When a microrobot is inside the body, a myriad of proteins will interact with its surface that will spontaneously form an adsorption layer around, called protein corona (figure 2(A)) [71, 72]. This is a thermodynamic process; upon protein binding, which is energetically favored, enthalpy is reduced and the hydration layer around the nanoparticles is displaced, which increases entropy [73]. More than a decade of research with nanoparticles and solid surfaces showed that the formation of protein corona depends on the physical design factors, such as the surface chemistry, charge, water retention capacity, surface topography at the nanoscale, exposure time, and hydrophobicity of the structures (table 1) [71, 74]. The identity of this dynamic thin layer might redefine some of the surface-governed behaviors of microrobots. First, the surface polarity of the microrobot may be altered, which could influence the swimming speed [75]. Second, the corona formation may trigger the biophysical process of protein misfolding and aggregation, which may elicit an immune response to eliminate the microrobots from the body. Third, the surface may hinder the chemical or biological functionalities imparted to the microrobot in its physical design, e.g. kinetics of the drug release and recognition (sensing) signals from the environment. Because microrobots are actively moving entities, their protein corona from one body fluid to another may be preserved [76]. This suggests that the route of entrance of microrobots can strongly influence the composition of the protein corona, and hence the functional behavior, in the downstream. Shear stress exerted on the microrobots, as a result of their active mobility or when they are in the circulatory system, may also have a significant impact on the protein corona formation. Shear stress can give rise to catch-and-slip bonds associated with the blood cell margination and their extravasation from the blood vessels [77]. An immediate conclusion from these physical phenomena is that in vitro and in vivo protein coronas could be different in the protein composition, surface coverage, protein abundance, and the dynamicity of the corona for the microrobots [76, 77].

Figure 2. Potential biological barriers for operation and functioning of a microrobot. (A) Protein corona formation on the surface of microrobots and attachment of opsonin proteins may result in subsequent (B) immune clearance by phagocytes, which may contribute to sub-optimal delivery and loss-of-function. (C) Hemorheological and blood flow limits the control of microrobots. Red blood cells alter rheological behavior of blood, and blood exhibits shear-thinning properties where viscosity decreases with the increasing shear rate. (D) Cellular barriers, such as endothelial lining in the lumen of vessels and (E) blood-brain barrier, (F) fibrous ECM of the tissues and high interstitial pressure in tumor sites and the (G) barrier of mucosal epithelial cells are other compelling barriers to microrobot extravasation into tissues. (H) Vitreous humor may also form a hurdle while targeting the eye for ocular application. Reproduced from [23]. CC BY 4.0.
Download figure:
Standard image High-resolution imageTable 1. Surface properties of microrobots and anti-adsorption factors that collectively influence the corona formation.
| Surface properties | Anti-adsorption factors |
|---|---|
| Free energy | Hydration, strong water binding |
| Charge, ion binding | Low protein flexibility |
| Hydrogen bonding capacity | High protein mobility |
| Surface water structure | Low net Coulomb interaction |
| Nano topography | High surface smoothness |
| Oxide layer | |
| Surface impurities |
When a microrobot is in the blood stream, important immunological constituents of the protein corona are the components of the complement system, which is a part of the innate immune system, the first line of defense against intruders [78]. Opsonin proteins present in the blood plasma might activate the complement system on the microrobot surface, which might result in a process called opsonization. Opsonization can enhance the ability of leukocytes to recognize microrobots, and thereby presenting one of the most important biological barriers to microrobots in the circulatory system (figure 2(B)). Once activated, the opsonization can further evolve to trigger the activation of mast cells and other immune cells to induce proinflammatory reactions. Such reaction cascade might significantly limit the ability of the microrobots to reach the desired destination and perform the medical tasks. To address these limitations, engineering the microrobot surfaces with neutrally charged and long hydrophilic polymers, such as the derivatives of the poly(ethylene glycol) (PEG) have significantly helped in nanoparticles [78]. PEG chains typically provide a protective hydrophilic layer around the nanoparticles that is able to repel the absorption of opsonin proteins via steric repulsion forces, which blocks and delays the first step of the opsonization process [78, 79]. It is important to note, however, PEG-conjugated therapeutics might also be eliciting an immune response in some patients [80].
The extent and strength of the immune system are not the same everywhere in the body. Certain sites of the human body have immune privilege, meaning they are able to actively keep an attenuated profile of immune reactions to avoid destructive inflammation. The introduction of foreign antigens is therefore accepted without eliciting an inflammatory immune response for long durations. The CNS, the eye, and the feto-maternal system are well-known immune-privileged sites [81–83]. Microrobotic operations in these sites might provide a degree of flexibility in the material and architectural design of the microrobot based on the clinical scenario or the testing of the microrobot, i.e. the tissue, the course of pathology, and the duration of exposure of the microrobots. Nevertheless, to alleviate the potential dangers of the uncontrolled immune response, an ultimate approach might be relying on the patient's own biomaterials to fabricate the microrobots. Such a personalized solution might significantly silence the immune response, as the body would recognize the microrobots as self. To this end, for instance, turning natural red blood cells (mean diameter of 7.8 µm and thickness of 1–2.5 µm) or platelets into functional microrobots might be a promising route [84–86]. These cells are available in the blood in high throughput: around 4.5–5.5 × 109 red blood cells ml−1 blood and around 1.5–3.0 × 108 platelets ml−1 blood [87]. Use of red blood cells as the base material could be interesting and useful to enable massive amounts of microrobots that could be hardly achieved by any of the existing microfabrication technologies. Moreover, the red blood cells can be deformed under applied stress without undergoing plastic deformation [18].
