Systematic Review with Meta-Analysis: Endoscopic and Surgical Resection for Ampullary Lesions

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Data Sources
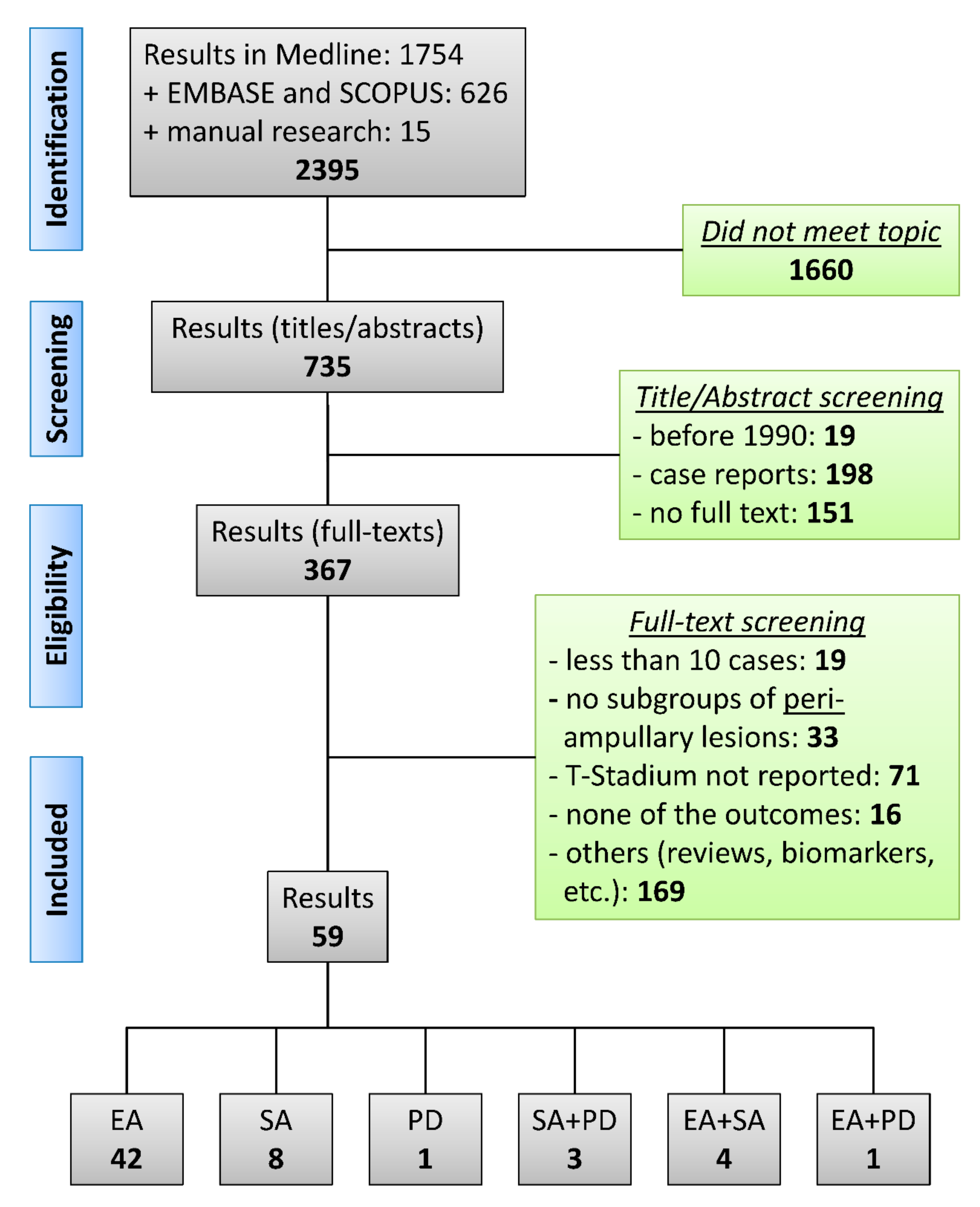
2.2. Study Selection Process and Outcome Measures
2.3. Quality Assessment
2.4. Statistical Analysis
3. Results
3.1. Study Characteristics and Quality
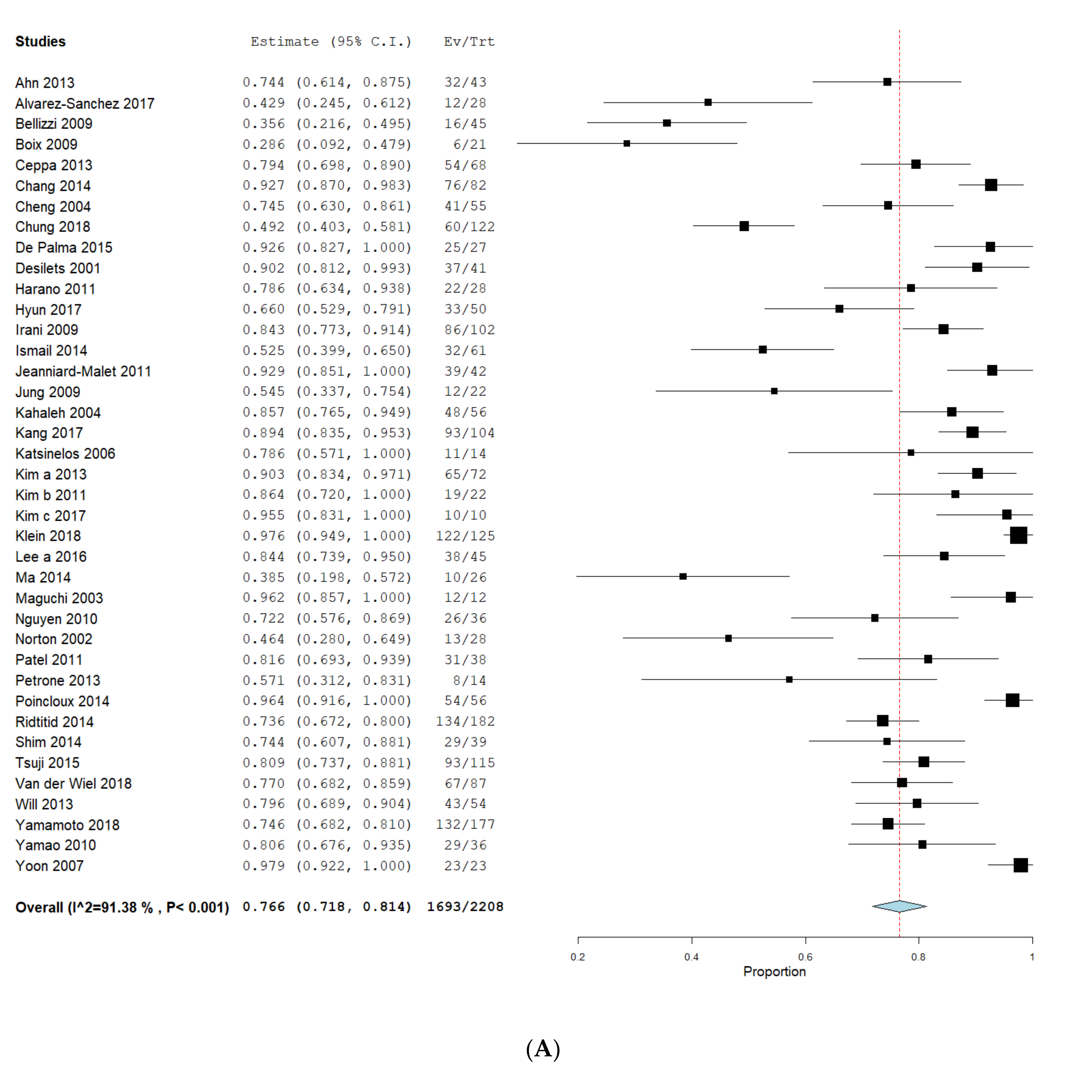
3.2. Complete Resection in Endoscopic and Surgical Interventions
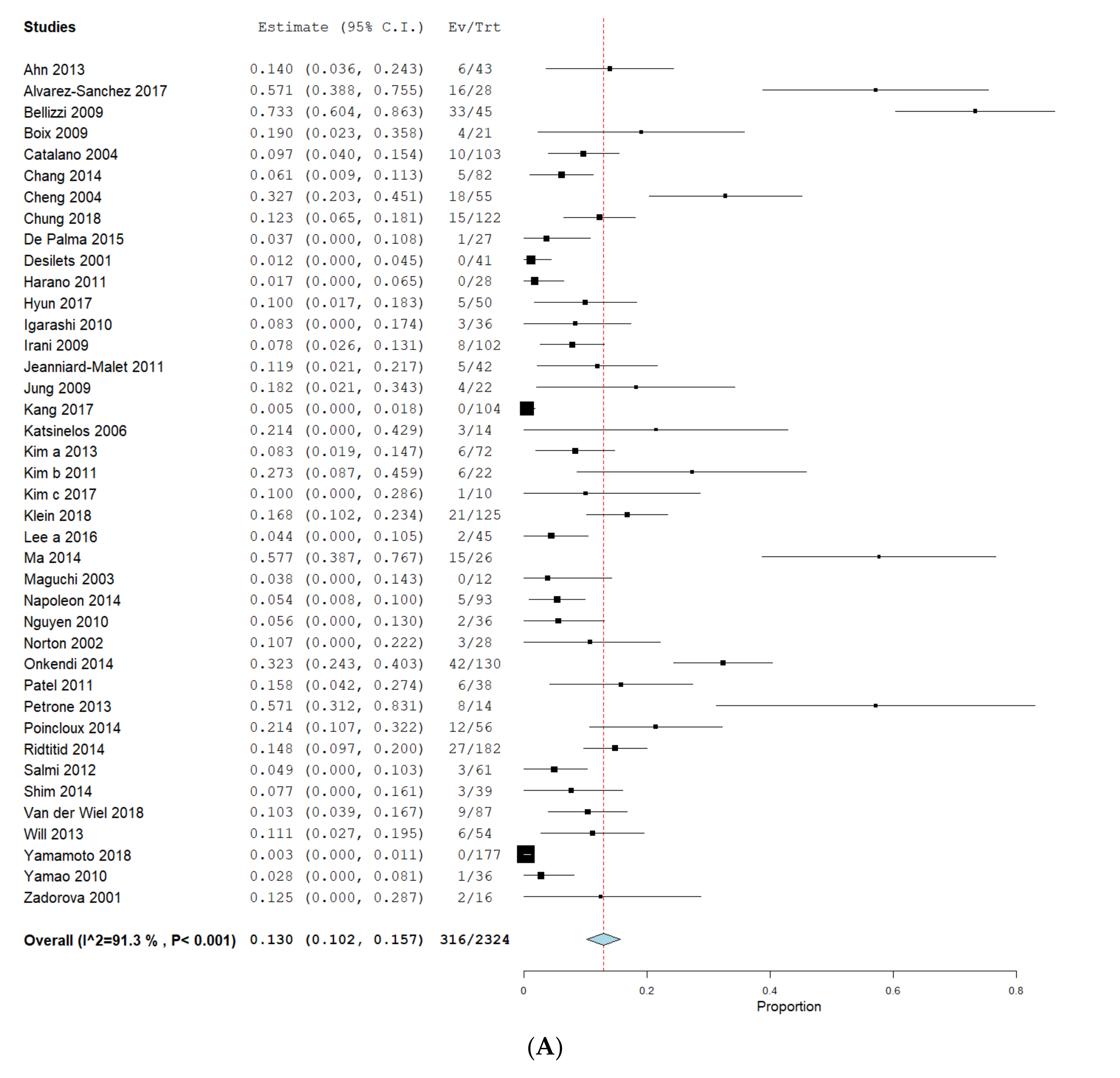
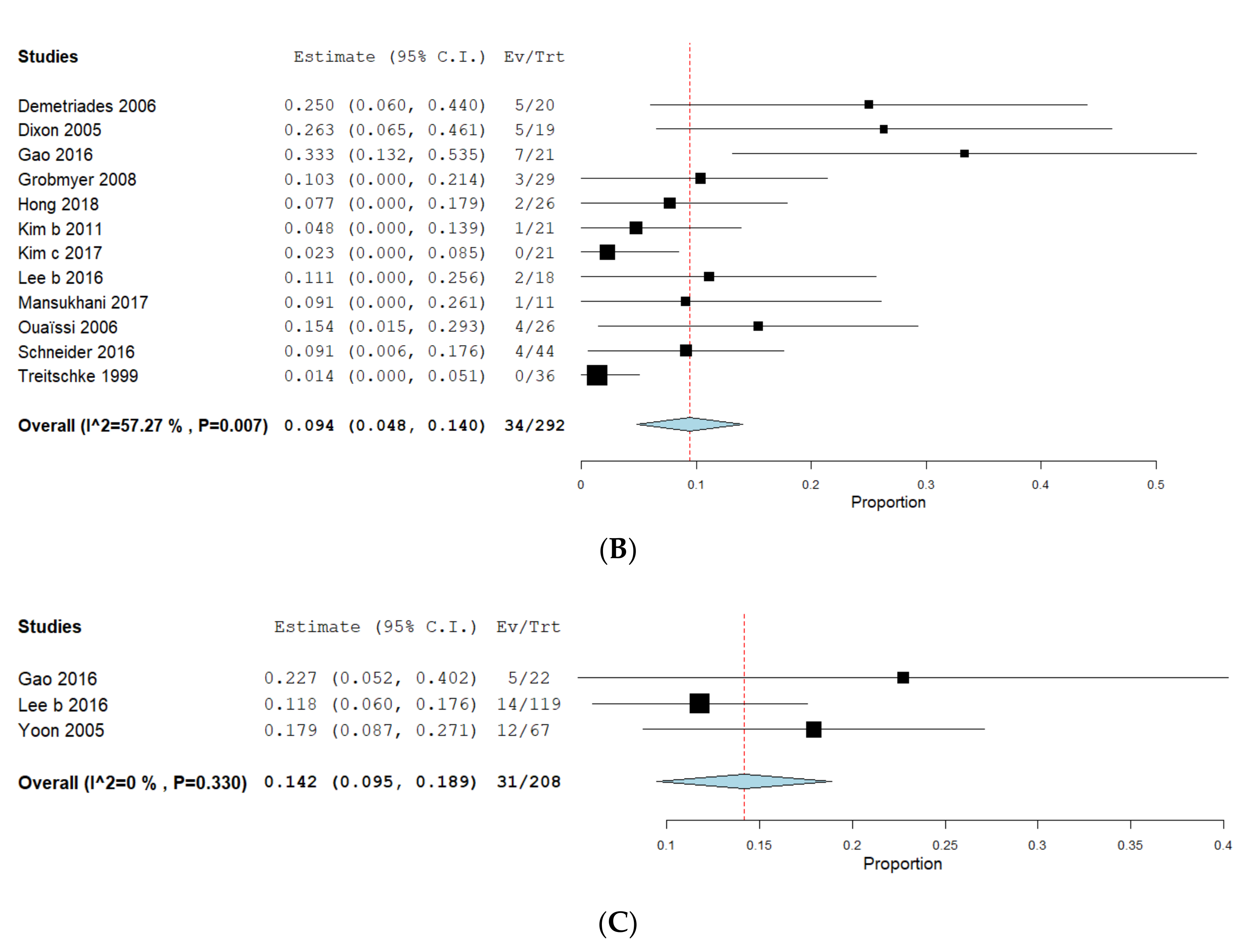
3.3. Complications
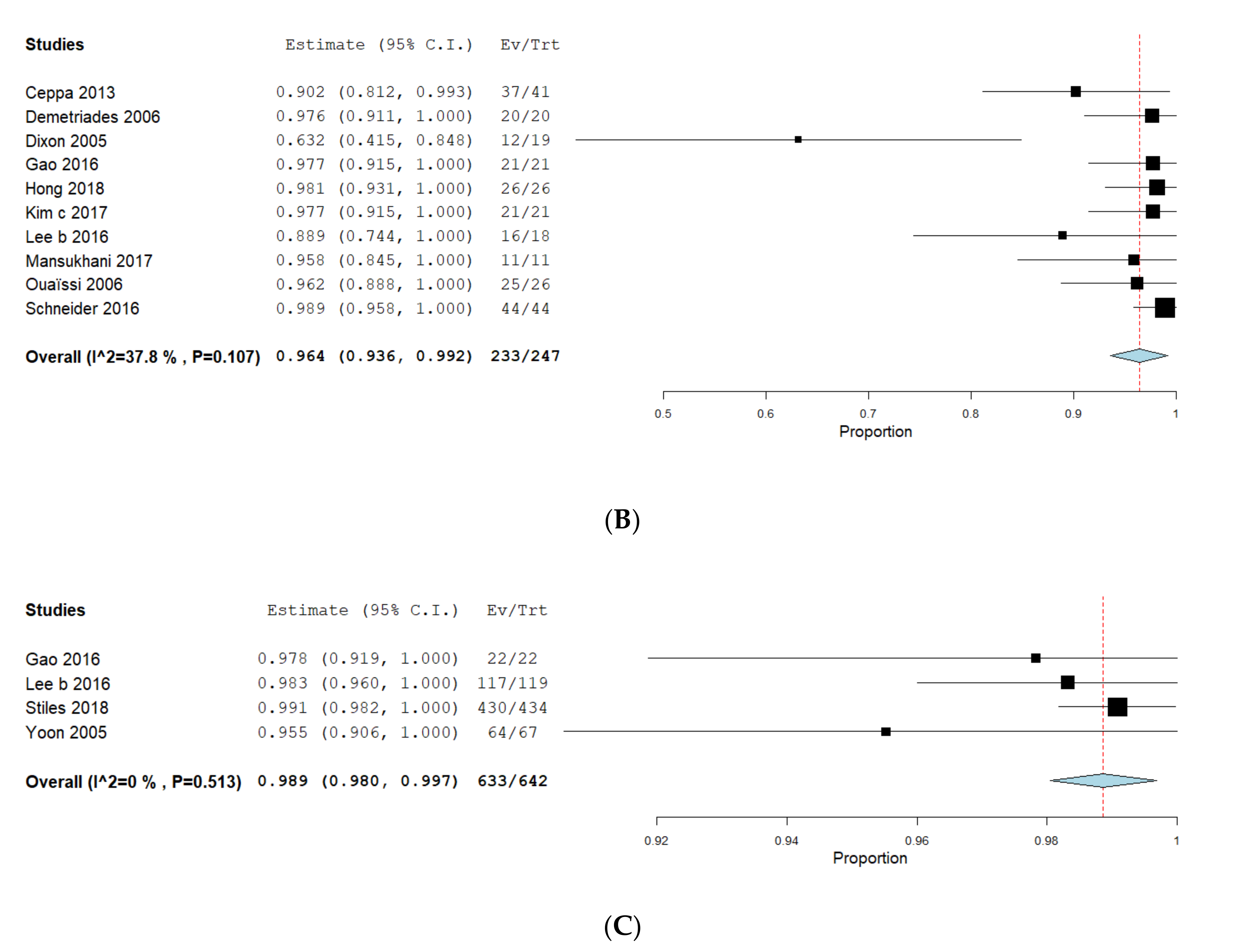
3.4. Recurrence
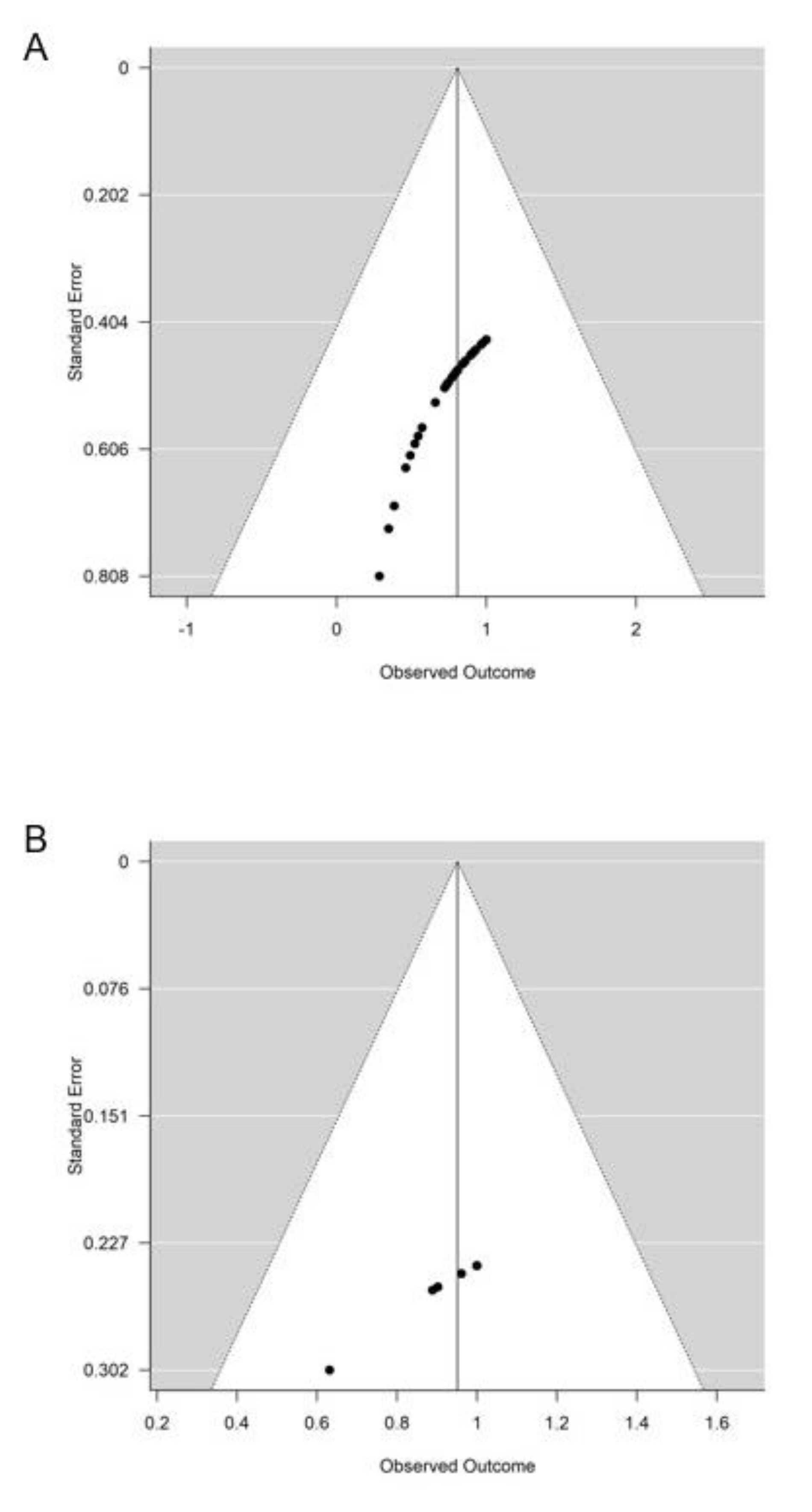
3.5. Publication Bias
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AA | ampullary adenoma |
| AC | ampullary adenocarcinoma |
| AE | adverse event |
| AL | ampullary lesion |
| APC | Argon plasma coagulation |
| CI | confidence interval |
| EA | Endoscopic ampullectomy |
| ESAP | Endoscopic versus Surgical Ampullectomy vs Pancreaticoduodenectomy |
| FAP | Familial adenomatous polyposis |
| GIST | Gastrointestinal stroma tumor |
| MeSH | medical subject headings |
| NOS | Newcastle-Ottawa-Scale |
| PD | Pancreaticoduodenectomy |
| PICO(S) | Population Intervention Comparison Outcome Study |
| PRISMA | Preferred Reporting Items for Systematic reviews and Meta-Analyses |
| RFA | Radiofrequency ablation |
| SA | Surgical ampullectomy |
References
- Jemal, A.; Siegel, R.; Ward, E.; Hao, Y.; Xu, J.; Murray, T.; Thun, M.J. Cancer statistics, 2008. CA Cancer J. Clin. 2008, 58, 71–96. [Google Scholar] [CrossRef] [PubMed]
- Albores-Saavedra, J.; Schwartz, A.M.; Batich, K.; Henson, D.E. Cancers of the ampulla of vater: Demographics, morphology, and survival based on 5,625 cases from the SEER program. J. Surg. Oncol. 2009, 100, 598–605. [Google Scholar] [CrossRef] [PubMed]
- Espinel, J.; Pinedo, E.; Ojeda, V.; Del Rio, M.G. Endoscopic management of adenomatous ampullary lesions. World J. Methodol. 2015, 5, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Espinel, J.; Pinedo, E.; Ojeda, V.; Del Rio, M.G. Endoscopic ampullectomy: A technical review. Rev. Esp. Enferm. Dig. 2016, 108, 271–278. [Google Scholar] [CrossRef] [Green Version]
- Gibbs, E.R.; Walton, G.F.; Kent, R.B., 3rd; Laws, H.L. Villous tumors of the ampulla Vater. Am. Surg. 1997, 63, 467–471. [Google Scholar]
- El Hajj, I.I.; Coté, G.A. Endoscopic diagnosis and management of ampullary lesions. Gastrointest. Endosc. Clin. N. Am. 2013, 23, 95–109. [Google Scholar] [CrossRef]
- Binmoeller, K.F.; Boaventura, S.; Ramsperger, K.; Soehendra, N. Endoscopic snare excision of benign adenomas of the papilla of Vater. Gastrointest. Endosc. 1993, 39, 127–131. [Google Scholar] [CrossRef]
- Kahn, M.B.; Rush, B.F. The overlooked technique of ampullary excision. Surg. Gynecol. Obstet. 1989, 169, 253–254. [Google Scholar]
