Low 25-Hydroxyvitamin D Levels on Admission to the Intensive Care Unit May Predispose COVID-19 Pneumonia Patients to a Higher 28-Day Mortality Risk: A Pilot Study on a Greek ICU Cohort

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
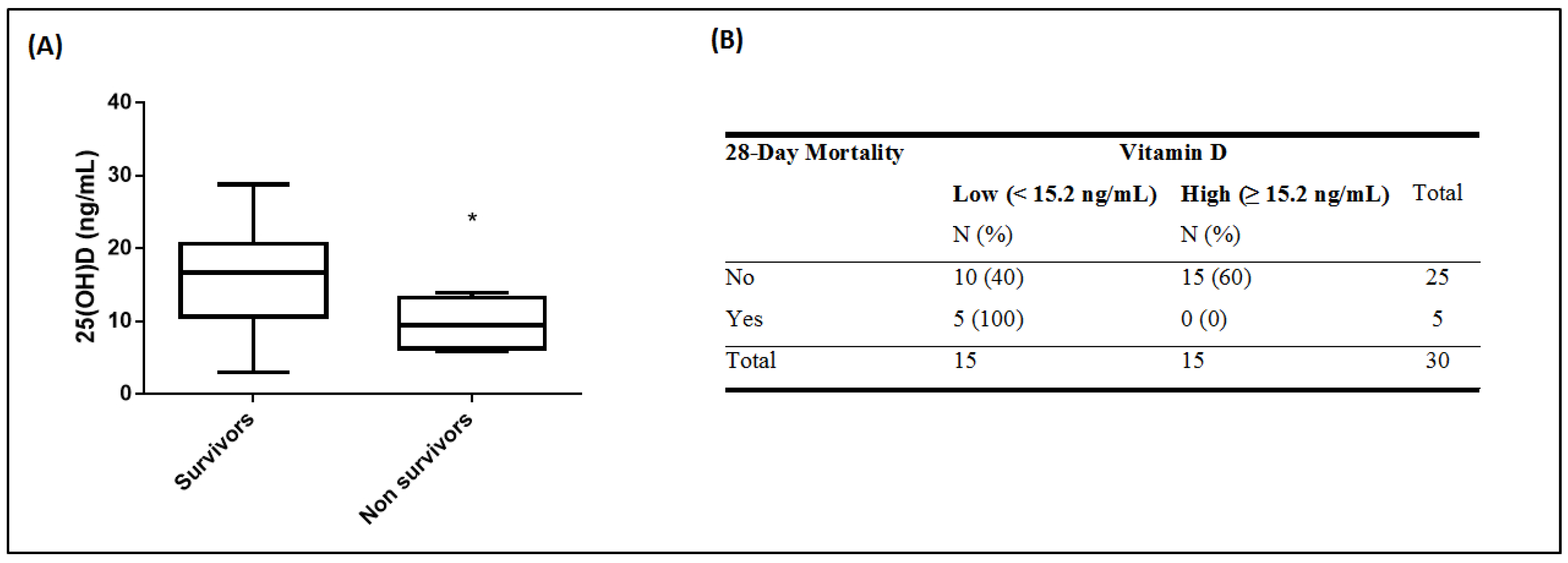
3. Results
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Moromizato, T.; Litonjua, A.A.; Braun, A.B.; Gibbons, F.K.; Giovannucci, E.; Christopher, K.B. Association of low serum 25-hydroxyvitamin D levels and sepsis in the critically ill. Crit. Care Med. 2014, 42, 97–107. [Google Scholar] [CrossRef]
- Liu, P.T.; Stenger, S.; Li, H.; Wenzel, L.; Tan, B.H.; Krutzik, S.R.; Ochoa, M.T.; Schauber, J.; Wu, K.; Meinken, C.; et al. Toll-like receptor triggering of a vitamin D-mediated human antimicrobial response. Science 2006, 311, 1770–1773. [Google Scholar] [CrossRef]
- Liu, P.T.; Stenger, S.; Tang, D.H.; Modlin, R.L. Cutting edge: Vitamin D-mediated human antimicrobial activity against Mycobacterium tuberculosis is dependent on the induction of cathelicidin. J. Immunol. 2007, 179, 2060–2063. [Google Scholar] [CrossRef] [Green Version]
- Wang, T.T.; Nestel, F.P.; Bourdeau, V.; Nagai, Y.; Wang, Q.; Liao, J.; Tavera-Mendoza, L.; Lin, R.; Hanrahan, J.W.; Mader, S.; et al. Cutting edge: 1,25-dihydroxyvitamin D3 is a direct inducer of antimicrobial peptide gene expression. J. Immunol. 2004, 173, 2909–2912. [Google Scholar] [CrossRef] [Green Version]
- Weir, E.K.; Thenappan, T.; Bhargava, M.; Chen, Y. Does vitamin D deficiency increase the severity of COVID-19? Clin. Med. 2020, 20, e107–e108. [Google Scholar] [CrossRef]
- Wang, R.; DeGruttola, V.; Lei, Q.; Mayer, K.H.; Redline, S.; Hazra, A.; Mora, S.; Willett, W.C.; Ganmaa, D.; Manson, J.E. The vitamin D for COVID-19 (VIVID) trial: A pragmatic cluster-randomized design. Contemp. Clin. Trials 2020, 106176. [Google Scholar] [CrossRef]
- Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute respiratory distress syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [CrossRef]