By virtue of its circulation throughout the body, it is possible to reach deep body sites by means of the vasculature. However, apart from opsonization and immune clearance, there are also other barriers acting on intravenously administered microrobots in the blood stream. These are mainly stemming from the anatomy of the vasculature and the fluidic properties of the blood. Propulsion and steering in the circulatory system put a major fluidic flow barrier against robust operations of microrobots. This circulatory loop consists of arteries, carrying blood from the heart, and veins specialized to carry blood collected from the tissues to the heart. The pulsatile blood flow in the arteries ranges from 100 to 400 mm s−1. Arteries branch into smaller arterioles, which further branch into capillaries for nutrient and gas exchange. Capillaries then come together to form venules, which connect to veins for returning blood to the heart. Despite the flow velocity becomes smaller with the branching, the slowest flow rate in the capillaries is still around 100 µm s−1 [88]. All these different forms of vessels vary in dimensions, hemorheological flow properties, and shear stress. Smallest capillaries can go down to several micrometers in diameters, which put a bottom size limit for the microrobots that are designed to navigate in the full loop of the vasculature. Hence, a rigid microrobot larger than 5 µm in diameter would fail to safely navigate through the smallest capillaries; microrobots with larger diameter can pass through these smallest capillaries if they are soft bodied and highly deformable, similar to red blood cells. Accumulation of such robots by accident in the arteries going to the brain or lung capillaries, may cause a stroke or pulmonary embolism, respectively. The most of the achievable velocities with microrobots are typically few to several orders magnitude slower than that of the blood flowing in the vessels. However, despite the high flow rates, operation in arteries is still conceivable by complementary technologies. As such, use of balloon catheter to control and reduce the flow velocity has been shown to enable microrobotic navigation by a clinical magnetic resonance imaging (MRI) system in swine carotid artery [89].
Another way of overcoming the intravascular flow barrier might be using the blood flow as the highway to reach the destination. For example, in order to increase the therapeutic efficacy of tissue plasminogen activator (t-PA), magnetic nanomotors were driven to the blood clot with the flow and when localized, the magnetic field was used to rotate the nanomotors. Rotating nanomotors enhanced the local mixing and interaction of co-administered t-PA with the blood clot and accelerated the thrombolysis in a mouse model [90]. A similar approach targeted blood clots in the middle cerebral artery with magnetic microrods carrying t-PA. Microrods were directed to the lesion by both the blood flow and the magnetic guidance and enhanced the disruption of the blood clot [91]. Despite the proof of the concept, there are unresolved challenges before going forward with a large animal or clinical study. First, aggregation of the nanoparticles under the magnetic field could be dangerous, particularly when they accumulate in an undesired vessel. A nanoparticle-free robotics approach used a smart DNA origami design and incorporated a DNA aptamer for targeted nucleolin protein, which is overexpressed in tumor-supplying blood vessels. With the help of the blood flow and targeting moiety, thrombin is delivered to the tumor-associated blood vessels for the intravascular thrombosis and the inhibition of tumor growth [92]. On the other side, CaCO3 based micromotors were propelled against the blood flow in both vertical and horizontal orientations of glass capillaries through a combination of lateral propulsion, buoyant rise, and convection. The construct was then shown to effectively deliver coagulation agents for the treatment of hemorrhage in an amputated mouse model [93]. Findings from these studies provide evidence that, despite the challenges, therapeutic outcome for intravascular applications can be achieved by proper use of microrobots. In addition, biohybrid strategies including the use of the body's own cells as cellular cyborgs could circumvent the intravascular motion challenge due to the inherent capability of leukocytes to navigate in the bloodstream [94]. While blood flow carries cells passively, upon encountering chemical signals from endothelium and sensing an increased level of cytokines, cells display active rolling-tumbling motion on endothelial surfaces for tissue extravasation [95]. Implementation of such chemical sensing-based activation of robotic mobility and function in synthetic designs would significantly enable autonomous smart behavior for microrobots in the future. If a microrobot reaches its destination at an organ and wants to leave the vasculature, the only reasonable place would be the capillaries. The wall thicknesses of arteries and veins hinder the microrobots to penetrate into the tissue at those sides. A breach in these vessels may also result in uncontrolled internal bleeding.
Another obstacle against the applied microrobots in the vasculature is the dynamic rheological behavior of the blood depending on the vessel diameter, flow rate, and hematocrit value (figure 2(C)). The latter parameter is the ratio of the volume of the red blood cells to the total volume of blood, which is the main determinant of the blood viscosity. At high shear rates, red blood cells deform and align their major axis with the flow direction, which reduces the viscosity and makes blood as a shear-thinning fluid together with the effects of plasma viscosity and temperature. This non-Newtonian behavior of blood is another barrier that alters the mechanics of swimming [96]. Hence, an adaptation of microrobots to the changing flow parameters and the viscosity properties is required to ensure the designed and predicted mobility.
Majority of the microrobot studies have shown propulsion in Newtonian or low-viscosity fluids, such as water, buffer solutions, and serum, lacking the possible interactions with blood cells [97–99]. Recapitulation of pulsatile flow conditions, the pressure gradients, and the composition of the blood in phantoms and microfluidic channels are necessary to understand the dynamics and behavior of microrobots in complex viscous environments. In this regard, magnetic helical-shaped micromotors have been successfully actuated in undiluted human blood and shown to undergo a stick-and-slip motion while going through the blood cells [100].
