
Use of Biological Treatments in Elderly Patients with Skin Psoriasis in the Real World


Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Patient Characteristics
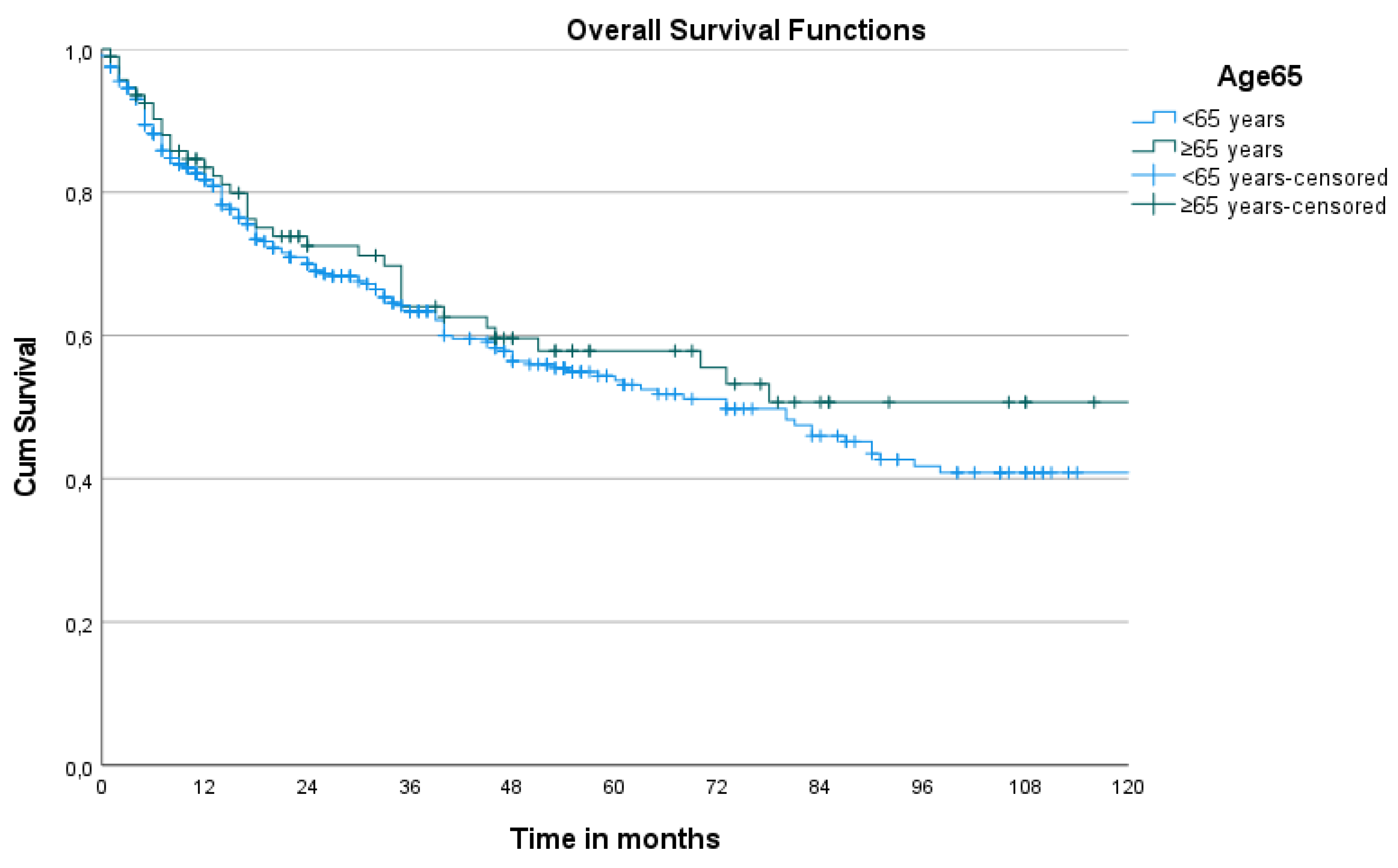
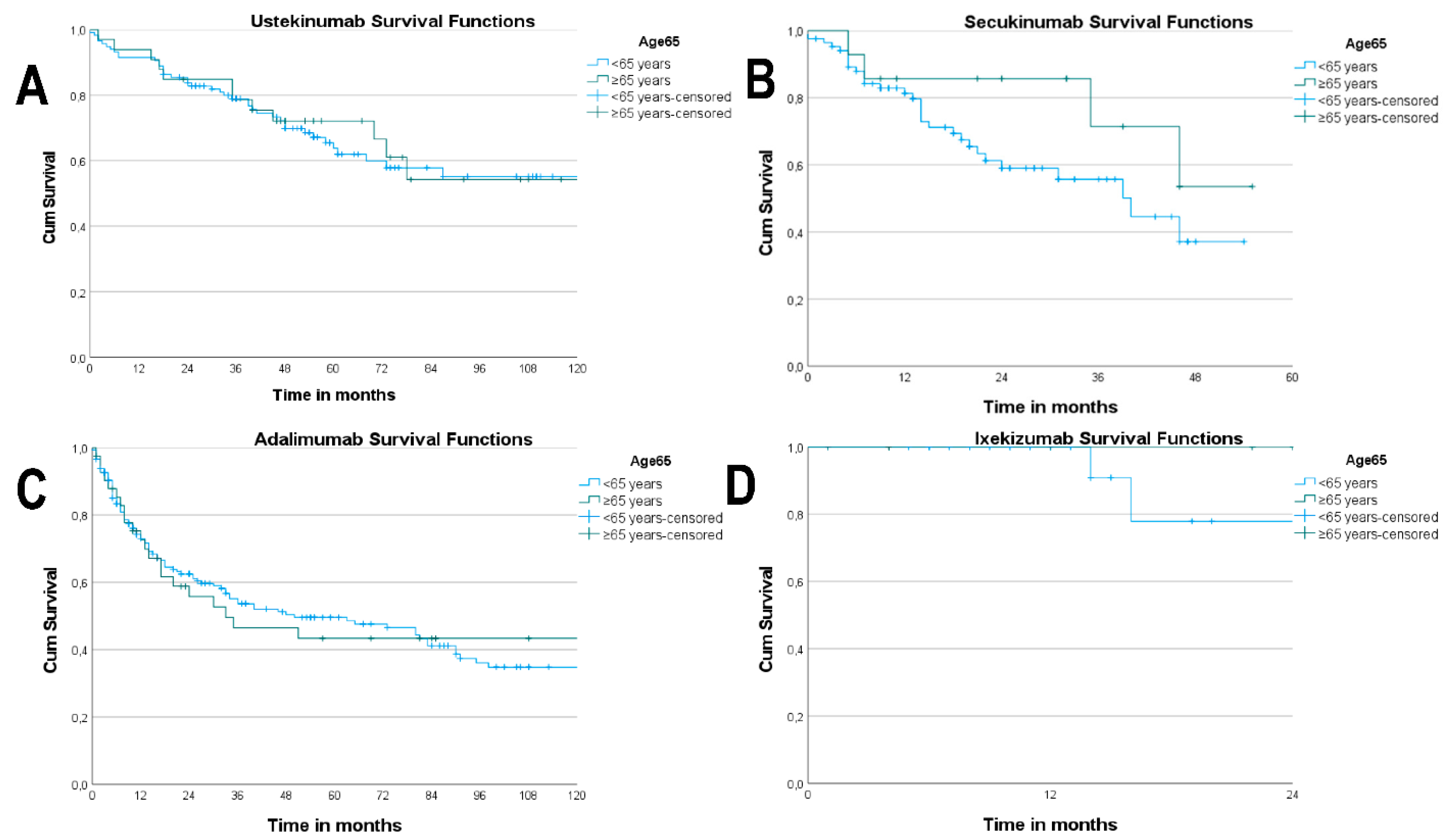
3.2. Drug Survival
3.3. Multivariate Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- OMIM Clinical Synopsis—#177900—PSORIASIS 1, SUSCEPTIBILITY TO; PSORS1. Available online: https://www.omim.org/entry/177900 (accessed on 1 October 2021).
