
Multiple Sclerosis, Disease-Modifying Therapies and COVID-19: A Systematic Review on Immune Response and Vaccination Recommendations

 ,
,
Abstract
:1. Introduction
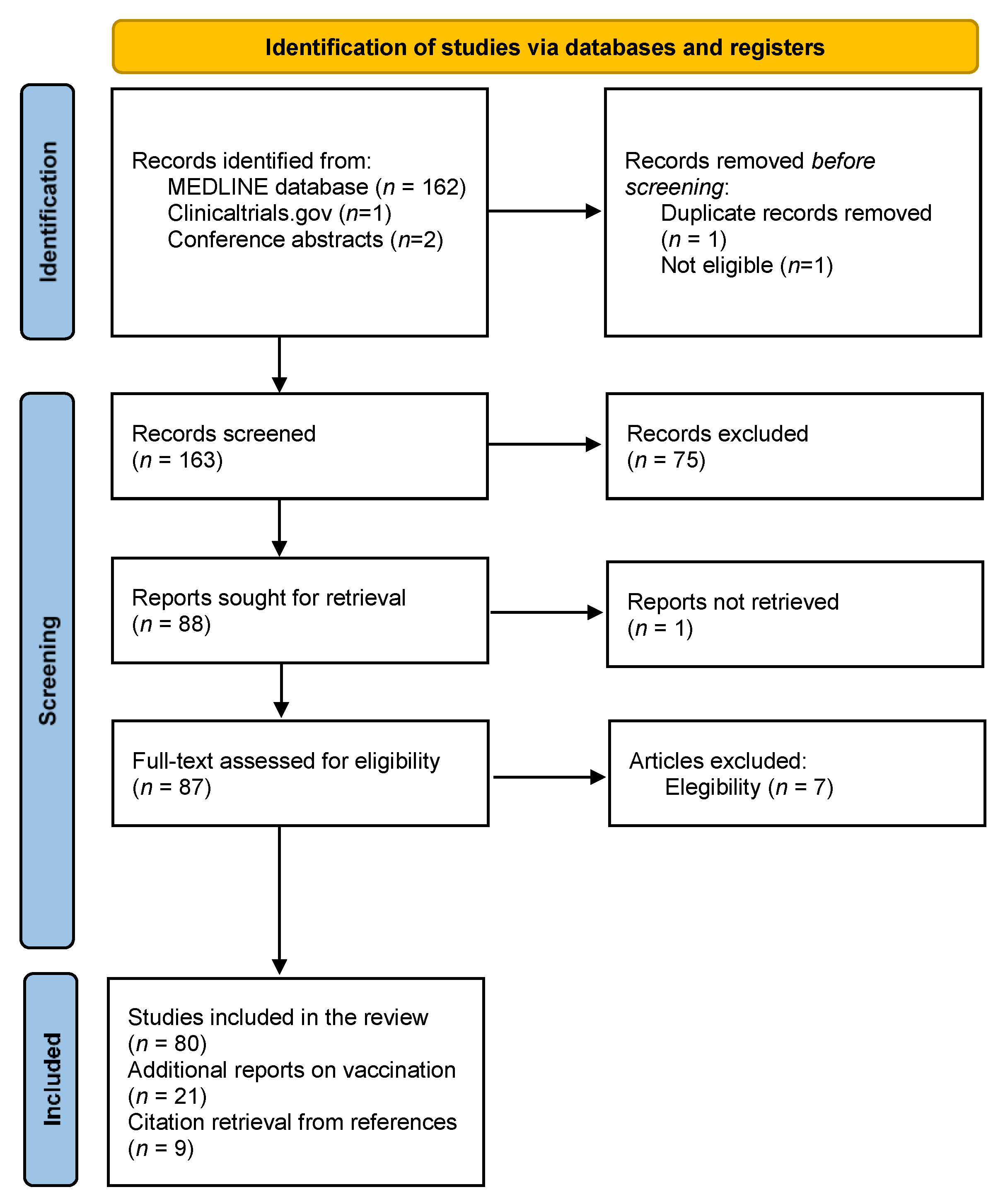
2. Materials and Methods
3. Results

{kind=link}
| Drug | COVID-19 Cases | Death See text for details | Total (%) | References | |
|---|---|---|---|---|---|
| Confirmed | Suspected | ||||
| Beta-interferon | 144 | 74 | 4 | 218 (4.9) | [7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25] |
| Glatiramer acetate | 196 | 73 | 4 | 269 (6.1) | [8,10,11,15,16,18,19,20,21,22,23,24,25,29,30,31] |
| Dimethyl fumarate | 408 | 195 | 19 | 603 (13.7) | [8,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,29,31,35,40,41] |
| Teriflunomide | 202 | 49 | 4 | 251 (5.7) | [7,8,10,13,15,16,17,18,19,20,21,22,23,24,25,31,32,33,34,35,36,37,38,39] |
| Dimethyl fumarate/teriflunomide § | - | 108 | - | 108 (2.4) | [30,31] |
| Fingolimod | 268 | 146 | 1 | 414 (9.4) | [7,8,10,11,14,15,16,17,18,19,20,22,23,24,25,30,31,35,37,43,44,45,46,47,48,49] |
| Siponimod | 19 | - | 2 | 19 (0.4) | [11,25] |
| Ponesimod | - | 1 | - | 1 (0) | [18] |
| Non-specified S1P 1 modulator | 29 | - | - | 29 (0.7) | [21] |
| Natalizumab | 325 | 136 | 20 | 461 (10.4) | [8,11,13,14,15,16,18,19,20,21,22,23,24,25,30,31,35,50,51,52] |
| Alemtuzumab | 35 | 23 | 1 | 58 (1.3) | [8,13,16,17,18,19,20,21,22,23,24,25,31,72,73,74,75,76,77] |
| Cladribine | 195 | 140 | 1 | 335 (7.6) | [8,17,18,19,20,23,25,31,78,79,80,81,82,83,84] |
| Alemtuzumab/cladribine § | - | 15 | - | 15 (0.3) | [30] |
| Ocrelizumab | 1042 | 173 | 35 | 1215 (27.5) | [8,11,13,15,16,18,19,22,23,24,25,29,35,53,54,55,56,57,58,59,60,61,62,63] |
| Rituximab | 211 | 25 | 8 | 236 (5.3) | [7,8,11,12,15,22,23,24,25,54,59,64,65,66,67,68] |
| Ofatumumab | 13 | - | - | 13 (0.3) | [70,71] |
| Non-specified anti-CD20 | 123 | 49 | - | 172 (3.9) | [21,30,31] |
| Total | 3210 | 1207 | 99 | 4417 (100) | |
COVID-19 Vaccine in MS Patients on DMTs
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Wang, J.; Jiang, M.; Chen, X.; Montaner, L.J. Cytokine storm and leukocyte changes in mild versus severe SARS-CoV-2 infection: Review of 3939 COVID-19 patients in China and emerging pathogenesis and therapy concepts. J. Leukoc. Biol. 2020, 108, 17–41. [Google Scholar] [CrossRef]
- Han, M.; Xu, M.; Zhang, Y.; Liu, Z.; Li, S.; He, T.; Li, J.; Gao, Y.; Liu, W.; Li, T.; et al. Assessing SARS-CoV-2 RNA levels and lymphocyte/T cell counts in COVID-19 patients revealed initial immune status as a major determinant of disease severity. Med. Microbiol. Immunol. 2020, 209, 657–668. [Google Scholar] [CrossRef] [PubMed]
- Ghaderi, S.; Berg-Hansen, P.; Bakken, I.J.; Magnus, P.; Trogstad, L.; Håberg, S.E. Hospitalization following influenza infection and pandemic vaccination in multiple sclerosis patients: A nationwide population-based registry study from Norway. Eur. J. Epidemiol. 2020, 35, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Bhise, V.; Dhib-Jalbut, S. Potential Risks and Benefits of Multiple Sclerosis Immune Therapies in the COVID-19 Era: Clinical and Immunological Perspectives. Neurotherapeutics 2021, 18, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.; Straus, S.; Thorlund, K.; Jansen, J.P.; et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: Checklist and explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef] [Green Version]
- Safavi, F.; Nourbakhsh, B.; Azimi, A.R. B-cell depleting therapies may affect susceptibility to acute respiratory illness among patients with multiple sclerosis during the early COVID-19 epidemic in Iran. Mult. Scler. Relat. Disord. 2020, 43, 102195. [Google Scholar] [CrossRef]
- Louapre, C.; Collongues, N.; Stankoff, B.; Giannesini, C.; Papeix, C.; Bensa, C.; Deschamps, R.; Créange, A.; Wahab, A.; Pelletier, J.; et al. Clinical Characteristics and Outcomes in Patients with Coronavirus Disease 2019 and Multiple Sclerosis. JAMA Neurol. 2020, 77, 1079–1088. [Google Scholar] [CrossRef]
- Gemcioglu, E.; Davutoglu, M.; Ozdemir, E.E.; Erden, A. Are type 1 interferons treatment in Multiple Sclerosis as a potential therapy against COVID-19? Mult. Scler. Relat. Disord. 2020, 42, 102196. [Google Scholar] [CrossRef] [PubMed]