For the extravascular deliveries and functions, crossing endothelial barrier may be required for precise accumulation at the desired site (figure 2(D)). The size effect is more pronounced in the application of microrobots, particularly for those cellular barriers. One of the most tightly regulated cellular barrier is the blood-brain barrier (BBB) and the opening of tight junctions in continuous capillaries is less than 1 nm in the brain, which severely impedes the transvascular penetration of microrobots (figure 2(E)) [101]. So far, myriad of invasive and non-invasive strategies, which breakdown the integrity of BBB, have been applied to bypass BBB for therapeutic delivery to the CNS [102]. One such strategy that can be co-opted with microrobots is an introduction of focused ultrasound systems (FUS) to transiently widen tight junctions. Although FUS-induced pores are only in the nanometer size range, which is beyond the penetration capability of existing microrobots, they can be further enlarged via microrobots by inducing mechanical force similar to the leukocyte extravasation strategy. However, BBB disruption can induce neuropathological alterations in the brain as well as leakage of plasma proteins, such as albumin, which is toxic to astrocytes [103]. Therefore, harnessing the existing tools in nature and following the footsteps of BBB penetrating pathogens, such as some meningitis bacteria, might provide an alternative transcellular route to cross the BBB. To do so, active control of microrobots within cytoplasm is necessary, which have been shown to be doable. Recently, maneuverability and manipulation of helical nanorobots inside cells with no adverse effect on cellular behavior have been demonstrated [104]. Another gateway to the brain is through the cerebrospinal canal, which also bears certain biological limitations against introduced microrobots (figure 3). Targeting brain in a non-invasive way is nontrivial and all the potential mechanisms to achieve it should be in depth reviewed elsewhere as it cannot be contained easily in one section.

Figure 3. Microrobot's deployment strategy determines the biological barriers on the way the target site. In a realistic clinical scenario, a microrobot will encounter several tissue barriers to pass. Each barrier will have unique biological conditions for which the microrobots should be equipped with functional components.
Download figure:
Standard image High-resolution imageThe structure and size barrier properties of capillaries vary among tissues. On the contrary to continuous capillaries found in the brain, potential easy-to-cross candidates for microrobots are fenestrated capillaries and sinusoid endothelium by virtue of having less tight junctions and intracellular clefts. Sinusoids, found in liver, spleen, bone marrow, and adrenal gland range in size from 30 µm to 40 µm in diameter and contain pores measure in size up to several micrometers. These pores and discontinuities between endothelial cells and the basement membrane allow paracellular passage of large molecules and even cells [105]. A microrobot in the size of a single cell can also penetrate through such clefts for extravascular applications while targeting abovementioned organs.
In other organs, which lack sinusoid or fenestrated capillaries, crossing endothelial barrier requires similar strategies, as in the case of BBB. On the other hand, in some pathological conditions, such as injury, inflammation, and cancer, endothelial dysfunction creates vessel fenestrations. Although the degree of fenestrations depends on the severity of the pathological condition and the tissue type, it may open up a penetration space for microrobots travelling in the blood. For example, capillaries in mouse mammary carcinomas are known to have leaky pores with a size range of 1.2–2 µm [106]. Upon identification of leaky blood vessels, a similar sized microrobot by taking the advantage of active motility and controllability might cross the disorganized endothelial barriers through these pores for cancer therapy with the help of integrated medical imaging modalities.
The story does not end with the endothelial barriers and the next challenge comes with the other barriers, such as interstitial fluid pressure and fibrous elements of tissue extracellular matrix (ECM) (figure 2(F)). There are pores with a size range from less than 1 µm to 20 µm in diameter and channel-like tracks with a size up to 30 µm in width in the tissue extracellular microenvironment for passage [107]. While these openings and microcracks are potential penetration routes for microrobots assuming negligible adhesive interactions with ECM proteins, gradual degradation of the surrounding fibrous ECM proteins to enlarge meshes, a strategy of metastatic tumor cells, could also be a clever strategy that can be followed by a microrobot. This strategy can be realized by surface engineering of microrobots with matrix remodeling enzymes. However, encoding different barrier crossing strategies to the single design of microrobot is nontrivial, yet a prerequisite and a pivotal step towards maximizing the localization precision. Otherwise, these biological and fluidic barriers prevent proper extravasation of the microrobots to distal regions, resulting in sub-optimal delivery and function.
The mucosal barriers play an essential role in the protection and separation of the body's internal milieu from the external dangers (figure 2(G)). They are distributed around the body's tracts, such as the oral cavity, nasal cavity, gastrointestinal tract, eyes, pulmonary airways, and genitourinary tract. Mucosa is a viscoelastic, dense interconnected network formed by epithelial cells and their secreted substances, such as antimicrobial peptides and mucin, which is composed of highly glycosylated proteins [108]. The composition, thickness (from tens to hundreds of microns), pH values, and mesh size differ in different mucosal organs and in a pathological state. This necessitates a dedicated design of microrobots for the targeted mucosal barrier. For example, a study inspired by the Helicobacter pylori reported the penetration of the magnetically actuated helical-shaped microswimmers into mucin gel when their surface was functionalized with the urease enzyme. In the presence of urea, catalytic reaction with the urease resulted in an increase in the local pH, which locally liquefies the mucin gel and enables propellers to penetrate into it [109]. A biohybrid microrobot design also showed gastrointestinal and urinary cargo delivery and epithelial cell attachment based on lectin-mannose interaction [110]. However, for in vivo translation of such approaches, additional mucolytic activity is essential to create mucus-free space, where epithelial cells are no more covered and exposed to microrobots for attachment. In this regard, agents that have mucolytic activity, such as nacystelyn and gelsolin, may be used to enhance the transport of microrobots [111, 112]. Otherwise, penetration into the mucosa and the underlying epithelial layer is a highly challenging task without compromising mucosal barrier properties. One strategy to this end could be being small enough to avoid blockage by mucus mesh. Viruses with a size smaller than 100 nm in diameter and of neutral charge can diffuse through mucosa easily, whereas diffusion coefficients decrease with an increase in the size [113]. However, these entities diffuse passively and do not necessarily set measures to the upper limit for size. As such, with active navigation, successful demonstration for overcoming vitreous-mimetic porous barriers with magnetically actuated helical sub-micron scale robots has been shown. However, small size limits the propulsion speed and the drug loading capacity for potential therapeutic delivery applications [114]. This pitfall was circumvented by coating the microrobot surface with a slippery liquid layer, which minimized sticking to the matrix (figure 2(H)) [23]. Thus, magnetically actuated propellers crossed the vitreous humor and reached to the retina ex vivo.