- Ross, A.C.; Manson, J.E.; Abrams, S.A.; Aloia, J.F.; Brannon, P.M.; Clinton, S.K.; Durazo-Arvizu, R.A.; Gallagher, J.C.; Gallo, R.L.; Jones, G.; et al. The 2011 report on dietary reference intakes for calcium and vitamin D from the Institute of Medicine: What clinicians need to know. J. Clin. Endocrinol. Metab. 2011, 96, 53–58. [Google Scholar] [CrossRef]
- Arvinte, C.; Singh, M.; Marik, P.E. Serum levels of vitamin C and vitamin D in a cohort of critically ill COVID-19 patients of a north American community hospital intensive care unit in may 2020. A pilot study. Med. Drug Discov. 2020, 8, 100064. [Google Scholar] [CrossRef]
- Carpagnano, G.E.; Di Lecce, V.; Quaranta, V.N.; Zito, A.; Buonamico, E.; Capozza, E.; Palumbo, A.; Di Gioia, G.; Valerio, V.N.; Resta, O. Vitamin D deficiency as a predictor of poor prognosis in patients with acute respiratory failure due to COVID-19. J. Endocrinol. Investig. 2020, 1–7. [Google Scholar] [CrossRef]
- Jain, A.; Chaurasia, R.; Sengar, N.S.; Singh, M.; Mahor, S.; Narain, S. Analysis of vitamin D level among asymptomatic and critically ill COVID-19 patients and its correlation with inflammatory markers. Sci. Rep. 2020, 10, 20191. [Google Scholar] [CrossRef]
- Radujkovic, A.; Hippchen, T.; Tiwari-Heckler, S.; Dreher, S.; Boxberger, M.; Merle, U. Vitamin D Deficiency and Outcome of COVID-19 Patients. Nutrients 2020, 12, 2757. [Google Scholar] [CrossRef]
- Munshi, R.; Hussein, M.H.; Toraih, E.A.; Elshazli, R.M.; Jardak, C.; Sultana, N.; Youssef, M.R.; Omar, M.; Attia, A.S.; Fawzy, M.S.; et al. Vitamin D insufficiency as a potential culprit in critical COVID-19 patients. J. Med Virol. 2020. [Google Scholar] [CrossRef]
- Mardani, R.; Alamdary, A.; Mousavi Nasab, S.D.; Gholami, R.; Ahmadi, N.; Gholami, A. Association of vitamin D with the modulation of the disease severity in COVID-19. Virus Res. 2020, 289, 198148. [Google Scholar] [CrossRef] [PubMed]
- Panagiotou, G.; Tee, S.A.; Ihsan, Y.; Athar, W.; Marchitelli, G.; Kelly, D.; Boot, C.S.; Stock, N.; Macfarlane, J.; Martineau, A.R.; et al. Low serum 25-hydroxyvitamin D (25[OH]D) levels in patients hospitalized with COVID-19 are associated with greater disease severity. Clin. Endocrinol. 2020. [Google Scholar] [CrossRef]
