
Breastfeeding Prevalence in Austria according to the WHO IYCF Indicators—The SUKIE-Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
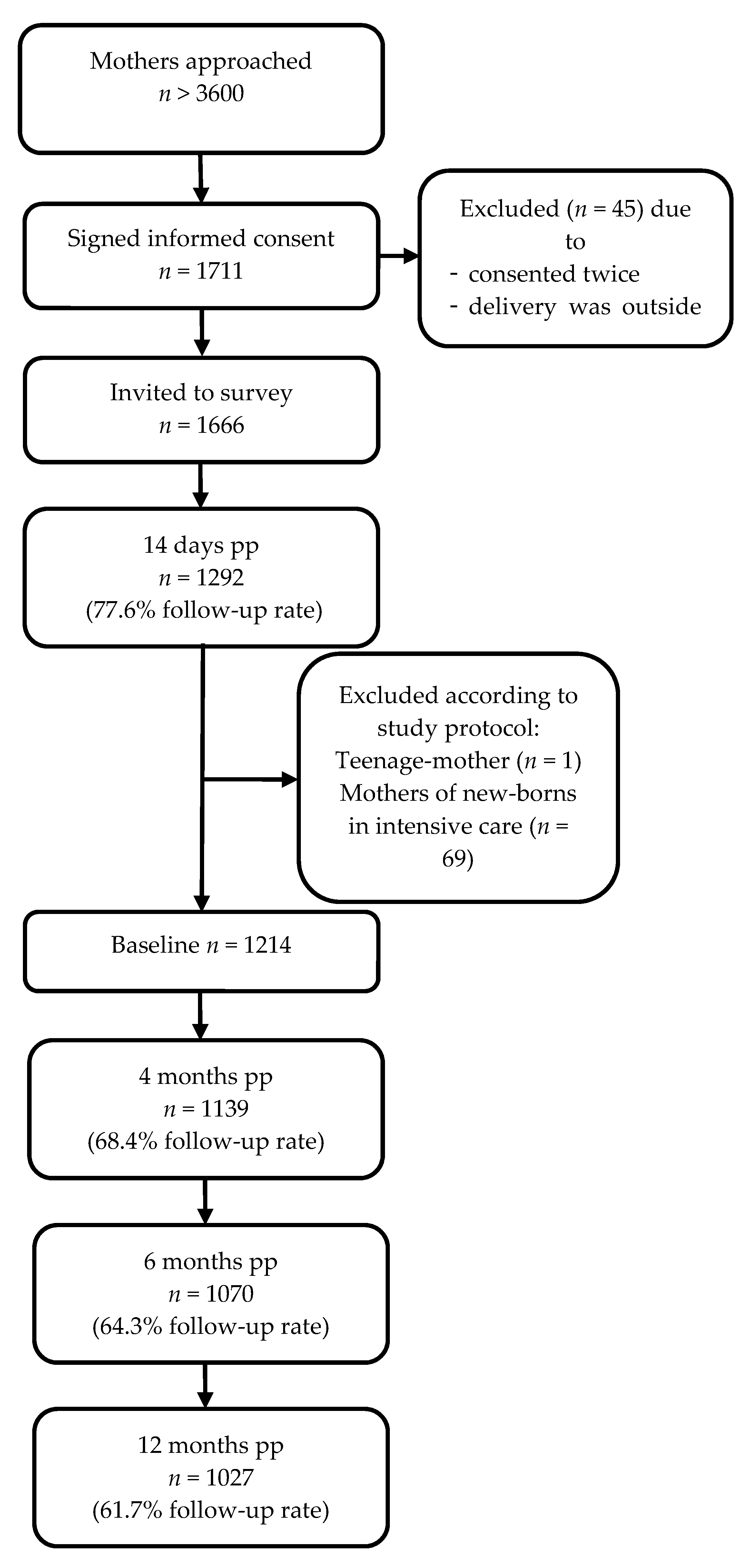
2.2. Subjects and Sample Selection
2.3. Survey and Questionnaire Development
2.4. Outcomes
2.5. Indicators and Definitions Used in the Present Paper
- Indicator 1: Early initiation of breastfeeding describes the proportion of infants who were put within one hour of birth to the breast.
- Indicator 2: Exclusively breastfeeding <six months is defined as the proportion of infants 0–182 days of age who received exclusively breast milk (included expressed breast milk) and if necessary, additional oral rehydration solution, syrups (medicines, vitamins, minerals) or drops.
- Indicator 9: Children ever breastfed as a percentage of infants.
- Indicator 11: Age-appropriate breastfeeding is the proportion of infants 0–182 days of age who are exclusively breastfed and infants 183–438 days who received additionally to breast milk semi-solid, solid or soft foods.