- Talamini, M.A.; Moesinger, R.C.; Pitt, H.A.; Sohn, T.A.; Hruban, R.H.; Lillemoe, K.D.; Yeo, C.J.; Cameron, J.L. Adenocarcinoma of the ampulla of Vater. A 28-year experience. Ann. Surg. 1997, 225, 590–599. [Google Scholar] [CrossRef]
- De Palma, G.D. Endoscopic papillectomy: Indications, techniques, and results. World J. Gastroenterol. 2014, 20, 1537–1543. [Google Scholar] [CrossRef] [Green Version]
- Ito, K.; Fujita, N.; Noda, Y.; Kobayashi, G.; Obana, T.; Horaguchi, J.; Koshita, S.; Kanno, Y.; Ogawa, T.; Kato, Y.; et al. Impact of technical modification of endoscopic papillectomy for ampullary neoplasm on the occurrence of complications. Dig. Endosc. 2012, 24, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Bohnacker, S.; Seitz, U.; Nguyen, D.; Thonke, F.; Seewald, S.; deWeerth, A.; Ponnadurai, R.; Omar, S.; Soehendra, N. Endoscopic resection of benign tumors of the duodenal papilla without and with intraductal growth. Gastrointest. Endosc. 2005, 62, 551–560. [Google Scholar] [CrossRef] [PubMed]
- Perez-Cuadrado-Robles, E.; Piessevaux, H.; Moreels, T.G.; Yeung, R.; Aouattah, T.; Komuta, M.; Dano, H.; Jouret-Mourin, A.; Deprez, P.H. Combined excision and ablation of ampullary tumors with biliary or pancreatic intraductal extension is effective even in malignant neoplasms. United Eur. Gastroenterol. J. 2019, 7, 369–376. [Google Scholar] [CrossRef] [Green Version]
- Ogawa, T.; Ito, K.; Fujita, N.; Noda, Y.; Kobayashi, G.; Horaguchi, J.; Koshita, S.; Kanno, Y.; Masu, K.; Ishii, S. Endoscopic papillectomy as a method of total biopsy for possible early ampullary cancer. Dig. Endosc. 2012, 24, 291. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, K.; Enjoji, M.; Kitamura, K. Endoscopic biopsy has limited accuracy in diagnosis of ampullary tumors. Gastrointest. Endosc. 1990, 36, 588–592. [Google Scholar] [CrossRef]
- Spadaccinie, M.; Fugazza, A.; Frazzoni, L.; Di Leo, M.; Auriemma, F.; Carrara, S.; Maselli, R.; Galtieri, P.A.; Chandrasekar, V.T.; Fuccio, L.; et al. Endoscopic papillectomy for neoplastic ampullary lesions: A systematic review with pooled analysis. United Eur. Gastroenterol. J. 2019, 8, 44–51. [Google Scholar] [CrossRef] [Green Version]
- Ito, K.; Noda, Y.; Fujita, N.; Horaguchi, J.; Kurose, A.; Sawai, T. Ampullary cancer with pancreas divisum treated by endoscopic partial papillectomy: A case report. J. Gastrointest. Liver Dis. 2011, 20, 205–207. [Google Scholar]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 350, g7647. [Google Scholar] [CrossRef] [Green Version]
- Lo, C.K.; Mertz, D.; Loeb, M. Newcastle-Ottawa Scale: Comparing reviewers’ to authors’ assessments. BMC Med. Res. Methodol. 2014, 14, 45. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.; Gavaghan, D.; Egger, M. Publication and related bias in meta-analysis: Power of statistical tests and prevalence in the literature. J. Clin. Epidemiol. 2000, 53, 1119–1129. [Google Scholar] [CrossRef]