Physiology of gastrointestinal system is complex and differs from segment to segment as well as the pathological state of the human body. The constant presence of gastric acid and digestive enzymes in stomach introduces another protective barrier against orally delivered agents. Preserving the stability of the microrobots in such harsh environment is crucial to fulfill the effective functioning. Recently, this acidic fluid was utilized as fuel to propel zinc-based micromotors in the stomach. In vivo binding, retention, and cargo delivery capabilities of the micromotors without causing any toxicity issues was also demonstrated [115]. Similarly, magnesium-based micromotors were propelled by neutralization of gastric acid through a chemical reaction that depletes the localized protons. pH-responsive polymer coating also enabled the release of the loaded drugs in a mouse model [116]. On the contrary to the acidic environment in the stomach, pH is alkaline and the mucosal thickness spatially varies in intestines. Therefore, orally administered microrobots, which target intestinal epithelium, need to be endowed with properties to safely traverse trough gastric environment, avoid non-specific interaction with the luminal content, such as microbiota, and penetrate into two layers of mucus lining. Also, changes in the intestinal permeability in certain pathophysiological situations, such as the Crohn's disease and inflammatory bowel disease, necessitates the application- and patient-oriented strategic designs to overcome these barriers.
Deployment strategy
The assessment of a microrobot's point of entry into the body is critical for developing an effective medical response. The route of a single microrobot, a team or swarm must be planned optimally based on the specific clinical scenario, considering the navigation distance and the biological barriers that need to be permeated. The complexity of the biological barriers varies depending on the size and the number of the microrobots, site of administration, pathophysiology of the target region, and the desired function (figure 3). A microrobot should permeate into minimum number of biological barriers to reach its intended site. This is important both for the minimization of the microrobot's overall design complexity and the invasiveness of the operation. Long-distance navigation of the microswimmer across distant body sites, i.e. on the order of tens of centimeters, may not be a viable approach, as this would require multiple tissue barriers that need to be crossed. As we discussed in the preceding section, moving microrobots from multiple body sites may leave protein corona imprints, which might severely affect the prescribed medical function of the microrobot. Additionally, the increased exposure of the microrobots as a result of long-distance navigation may increase the chance of clearance by the immune system. Consequently, the mobility of the microrobots should rather be seen as an enabler for short-distance navigations and precision in operations. In a realistic medical operation, however, some routes may require long-range navigation whereas with some other routes short-distance navigation suffices the completion of the task. For the short distance navigation, microrobots can be injected in the vicinity of a target site. Biohybrid designs using body's own immune cells, however, could be administered through the vasculature, as these cells are already adapted to navigate long distances in the bloodstream. These cells also possess an inherent machinery for transmigration across some of the tissues, intra and extravasation for long-distance navigation inside the body.
Actuation and control methods for medical microrobots
Enhancements in actuation, navigation, and control competencies of microrobots will have a high impact in their translation from bench to bedside. However, driving these untethered microrobots inside biological environments along pre-defined trajectories requires integrated actuation and control tools, which should fulfill at least four requirements: (1) They should establish a reliable connection between the microrobot operating in vivo and the external world, e.g. the medical doctor. (2) Actuation tools should provide sufficient power and force/torque to enable fast and efficient propulsion and accomplish the given medical tasks. (3) All these tools should be compatible with the human body. In addition, the integration of medical imaging and control modalities is critical to enable real-time control and feedback-guided robot navigation. (4) These instruments should be preferably present in the hospitals or be cost effective and suitable for the clinician and patient adoption.
Among the various actuation and control tools that have been proposed [18, 44, 117–121], so far the magnetic field is the most popular one, as large B fields can safely penetrate through human body [122, 123], making it meet all the requirements mentioned above. Different magnetic field signals have been prescribed to manipulate microrobots. Most intuitively, the magnetic spatial gradient can be used to pull or push the microrobot. The magnetic spatial gradient can be generated by different permanent [124] or electromagnet coil systems [117, 119] (figures 4(A)–(C)). Especially, implementing such an approach in an MRI system [125–130], such as interventional MRI [131], could dramatically transform this common medical imaging tool into robotic equipment, expanding its medical functionalities. Compared to the magnetic spatial gradient (decays as ~L−4, L is the distance away from the coil), the magnitude of the B field decays slower (decays as ~L−3). Thereby, it is easier to project B field into the human body and create magnetic torque on the microrobots [132]. In the millimeter scale, the field applicator of a clinical magnetic particle imaging (MPI) system (figure 4(B)) has used the magnetic torque on a millirobot to drill through muscle tissue and insert the needle for biopsy [44]. The same principle has also been demonstrated to clean the thrombosis in blood vessels [133, 134]. On micrometer scale, a rotating B field is used to drive corkscrew-shape microrobots [97, 135, 136], and an oscillating B field is used to drive a microrobot with a tail [137]. These actuation principles are proved to be more efficient than gradient pulling at the micron scale [132]. At last, varying both the B field and B field spatial gradient can produce complex field signals. This is especially suitable to control magnetic soft milli/microrobots to realize more complex motions [138–140]. Most of the field applicator of the current microrobotic systems assume an isotropy in the workspace. In the future, the development of high-temperature superconducting materials could greatly reduce coil size and increase the coil number of the magnetic setup [141]. Thereby, anisotropy could be generated in the workspace and in the human body. Such an effort can be used to control multiple microrobots [142, 143] or multiple elements on the robots independently to generate complex motions. Thereby, more sophisticated medical manipulations could be possible.