- Indicator 12: Predominant breastfeeding <six months describes the proportion of infants 0–182 days of age who received the predominant source breastmilk but were allowed to receive other liquids such as water or water-based drinks.
- Indicator 13: Duration of breastfeeding as the median duration.
- Indicator 14: Bottle feeding describes the proportion of infants who were fed with a bottle in the first year of life.
2.6. Sample Size Calculation
2.7. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. Breastfeeding Prevalence in the First Year of Life
3.3. IYCF Indicators
4. Discussion
4.1. Breastfeeding Prevalence in Comparisson with Previous Research
4.2. Exclusive Breastfeeding within the First six Months of Age
4.3. Strengths and Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rito, A.I.; Buoncristiano, M.; Spinelli, A.; Salanave, B.; Kunešová, M.; Hejgaard, T.; Solano, M.G.; Fijałkowska, A.; Sturua, L.; Hyska, J. Association between characteristics at birth, breastfeeding and obesity in 22 countries: The WHO European Childhood Obesity Surveillance Initiative–COSI 2015/2017. Obes. Facts 2019, 12, 226–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. World Health Statistics 2018: Monitoring Health for the SDGs Sustainable Development Goals; 9241565586; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Horta, B.L.; Loret de Mola, C.; Victora, C.G. Long-term consequences of breastfeeding on cholesterol, obesity, systolic blood pressure and type 2 diabetes: A systematic review and meta-analysis. Acta Paediatr. 2015, 104, 30–37. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Nutrition Targets 2025: Childhood Overweight Policy Brief; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- WHO. Global Nutrition Targets 2025: Breastfeeding Policy Brief; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Horta, B.; Victora, C. Short-Term Effects of Breastfeeding: A Systematic Review on the Benefits of Breastfeeding on Diarrhoea and Pneumonia; WHO Press: Geneva, Switzerland, 2013. [Google Scholar]
- WHO; UNICEF. Global Breastfeeding Scorecard, 2019: Increasing Commitment to Breastfeeding through Funding and Improved Policies and Programmes; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- WHO. WHO European Region Has Lowest Global Breastfeeding Rates. Available online: https://www.euro.who.int/en/health-topics/Life-stages/maternal-and-newborn-health/news/news/2015/08/who-european-region-has-lowest-global-breastfeeding-rates (accessed on 13 February 2021).
- Chzhen, Y.; Gromada, A.; Rees, G. Are the World’s Richest Countries Family Friendly; United Nations Children’s Fund (UNICEF): Florence, Italy, 2019; p. 22. [Google Scholar]
- Victora, C.G.; Bahl, R.; Barros, A.J.; França, G.V.; Horton, S.; Krasevec, J.; Murch, S.; Sankar, M.J.; Walker, N.; Rollins, N.C. Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. Lancet 2016, 387, 475–490. [Google Scholar] [CrossRef] [Green Version]
- WHO. Guideline: Protecting, Promoting and Supporting Breastfeeding in Facilities Providing Maternity and Newborn Services; 9789241550086; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- European Commission. EU Action Plan on Childhood Obesity 2014–2020; European Commission: Brussels, Belgium, 2014. [Google Scholar]
- BMG. NAP.e Nationaler Aktionsplan Ernährung inkl. Maßnahmenübersicht und Planung 2013; Bundesministerium für Gesundheit: Vienna, Austria, 2013. [Google Scholar]
- Agostoni, C.; Braegger, C.; Decsi, T.; Kolacek, S.; Koletzko, B.; Michaelsen, K.F.; Mihatsch, W.; Moreno, L.A.; Puntis, J.; Shamir, R. Breast-feeding: A commentary by the ESPGHAN Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2009, 49, 112–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rollins, N.C.; Bhandari, N.; Hajeebhoy, N.; Horton, S.; Lutter, C.K.; Martines, J.C.; Piwoz, E.G.; Richter, L.M.; Victora, C.G.; The Lancet Breastfeeding Series Group. Why invest, and what it will take to improve breastfeeding practices? Lancet 2016, 387, 491–504. [Google Scholar] [CrossRef]
- Ritchie, R.; Ortiz-Ospina, M. Measuring Progress towards the Sustainable Development Goals. Available online: https://sdg-tracker.org/zero-hunger (accessed on 30 March 2021).