- Mccarty, T.R.; Rustagi, T. Comparative effectiveness and safety of radiofrequency ablation versus argon plasma coagulation for treatment of gastric antral vascular ectasia: A systematic review and meta-analysis. J. Clin. Gastroenterol. 2019, 53, 599–606. [Google Scholar] [CrossRef] [PubMed]
- Ahn, K.S.; Han, H.S.; Yoon, Y.S.; Cho, J.Y.; Khalikov, K. Laparoscopic transduodenal ampullectomy for benign ampullary tumors. J. Laparoendosc. Adv. Surg. Tech. 2010, 20, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Sanchez, M.V.; Oria, I.; Luna, O.B.; Pialat, J.; Gincul, R.; Lefort, C.; Bourdariat, R.; Fumex, F.; Lepilliez, V.; Scoazec, J.Y.; et al. Can endoscopic papillectomy be curative for early ampullary adenocarcinoma of the ampulla of Vater? Surg. Endosc. 2017, 31, 1564–1572. [Google Scholar] [CrossRef] [PubMed]
- Amini, A.; Miura, J.T.; Jayakrishnan, T.T.; Johnston, F.M.; Tsai, S.; Christians, K.K.; Gamblin, T.C.; Turaga, K.K. Is local resection adequate for T1 stage ampullary cancer? HPB 2015, 17, 66–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellizzi, A.M.; Kahaleh, M.; Stelow, E.B. The assessment of specimens procured by endoscopic ampullectomy. Am. J. Clin. Pathol. 2009, 132, 506–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boix, J.; Lorenzo-Zuniga, V.; de Vega, V.M.; Domènech, E.; Gassull, M.A. Endoscopic resection of ampullary tumors: 12-year review of 21 cases. Surg. Endosc. 2009, 23, 45–49. [Google Scholar] [CrossRef]
- Catalano, M.F.; Linder, J.D.; Chak, A.; Sivak, M.V., Jr.; Raijman, I.; Geenen, J.E.; Howell, D.A. Endoscopic management of adenoma of the major duodenal papilla. Gastrointest. Endosc. 2004, 59, 225–232. [Google Scholar] [CrossRef]
- Ceppa, E.P.; Burbridge, R.A.; Rialon, K.L.; Omotosho, P.A.; Emick, D.; Jowell, P.S.; Branch, M.S.; Pappas, T.N. Endoscopic versus surgical ampullectomy: An algorithm to treat disease of the ampulla of Vater. Ann. Surg. 2013, 257, 315–322. [Google Scholar] [CrossRef]
- Chang, W.I.; Min, Y.W.; Yun, H.S.; Lee, K.H.; Lee, J.K.; Lee, K.T.; Rhee, P.L. Prophylactic pancreatic stent placement for endoscopic duodenal ampullectomy: A single-center retrospective study. Gut Liver 2014, 8, 306–312. [Google Scholar] [CrossRef] [Green Version]
- Cheng, C.L.; Sherman, S.; Fogel, E.L.; McHenry, L.; Watkins, J.L.; Fukushima, T.; Howard, T.J.; Lazzell-Pannell, L.; Lehman, G.A. Endoscopic snare papillectomy for tumors of the duodenal papillae. Gastrointest. Endosc. 2004, 60, 757–764. [Google Scholar] [CrossRef]
- Chung, K.H.; Lee, S.H.; Choi, J.H.; Kang, J.; Paik, W.H.; Ahn, D.W.; Ryu, J.K.; Kim, Y.T. Effect of submucosal injection in endoscopic papillectomy of ampullary tumor: Propensity-score matching analysis. United Eur. Gastroenterol. J. 2018, 6, 576–585. [Google Scholar] [CrossRef] [PubMed]