- Bowen, J.D.; Brink, J.; Brown, T.R.; Lucassen, E.B.; Smoot, K.; Wundes, A.; Repovic, P. COVID-19 in MS: Initial observations from the Pacific Northwest. Neurol. Neuroimmunol. neuroinflammation 2020, 7, e783. [Google Scholar] [CrossRef] [PubMed]
- Parrotta, E.; Kister, I.; Charvet, L.; Sammarco, C.; Saha, V.; Charlson, R.E.; Jonathan, H.; Gutman, J.M.; Gottesman, M.; Abou-Fayssal, N.; et al. COVID-19 outcomes in MS: Observational study of early experience from NYU Multiple Sclerosis Comprehensive Care Center. Neurol. Neuroimmunol. Neuroinflammation. 2020, 7, e835. [Google Scholar] [CrossRef]
- Barzegar, M.; Mirmosayyeb, O.; Ghajarzadeh, M.; Nehzat, N.; Vaheb, S.; Shaygannejad, V.; Vosoughi, R. Characteristics of COVID-19 disease in multiple sclerosis patients. Mult. Scler. Relat. Disord. 2020, 45, 102276. [Google Scholar] [CrossRef]
- Ciampi, E.; Uribe-San-Martin, R.; Cárcamo, C. COVID-19 pandemic: The experience of a multiple sclerosis centre in Chile. Mult. Scler. Relat. Disord. 2020, 42, 102204. [Google Scholar] [CrossRef]
- Mantero, V.; Abate, L.; Balgera, R.; Basilico, P.; Salmaggi, A.; Cordano, C. Assessing the susceptibility to acute respiratory illness COVID-19-related in a cohort of multiple sclerosis patients. Mult. Scler. Relat. Disord. 2020, 46, 102453. [Google Scholar] [CrossRef]
- Sahraian, M.A.; Azimi, A.; Navardi, S.; Ala, S.; Naser Moghadasi, A. Evaluation of the rate of COVID-19 infection, hospitalization and death among Iranian patients with multiple sclerosis. Mult. Scler. Relat. Disord. 2020, 46, 102472. [Google Scholar] [CrossRef] [PubMed]
- Chaudhry, F.; Bulka, H.; Rathnam, A.S.; Said, O.M.; Lin, J.; Lorigan, H.; Bernitsas, E.; Rube, J.; Korzeniewski, S.J.; Memon, A.B.; et al. COVID-19 in multiple sclerosis patients and risk factors for severe infection. J. Neurol. Sci. 2020, 418, 117147. [Google Scholar] [CrossRef]
- Castillo Álvarez, F.; López Pérez, M.; Marzo Sola, M.E. Risk of SARS-CoV-2 infection and clinical outcomes in multiple sclerosis patients in La Rioja (Spain): Riesgo de infección por SARS-CoV-2 y resultados clínicos en pacientes con esclerosis múltiple en la Rioja (España). Med. Clin. 2020, 155, 362. [Google Scholar] [CrossRef] [PubMed]
- Sormani, M.P.; De Rossi, N.; Schiavetti, I.; Carmisciano, L.; Cordioli, C.; Moiola, L.; Radaelli, M.; Immovilli, P.; Capobianco, M.; Trojano, M.; et al. Disease-Modifying Therapies and Coronavirus Disease 2019 Severity in Multiple Sclerosis. Ann. Neurol. 2021, 89, 780–789. [Google Scholar] [CrossRef]
- Evangelou, N.; Garjani, A.; Dasnair, R.; Hunter, R.; A Tuite-Dalton, K.; Craig, E.M.; Rodgers, W.J.; Coles, A.; Dobson, R.; Duddy, M.; et al. Self-diagnosed COVID-19 in people with multiple sclerosis: A community-based cohort of the UK MS Register. J. Neurol. Neurosurg. psychiatry 2020, 92, 107–109. [Google Scholar] [CrossRef] [PubMed]
- Loonstra, F.C.; Hoitsma, E.; van Kempen, Z.L.; Killestein, J.; Mostert, J.P. COVID-19 in multiple sclerosis: The Dutch experience. Mult. Scler. 2020, 26, 1256–1260. [Google Scholar] [CrossRef]
- Reder, A.T.; Centonze, D.; Naylor, M.L.; Nagpal, A.; Rajbhandari, R.; Altincatal, A.; Kim, M.; Berdofe, A.; Radhakrishnan, M.; Jung, E.; et al. COVID-19 in Patients with Multiple Sclerosis: Associations with Disease-Modifying Therapies. CNS Drugs 2021, 35, 317–330. [Google Scholar] [CrossRef]
- Zabalza, A.; Cárdenas-Robledo, S.; Tagliani, P.; Arrambide, G.; Otero-Romero, S.; Carbonell-Mirabent, P.; Rodriguez-Barranco, M.; Rodríguez-Acevedo, B.; Vera, J.L.R.; Resina-Salles, M.; et al. COVID-19 in multiple sclerosis patients: Susceptibility, severity risk factors and serological response. Eur. J. Neurol. 2020. [Google Scholar] [CrossRef]
- Alonso, R.; Silva, B.; Garcea, O.; Diaz, P.E.C.; Dos Passos, G.R.; Navarro, D.A.R.; Garcia Valle, L.A.; Salinas, L.; Negrotto, L.; Luetic, G.; et al. COVID-19 in multiple sclerosis and neuromyelitis optica spectrum disorder patients in Latin America: COVID-19 in MS and NMOSD patients in LATAM. Mult. Scler. Relat. Disord. 2021, 51, 102886. [Google Scholar] [CrossRef] [PubMed]