- Griffiths, C.E.; Barker, J.N. Pathogenesis and clinical features of psoriasis. Lancet 2007, 370, 263–271. [Google Scholar] [CrossRef]
- Boehncke, W.-H.; Schön, M.P. Psoriasis. Lancet 2015, 386, 983–994. [Google Scholar] [CrossRef]
- Phan, C.; Sigal, M.-L.; Estève, E.; Reguiai, Z.; Barthélémy, H.; Beneton, N.; Maccari, F.; Lahfa, M.; Thomas-Beaulieu, D.; Le Guyadec, T.; et al. Psoriasis in the elderly: Epidemiological and clinical aspects, and evaluation of patients with very late onset psoriasis. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 78–82. [Google Scholar] [CrossRef]
- Kim, W.B.; Jerome, D.; Yeung, J. Diagnosis and management of psoriasis. Can. Fam. Physician 2017, 63, 278–285. [Google Scholar]
- Scher, J.U.; Ogdie, A.; Merola, J.F.; Ritchlin, C. Preventing psoriatic arthritis: Focusing on patients with psoriasis at increased risk of transition. Nat. Rev. Rheumatol. 2019, 15, 153–166. [Google Scholar] [CrossRef] [PubMed]
- Yamazaki, F. Psoriasis: Comorbidities. J. Dermatol. 2021, 48, 732–740. [Google Scholar] [CrossRef]
- Semenov, Y.R.; Herbosa, C.M.; Rogers, A.T.; Huang, A.; Kwatra, S.G.; Cohen, B.; Anadkat, M.J.; Silverberg, J.I. Psoriasis and mortality in the United States: Data from the National Health and Nutrition Examination Survey. J. Am. Acad. Dermatol. 2021, 85, 396–403. [Google Scholar] [CrossRef] [PubMed]
- Hajiebrahimi, M.; Song, C.; Hägg, D.; Andersson, T.M.-L.; Villacorta, R.; Linder, M. The Occurrence of Metabolic Risk Factors Stratified by Psoriasis Severity: A Swedish Population-Based Matched Cohort Study. Clin. Epidemiol. 2020, 12, 737–744. [Google Scholar] [CrossRef]
- Mehrmal, S.; Uppal, P.; Nedley, N.; Giesey, R.L.; Delost, G.R. The global, regional, and national burden of psoriasis in 195 countries and territories, 1990 to 2017: A systematic analysis from the Global Burden of Disease Study 2017. J. Am. Acad. Dermatol. 2021, 84, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, A.B.; Dann, F. Comorbidities in Patients with Psoriasis. Am. J. Med. 2009, 122, 1150.e1–1150.e9. [Google Scholar] [CrossRef] [PubMed]
- Takeshita, J.; Grewal, S.; Langan, S.M.; Mehta, N.N.; Ogdie, A.; Van Voorhees, A.S.; Gelfand, J.M. Psoriasis and comorbid diseases: Epidemiology. J. Am. Acad. Dermatol. 2017, 76, 377–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karmacharya, P.; Chakradhar, R.; Ogdie, A. The epidemiology of psoriatic arthritis: A literature review. Best Pract. Res. Clin. Rheumatol. 2021, 35, 101692. [Google Scholar] [CrossRef]
- Gladman, D.D. Psoriatic arthritis. Dermatol. Ther. 2004, 17, 350–363. [Google Scholar] [CrossRef] [PubMed]
- Mourad, A.; Straube, S.; Armijo-Olivo, S.; Gniadecki, R. Factors predicting persistence of biologic drugs in psoriasis: A systematic review and meta-analysis. Br. J. Dermatol. 2019, 181, 450–458. [Google Scholar] [CrossRef]
- Santos-Juanes, J.; Galache, C.; Coto-Segura, P.; Rodrigo, L. The Actual State of Psoriasis Therapies. In Psoriasis·Monograph; 2016; ISBN 978-1-944685-71-3. Available online: www.smgebooks.com (accessed on 1 October 2021).