- De Palma, G.D.; Luglio, G.; Maione, F.; Esposito, D.; Siciliano, S.; Gennarelli, N.; Cassese, G.; Persico, M.; Forestieri, P. Endoscopic snare papillectomy: A single institutional experience of a standardized technique. A retrospective cohort study. Int. J. Surg. 2015, 13, 180–183. [Google Scholar] [CrossRef] [PubMed]
- Demetriades, H.; Zacharakis, E.; Kirou, I.; Pramateftakis, M.G.; Sapidis, N.; Kanellos, I.; Betsis, D. Local excision as a treatment for tumors of ampulla of Vater. World J. Surg. Oncol. 2006, 4, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Desilets, D.J.; Dy, R.M.; Ku, P.M.; Hanson, B.L.; Mattia, A.; Howell, D.A. Endoscopic management of tumors of the major duodenal papilla: Refined techniques to improve outcome and avoid complications. Gastrointest. Endosc. 2001, 54, 202–208. [Google Scholar] [CrossRef]
- Dixon, E.; Vollmer, C.M., Jr.; Sahajpal, A.; Cattral, M.S.; Grant, D.R.; Taylor, B.R.; Langer, B.; Gallinger, S.; Greig, P.D. Transduodenal resection of peri-ampullary lesions. World J. Surg. 2005, 29, 649–652. [Google Scholar] [CrossRef] [PubMed]
- Dubois, M.; Labgaa, I.; Dorta, G.; Halkic, N. Endoscopic and surgical ampullectomy for non-invasive ampullary tumors: Short-term outcomes. Biosci. Trends 2017, 10, 507–511. [Google Scholar] [CrossRef] [Green Version]
- Gao, Y.; Zhu, Y.; Huang, X.; Wang, H.; Huang, X.; Yuan, Z. Transduodenal ampullectomy provides a less invasive technique to cure early ampullary cancer. BMC Surg. 2016, 16, 36. [Google Scholar] [CrossRef] [Green Version]
- Grobmyer, S.R.; Stasik, C.N.; Dragonov, P.; Hemming, A.W.; Dixon, L.R.; Vogel, S.B.; Hochwald, S.N. Contemporary results with ampullectomy for 29 “benign” neoplasms of the ampulla. J. Am. Coll. Surg. 2008, 206, 466–471. [Google Scholar] [CrossRef]
- Harano, M.; Ryozawa, S.; Iwano, H.; Taba, K.; Sen-Yo, M.; Sakaida, I. Clinical impact of endoscopic papillectomy for benign-malignant borderline lesions of the major duodenal papilla. J. Hepato Biliary Pancreat. Sci. 2011, 18, 190–194. [Google Scholar] [CrossRef]
- Hong, S.; Song, K.B.; Lee, Y.J.; Park, K.M.; Kim, S.C.; Hwang, D.W.; Lee, J.H.; Shin, S.H.; Kwon, J.; Ma, C.H.; et al. Transduodenal ampullectomy for ampullary tumors—Single center experience of consecutive 26 patients. Ann. Surg. Treat. Res. 2018, 95, 22–28. [Google Scholar] [CrossRef]
- Hyun, J.J.; Lee, T.H.; Park, J.S.; Han, J.H.; Jeong, S.; Park, S.M.; Lee, H.S.; Moon, J.H.; Park, S.H. A prospective multicenter study of submucosal injection to improve endoscopic snare papillectomy for ampullary adenoma. Gastrointest. Endosc. 2017, 85, 746–755. [Google Scholar] [CrossRef] [PubMed]
- Igarashi, Y.; Okano, N.; Ito, K.; Mimura, T.; Nakano, S. Endoscopic snare excision of a major duodenal papillary tumor. Dig. Surg. 2010, 27, 119–122. [Google Scholar] [CrossRef] [PubMed]
- Irani, S.; Arai, A.; Ayub, K.; Biehl, T.; Brandabur, J.J.; Dorer, R.; Gluck, M.; Jiranek, G.; Patterson, D.; Schembre, D.; et al. Papillectomy for ampullary neoplasm: Results of a single referral center over a 10-year period. Gastrointest. Endosc. 2009, 70, 923–932. [Google Scholar] [CrossRef] [PubMed]