- REDONE.br – Neuroimmunology Brazilian Study Group Focused on COVID-19 and MS. Incidence and clinical outcome of Coronavirus disease 2019 in a cohort of 11,560 Brazilian patients with multiple sclerosis. Mult. Scler. 2021. [CrossRef]
- Salter, A.; Fox, R.J.; Newsome, S.D.; Halper, J.; Li, D.K.; Kanellis, P.; Costello, K.; Bebo, B.; Rammohan, K.; Cutter, G.R.; et al. Outcomes and Risk Factors Associated With SARS-CoV-2 Infection in a North American Registry of Patients With Multiple Sclerosis. JAMA Neurol. 2021, 78, 699–708. [Google Scholar] [CrossRef] [PubMed]
- Berger, J.R.; Brandstadter, R.; Bar-Or, A. COVID-19 and MS disease-modifying therapies. Neurol. Neuroimmunol. Neuroinflammation 2020, 7. [Google Scholar] [CrossRef]
- Laroni, A.; Schiavetti, I.; Sormani, M.P.; Uccelli, A. COVID-19 in patients with multiple sclerosis undergoing disease-modifying treatments. Mult. Scler. 2020. [Google Scholar] [CrossRef]
- Stertz, S.; Hale, B.G. Interferon system deficiencies exacerbating severe pandemic virus infections. Trends Microbiol. 2021. [Google Scholar] [CrossRef]
- Kataria, S.; Tandon, M.; Melnic, V.; Sriwastava, S. A case series and literature review of multiple sclerosis and COVID-19: Clinical characteristics, outcomes and a brief review of immunotherapies. Eneurologicalsci 2020, 21, 100287. [Google Scholar] [CrossRef]
- Costa, G.D.; Leocani, L.; Montalban, X.; Guerrero, A.I.; Sørensen, P.S.; Magyari, M.; Dobson, R.J.B.; Cummins, N.; Narayan, V.A.; Hotopf, M.; et al. Real-time assessment of COVID-19 prevalence among multiple sclerosis patients: A multicenter European study. Neurol. Sci. 2020, 41, 1647–1650. [Google Scholar] [CrossRef]
- Nesbitt, C.; Rath, L.; Yeh, W.Z.; Zhong, M.; Wesselingh, R.; Monif, M.; Richards, J.; Minh, V.B.; Jokubaitis, V.G.; Skibina, O.; et al. MSCOVID19: Using social media to achieve rapid dissemination of health information. Mult. Scler. Relat. Disord. 2020, 45, 102338. [Google Scholar] [CrossRef] [PubMed]
- Maghzi, A.H.; Houtchens, M.K.; Preziosa, P.; Ionete, C.; Beretich, B.D.; Stankiewicz, J.M.; Tauhid, S.; Cabot, A.; Berriosmorales, I.; Schwartz, T.H.W.; et al. COVID-19 in teriflunomide-treated patients with multiple sclerosis. J. Neurol. 2020, 267, 2790–2796. [Google Scholar] [CrossRef] [PubMed]
- Ciardi, M.R.; Zingaropoli, M.A.; Pasculli, P.; Perri, V.; Tartaglia, M.; Valeri, S.; Russo, G.; Conte, A.; Mastroiannia, C.M. The peripheral blood immune cell profile in a teriflunomide-treated multiple sclerosis patient with COVID-19 pneumonia. J. Neuroimmunol. 2020, 346, 577323. [Google Scholar] [CrossRef] [PubMed]
- Mantero, V.; Baroncini, D.; Balgera, R.; Guaschino, C.; Basilico, P.; Annovazzi, P.; Zaffaroni, M.; Salmaggi, A.; Cordano, C. Mild COVID-19 infection in a group of teriflunomide-treated patients with multiple sclerosis. J. Neurol. 2020, 268, 2029–2030. [Google Scholar] [CrossRef]
- Crescenzo, F.; Marastoni, D.; Bovo, C.; Calabrese, M. Frequency and severity of COVID-19 in multiple sclerosis: A short single-site report from northern Italy. Mult. Scler. Relat. Disord. 2020, 44, 102372. [Google Scholar] [CrossRef]
- Möhn, N.; Saker, F.; Bonda, V.; Respondek, G.; Bachmann, M.; Stoll, M.; Wattjes, M.P.; Stangel, M.; Skripuletz, T. Mild COVID-19 symptoms despite treatment with teriflunomide and high-dose methylprednisolone due to multiple sclerosis relapse. J. Neuro. 2020, 267, 2803–2805. [Google Scholar] [CrossRef] [PubMed]
- Bollo, L.; Guerra, T.; Bavaro, D.F.; Monno, L.; Saracino, A.; Angarano, G.; Paolicelli, D.; Trojano, M.; Iaffaldano, P. Seroconversion and indolent course of COVID-19 in patients with multiple sclerosis treated with fingolimod and teriflunomide. J. Neurol. Sci. 2020, 416, 117011. [Google Scholar] [CrossRef]
- Capone, F.; Motolese, F.; Luce, T.; Rossi, M.; Magliozzi, A.; Di Lazzaro, V. COVID-19 in teriflunomide-treated patients with multiple sclerosis: A case report and literature review. Mult. Scler. Relat. Disord. 2021, 48, 102734. [Google Scholar] [CrossRef]
- Yetkin, M.F.; Yetkin, N.A.; Akcakoyunlu, M.; Mirza, M. Transient monocular visual impairment as an initial symptom of COVID-19 infection in an individual with multiple sclerosis receiving teriflunomide. Neurol. Sci. 2021, 42, 1661–1664. [Google Scholar] [CrossRef]