- Puig, L.; Carrascosa, J.M.; Carretero, G.; de la Cueva, P.; Lafuente-Urrez, R.F.; Belinchón, I.; Sánchez-Regaña, M.; García-Bustínduy, M.; Ribera, M.; Alsina, M.; et al. Spanish Evidence-Based Guidelines on the Treatment of Psoriasis With Biologic Agents, 2013. Part 1: On Efficacy and Choice of Treatment. Actas Dermo-Sifiliográficas 2013, 104, 694–709. [Google Scholar] [CrossRef]
- World Health Organization. Proposed Working Definition of an Older Person in Africa for the MDS Project; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Shary, N.; Kalb, R.E. Optimizing the Treatment of Moderate-to-Severe Psoriasis in Older Adults. Drugs Aging 2020, 37, 715–723. [Google Scholar] [CrossRef] [PubMed]
- Balato, N.; Patruno, C.; Napolitano, M.; Patrì, A.; Ayala, F.; Scarpa, R. Managing Moderate-to-Severe Psoriasis in the Elderly. Drugs Aging 2014, 31, 233–238. [Google Scholar] [CrossRef]
- Megna, M.; Camela, E.; Cinelli, E.; Fabbrocini, G. Real-life efficacy and safety of secukinumab in elderly patients with psoriasis over a 2-year period. Clin. Exp. Dermatol. 2020, 45, 848–852. [Google Scholar] [CrossRef]
- van Winden, M.E.C.; van der Schoot, L.S.; van de L’Isle Arias, M.; van Vugt, L.J.; van den Reek, J.M.P.A.; van de Kerkhof, P.C.M.; de Jong, E.M.G.J.; Lubeek, S.F.K. Effectiveness and Safety of Systemic Therapy for Psoriasis in Older Adults: A Systematic Review. JAMA Dermatol. 2020, 156, 1229. [Google Scholar] [CrossRef] [PubMed]
- Ten Bergen, L.L.; Petrovic, A.; Krogh Aarebrot, A.; Appel, S. The TNF/IL-23/IL-17 Axis-Head-to-Head Trials Comparing Different Biologics in Psoriasis Treatment. Scand. J. Immunol. 2020, 92, e12946. [Google Scholar] [CrossRef]
- Singh, J.A.; Wells, G.A.; Christensen, R.; Tanjong Ghogomu, E.; Maxwell, L.J.; MacDonald, J.K.; Filippini, G.; Skoetz, N.; Francis, D.K.; Lopes, L.C.; et al. Adverse effects of biologics: A network meta-analysis and Cochrane overview. Cochrane. Database Syst. Rev. 2011, 2011, CD008794. [Google Scholar] [CrossRef]
- Dávila-Seijo, P.; Dauden, E.; Carretero, G.; Ferrandiz, C.; Vanaclocha, F.; Gómez-García, F.-J.; Herrera-Ceballos, E.; De la Cueva-Dobao, P.; Belinchón, I.; Sánchez-Carazo, J.-L.; et al. Survival of classic and biological systemic drugs in psoriasis: Results of the BIOBADADERM registry and critical analysis. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 1942–1950. [Google Scholar] [CrossRef] [PubMed]
- Carrascosa, J.M.; Notario, J. Supervivencia en terapia biológica. ¿Sabemos a qué nos referimos? ¿Podemos usarla? Actas. Dermo-Sifiliográficas 2014, 105, 729–733. [Google Scholar] [CrossRef] [PubMed]
- van den Ree, J.M.P.A.; Kievit, W.; Gniadecki, R.; Goeman, J.J.; Zweegers, J.; van de Kerkhof, P.C.M.; Seyger, M.M.B.; de Jong, E.M.G.J. Drug Survival Studies in Dermatology: Principles, Purposes, and Pitfalls. J. Investig. Dermatol. 2015, 135, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Iannone, L.F.; Bennardo, L.; Palleria, C.; Roberti, R.; De Sarro, C.; Naturale, M.D.; Dastoli, S.; Donato, L.; Manti, A.; Valenti, G.; et al. Safety Profile of Biologic Drugs for Psoriasis in Clinical Practice: An Italian Prospective Pharmacovigilance Study. PLoS ONE 2020, 15, e0241575. [Google Scholar] [CrossRef]