- Ismail, S.; Marianne, U.; Heikki, J.; Jorma, H.; Leena, K. Endoscopic papillectomy, single-centre experience. Surg. Endosc. 2014, 28, 3234–3239. [Google Scholar] [CrossRef]
- Jeanniard-Malet, O.; Caillol, F.; Pesenti, C.; Bories, E.; Monges, G.; Giovannini, M. Short-term results of 42 endoscopic ampullectomies: A single-center experience. Scand. J. Gastroenterol. 2011, 46, 1014–1019. [Google Scholar] [CrossRef]
- Jung, S.; Kim, M.H.; Seo, D.W.; Lee, S.K. Endoscopic snare papillectomy of adenocarcinoma of the major duodenal papilla. Gastrointest. Endosc. 2001, 54, 622. [Google Scholar] [CrossRef]
- Kahaleh, M.; Shami, V.M.; Brock, A.; Conaway, M.R.; Yoshida, C.; Moskaluk, C.A.; Adams, R.B.; Tokar, J.; Yeaton, P. Factors predictive of malignancy and endoscopic resectability in ampullary neoplasia. Am. J. Gastroenterol. 2004, 99, 2335–2339. [Google Scholar] [CrossRef]
- Kang, S.H.; Kim, K.H.; Kim, T.N.; Jung, M.K.; Cho, C.M.; Cho, K.B.; Han, J.M.; Kim, H.G.; Kim, H.S. Therapeutic outcomes of endoscopic papillectomy for ampullary neoplasms: Retrospective analysis of a multicenter study. BMC Gastroenterol. 2017, 17, 69. [Google Scholar] [CrossRef]
- Katsinelos, P.; Kountouras, J.; Chatzimavroudis, G.; Zavos, C.; Paroutoglou, G.; Kotakidou, R.; Panagiotopoulou, K.; Papaziogas, B. A case of early depressed-type ampullary carcinoma treated by wire-guided endoscopic resection. Surg. Laparosc. Endosc. Percutaneous Tech. 2007, 17, 533–537. [Google Scholar] [CrossRef]
- Kim, S.H.; Moon, J.H.; Choi, H.J.; Kim, D.C.; Lee, T.H.; Cheon, Y.K.; Cho, Y.D.; Park, S.H.; Kim, S.J. Usefulness of pancreatic duct wire-guided endoscopic papillectomy for ampullary adenoma for preventing post-procedure pancreatitis. Endoscopy 2013, 45, 838–841. [Google Scholar] [CrossRef]
- Kim, A.L.; Choi, Y.I. Safety of duodenal ampullectomy for benign periampullary tumors. Ann. Hepato Biliary Pancreat. Surg. 2017, 21, 146–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.; Choi, S.H.; Choi, D.W.; Heo, J.S.; Jang, K.T. Role of transduodenal ampullectomy for tumors of the ampulla of Vater. J. Korean Surg. Soc. 2011, 81, 250–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klein, A.; Qi, Z.; Bahin, F.F.; Awadie, H.; Nayyar, D.; Ma, M.; Voermans, R.P.; Williams, S.J.; Lee, E.; Bourke, M.J. Outcomes after endoscopic resection of large laterally spreading lesions of the papilla and conventional ampullary adenomas are equivalent. Endoscopy 2018, 50, 972–983. [Google Scholar]
- Lee, H.; Park, J.Y.; Kwon, W.; Heo, J.S.; Choi, D.W.; Choi, S.H. Transduodenal Ampullectomy for the Treatment of Early-Stage Ampulla of Vater Cancer. World J. Surg. 2016, 40, 967–973. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.Y.; Cheon, Y.K.; Shim, C.S.; Choi, H.J.; Moon, J.H.; Choi, J.S.; Oh, H.C. Endoscopic wire-guided papillectomy versus conventional papillectomy for ampullary tumors: A prospective comparative pilot study. J. Gastroenterol. Hepatol. 2016, 31, 897–902. [Google Scholar] [CrossRef] [PubMed]