- Capone, F.; Ferraro, E.; Motolese, F.; Di Lazzaro, V. COVID-19 in multiple sclerosis patients treated with dimethyl fumarate. J. Neurol. 2021, Epub, 1–3. [Google Scholar]
- Mantero, V.; Abate, L.; Basilico, P.; Balgera, R.; Salmaggi, A.; Nourbakhsh, B.; Cordano, C. COVID-19 in dimethyl fumarate-treated patients with multiple sclerosis. J. Neurol. 2020, 268, 2023–2025. [Google Scholar] [CrossRef]
- Giovannoni, G.; Hawkes, C.; Lechner-Scott, J.; Levy, M.; Waubant, E.; Gold, J. The COVID-19 pandemic and the use of MS disease-modifying therapies. Mult. Scler. Relat. Disord. 2020, 39, 102073. [Google Scholar] [CrossRef]
- Barzegar, M.; Mirmosayyeb, O.; Nehzat, N.; Sarrafi, R.; Khorvash, F.; Maghzi, A.-H.; Shaygannejad, V. COVID-19 infection in a patient with multiple sclerosis treated with fingolimod. Neurol. Neuroimmunol. neuroinflammation 2020, 7. [Google Scholar] [CrossRef]
- Valencia-Sanchez, C.; Wingerchuk, D.M. A fine balance: Immunosuppression and immunotherapy in a patient with multiple sclerosis and COVID-19. Mult. Scler. Relat. Disord. 2020, 42, 102182. [Google Scholar] [CrossRef]
- Foerch, C.; Friedauer, L.; Bauer, B.; Wolf, T.; Adam, E.H. Severe COVID-19 infection in a patient with multiple sclerosis treated with fingolimod. Mult. Scler. Relat. Disord. 2020, 42, 102180. [Google Scholar] [CrossRef] [PubMed]
- Chiarini, M.; Paghera, S.; Moratto, D.; Rossi, N.; Giacomelli, M.; Badolato, R.; Capra, R.; Imberti, L. Immunologic characterization of a immunosuppressed multiple sclerosis patient that recovered from SARS-CoV-2 infection. J. Neuroimmunol. 2020, 345, 577282. [Google Scholar] [CrossRef]
- Gomez-Mayordomo, V.; Montero-Escribano, P.; Matías-Guiu, J.A.; González-García, N.; Porta-Etessam, J.; Matías-Guiu, J. Clinical exacerbation of SARS-CoV2 infection after fingolimod withdrawal. J. Med. Virol. 2021, 93, 546–549. [Google Scholar] [CrossRef] [PubMed]
- Mallucci, G.; Zito, A.; Fabbro, B.D.; Bergamaschi, R. Asymptomatic SARS-CoV-2 infection in two patients with multiple sclerosis treated with fingolimod. Mult. Scler. Relat. Disord. 2020, 45, 102414. [Google Scholar] [CrossRef]
- Mohammadpour, M.F.M.; Sahraian, M.A.; Moghadasi, A.N.; Navardi, S. Mild COVID-19 Infection in a Patient with Multiple Sclerosis, while Taking Fingolimod: A Case Report. J. Neurol. Neurosci. 2021, 44, 102314. [Google Scholar]
- Borriello, G.; Ianniello, A. COVID-19 occurring during Natalizumab treatment: A case report in a patient with extended interval dosing approach. Mult. Scler. Relat. Disord. 2020, 41, 102165. [Google Scholar] [CrossRef] [PubMed]
- Aguirre, C.; Meca-Lallana, V.; Barrios-Blandino, A.; Del Río, B.; Vivancos, J. Covid-19 in a patient with multiple sclerosis treated with natalizumab: May the blockade of integrins have a protective role? Mult. Scler. Relat. Disord. 2020, 44, 102250. [Google Scholar] [CrossRef]
- Rimmer, K.; Farber, R.; Thakur, K.; Braverman, G.; Podolsky, D.; Sutherland, L.; Migliore, C.; Ryu, Y.K.; Levin, S.; De Jager, P.L.; et al. Fatal COVID-19 in an MS patient on natalizumab: A case report. Mult. Scler. J. Exp. Transl. Clin. 2020, 6. [Google Scholar] [CrossRef]
- Ghajarzadeh, M.; Mirmosayyeb, O.; Barzegar, M.; Nehzat, N.; Vaheb, S.; Shaygannejad, V.; Maghzi, A.-H. Favorable outcome after COVID-19 infection in a multiple sclerosis patient initiated on ocrelizumab during the pandemic. Mult. Scler. Relat. Disord. 2020, 43, 102222. [Google Scholar] [CrossRef]
- Montero-Escribano, P.; Matías-Guiu, J.; Gómez-Iglesias, P.; Porta-Etessam, J.; Pytel, V.; Matias-Guiu, J.A. Anti-CD20 and COVID-19 in multiple sclerosis and related disorders: A case series of 60 patients from Madrid, Spain. Mult. Scler. Relat. Disord. 2020, 42, 102185. [Google Scholar] [CrossRef] [PubMed]
- Suwanwongse, K.; Shabarek, N. Benign course of COVID-19 in a multiple sclerosis patient treated with Ocrelizumab. Mult. Scler. Relat. Disord. 2020, 42, 102201. [Google Scholar] [CrossRef] [PubMed]
- Novi, G.; Mikulska, M.; Briano, F.; Toscanini, F.; Tazza, F.; Uccelli, A.; Inglese, M. COVID-19 in a MS patient treated with ocrelizumab: Does immunosuppression have a protective role? Mult. Scler. Relat. Disord. 2020, 42, 102120. [Google Scholar] [CrossRef] [PubMed]