Figure 4. Potential actuation and control methods for medical microrobots in the body. (A) A preclinical magnetic resonance imaging (MRI) system [128] (2014) © Biomedical Engineering Society 2014. With permission of Springer. (B) A preclinical MPI system. Reproduced by [44]. CC BY 4.0. (C) OctoMag system with a rabbit placed in the workspace. Reproduced with permission from [118].
Download figure:
Standard image High-resolution imageThe acoustic waves are also external physical force generators, where they could easily meet the requirements for the actuation properties of untethered microrobots inside the human body [144]. To control miniaturized devices similar to microrobots, the acoustic actuation can be classified into two types. The first type is to remotely transmit energy by generating resonance, which can be produced by the bubble trapped onto the robot body [145–147] or by the robot body itself [148]. The second type is to generate a complex acoustic pattern to control multiple agents. Especially, the holographic acoustic tweezer could be generated by arranging transducers into different patterns [120]. Alternatively, a 3D-printed transmission hologram plate can be used to reconstruct acoustic wave into arbitrary patterns [121]. However, the acoustic waves have still not been used clinically for controlling microrobots. This could be due to the limited transmission of acoustic waves through hard tissues. Strong reflectors, such as diaphragms and bones, could greatly interfere with their transmission, which makes controlling microrobots acoustically inside the human body challenging [149].
Besides magnetic and acoustic actuations, light has also been applied to actuate and control microrobots in vitro, as it is easy to modulate light into complex patterns temporally and spatially to obtain a large degree of freedom [150–153]. In the future, light may potentially be used in the eye, as it's translucent, or under the skin, where the near infrared light (NIR) can penetrate to a certain depth [154]. Moreover, unicellular microorganisms [155] or catalyst-based designs [156, 157] can propel microrobots by harvesting energy from the surrounding environments. However, such an autonomous biohybrid or catalytic microrobot needs further control tools for steering and precise localization.
Medical imaging and tracking of microrobots
Reliable, safe, and precise application of microrobots inside the body requires feedback and communication with the operator. The design of a microrobot should thus always include a medical imaging strategy that is compatible with the given specific medical application scenario [158–160]. Optical microscopes have so far been the primary tool for the localization and real-time tracking of microrobots in the in vitro conceptual studies and the preclinical experiments [161]. Their success in the light-of-sight access to the microrobots in vitro is mostly not transferrable to in vivo workspace. Main criteria for the selection of in vivo and clinical imaging modalities are as follows: (1) Imaging modalities that have evidence-based reliability in clinics, (2) compatibility of the imaging modalities with the actuation, control and other hardware and software of the microrobotic system, (3) medical personnel familiar with the clinical imaging modalities, so there will not be a steep learning curve for the imaging of microrobots, (4) wide availability and easy access that will reduce the cost of adoption toward the use of microrobots in clinics. The spatial resolution of the instrument, the image acquisition rate and the penetration depth may be interdependent and can be best optimized for a given medical task. The microrobot parameters, such as size, material type, localization accuracy, etc, should always be evaluated given the medical requirements and the interdependent parameters of the imaging modalities (table 2). In this section, we assess the potential of the state-of-the-art medical imaging modalities for their potential integration with microrobots.
Table 2. Potential medical imaging modalities for localization and tracking of microrobots. The capabilities of the medical imaging instruments may vary in clinical (human) and animal setups. The resolving power of the instrument, the image acquisition rate and the penetration depth may be interdependent and can be best optimized for a given medical task. The microrobot parameters, such as size, material type, localization accuracy, etc, should always be evaluated given the medical requirements and the interdependent parameters of the imaging modalities.