- BMGFJ. Säuglingsernährung Heute 2006 Struktur- und Beratungsqualität an den Geburtenkliniken in Österreich Ernährung von Säuglingen im ersten Lebensjahr; Bundesministerium für Gesundheit, Familie und Jugend: Vienna, Austria, 2007. [Google Scholar]
- Bagci Bosi, A.T.; Eriksen, K.G.; Sobko, T.; Wijnhoven, T.M.; Breda, J. Breastfeeding practices and policies in WHO European Region Member States. Public Health Nutr. 2016, 19, 753–764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kersting, M.; Hockamp, N.; Burak, C.; Lücke, T. Studie zur Erhebung von Daten zum Stillen und zur Säuglingsernährung in Deutschland—SuSe II; 14. DGE Ernährungsbericht. Vorveröffentlichung Kapitel 3; Deutsche Gesellschaft für Ernährung: Bonn, Germany, 2020. [Google Scholar]
- Gross, K.; Späth, A.; Dratva, J.; Zemp Stutz, E. SWIFS—Swiss Infant Feeding Study Eine Nationale Studie zur Säuglingsernährung und Gesundheit im Ersten Lebensjahr; Bundesamt für Gesundheit (BAG) und Bundesamt für Lebensmittelsicherheit und Veterinärwesen (BLV): Basel, Switzerland, 2014. [Google Scholar]
- Theurich, M.A.; Davanzo, R.; Busck-Rasmussen, M.; Díaz-Gómez, N.M.; Brennan, C.; Kylberg, E.; Bærug, A.; McHugh, L.; Weikert, C.; Abraham, K.; et al. Breastfeeding rates and programs in Europe: A survey of 11 national breastfeeding committees and representatives. J. Pediatr. Gastroenterol. Nutr. 2019, 68, 400–407. [Google Scholar] [CrossRef] [PubMed]
- WHO. Indicators for Assessing Infant and Young Child Feeding Practices Part 1 Definitions; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- WHO. Indicators for Assessing Infant and Young Child Feeding Practices Part 2 Measurement; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- WHO. Indicators for Assessing Breast-Feeding Practices: Report of an Informal Meeting, 11–12 June 1991; World Health Organization: Geneva, Switzerland, 1991. [Google Scholar]
- Kersting, M.; Dulon, M. Assessment of breast-feeding promotion in hospitals and follow-up survey of mother-infant pairs in Germany: The SuSe Study. Public Health Nutr. 2002, 5, 547–552. [Google Scholar] [CrossRef] [PubMed]
- REVAN; Bruckmüller, M.; Hitthaller, A.; Kiefer, I.; Zwiauer, K. Österreichische Beikostempfehlungen; AGES, BMG & HVB: Vienna, Austria, 2010. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Lumley, T. Survey: Analysis of Complex Survey Samples; R Package Version 4.0; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Statistik Austria. Available online: https://www.statistik.at (accessed on 3 February 2021).
- UNICEF. Breastfeeding: A Mother’s Gift, for Every Child; United Nations Children´s Fund (UNICEF): New York, NY, USA, 2018. [Google Scholar]
- UNICEF. Capture the Moment—Early Initiation of Breastfeeding: The Best Start for Every Newborn; UNICEF: New York, NY, USA, 2018. [Google Scholar]
- Hemmingway, A.; Fisher, D.; Berkery, T.; Dempsey, E.; Murray, D.M.; Kiely, M.E. A detailed exploration of early infant milk feeding in a prospective birth cohort study in Ireland: Combination feeding of breast milk and infant formula and early breast-feeding cessation. Br. J. Nutr. 2020, 124, 440–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Comprehensive Implementation Plan on Maternal, Infant and Young Child Nutrition; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Zwiauer, K.; Bichler, I.; Golser, A.; Holubowsky, A.; Kern, A.; Kleyn, M.; Köglberger, S.; Pietschnig, B.; Safar, P.; Salzer, H. Stillempfehlungen der Österreichischen Stillkommission des Obersten Sanitätsrates. Information für Mütter, Väter und alle, die mit jungen Säuglingen und deren Eltern arbeiten. Speculum 2007, 25, 24–28. [Google Scholar]