- Hughes, R.; Pedotti, R.; Koendgen, H. COVID-19 in persons with multiple sclerosis treated with ocrelizumab—A pharmacovigilance case series. Mult. Scler. Relat. Disord. 2020, 42, 102192. [Google Scholar] [CrossRef] [PubMed]
- Hughes, R.; Whitley, L.; Fitovski, K.; Schneble, H.-M.; Muros, E.; Sauter, A.; Craveiro, L.; Dillon, P.; Bonati, U.; Jessop, N.; et al. COVID-19 in ocrelizumab-treated people with multiple sclerosis. Mult. Scler. Relat. Disord. 2021, 49, 102725. [Google Scholar] [CrossRef]
- Meca-Lallana, V.; Aguirre, C.; Beatrizdel, R.; Cardeñoso, L.; Alarcon, T.; Vivancos, J. COVID-19 in 7 multiple sclerosis patients in treatment with ANTI-CD20 therapies. Mult. Scler. Relat. Disord. 2020, 44, 102306. [Google Scholar] [CrossRef]
- Conte, W.L. Attenuation of antibody response to SARS-CoV-2 in a patient on ocrelizumab with hypogammaglobulinemia. Mult. Scler. Relat. Disord. 2020, 44, 102315. [Google Scholar] [CrossRef]
- Lucchini, M.; Bianco, A.; Del Giacomo, P.; De Fino, C.; Nociti, V.; Mirabella, M. Is serological response to SARS-CoV-2 preserved in MS patients on ocrelizumab treatment? A case report. Mult. Scler. Relat. Disord. 2020, 44, 102323. [Google Scholar] [CrossRef] [PubMed]
- Thornton, J.R.; Harel, A. Negative SARS-CoV-2 antibody testing following COVID-19 infection in Two MS patients treated with ocrelizumab. Mult. Scler. Relat. Disord. 2020, 44, 102341. [Google Scholar] [CrossRef]
- Iannetta, M.; Cesta, N.; Stingone, C.; Malagnino, V.; Teti, E.; Vitale, P.; Simone, G.; Rossi, B.; Ansaldo, L.; Compagno, M.; et al. Mild clinical manifestations of SARS-CoV-2 related pneumonia in two patients with multiple sclerosis under treatment with ocrelizumab. Mult. Scler. Relat. Disord. 2020, 45, 102442. [Google Scholar] [CrossRef] [PubMed]
- Devogelaere, J.; D’Hooghe, M.B.; Vanderhauwaert, F.; D’Haeseleer, M. Coronavirus disease 2019: Favorable outcome in an immunosuppressed patient with multiple sclerosis. Neurol. Sci. 2020, 41, 1981–1983. [Google Scholar] [CrossRef]
- Woo, M.S.; Steins, D.; Häußler, V.; Kohsar, M.; Haag, F.; Elias-Hamp, B.; Heesen, C.; Lütgehetmann, M.; Schulze zur Wiesch, J.; Friese, M.A. Control of SARS-CoV-2 infection in rituximab-treated neuroimmunological patients. J. Neuro. 2021, 268, 5–7. [Google Scholar] [CrossRef] [PubMed]
- Wurm, H.; Attfield, K.; Iversen, A.K.; Gold, R.; Fugger, L.; Haghikia, A. Recovery from COVID-19 in a B-cell-depleted multiple sclerosis patient. Mult. Scler. 2020, 26, 1261–1264. [Google Scholar] [CrossRef]
- Langer-Gould, A.; Smith, J.B.; Li, B.H. Multiple sclerosis, rituximab, and COVID-19. Ann. Clin. Transl. Neurol. 2021, 8, 938–943. [Google Scholar] [CrossRef]
- Bose, G.; Galetta, K. Reactivation of SARS-CoV-2 after Rituximab in a Patient with Multiple Sclerosis. Mult. Scler. Relat. Disord. 2021, 52, 102922. [Google Scholar] [CrossRef]
- Soresina, A.; Moratto, D.; Chiarini, M.; Paolillo, C.; Baresi, G.; Focà, E.; Bezzi, M.; Baronio, M.; Giacomelli, M.; Badolato, R. Two X-linked agammaglobulinemia patients develop pneumonia as COVID-19 manifestation but recover. Pediatric allergy. Immunol. 2020, 31, 565–569. [Google Scholar] [CrossRef] [Green Version]
- Flores-Gonzalez, R.E.; Hernandez, J.; Tornes, L.; Rammohan, K.; Delgado, S. Development of SARS-CoV-2 IgM and IgG antibodies in a relapsing multiple sclerosis patient on ofatumumab. Mult. Scler. Relat. Disord. 2021, 49, 102777. [Google Scholar] [CrossRef]
- Anne, H.; Cross, S.D.; Habek, M.; Davydovskaya, M.; Totolyan, N.; Pingili, R.; Mancione, L.; Sullivan, R.; Zalesak, M.; Su, W.; et al. Characteristics and Outcome of COVID-19 in Patients with Relapsing Multiple Sclerosis Receiving Ofatumumab. Neurology 2021, 96. [Google Scholar]
- Amor, S.; Baker, D.; Khoury, S.J.; Schmierer, K.; Giovanonni, G. SARS-CoV-2 and Multiple Sclerosis: Not All Immune Depleting DMTs are Equal or Bad. Ann. Neurol. 2020, 87, 794–797. [Google Scholar] [CrossRef]
- Carandini, T.; Pietroboni, A.M.; Sacchi, L.; De Riz, M.A.; Pozzato, M.; Arighi, A.; Fumagalli, G.G.; Boneschi, F.M.; Galimberti, D.; Scarpini, E. Alemtuzumab in multiple sclerosis during the COVID-19 pandemic: A mild uncomplicated infection despite intense immunosuppression. Mult. Scler. 2020, 26, 1268–1269. [Google Scholar] [CrossRef]