- Benskin, L.L. A Basic Review of the Preliminary Evidence That COVID-19 Risk and Severity is Increased in Vitamin D Deficiency. Front. Public Health 2020, 8, 513. [Google Scholar] [CrossRef]
- Maghbooli, Z.; Sahraian, M.A.; Ebrahimi, M.; Pazoki, M.; Kafan, S.; Tabriz, H.M.; Hadadi, A.; Montazeri, M.; Nasiri, M.; Shirvani, A.; et al. Vitamin D sufficiency, a serum 25-hydroxyvitamin D at least 30 ng/mL reduced risk for adverse clinical outcomes in patients with COVID-19 infection. PLoS ONE 2020, 15, e0239799. [Google Scholar] [CrossRef]
- Hosack, T.; Baktash, V.; Mandal, A.K.J.; Missouris, C.G. Prognostic implications of vitamin D in patients with COVID-19. Eur. J. Nutr. 2020, 1–2. [Google Scholar] [CrossRef]
- Annweiler, C.; Hanotte, B.; Grandin de l’Eprevier, C.; Sabatier, J.M.; Lafaie, L.; Célarier, T. Vitamin D and survival in COVID-19 patients: A quasi-experimental study. J. Steroid Biochem. Mol. Biol. 2020, 204, 105771. [Google Scholar] [CrossRef]
- Annweiler, G.; Corvaisier, M.; Gautier, J.; Dubée, V.; Legrand, E.; Sacco, G.; Annweiler, C. Vitamin D Supplementation Associated to Better Survival in Hospitalized Frail Elderly COVID-19 Patients: The GERIA-COVID Quasi-Experimental Study. Nutrients 2020, 12, 3377. [Google Scholar] [CrossRef]
- Merzon, E.; Tworowski, D.; Gorohovski, A.; Vinker, S.; Golan Cohen, A.; Green, I.; Frenkel-Morgenstern, M. Low plasma 25(OH) vitamin D level is associated with increased risk of COVID-19 infection: An Israeli population-based study. FEBS J. 2020, 287, 3693–3702. [Google Scholar] [CrossRef] [PubMed]
- D’Avolio, A.; Avataneo, V.; Manca, A.; Cusato, J.; De Nicolò, A.; Lucchini, R.; Keller, F.; Cantù, M. 25-Hydroxyvitamin D Concentrations Are Lower in Patients with Positive PCR for SARS-CoV-2. Nutrients 2020, 12, 1359. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Parameters | All Patients |
|---|---|
| Number of patients, N (%) | 30 |
| Age (years), (mean ± SD) | 65 ± 11 |
| Sex, N (%) | |
| Male | 24 (80) |
| Female | 6 (20) |