| Imaging modality | Detectable robot size (estimate based on animal setups) | Contrast enhancement | Advantages | Disadvantages |
|---|---|---|---|---|
| Magnetic resonance imaging | ≈100 µm | Magnetic micro/nanoparticles, gadolinium complexes | High resolution and soft-tissue contrast, non-invasive, 3D localization | Long acquisition time, low sensitivity, high cost |
| Fluoroscopy | ≈200 µm | Iodinated molecules, metals, nanoparticles | Real-time imaging, high sensitivity, high body penetration | X-ray radiation, 2D, poor soft contrast |
| Computed tomography imaging | <10 µm | Iodinated molecules, metals, nanoparticles | High spatial resolution | Slow scanning rate, x-ray radiation, poor soft contrast |
| Ultrasound imaging | ≈30 µm | Echogenic micro bubbles | Real-time imaging, simple, low cost, safe | Operator dependency, tissue penetration limit |
| Positron emission tomography | ≈1 mm | Radioisotopes (e.g. 18F) | Very high sensitivity with unlimited depth penetration, molecular imaging | High cost, slow, limited anatomical information without CT scan |
Magnetic resonance imaging (MRI)
MRI provides the highest resolution in the 3D images of soft tissues, organs, and the vasculature without radiation exposure and invasive interventions. It is an essential diagnostic tool and a part of the daily routine in clinics, as 1 of 10 patients received an MRI scan in USA in 2017 [162]. To generate an image, MRI scanners use a very high (1.5–7 T) uniform magnetic field, precisely-controlled superimposed field gradients, and radio waves. MRI instruments in clinics derives the signal from the proton of hydrogens of water molecules. When these protons are exposed to a strong uniform field, they take one of two possible orientations with respect to the applied field. These two orientations have slightly different energy levels proportional to the applied field and hence produce a net magnetization that enables the imaging. The imaging intensity is modulated by the local density of water. Because the magnetic fields can safely penetrate deep inside the body and create detailed scanned images of tissues, MRI can be a very robust and potential modality for the 3D localization and tracking of microrobots (figure 5(A)). The voxel size of a clinical MRI instrument is around 500 µm, which could be much bigger than the size of a single microrobot, depending on the application requirements [160]. As a result, the localization of microrobots with MRI may not be sufficient to detect a single microrobot easily [163, 164]. To alleviate this problem, a microrobot with high magnetic susceptibility, such as with a ferromagnetic compartment, can be used to create an image signal bigger than the robot itself. Coating spiral-shape microalgae with a ferromagnetic material was shown to enhance the imaging contrast for localization [165]. For synthetic microswimmers, incorporation of ferromagnetic materials or encapsulating the robot with iron oxide nanoparticles allowed their easier monitoring with MRI [21, 166–168]. However, a potential downside of this method is the resulting imaging artifacts, which could reduce the accuracy in localization. Obtaining scanned images with MRI takes a comparatively long time, which may restrict the utilization of MRI as a real-time in vivo tracker.

Figure 5. Medical imaging modalities for microrobots. (A) Magnetic resonance imaging (MRI) of swarms of magnetic S. platensis inside rat stomach, actuated for 5 min and 12 min. From [21]. Reprinted with permission from AAAS. (B) Ultrasound imaging of a magnetic robot ex vivo in chicken muscle tissue. Reprinted by permission from: Springer Nature [139] 2018. (C) X-ray angiography image showing the locomotion of a robot in the rabbit aorta. Reproduced from [193]. CC BY 3.0. (D) In vivo fluorescence imaging of S. platensis in the intraperitoneal cavity of mice. From [21]. Reprinted with permission from AAAS.
Download figure:
Standard image High-resolution imageX-ray imaging
Medical x-ray imaging is a well-established method coupled with different modalities, such as fluoroscopy and computed tomography (CT). It is used in diagnostic and interventional practices coupled with contrast agents. Its working principle relies on the emitted x-ray from a focused source that crosses the body and the absorption of x-rays is inversely proportional to the density of the tissue of the body. Conventional fluoroscopy can have high frame rates up to 30 frames per second (fps) with low dose x-ray exposure thus it is able to monitor interventions in real time [169]. Fluoroscopy is able to provide real time movies of swallowing, urination, or flow through the luminal organs such as fallopian tubes. Soft materials and tissues require contrast agents, such as metals, iodinated molecules, tantalum and gold nanoparticles for fluoroscopy imaging [170]. However, it has low resolution (with the spot size of around 0.3 mm), limiting the bottom size in microrobotic applications. In contrast to MRI, which has a very limited work space, fluoroscopy allows for considerably more space and flexibility for the installation of other actuation and microrobotic controllers around the patient. CT can perform high-resolution 3D x-ray scans and provide large penetration depths. However, it requires much higher exposure to the ionizing radiation and hence the image acquisition times become longer. CT fluoroscopy (CTF) may also prove useful for the real-time tracking of microrobots in higher resolution than provided by fluoroscopy with a higher frame than provided by conventional CT [171]. In imaging-guided percutaneous applications, CTF provides fast correction for depth and direction of needles. In microrobotics, CTF can provide fast 3D information for more precise localization of microrobots inside the tissue. However, an important disadvantage of x-ray related imaging modalities is the invasiveness of the imaging and the presence of ionizing radiation that can cause DNA damage to cells in high and long exposures.
Ultrasonography
Ultrasonography is a non-invasive, inexpensive and real-time medical imaging type, which is widely used even in office practices. In clinics, ultrasonography is frequently used for the detection of intrauterine abnormalities, cardiac function analysis and vascular abnormalities. The imaging relies on high-frequency sound waves, typically in the diagnostic range of 1–40 MHz, which propagate through the soft tissue and the returning echoes are analyzed to create the image. Frequency of ultrasound waves determines the penetration depth and resolution. Higher-frequency ultrasound allows higher resolving power whereas the tissue penetration is better at lower frequencies. Therefore, coupling ultrasound imaging with microrobots is a promising approach for microrobot-aided less-invasive inpatient and outpatient interventions within up to 10–15 cm in the soft tissues. The inverse relationship between the size and the depth of the operable site in the body determines the suitability of this imaging type in the given microrobotic operation. The imaging acquisition rate of ultrasound is typically much faster than those of PET, x-ray, and MRI. A soft robot with the length of 3.7 mm and a gripper with the diameter of 4 mm were successfully visualized via ultrasonographic investigation (figure 5(B)) [139, 172]. However, beads down to 200 µm, could still be resolved with high-frequency ultrasound devices [173]. To enhance the visibility of microrobots, different contrast agents can be used, such as echogenic micro bubbles [174, 175] and iron oxide nanoparticles [176]. Ultrasound imaging contains its own limitations in the positioning errors, background signals, and artifacts. Additionally, interpretation of US images requires significant expertise.