- Matías-Guiu, J.; Montero-Escribano, P.; Pytel, V.; Porta-Etessam, J.; Matias-Guiu, J.A. Potential COVID-19 infection in patients with severe multiple sclerosis treated with alemtuzumab. Mult. Scler. Relat. Disord. 2020, 44, 102297. [Google Scholar] [CrossRef]
- Guevara, C.; Villa, E.; Cifuentes, M.; Naves, R.; Grazia, J. Mild COVID-19 infection in a patient with multiple sclerosis and severe depletion of T-lymphocyte subsets due to alemtuzumab. Mult. Scler. Relat. Disord. 2020, 44, 102314. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Díaz, E.; Gracia-Gil, J.; García-García, J.G.; Palao, M.; Romero-Sánchez, C.M.; Segura, T. COVID-19 and multiple sclerosis: A description of two cases on alemtuzumab. Mult. Scler. Relat. Disord. 2020, 45, 102402. [Google Scholar] [CrossRef]
- Fiorella, C.; Lorna, G. COVID-19 in a multiple sclerosis (MS) patient treated with alemtuzumab: Insight to the immune response after COVID. Mult. Scler. Relat. Disord. 2020, 46, 102447. [Google Scholar] [CrossRef] [PubMed]
- Iovino, A.; Olivieri, N.; Aruta, F.; Giaquinto, E.; Ruggiero, L.; Spina, E.; Tozza, S.; Manganelli, F.; Iodice, R. Alemtuzumab in Covid era. Mult. Scler. Relat. Disord. 2021, 51, 102908. [Google Scholar] [CrossRef] [PubMed]
- Dersch, R.; Wehrum, T.; Fähndrich, S.; Engelhardt, M.; Rauer, S.; Berger, B. COVID-19 pneumonia in a multiple sclerosis patient with severe lymphopenia due to recent cladribine treatment. Mult. Scler. 2020, 26, 1264–1266. [Google Scholar] [CrossRef] [PubMed]
- De Angelis, M.; Petracca, M.; Lanzillo, R.; Brescia Morra, V.; Moccia, M. Mild or no COVID-19 symptoms in cladribine-treated multiple sclerosis: Two cases and implications for clinical practice. Mult. Scler. Relat. Disord. 2020, 45, 102452. [Google Scholar] [CrossRef]
- Celius, E.G. Normal antibody response after COVID-19 during treatment with cladribine. Mult. Scler. Relat. Disord. 2020, 46, 102476. [Google Scholar] [CrossRef] [PubMed]
- Jack, D.; Nolting, A.; Galazka, A. Favorable outcomes after COVID-19 infection in multiple sclerosis patients treated with cladribine tablets. Mult. Scler. Relat. Disord. 2020, 46, 102469. [Google Scholar] [CrossRef]
- Jack, D.; Damian, D.; Nolting, A.; Galazka, A. COVID-19 in patients with multiple sclerosis treated with cladribine tablets: An update. Mult. Scler. Relat. Disord. 2021, 51, 102929. [Google Scholar] [CrossRef]
- Preziosa, P.; Rocca, M.A.; Nozzolillo, A.; Moiola, L.; Filippi, M. COVID-19 in cladribine-treated relapsing-remitting multiple sclerosis patients: A monocentric experience. J. Neurol. 2020, Epub, 1–3. [Google Scholar]
- Gelibter, S.; Orrico, M.; Filippi, M.; Moiola, L. COVID-19 with no antibody response in a multiple sclerosis patient treated with cladribine: Implication for vaccination program? Mult. Scler. Relat. Disord. 2021, 49, 102775. [Google Scholar] [CrossRef] [PubMed]
- Gheblawi, M.; Wang, K.; Viveiros, A.; Nguyen, Q.; Zhong, J.C.; Turner, A.J.; Raizada, M.K.; Grant, M.B.; Oudit, G.Y. Angiotensin-Converting Enzyme 2: SARS-CoV-2 Receptor and Regulator of the Renin-Angiotensin System: Celebrating the 20th Anniversary of the Discovery of ACE2. Circ. Res. 2020, 126, 1456–1474. [Google Scholar] [CrossRef]
- Corbett, K.S.; Edwards, D.K.; Leist, S.R.; Abiona, O.M.; Boyoglu-Barnum, S.; Gillespie, R.A.; Himansu, S.; Schäfer, A.; Ziwawo, C.T.; DiPiazza, A.T.; et al. SARS-CoV-2 mRNA vaccine design enabled by prototype pathogen preparedness. Nature 2020, 586, 567–571. [Google Scholar] [CrossRef] [PubMed]
- Jeyanathan, M.; Afkhami, S.; Smaill, F.; Miller, M.S.; Lichty, B.D.; Xing, Z. Immunological considerations for COVID-19 vaccine strategies. Nat. Rev. Immunol. 2020, 20, 615–632. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Marc, G.P.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Ramasamy, M.N.; Minassian, A.M.; Ewer, K.J.; Flaxman, A.L.; Folegatti, P.M.; Owens, D.R.; Voysey, M.; Aley, P.K.; Angus, B.; Babbage, G.; et al. Safety and immunogenicity of ChAdOx1 nCoV-19 vaccine administered in a prime-boost regimen in young and old adults (COV002): A single-blind, randomised, controlled, phase 2/3 trial. Lancet 2021, 396, 1979–1993. [Google Scholar] [CrossRef]