- Ma, T.; Jang, E.J.; Zukerberg, L.R.; Odze, R.; Gala, M.K.; Kelsey, P.B.; Forcione, D.G.; Brugge, W.R.; Casey, B.W.; Syngal, S.; et al. Recurrences are common after endoscopic ampullectomy for adenoma in the familial adenomatous polyposis (FAP) syndrome. Surg. Endosc. 2014, 28, 2349–2356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maguchi, H.; Takahashi, K.; Katanuma, A.; Hayashi, T.; Yoshida, A. Indication of endoscopic papillectomy for tumors of the papilla of vater and its problems. Dig. Endosc. 2003, 15, S33–S35. [Google Scholar] [CrossRef]
- Mansukhani, V.M.; Desai, G.S.; Mouli, S.; Shirodkar, K.; Shah, R.C.; Palepu, J. Transduodenal ampullectomy for ampullary tumors. Indian J. Gastroenterol. 2017, 36, 62–65. [Google Scholar] [CrossRef]
- Napoleon, B.; Gincul, R.; Ponchon, T.; Berhiller, J.; Escourrou, J.; Canard, J.M.; Boyer, J.; Barthet, M.; Ponsot, P.; Laugier, R.; et al. Endoscopic papillectomy for early ampullary tumors: Long-term results from a large multicenter prospective study. Endoscopy 2014, 46, 127–134. [Google Scholar] [CrossRef]
- Nguyen, N.; Shah, J.N.; Binmoeller, K.F. Outcomes of endoscopic papillectomy in elderly patients with ampullary adenoma or early carcinoma. Endoscopy 2010, 42, 975–977. [Google Scholar] [CrossRef]
- Norton, I.D.; Gostout, C.J.; Baron, T.H.; Geller, A.; Petersen, B.T.; Wiersema, M.J. Safety and outcome of endoscopic snare excision of the major duodenal papilla. Gastrointest. Endosc. 2002, 56, 239–243. [Google Scholar] [CrossRef]
- Onkendi, E.O.; Naik, N.D.; Rosedahl, J.K.; Harmsen, S.W.; Gostout, C.J.; Baron, T.H., Sr.; Sarr, M.G.; Que, F.G. Adenomas of the ampulla of Vater: A comparison of outcomes of operative and endoscopic resections. J. Gastrointest. Surg. 2014, 18, 1588–1596. [Google Scholar] [CrossRef]
- Ouaissi, M.; Sielezneff, I.; Alves, A.; Pirro, N.; Heyries, L.; Robitail, S.; Consentino, B.; Payan, M.J.; Valleur, P.; Panis, Y.; et al. Long term outcome following 26 surgical ampullectomies. Ann. Chir. 2006, 131, 322–327. [Google Scholar] [PubMed]
- Patel, R.; Davitte, J.; Varadarajulu, S.; Wilcox, C.M. Endoscopic resection of ampullary adenomas: Complications and outcomes. Dig. Dis. Sci. 2011, 56, 3235–3240. [Google Scholar] [CrossRef] [PubMed]
- Petrone, G.; Ricci, R.; Familiari, P.; Inzani, F.; Matsuoka, M.; Mutignani, M.; Delle Fave, G.; Costamagna, G.; Rindi, G. Endoscopic snare papillectomy: A possible radical treatment for a subgroup of T1 ampullary adenocarcinomas. Endoscopy 2013, 45, 401–404. [Google Scholar] [CrossRef]
- Poincloux, L.; Scanzi, J.; Goutte, M.; Pereira, B.; Devaud, H.; Joubert, J.; Dapoigny, M.; Bommelaer, G.; Abergel, A. Pancreatic intubation facilitated by methylene blue injection decreases the risk for postpapillectomy acute pancreatitis. Eur. J. Gastroenterol. Hepatol. 2014, 26, 990–995. [Google Scholar] [CrossRef]