- Militello, G.; Xia, A.; Stevens, S.R.; Van Voorhees, A.S. Etanercept for the treatment of psoriasis in the elderly. J. Am. Acad. Dermatol. 2006, 55, 517–519. [Google Scholar] [CrossRef]
- Dattola, A.; Silvestri, M.; Tamburi, F.; Amoruso, G.F.; Bennardo, L.; Nisticò, S.P. Emerging Role of Anti-IL23 in the Treatment of Psoriasis: When Humanized Is Very Promising. Dermatol. Ther. 2020, 33, e14504. [Google Scholar] [CrossRef]
- Momose, M.; Asahina, A.; Hayashi, M.; Yanaba, K.; Umezawa, Y.; Nakagawa, H. Biologic treatments for elderly patients with psoriasis. J. Dermatol. 2017, 44, 1020–1023. [Google Scholar] [CrossRef] [PubMed]
- Ricceri, F.; Bardazzi, F.; Chiricozzi, A.; Dapavo, P.; Ferrara, F.; Mugheddu, C.; Romanelli, M.; Rongioletti, F.; Prignano, F. Elderly psoriatic patients under biological therapies: An Italian experience. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 143–146. [Google Scholar] [CrossRef] [Green Version]
- Carretero, G. Risk of Serious Adverse Events Associated with Biologic and Nonbiologic Psoriasis Systemic Therapy: Patients Ineligible vs Eligible for Randomized Controlled Trials. Arch. Dermatol. 2012, 148, 463. [Google Scholar] [CrossRef] [Green Version]
- Medina, C.; Carretero, G.; Ferrandiz, C.; Dauden, E.; Vanaclocha, F.; Gómez-García, F.J.; Herrera-Ceballos, E.; De la Cueva-Dobao, P.; Belinchón, I.; Sánchez-Carazo, J.L.; et al. Safety of classic and biologic systemic therapies for the treatment of psoriasis in elderly: An observational study from national BIOBADADERM registry. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 858–864. [Google Scholar] [CrossRef]
- Garber, C.; Plotnikova, N.; Au, S.; Sorensen, E.P.; Gottlieb, A. Biologic and Conventional Systemic Therapies Show Similar Safety and Efficacy in Elderly and Adult Patients with Moderate to Severe Psoriasis. J. Drugs Dermatol. 2015, 14, 846–852. [Google Scholar]
- Phan, C.; Beneton, N.; Delaunay, J.; Reguiai, Z.; Boulard, C.; Fougerousse, A.; Cinotti, E.; Romanelli, M.; Mery-Bossard, L.; Thomas-Beaulieu, D.; et al. Effectiveness and Safety of Anti-interleukin-17 Therapies in Elderly Patients with Psoriasis. Acta Derm. Venereol. 2020, 100, adv00316. [Google Scholar] [CrossRef] [PubMed]
- Sbidian, E.; Chaimani, A.; Afach, S.; Doney, L.; Dressler, C.; Hua, C.; Mazaud, C.; Phan, C.; Hughes, C.; Riddle, D.; et al. Systemic Pharmacological Treatments for Chronic Plaque Psoriasis: A Network Meta-Analysis. Cochrane Database Syst. Rev. 2020, 12, CD011535. [Google Scholar] [CrossRef]
- Fernandez-Torres, R.M.; Paradela, S.; Fonseca, E. Psoriasis in patients older than 65 years. A comparative study with younger adult psoriatic patients. J. Nutr. Health Aging 2012, 16, 586–591. [Google Scholar] [CrossRef] [PubMed]
- Puig, L.; Kirby, B.; Mallbris, L.; Strohal, R. Psoriasis beyond the Skin: A Review of the Literature on Cardiometabolic and Psychological Co-Morbidities of Psoriasis. Eur. J. Dermatol. 2014, 24, 305–311. [Google Scholar] [CrossRef]