Optical tracking, fluorescence imaging, and MPI are other emerging tools pursued for the medical imaging of microrobots in vivo (figure 5(D)) [21]. Indeed, each method accommodates particular advantages and disadvantages, which need to be balanced to optimize the imaging-function coupling. Radiation exposure of healthcare providers and patients and cost effectiveness are additional critical parameters to consider during design of the proper medical imaging and tracking modality for microrobots. Inherent limitations and strengths of each imaging modality have spurred the development of combinatorial systems to obtain maximum performance with synergistic imaging. For example, positron emission tomography (PET) combined with CT has been used to track large numbers of microrobots in vivo [161].
Shape, materials, and manufacturing of multi-functional microrobots
The physical design of a microrobot should contain all the functions necessary to implement it during the course of a medical application, which is manifested in its size, body shape, and the material composition (figure 6). The size of a microrobot puts a major limitation on in which body part a microrobot can be used and the deployment strategy that can be planned. The impact of size as a design criterion is separately discussed in above biological barriers and deployment sections in detail. The body shape mainly defines the dynamic interactions of the microrobot body with the surrounding body fluid. In the low Reynolds number regime, the fundamental characteristics of a microscopic swimmer is to do time-irreversible, i.e. non-reciprocal, shape changes with its body [132, 177]. Nevertheless, most biological fluids are heterogeneous and exhibit viscoelastic behavior. They are vastly different from fully viscous in vitro test environments for microrobots. A microrobot can also move with reciprocal periodic body-shape changes in physiological fluids with viscoelastic character [178]. The net propulsion here is enabled by the modulation of the local fluid viscosity by varying the shear rate exerted by the swimmer body. The optimization of each body shape design should consider the operational conditions of the physiological and pathological body fluids, such as blood, cerebrospinal fluid, synovial fluid, and vitreous humor. An interesting example to this end is the bile secreted from gallbladder. Physiological bile is a Newtonian fluid whereas a pathological formation changes it to a non-Newtonian character [179]. Operating in a dynamic and harsh environment inside the human body thus requires immense adaptability and versatility to the changes in the environment. Compliant structures that self-regulate their mobility to adapt the dynamic properties of the fluid might present a viable solution to this end [139, 180]. Formerly proposed microswimmers may also need to be revisited for their optimal design and performance toward their in vivo and later clinical applications, as their propulsion speed, energy efficiency, and control may significantly vary in different body fluids and based on the type and severity of the pathogen. When a microrobot is inside the body, it is prone to attacks by the host immune system, and hence its active operation time is closely related with the time of recognition. This recognition is primarily governed by the surface chemistry, which is discussed in the biological barriers section, and body shape of the microrobots. At comparable size scales, microstructures with spiral geometry are less prone to attack by the macrophages compared to spherical or rod geometries [181].

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Figure 6. Physical design of a medical microrobot. The physical design of a microrobot contains all the information necessary to implement it during the course of a medical application. The choice of size, material, and body shape have individual and confounding effects on various robotic and medical functions as well as the ultimate fate of the microrobot, including swimming behavior, site of administration, barriers that will be encountered, the complex interactions with biological environment, and biodegradation.
Download figure:
Standard image High-resolution image{kind=link}
The material composition of a microrobot plays the foremost role in enabling its prescribed smart performance. Typically, a base material forms the body shape and acts as that the carrier matrix for the other subcomponents to be incorporated with. The choice of the right base material needs evaluation based on the biocompatibility, mechanical properties, and suitability for manufacturing in the desired body shape and composition. The biocompatibility and related aspects are discussed in detail in below section related to regulatory aspects. The mechanical properties may be important for making soft microrobots that rely on body shape deformation [18, 139]. A diverse type of information can be encoded by controlling physical and chemical properties of the microrobots locally [14]. The interior body shape is important to create hierarchical and composite designs for encoding magnetic information [24, 139]. Coupled sensing and response capabilities in the material composition can further enable robust design routes for achieving dynamic interactions with the environment [170]. This is achievable with materials that are responsive to either remote, e.g. light [22, 151, 182], temperature [182], magnetic [183], and acoustic [146] or local biochemical signals [24], and pH [184] in the body. When the medical task of a microrobot is accomplished, it needs to be fully retrieved from the body [185]. Another safe option for removing it from the body is to expect its degradation to non-toxic products. Materials that predictably decompose and disappear over time as a result of the resident biological activity have become increasingly important for medical applications [186]. Such degradation could be achieved by means of enzymatic degradation or disintegration in the salt solution [7, 21]. Microrobots not adopting this design aspect may complicate their clinical use due to potential adverse effects in the body, which might result in serious acute and chronic toxicities and might require surgical revisions.
Encoding diverse types of functional information in microrobots requires powerful fabrication methods, as it integrates the 3D body shape, material composition and the other essential aspects summarized in figures 1 and 6. However, as the size of a microrobot goes smaller, the availability of the potential techniques become scarce. A variety of 2D and 3D microfabrication techniques, including photolithography, material deposition, electroplating, and micromolding have been used for developing various types of microrobots [7, 11]. The breakthrough came, however, with the integration of computer-aided design (CAD) to two-photon lithography type of 3D printing-based microfabrication technologies. As a result, almost all arbitrary and challenging 3D body shapes became possible to print with submicron feature size [187]. Additive manufacturing processes enabled by two-photon crosslinking has enabled an unprecedented 3D design and manufacturing freedom for various microrobot designs [14, 22, 24].