- Ridtitid, W.; Schmidt, S.E.; Al-Haddad, M.A.; LeBlanc, J.; DeWitt, J.M.; McHenry, L.; Fogel, E.L.; Watkins, J.L.; Lehman, G.A.; Sherman, S.; et al. Performance characteristics of EUS for locoregional evaluation of ampullary lesions. Gastrointest. Endosc. 2015, 81, 380–388. [Google Scholar] [CrossRef] [Green Version]
- Salmi, S.; Ezzedine, S.; Vitton, V.; Ménard, C.; Gonzales, J.M.; Desjeux, A.; Grimaud, J.C.; Barthet, M. Can papillary carcinomas be treated by endoscopic ampullectomy? Surg. Endosc. 2012, 26, 920–925. [Google Scholar] [CrossRef]
- Schneider, L.; Contin, P.; Fritz, S.; Strobel, O.; Büchler, M.W.; Hackert, T. Surgical ampullectomy: An underestimated operation in the era of endoscopy. HPB 2016, 18, 65–71. [Google Scholar] [CrossRef] [Green Version]
- Shim, C.N.; Chung, M.J.; Bang, S.; Park, S.W.; Song, S.Y.; Chung, J.B.; Park, J.Y. Clinicopathologic characteristics associated with complications and long-term outcomes of endoscopic papillectomy for adenoma. Yonsei Med. J. 2014, 55, 644–650. [Google Scholar] [CrossRef] [Green Version]
- Stiles, Z.E.; Behrman, S.W.; Deneve, J.L.; Glazer, E.S.; Dong, L.; Wan, J.Y.; Martin, M.G.; Dickson, P.V. Ampullary adenocarcinoma: Defining predictors of survival and the impact of adjuvant therapy following surgical resection for stage I disease. J. Surg. Oncol. 2018, 117, 1500–1508. [Google Scholar] [CrossRef]
- Treitschke, F.; Beger, H.G. Local resection of benign periampullary tumors. Ann. Oncol. 1999, 10 (Suppl. 4), 212–214. [Google Scholar] [CrossRef] [PubMed]
- Tsuji, S.; Itoi, T.; Sofuni, A.; Mukai, S.; Tonozuka, R.; Moriyasu, F. Tips and tricks in endoscopic papillectomy of ampullary tumors: Single-center experience with large case series (with videos). J. Hepato Biliary Pancreat. Sci. 2015, 22, E22–E27. [Google Scholar] [CrossRef] [PubMed]
- Van der Wiel, S.E.; Poley, J.W.; Koch, A.D.; Bruno, M.J. Endoscopic resection of advanced ampullary adenomas: A single-center 14-year retrospective cohort study. Surg. Endosc. 2019, 33, 1180–1188. [Google Scholar] [CrossRef] [Green Version]
- Will, U.; Muller, A.K.; Fueldner, F.; Wanzar, I.; Meyer, F. Endoscopic papillectomy: Data of a prospective observational study. World J. Gastroenterol. 2013, 19, 4316–4324. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, K.; Itoi, T.; Sofuni, A.; Tsuchiya, T.; Tanaka, R.; Tonuzuka, R.; Honjo, M.; Mukai, S.; Fujita, M.; Asai, Y.; et al. Expanding the indication of endoscopic papillectomy for T1a ampullary carcinoma. Dig. Endosc. 2019, 31, 188–196. [Google Scholar] [CrossRef]
- Yamao, T.; Isomoto, H.; Kohno, S.; Mizuta, Y.; Yamakawa, M.; Nakao, K.; Irie, J. Endoscopic snare papillectomy with biliary and pancreatic stent placement for tumors of the major duodenal papilla. Surg. Endosc. 2010, 24, 119–124. [Google Scholar] [CrossRef]