- Puig, L. Cardiometabolic Comorbidities in Psoriasis and Psoriatic Arthritis. Int. J. Mol. Sci. 2017, 19, 58. [Google Scholar] [CrossRef] [Green Version]
- Napolitano, M.; Balato, N.; Ayala, F.; Patruno, C.; Patrì, A.; Megna, M.; Balato, A. Psoriasis in elderly and non-elderly population: Clinical and molecular features. G Ital. Dermatol. Venereol. 2016, 151, 587–595. [Google Scholar]
- Chen, L.; Tsai, T.-F. HLA-Cw6 and Psoriasis. Br. J. Dermatol. 2018, 178, 854–862. [Google Scholar] [CrossRef] [PubMed]
- Sandhu, V.K.; Ighani, A.; Fleming, P.; Lynde, C.W. Biologic Treatment in Elderly Patients with Psoriasis: A Systematic Review. J. Cutan. Med. Surg. 2020, 24, 174–186. [Google Scholar] [CrossRef] [PubMed]
- Dommasch, E.D.; Kim, S.C.; Lee, M.P.; Gagne, J.J. Risk of Serious Infection in Patients Receiving Systemic Medications for the Treatment of Psoriasis. JAMA Dermatol. 2019, 155, 1142. [Google Scholar] [CrossRef]
- Hayashi, M.; Umezawa, Y.; Fukuchi, O.; Ito, T.; Saeki, H.; Nakagawa, H. Efficacy and safety of ustekinumab treatment in elderly patients with psoriasis. J. Dermatol. 2014, 41, 974–980. [Google Scholar] [CrossRef] [PubMed]
- Chiricozzi, A.; Zangrilli, A.; Bavetta, M.; Bianchi, L.; Chimenti, S.; Saraceno, R. Real-life 9-year experience with adalimumab in psoriasis and psoriatic arthritis: Results of a single-centre, retrospective study. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 304–311. [Google Scholar] [CrossRef]
- Körber, A.; Papavassilis, C.; Bhosekar, V.; Reinhardt, M. Efficacy and Safety of Secukinumab in Elderly Subjects with Moderate to Severe Plaque Psoriasis: A Pooled Analysis of Phase III Studies. Drugs Aging 2018, 35, 135–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Megna, M.; Cinelli, E.; Balato, A.; Gallo, L.; Fabbrocini, G. Efficacy and safety of ixekizumab in a group of 16 elderly patients with psoriasis over a 1-year period. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e152–e153. [Google Scholar] [CrossRef]
- Yiu, Z.Z.N.; Mason, K.J.; Hampton, P.J.; Reynolds, N.J.; Smith, C.H.; Lunt, M.; Griffiths, C.E.M.; Warren, R.B.; the BADBIR Study Group. Drug survival of adalimumab, ustekinumab and secukinumab in patients with psoriasis: A prospective cohort study from the British Association of Dermatologists Biologics and Immunomodulators Register (BADBIR). Br. J. Dermatol. 2020, 183, 294–302. [Google Scholar] [CrossRef] [Green Version]
- Kojanova, M.; Fialova, J.; Cetkovska, P.; Dolezal, T.; Lomicova, I.; Arenberger, P.; Gkalpakiotis, S.; the BIOREP Study Group. Demographic Data, Comorbidities, Quality of Life, and Survival Probability of Biologic Therapy Associated with Sex-specific Differences in Psoriasis in the Czech Republic. Dermatol. Ther. 2021, 34, e14849. [Google Scholar] [CrossRef] [PubMed]
- Menter, A.; Papp, K.A.; Gooderham, M.; Pariser, D.M.; Augustin, M.; Kerdel, F.A.; Fakharzadeh, S.; Goyal, K.; Calabro, S.; Langholff, W.; et al. Drug survival of biologic therapy in a large, disease-based registry of patients with psoriasis: Results from the Psoriasis Longitudinal Assessment and Registry (PSOLAR). J. Eur. Acad. Dermatol. Venereol. 2016, 30, 1148–1158. [Google Scholar] [CrossRef]