- Fewtrell, M.; Bronsky, J.; Campoy, C.; Domellof, M.; Embleton, N.; Fidler Mis, N.; Hojsak, I.; Hulst, J.M.; Indrio, F.; Lapillonne, A.; et al. Complementary Feeding: A Position Paper by the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2017, 64, 119–132. [Google Scholar] [CrossRef] [PubMed]
- Zakarija-Grković, I. Exclusive breastfeeding in the hospital: How accurate are the data? J. Hum. Lactation 2012, 28, 139–144. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic of Mothers | Population in Austria (%) | n | Sample 14 days (%) | n | Sample 4 mos. (%) | n | Sample 6 mos. (%) | n | Sample 12 mos. (%) | n |
|---|---|---|---|---|---|---|---|---|---|---|
| Age at delivery (year) | ||||||||||
| 18–24 | 10.8 * | 9171 | 7.7 | 93 | 7.0 | 72 | 6.0 | 58 | 5.0 | 47 |
| 25–29 | 29.0 | 24,621 | 26.8 | 325 | 25.8 | 265 | 26.0 | 253 | 26.1 | 246 |
| 30–34 | 34.8 | 29,550 | 38.9 | 472 | 39.9 | 409 | 40.4 | 394 | 40.6 | 383 |
| 35–39 | 19.7 | 16,770 | 21.1 | 256 | 21.8 | 224 | 21.9 | 213 | 22.6 | 213 |
| ≥40 | 4.4 | 3731 | 5.5 | 68 | 5.5 | 56 | 5.7 | 56 | 5.7 | 54 |
| Educational level | ||||||||||
| Low (ISCED 0–2) | 10.1 ** | 8229 | 4.0 | 49 | 2.6 | 27 | 2.0 | 19 | 2.2 | 21 |
| Middle (ISCED 3–4) | 47.1 ** | 38,474 | 52.0 | 631 | 51.7 | 530 | 50.7 | 494 | 49.5 | 467 |
| High (ISCED 5–8) | 13.1 ** | 10,722 | 44.0 | 534 | 45.7 | 469 | 47.3 | 461 | 48.3 | 455 |
| State/Residence | ||||||||||
| Vienna | 23.5 | 19,935 | 23.3 | 283 | 19.8 | 203 | 19.4 | 189 | 18.7 | 176 |
| Vorarlberg | 5.1 | 4319 | 4.7 | 57 | 4.7 | 48 | 4.7 | 46 | 5.0 | 47 |
| Tyrol | 8.9 | 7522 | 7.9 | 96 | 8.0 | 82 | 8.4 | 82 | 8.4 | 79 |
| Styria | 12.9 | 10,970 | 14.7 | 179 | 14.9 | 153 | 15.0 | 146 | 14.9 | 141 |
| Salzburg | 6.8 | 5780 | 7.3 | 89 | 7.5 | 77 | 7.5 | 73 | 7.4 | 70 |
| Upper Austria | 17.7 | 15,057 | 16.1 | 196 | 17.1 | 175 | 17.2 | 167 | 17.7 | 167 |
| Lower Austria | 17.2 | 14,652 | 17.8 | 216 | 19.3 | 198 | 19.7 | 192 | 19.5 | 184 |
| Carintia | 5.3 | 4485 | 5.0 | 61 | 5.8 | 60 | 5.3 | 52 | 5.6 | 53 |
| Burgenland | 2.6 | 2232 | 3.0 | 37 | 2.9 | 30 | 2.8 | 27 | 2.8 | 26 |
| According to WHO Definitions * | According to Austrian Recommendations ** | |||
|---|---|---|---|---|
| % | 95% CI | % | 95% CI | |
| Early initiation of breastfeeding (<1 h) (Ind. 1) | 68.2 | 66.1; 71.3 | 68.2 | 66.1; 71.3 |
| Exclusive breastfeeding (Ind. 2) | 1.9 | 1.2; 2.5 | 30.5 | 28.2; 33.4 |
| Children ever breastfed (Ind. 9) | 97.5 | 96.4; 98.5 | 97.5 | 96.4; 98.5 |
| Age-appropriate breastfeeding (Ind. 11) | 1.7 | 1.1; 2.4 | 29.4 | 26.8; 32.1 |
| Predominant breastfeeding (Ind. 12) | 1.8 | 1.2; 2.5 | 3.7 | 2.6; 4.9 |
| Bottle feeding (Ind. 14) | 81.9 | 79.5; 84.2 | 81.9 | 79.5; 84.2 |
| Age in Weeks | Min | Q1 | Median | Mean | Q3 | Max |
|---|---|---|---|---|---|---|
| Introduction infant formula | 0 | 0 | 0 | 7 | 7 | 55 |
| Introduction water and/or tea | 0 | 2 | 22 | 22 | 26 | 60 |
| Introduction complementary food | 9 | 17 | 22 | 21 | 24 | 56 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bürger, B.; Schindler, K.; Tripolt, T.; Stüger, H.P.; Wagner, K.-H.; Weber, A.; Wolf-Spitzer, A. Breastfeeding Prevalence in Austria according to the WHO IYCF Indicators—The SUKIE-Study. Nutrients 2021, 13, 2096. https://doi.org/10.3390/nu13062096
Bürger B, Schindler K, Tripolt T, Stüger HP, Wagner K-H, Weber A, Wolf-Spitzer A. Breastfeeding Prevalence in Austria according to the WHO IYCF Indicators—The SUKIE-Study. Nutrients. 2021; 13(6):2096. https://doi.org/10.3390/nu13062096
Chicago/Turabian StyleBürger, Bernadette, Karin Schindler, Tanja Tripolt, Hans Peter Stüger, Karl-Heinz Wagner, Adelheid Weber, and Alexandra Wolf-Spitzer. 2021. "Breastfeeding Prevalence in Austria according to the WHO IYCF Indicators—The SUKIE-Study" Nutrients 13, no. 6: 2096. https://doi.org/10.3390/nu13062096