| Sick days prior to ICU admission | 6 ± 2 |
| Comorbidities | 23 (77) |
| Hypertension | 15 |
| Hyperlipidaemia | 9 |
| Diabetes | 5 |
| CAD | 4 |
| COPD | 1 |
| Asthma | 1 |
| Smoking | 3 (10) |
| ARDS | 27 (90) |
| Mild (200–300 mmHg) | 11 |
| Moderate (100–200 mmHg) | 14 |
| Severe (<100 mmHg) | 2 |
| PaO2/FiO2 (mmHg), (median, IQR) | 189 (125–260) |
| APACHE II, (mean ± SD) | 14 ± 5 |
| SOFA, (mean ± SD) | 7 ± 3 |
| Temperature (°C), (mean ± SD) | 37.5 ± 1.1 |
| Heart rate (bpm), (median, IQR) | 86 (80–104) |
| Mean arterial pressure (mmHg), (mean ± SD) | 83 ± 15 |
| Respiratory rate (breaths/min), (mean ± SD) | 23 ± 4 |
| White blood cell count (cells/µL), (mean ± SD) | 10,000 ± 5000 |
| Neutrophil count (cells/µL), (mean ± SD) | 8000 ± 5000 |
| Platelets (cells/µL), (median, IQR) | 220,000 (180,000–280,000) |
| 25(OH)D (ng/mL), (median, IQR) | 15.2 (9.6–19.1) |
| CRP (mg/dL), (median, IQR) | 12 (5–20) |
| Lactate (mmol/L), (mean ± SD) | 1.3 ± 0.5 |
| LDH (U/L), (median, IQR) | 440 (350–630) |
| Albumin (g/dL), (mean ± SD) | 3.4 ± 0.6 |
| Globulin (g/dL), (mean ± SD) | 2.8 ± 0.5 |
| INR, (median, IQR) | 1.1 (1.02–1.12) |
| Fibrinogen (mg/dL), (mean ± SD) | 610 ± 170 |
| CK (IU/L), (median, IQR) | 150 (70–370) |
| CKMB (U/L), (median, IQR) | 24 (17–37) |
| High-sensitive troponin T (ng/mL), | |
| (median, IQR) | 20 (10–60) |
| Creatinine (mg/mL), (mean ± SD) | 1 ± 0.3 |
| Urea (mg/dL), (median, IQR) | 45 (27–56) |
| Glucose (mg/dL), (median, IQR) | 140 (110–190) |
| Total Bilirubin (mg/dL), | |
| (median, IQR) | 0.6 (0.4–1.0) |
| ALT (IU/L), (median, IQR) | 40 (20–60) |
| AST (IU/L), (median, IQR) | 40 (36–62) |
| ALP (U/L), (median, IQR) | 65 (46–88) |
| Amylase (U/L), (median, IQR) | 66 (47–114) |
| γ-GT (IU/L), (media, IQR) | 55 (22–78) |
| Outcomes | |
| ICU stay (days), (median, IQR) | 19 (13–40) |
| 28-Day Mortality | 5 (17) |
| Mechanical ventilation, N (%) | 23 (77) |
| Anti-COVID-19 therapy | 30 (100) |
| Azithromycin/chloroquine/lopinavir/ritonavir | 12 |
| Azithromycin/chloroquine | 9 |
| Lopinavir/ritonavir/chloroquine | 4 |