- Gniadecki, R.; Bang, B.; Bryld, L.E.; Iversen, L.; Lasthein, S.; Skov, L. Comparison of long-term drug survival and safety of biologic agents in patients with psoriasis vulgaris. Br. J. Dermatol. 2015, 172, 244–252. [Google Scholar] [CrossRef]
- Galluzzo, M.; Talamonti, M.; De Simone, C.; D’Adamio, S.; Moretta, G.; Tambone, S.; Caldarola, G.; Fargnoli, M.C.; Peris, K.; Bianchi, L. Secukinumab in moderate-to-severe plaque psoriasis: A multi-center, retrospective, real-life study up to 52 weeks observation. Expert Opin. Biol. Ther. 2018, 18, 727–735. [Google Scholar] [CrossRef] [Green Version]
- Megna, M.; Di Costanzo, L.; Argenziano, G.; Balato, A.; Colasanti, P.; Cusano, F.; Galluccio, A.G.; Gambardella, A.; Lembo, S.; Mozzillo, R.; et al. Effectiveness and safety of secukinumab in Italian patients with psoriasis: An 84 week, multicenter, retrospective real-world study. Expert Opin. Biol. Ther. 2019, 19, 855–861. [Google Scholar] [CrossRef] [PubMed]
- Kojanova, M.; Cetkovska, P.; Strosova, D.; Fialova, J.; Arenberger, P.; Dolezal, T.; Gkalpakiotis, S.; BIOREP Study Group. Real-World Evidence from More Than 1000 Patients Treated with Adalimumab for Moderate-to-Severe Psoriasis in the Czech Republic. Dermatol. Ther. 2021, 11, 543–553. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Total Patients (n = 300) | |
| Sex (male), n (%) | 189 (63%) |
| Median age | 52.6 ± 13.6 |
| Age ≥65 | 60 (20.0%) |
| Positive family history of psoriasis (yes), n (%) | 185 (61.7%) |
| Onset before 40 years of age (%) | 236 (78.7%) |
| Duration of disease (months); mean ± SD; median | 26.58 ± 13.5; 27 |
| Cw6-positive (n = 152) | 68 (44.0%) |
| Comorbidities, n (%) | |
| Obesity (BMI ≥30) | 114 (38.0%) |
| Diabetes mellitus | 48 (16.0%) |
| Arterial hypertension | 92 (30.7%) |
| Dyslipidaemia | 138 (46.0%) |
| Arthritis | 124 (41.3%) |
| Prior treatments with biologics (%) | 137 (45.7%) |
| <65 Years | ≥65 Years | p | |
|---|---|---|---|
| Age | 47.8 ± 10.6 | 71.5 ± 5.4 | <0.001 |
| Male/Female, n (%) | 153 (63.8)/87 (36.3) | 36 (60.0)/24 (40.0) | 0.654 |
| Family history, No/Yes, n (%) | 79 (32.9)/161 (67.1) | 36 (60.0)/24 (40.0) | <0.001 |
| Early/late onset, n (%) | 211 (87.9)/29 (12.1) | 25 (41.7)/35 (58.3) | <0.001 |
| Cw6, positive/negative, n (%) | 64 (54.2)/54 (45.8) | 4 (11.8)/30 (82.2) | <0.001 |
| Evolution time ± SD | 25.8 ±13.2 | 29.6 ± 14.9 | 0.077 |
| Naive, Yes/No, n (%) | 135 (56.1)/105 (43.9) | 28 (46.7)/32 (53.3) | 0.196 |
| Obesity, No/Yes, n (%) | 149 (62.1)/91 (37.9) | 37 (61.7)/23 (38.3) | 0.928 |
| Dyslipidaemia, No/Yes, n (%) | 140 (58.3)/100 (41.7) | 22 (36.7)/38 (63.3) | 0.004 |
| Diabetes mellitus, No/Yes, n (%) | 213 (88.8)/27 (11.3) | 39 (65.0)/21 (35.0) | <0.001 |
| Arterial hypertension, No/Yes, n (%) | 180 (75.0)/60 (25.0) | 28 (46.7)/32 (53.3) | <0.001 |
| Arthritis, No/Yes, n (%) | 140 (58.3)/100 (41.7) | 36 (60.0)/24 (40.0) | 0.884 |