- Torjesen, I. Covid-19: First doses of vaccines in Scotland led to a substantial fall in hospital admissions. BMJ 2021, 372, n523. [Google Scholar] [CrossRef]
- Baker, D.; Roberts, C.A.K.; Pryce, G.; Kang, A.S.; Marta, M.; Reyes, S.; Schmierer, K.; Giovannoni, G.; Amor, S. COVID-19 vaccine-readiness for anti-CD20-depleting therapy in autoimmune diseases. Clin. Exp. Immunol. 2020, 202, 149–161. [Google Scholar] [CrossRef] [PubMed]
- Serrazina, F.; Sobral Pinho, A.; Cabral, G.; Salavisa, M.; Correia, A.S. Willingness to be vaccinated against COVID-19: An exploratory online survey in a Portuguese cohort of multiple sclerosis patients. Mult. Scler. Relat. Disord. 2021, 51, 102880. [Google Scholar] [CrossRef]
- Ehde, D.M.; Roberts, M.K.; Herring, T.E.; Alschuler, K.N. Willingness to obtain COVID-19 vaccination in adults with multiple sclerosis in the United States. Mult. Scler. Relat. Disord. 2021, 49, 102788. [Google Scholar] [CrossRef] [PubMed]
- Ciotti, J.R.; Valtcheva, M.V.; Cross, A.H. Effects of MS disease-modifying therapies on responses to vaccinations: A review. Mult. Scler. Relat. Disord. 2020, 45, 102439. [Google Scholar] [CrossRef] [PubMed]
- Achiron, A.; Dolev, M.; Menascu, S.; Zohar, D.-N.; Dreyer-Alster, S.; Miron, S.; Shirbint, E.; Magalashvili, D.; Flechter, S.; Givon, U.; et al. COVID-19 vaccination in patients with multiple sclerosis: What we have learnt by February 2021. Mult. Scler. 2021. [Google Scholar] [CrossRef]
- Olberg, H.K.; Eide, G.E.; Cox, R.J.; Jul-Larsen, Å.; Lartey, S.L.; Vedeler, C.A.; Myhr, K.-M. Antibody response to seasonal influenza vaccination in patients with multiple sclerosis receiving immunomodulatory therapy. Eur. J. Neurol. 2018, 25, 527–534. [Google Scholar] [CrossRef] [Green Version]
- Korsukewitz, C.; Reddel, S.W.; Bar-Or, A.; Wiendl, H. Neurological immunotherapy in the era of COVID-19—Looking for consensus in the literature. Nat. Rev. Neurol. 2020, 16, 493–505. [Google Scholar] [CrossRef]
- Von Hehn, C.; Howard, J.; Liu, S.; Meka, V.; Pultz, J.; Mehta, D.; Prada, C.; Ray, S.; Edwards, M.R.; Sheikh, S.I. Immune response to vaccines is maintained in patients treated with dimethyl fumarate. Neurol. Neuroimmunol. neuroinflammation 2018, 5, e409. [Google Scholar] [CrossRef] [Green Version]
- Bar-Or, A.; Calkwood, J.C.; Chognot, C.; Evershed, J.; Fox, E.J.; Herman, A.; Manfrini, M.; McNamara, J.; Robertson, D.S.; Stokmaier, D.; et al. Effect of ocrelizumab on vaccine responses in patients with multiple sclerosis: The VELOCE study. Neurology 2020, 95, e1999–e2008. [Google Scholar] [CrossRef]
- Buttari, F.; Bruno, A.; Dolcetti, E.; Azzolini, F.; Bellantonio, P.; Centonze, D.; Fantozzi, R. COVID-19 vaccines in multiple sclerosis treated with cladribine or ocrelizumab. Mult. Scler. Relat. Disord. 2021, 52, 102983. [Google Scholar] [CrossRef]
- Khayat-Khoei, M.; Conway, S.; Rubinson, D.A.; Jarolim, P.; Houtchens, M.K. Negative anti-SARS-CoV-2 S antibody response following Pfizer SARS-CoV-2 vaccination in a patient on ocrelizumab. J. Neurol. 2021. [Google Scholar] [CrossRef]
- Chilimuri, S.; Mantri, N.; Gongati, S.; Zahid, M.; Sun, H. COVID-19 Vaccine Failure in a Patient with Multiple Sclerosis on Ocrelizumab. Vaccines 2021, 9, 219. [Google Scholar] [CrossRef]
- Tillett, R.L.; Sevinsky, J.R.; Hartley, P.D.; Kerwin, H.; Crawford, N.; Gorzalski, A.; Laverdure, C.; Verma, S.C.; Rossetto, C.C.; Jackson, D.; et al. Genomic evidence for reinfection with SARS-CoV-2: A case study. Lancet Infect Dis. 2021, 21, 52–58. [Google Scholar] [CrossRef]
- Cook, S.; Vermersch, P.; Comi, G.; Giovannoni, G.; Rammohan, K.; Rieckmann, P.; Sorensen, P.S.; Hamlett, A.; Miret, M.; Weiner, J.; et al. Safety and tolerability of cladribine tablets in multiple sclerosis: The CLARITY (CLAdRIbine Tablets treating multiple sclerosis orallY) study. Mult. Scler. 2011, 17, 578–593. [Google Scholar] [CrossRef] [PubMed]
- Riva, A.; Barcella, V.; Benatti, S.V.; Capobianco, M.; Capra, R.; Cinque, P.; Comi, C.; Fasolo, M.M.; Franzetti, F.; Galli, M.; et al. Vaccinations in patients with multiple sclerosis: A Delphi consensus statement. Mult. Scler. 2021, 27, 347–359. [Google Scholar] [CrossRef] [PubMed]