| Chloroquine | 2 |
| Convalescent Plasma | 2 |
| Other | 1 |
| Parameters | Vitamin D | p-Value | |
|---|---|---|---|
| Low | High | ||
| <15.2 ng/mL | ≥15.2 ng/mL | ||
| Number of patients, N (%) | 15 (50) | 15 (50) | |
| Age (years), (mean ± SD) | 67 ± 13 | 63 ± 9 | 0.3 |
| Body mass index (kg/m2), (mean ± SD) | 26.4 ± 1.9 | 27.6 ± 1.9 | 0.1 |
| Sex, N (%) | 0.4 | ||
| Male | 11 (73) | 13 (87) | |
| Female | 4 (27) | 2 (13) | |
| Days sick prior to admission | 6 ± 3 | 6 ± 2 | 0.7 |
| Characteristics on ICU admission | |||
| Comorbidities | 11 (73) | 12 (80) | 0.7 |
| ARDS | 14 (93) | 13 (87) | 0.5 |
| Mild (200–300 mmHg) | 4 | 7 | |
| Moderate (100–200 mmHg) | 9 | 5 | |
| Severe (<100 mmHg) | 1 | 1 | |
| PaO2/FiO2 (mmHg), (mean ± SD) | 180 ± 70 | 210 ± 110 | 0.4 |
| APACHE II score, (mean ± SD) | 14 ± 5 | 15 ± 5 | 0.8 |
| SOFA score, (mean ± SD) | 7 ± 3 | 7 ± 3 | 0.5 |
| Temperature (°C), (mean ± SD) | 37.6 ± 1.0 | 37.4 ± 1.1 | 0.6 |
| Heart rate (bpm), (median, IQR) | 85 (78–105) | 88 (82–100) | 0.4 |
| Mean arterial pressure (mmHg), (mean ± SD) | 85 ± 19 | 82 ± 11 | 0.6 |
| Respiratory rate (breaths/min), | |||
| (mean ± SD) | 24 ± 5 | 22 ± 3 | 0.2 |
| White blood cell count (cells/µL), (mean ± SD) | 11,000 ± 5000 | 10,000 ± 5000 | 0.3 |
| Neutrophils (cells/µL), (median, IQR) | 7000 (5000–14,000) | 5000 (3000–7000) | 0.2 |
| Platelets (cells/µL), (median, IQR) | 220,000 (190,000–370,000) | 220,000 (140,000–250,000) | 0.2 |
| CRP (mg/dL), (median, IQR) | 19 (5–26) | 10 (4–17) | 0.06 |
| Lactate (mmol/L), (mean ± SD) | 1.3 ± 0.5 | 1.2 ± 0.6 | 0.7 |
| LDH (U/L), (median, IQR) | 470 (400–640) | 420 (340–530) | 0.9 |
| Albumin (g/dL), (mean ± SD) | 3.3 ± 0.6 | 3.5 ± 0.5 | 0.2 |
| Globulin (g/dL), (mean ± SD) | 2.9 ± 0.5 | 2.7 ± 0.5 | 0.2 |
| INR, (median, IQR) | 1.11 (1.05–1.30) | 1.05 (1.00–1.10) | 0.1 |
| Fibrinogen (mg/dL), (mean ± SD) | 660 ± 190 | 570 ± 140 | 0.2 |
| CK (IU/L), (median, IQR) | 200 (70–300) | 120 (80–510) | 0.2 |
| CKMB (U/L), (median, IQR) | 23 (18–42) | 29 (17–37) | 0.3 |
| High-sensitive troponin T (ng/mL), (median, IQR) | |||