Regulatory aspects of translational microrobotics research
Developing a translational research project for microrobotics is not an easy task. From the preclinical testing of a microrobot to its bedside application, a number of safety-related regulatory aspects need to be taken under consideration. First critical distinction for the regulatory assessment of a microrobot is to decide whether it is a drug or a medical device. According to the Food and Drug Administration (FDA) in USA, the distinction of a drug from a medical device is that a drug achieves its primary action by means of a chemical reaction inside the body or after being metabolized by the body [188]. Because the physical design, composition, medical functions and control methods of a microrobot are application-oriented, each microrobot should be decided separately for evaluation as a drug or a device. The theme of the present perspective is more inclined to see the microrobots as medical devices, so the rest of the discussion will be based on this presumption.
Any material that comes in contact with the biological system must be compatible with it. Biocompatibility is rather a nebulous term, and it might require different considerations based on the types of tissue that the microrobot will be exposed to and the duration of that exposure. For example, a microrobot developed to operate inside the circulatory system must possess hemocompatibility, and a microrobot intended to operate for long durations might require reproductive and developmental toxicity tests. As a general rule, all preclinical safety assessments of a medical product should be conducted according to good laboratory practice (GLP) procedures [189]. GLP provides the quality and integrity basis of the preclinical (non-clinical, i.e. not involving human subjects) research and development. When planning a medical microrobot, GLP compliance will be required for biocompatibility regulatory submissions [190]. Bedside translation of untethered microrobots will prerequisite traditional in vitro and in vivo biocompatibility tests to be carried out under International Organization for Standardization (ISO) Standard 10993, Biological Evaluation of Medical Devices. Testing strategies that comply with ISO 10993 is acceptable in Europe and mostly in USA [191].
Cytotoxicity provides safety information for the short durations in vitro while the long duration impact of a material might also be evaluated for unanticipated foreign responses [192]. Because a microrobot is typically a composite material, material characterization and analysis of the microrobot's components should be conducted even before any biological testing. The chemical characterization of the microrobots should be able to detect leachable materials that might compromise the in vivo safety. There is risk in testing the assembled microrobot without obtaining safety data on its component materials. If an adverse result occurs, it could be difficult to integrate all the components from alternative materials, as the intrinsic material properties might unexpectedly complicate the assembly. Such iterations might later end up delaying the translation process and repeating some of the critical safety tests. While potentially leachable toxic materials might be desirable for preclinical concept development, their in vivo and translational applications require strict consideration. There is accumulating knowledge and expertise in the biomaterials field along the same line that could provide a wealth of inspirations regarding type and composition of the materials that to inspire the fabric of microrobots. Pharmacokinetic studies must be given a special emphasis here to investigate the metabolic processes of absorption, distribution, biotransformation, and elimination of leachable materials and degradation products. These studies are also essential to investigate the therapeutic and diagnostic release performance of the microrobots in vivo.
However, additional new types of tests for microrobots may be necessary at the preclinical level. Given the sensitivity of the operations in the body, the degree of autonomy and its potential ethical and legal aspects must be taken into account [165]. As the level of autonomy in the microrobots increases, a master switch that turns off all microrobots, or fail-safe strategies may be needed that would contain the situation in case the execution of the medical task fails or adverse effects are observed. For example, in the biohybrid design strategy, uncontrolled proliferation of unicellular organisms may lead to a heavy infection in the body, might be prevented by introducing conditional knockout of critical genes. When some of the biohybrid microrobots go out of control, such genes are knocked out and the microorganisms are destined to die. In these aspects, medical microrobots are substantially different than any current FDA-approved medical device and have typically moderate or high risk to the patient, similar to most commercial medical robot systems. Therefore, they would likely be Class II or III medical devices for commercialization in the future, which would need special controls (in addition to general controls), which would increase their cost and duration of receiving regulatory permissions before using them in the clinical setting.
Conclusion and outlook
There are exciting opportunities using microrobots in minimally invasive medical interventions and targeted diagnosis and therapy. Their active mobility can make them unrivalled for accessing into any body part to perform very robust and precise operations. However, realization of their full potential requires dealing with multiple layers of complexity, which is uniquely defined in each potential clinical scenario. To alleviate this complexity, there are several take-home messages from this perspective:
- We need to foster to the greatest extent an application-specific design strategy for any microrobotic system, well-defined in a medical project from the point of administration to their final removal/extraction as a whole process.
- All functions required to operate a medical microrobot must be reflected in its physical design, where all parts of a microrobot are highly interconnected and embedded in its material fabric. Integration strategies and methods of all functional parts together simultaneously is one of the main grand challenges in this field.
- The choice of right material and its biocompatibility, biodegradability, smart performance, and suitability for manufacturing with the right body shape and composition depends on the availability of the material. Microrobotics can appreciate plenty of leverage from biomaterials research. Synthesis of new smart materials and adoption of the existing biomaterials from the drug delivery and tissue engineering fields can greatly help microrobots improve their overall performance. Relying on the safe biomaterials to the greatest extent possible will help alleviate potential delays during the bench-to-bedside translation of the microrobots.
- Despite the success achieved in precise actuation, control, and localization of microrobots in vitro, further improvement is required for in vivo adaptation of actuation, control, and medical imaging techniques for the demands of a clinical-level application.
- Biological barriers constitute the biggest challenge for operation of a microrobot in vivo. A microrobot should permeate into minimum number of barriers to reach its intended site. This is important both for the minimization of the microrobot's overall design complexity and the invasiveness of the operation.
- All these new design considerations, summarized in figures 1 and 6, require the development of more realistic preclinical tests rather than simple in vitro tests. In order to reduce the animal use, the iterative designs of microrobots can be improved in the ex vivo tissues and realistic phantoms. Considering the regulatory permission aspects already in the preclinical tests can greatly speed up the bench-to-bedside translation of microrobots.