- Sellner, J.; Rommer, P.S. Multiple Sclerosis and SARS-CoV-2. Vaccination 2021, 9, 99. [Google Scholar]
- Ilya Kister, K.M.; Mulligan, M.J.; Patskovsky, Y.; Voloshyna Ferstler, N.; Zhavtis Ryerson, L.; Curtin, R.; Kim, J.; Tardio, E.; Rimier, Z.; Silverman, G.J. Preliminary results of Ongoing, prospective study of antibody and T-cell responses to SARS-CoV-2 in patients with MS on ocrelizumab and other disease-modifying therapies. In Proceedings of the American Academy of Neurology (AAN) 2021 Annual Meeting Emerging Science Session, Virtual, 18 April 2021. [Google Scholar]
- Reyes, S.; Ramsay, M.; Ladhani, S.; Amirthalingam, G.; Singh, N.; Cores, C.; Mathews, J.; Lambourne, J.; Marta, M.; Turner, B.; et al. Protecting people with multiple sclerosis through vaccination. Pract. Neurol. 2020, 20, 435–445. [Google Scholar] [CrossRef] [PubMed]

| Drug | Impact on Vaccination Response | Recommendation |
|---|---|---|
| Interferons | No impact | Similar to other vaccines |
| Glatiramer acetate | Some studies have suggested a blunted humoral response to Influenza vaccine. No data for other vaccines. | If possible, vaccination must be administered previously to first drug administration |
| Terifluonomide | Possibly no impact | If possible, vaccination must be administered previously to first drug administration |
| Dymethil fumarate | Response to toxoid, conjugate and polysaccharide vaccines was not affected | If possible, vaccination must be administered previously to first drug administration, due to lymphopenia risk |
| S1P modulators 1 | Reduced response to inactivated, toxoid and polysaccharide vaccines with fingolimod Slightly blunted response to Influenza vaccine with Siponimod | If possible, vaccination must be administered previously to first drug administration |
| Cladribine | No specific studies but MS 2 patients under cladribine have mounted immune response to influenza vaccine after four weeks from vaccination, without additional adverse events. COVID-19 vaccine three months after the second cycle of treatment promoted a protective antibody response despite an incomplete immune reconstitution. | A three-month gap after the treatment cycle until vaccination is recommended (or until the recovery of lymphocyte count) |
| Natalizumab | Possibly no impact | If possible, vaccination must be administered previously to first drug administration |
| Anti-CD20 | Attenuated humoral responses to tetanus, seasonal flu, pneumococcus and SARS-CoV-2 vaccines were observed | Ocrelizumab/rituximab: vaccination should be deferred toward the end of the cycle (12 weeks or more after the last drug dose) and the next drug dose administered at least 4–6 weeks after completing vaccination. Ofatumumab: vaccination might be delivered toward the end of the monthly cycle and the next two ofatumumab doses skipped. |
| Alemtuzumab | Blunted immune response until six months after last treatment cycle, but retained after that period | Vaccination should be delayed for at least six months after the last treatment cycle and the second cycle adjusted to ensure an optimal vaccination response. |
| All | - | Live vaccines are generally contraindicated. Pre-vaccination lymphocyte count is advised. Treatment withdrawal to promote vaccination response is not recommended. Post-vaccination serology status checking is encouraged. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cabreira, V.; Abreu, P.; Soares-dos-Reis, R.; Guimarães, J.; Sá, M.J. Multiple Sclerosis, Disease-Modifying Therapies and COVID-19: A Systematic Review on Immune Response and Vaccination Recommendations. Vaccines 2021, 9, 773. https://doi.org/10.3390/vaccines9070773
Cabreira V, Abreu P, Soares-dos-Reis R, Guimarães J, Sá MJ. Multiple Sclerosis, Disease-Modifying Therapies and COVID-19: A Systematic Review on Immune Response and Vaccination Recommendations. Vaccines. 2021; 9(7):773. https://doi.org/10.3390/vaccines9070773
Chicago/Turabian StyleCabreira, Verónica, Pedro Abreu, Ricardo Soares-dos-Reis, Joana Guimarães, and Maria José Sá. 2021. "Multiple Sclerosis, Disease-Modifying Therapies and COVID-19: A Systematic Review on Immune Response and Vaccination Recommendations" Vaccines 9, no. 7: 773. https://doi.org/10.3390/vaccines9070773