| 39 (14–125) | 14 (10–27) | 0.1 | |
| Creatinine (mg/mL), (mean ± SD) | 1.2 ± 0.4 | 0.9 ± 0.3 | 0.1 |
| Urea (mg/dL), (median, IQR) | 48 (25–63) | 31 (27–56) | 0.4 |
| Glucose (mg/dL), (median, IQR) | 130 (117–182) | 170 (109–196) | 0.7 |
| Total Bilirubin (mg/dL), | |||
| (median, IQR) | 0.7 (0.5–0.9) | 0.6 (0.4–1.0) | 0.9 |
| ALT (IU/L), (median, IQR) | 44 (20–70) | 38 (23–49) | 0.3 |
| AST (IU/L), (median, IQR) | 46 (33–63) | 41 (37–61) | 0.5 |
| ALP (U/L), (median, IQR) | 68 (50–80) | 55 (41–117) | 0.9 |
| Amylase (U/L), (median, IQR) | 64 (40–93) | 75 (55–132) | 0.8 |
| γ-GT (IU/L), (media, IQR) | 43 (20–70) | 60 (24–89) | 0.9 |
| Outcomes | |||
| 28-Day ICU mortality, N (%) | 0.01 * | ||
| No | 10 (67) | 15 (100) | |
| Yes | 5 (33) | 0 (0) | |
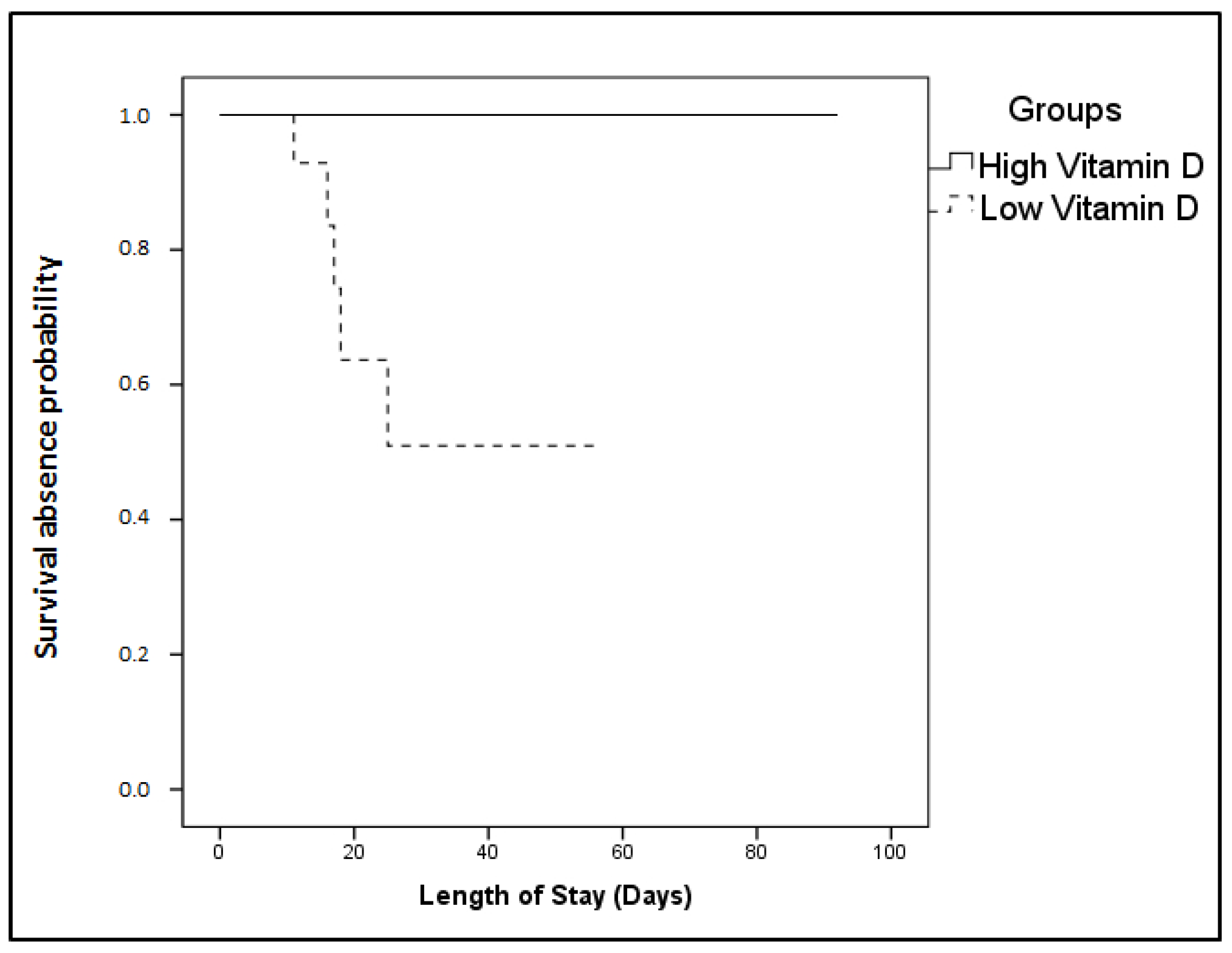
| Day of ICU death (days), (mean ± SD) | 20 ± 7 | 44 ± 7 | 0.001 * |
| ICU stay (days), (median, IQR) | 17 (13–30) | 35 (11–54) | 0.1 |
| Mechanical ventilation, N (%) | 11 (73) | 12 (80) | 0.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vassiliou, A.G.; Jahaj, E.; Pratikaki, M.; Orfanos, S.E.; Dimopoulou, I.; Kotanidou, A. Low 25-Hydroxyvitamin D Levels on Admission to the Intensive Care Unit May Predispose COVID-19 Pneumonia Patients to a Higher 28-Day Mortality Risk: A Pilot Study on a Greek ICU Cohort. Nutrients 2020, 12, 3773. https://doi.org/10.3390/nu12123773
Vassiliou AG, Jahaj E, Pratikaki M, Orfanos SE, Dimopoulou I, Kotanidou A. Low 25-Hydroxyvitamin D Levels on Admission to the Intensive Care Unit May Predispose COVID-19 Pneumonia Patients to a Higher 28-Day Mortality Risk: A Pilot Study on a Greek ICU Cohort. Nutrients. 2020; 12(12):3773. https://doi.org/10.3390/nu12123773
Chicago/Turabian StyleVassiliou, Alice G., Edison Jahaj, Maria Pratikaki, Stylianos E. Orfanos, Ioanna Dimopoulou, and Anastasia Kotanidou. 2020. "Low 25-Hydroxyvitamin D Levels on Admission to the Intensive Care Unit May Predispose COVID-19 Pneumonia Patients to a Higher 28-Day Mortality Risk: A Pilot Study on a Greek ICU Cohort" Nutrients 12, no. 12: 3773. https://doi.org/10.3390/nu12123773