| All Biological Drug Treatments | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Global (n = 517) | Under 65 Years (n = 418) | 65+ Years (n = 99) | |||||||
| RR | 95% CI | p | RR | 95% CI | p | RR | 95% CI | p | |
| Sex | 1.398 | 1.053–1.855 | 0.020 | 1.517 | 1.106–2.081 | 0.010 | 1.323 | 0.679–2.756 | 0.411 |
| Obesity | 1.668 | 1.258–2.212 | 0.000 | 2.003 | 1.462–2.745 | 0.000 | 0.759 | 0.383–1.502 | 0.428 |
| Non-naive | 1.373 | 1.032–1.827 | 0.030 | 1.495 | 1.093–2.046 | 0.012 | 0.872 | 0.432–1.758 | 0.702 |
| Arthritis | 1.472 | 1.096–1.977 | 0.010 | 1.365 | 0.990–1.880 | 0.057 | 2.802 | 1.268–6.190 | 0.011 |
| Ustekinumab | |||||||||
| Global (n = 150) | Under 65 years (n = 117) | 65+ years (n = 33) | |||||||
| RR | 95% CI | p | RR | 95% CI | p | RR | 95% CI | p | |
| Sex | 0.982 | 0.550–1.756 | 0.952 | 0.991 | 0.499–1.967 | 0.980 | 1.113 | 0.328–3.780 | 0.864 |
| Obesity | 1.076 | 0.606–1.910 | 0.803 | 1.275 | 0.649–2.508 | 0.480 | 0.607 | 0.151–2.440 | 0.482 |
| Non-naive | 1.374 | 0.728–2.596 | 0.327 | 1.548 | 0.753–3.182 | 0.235 | 0.644 | 0.148–2.798 | 0.557 |
| Arthritis | 2.591 | 1.403–4.788 | 0.002 | 2.158 | 1.085–4.290 | 0.028 | 6.716 | 1.310–34.433 | 0.022 |
| Secukinumab | |||||||||
| Global (n = 100) | Under 65 years (n = 86) | 65+ years (n = 14) | |||||||
| RR | 95% CI | p | RR | 95% CI | p | RR | 95% CI | p | |
| Sex | 0.751 | 0.363–1.553 | 0.439 | 0.907 | 0.419–1.959 | 0.803 | |||
| Obesity | 2.248 | 1.094–4.617 | 0.027 | 2.541 | 1.188–5.433 | 0.016 | * | ||
| Non-naive | 2.341 | 0.954–5.743 | 0.063 | 2.822 | 1.072–7.425 | 0.036 | |||
| Arthritis | 1.626 | 0.768–3.443 | 0.204 | 1.506 | 0.705–3.217 | 0.291 | |||
| Adalimumab | |||||||||
| Global (n = 237) | Under 65 years (n = 191) | 65+ years (n = 46) | |||||||
| RR | 95% CI | p | RR | 95% CI | p | RR | 95% CI | p | |
| Sex | 1.768 | 1.214–2.574 | 0.003 | 1.970 | 1.291–3.007 | 0.002 | 1.296 | 0.522–3.216 | 0.576 |
| Obesity | 1.790 | 1.233–2.600 | 0.002 | 2.113 | 1.393–3.206 | 0.000 | 0.946 | 0.377–2.374 | 0.905 |
| Non-naive | 1.632 | 1.130–2.358 | 0.009 | 1.733 | 1.157–2.596 | 0.008 | 1.482 | 0.568–3.864 | 0.421 |
| Arthritis | 1.023 | 0.700–1.496 | 0.906 | 1.025 | 0.674–1.559 | 0.907 | 1.221 | 0.429–3.473 | 0.708 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Osuna, C.G.; García, S.R.; Martín, J.C.; Jiménez, V.G.; López, F.V.; Santos-Juanes, J. Use of Biological Treatments in Elderly Patients with Skin Psoriasis in the Real World. Life 2021, 11, 1348. https://doi.org/10.3390/life11121348
Osuna CG, García SR, Martín JC, Jiménez VG, López FV, Santos-Juanes J. Use of Biological Treatments in Elderly Patients with Skin Psoriasis in the Real World. Life. 2021; 11(12):1348. https://doi.org/10.3390/life11121348
Chicago/Turabian StyleOsuna, Cristina Galache, Sebastián Reyes García, Jimena Carrero Martín, Virginia García Jiménez, Francisco Vázquez López, and Jorge Santos-Juanes. 2021. "Use of Biological Treatments in Elderly Patients with Skin Psoriasis in the Real World" Life 11, no. 12: 1348. https://doi.org/10.3390/life11121348