- Yoon, S.M.; Kim, M.H.; Kim, M.J.; Jang, S.J.; Lee, T.Y.; Kwon, S.; Oh, S.C.; Lee, S.S.; Seo, D.W.; Lee, S.K. Focal early stage cancer in ampullary adenoma: Surgery or endoscopic papillectomy? Gastrointest. Endosc. 2007, 66, 701–707. [Google Scholar] [CrossRef] [Green Version]
- Zadorova, Z.; Dvofak, M.; Hajer, J. Endoscopic therapy of benign tumors of the papilla of Vater. Endoscopy 2001, 33, 345–347. [Google Scholar] [CrossRef]
- Ardengh, J.C.; Kemp, R.; Lima-Filho, E.R.; Dos Santos, J.S. Endoscopic papillectomy: The limits of the indication, technique and results. World J. Gastrointest. Endosc. 2015, 7, 987–994. [Google Scholar] [CrossRef]
- Beger, H.G.; Treitschke, F.; Gansauge, F.; Harada, N.; Hiki, N.; Mattfeldt, T. Tumor of the ampulla of Vater: Experience with local or radical resection in 171 consecutively treated patients. Arch. Surg. 1999, 134, 526–532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winter, J.M.; Cameron, J.L.; Olino, K.; Herman, J.M.; de Jong, M.C.; Hruban, R.H.; Wolfgang, C.L.; Eckhauser, F.; Edil, B.H.; Choti, M.A.; et al. Clinicopathologic analysis of ampullary neoplasms in 450 patients: Implications for surgical strategy and long-term prognosis. J. Gastrointest. Surg. 2010, 14, 379–387. [Google Scholar] [CrossRef] [PubMed]
- Yoon, Y.S.; Kim, S.W.; Park, S.J.; Lee, H.S.; Jang, J.Y.; Choi, M.G.; Kim, W.H.; Lee, K.U.; Park, Y.H. Clinicopathologic analysis of early ampullary cancers with a focus on the feasibility of ampullectomy. Ann. Surg. 2005, 242, 92–100. [Google Scholar] [CrossRef] [PubMed]
- Bassan, M.; Bourke, M. Endoscopic ampullectomy: A practical guide. J. Interv. Gastroenterol. 2012, 2, 23–30. [Google Scholar] [CrossRef] [Green Version]
- Chang, D.K.; Jamieson, N.B.; Johns, A.L.; Scarlett, C.J.; Pajic, M.; Chou, A.; Pinese, M.; Humphris, J.L.; Jones, M.D.; Toon, C.; et al. Histomolecular phenotypes and outcome in adenocarcinoma of the ampulla of vater. J. Clin. Oncol. 2013, 10, 1348–1356. [Google Scholar] [CrossRef]
- Agoritsas, T.; Merglen, A.; Courvoisier, D.S.; Combescure, C.; Garin, N.; Perrier, A.; Perneger, T.V. Sensitivity and predictive value of 15 PubMed search strategies to answer clinical questions rated against full systematic reviews. J. Med. Internet Res. 2012, 14, e85. [Google Scholar] [CrossRef]
- Haraldsson, E.; Swahn, F.; Verbeke, C.; Mattsson, J.S.M.; Enochsson, L.; Ung, K.A.; Lundell, L.; Heuchel, R.; Löhr, J.M.; Arnelo, U. Endoscopic papillectomy and KRAS expression in the treatment of adenoma in the major duodenal papilla. Scand. J. Gastroenterol. 2015, 50, 1419–1427. [Google Scholar] [CrossRef] [Green Version]
- Dumonceau, J.M.; Andriulli, A.; Elmunzer, B.J.; Mariani, A.; Meister, T.; Deviere, J.; Marek, T.; Baron, T.H.; Hassan, C.; Testoni, P.A.; et al. Prophylaxis of post-ERCP pancreatitis: European Society of Gastrointestinal Endoscopy (ESGE) Guideline—Updated June 2014. Endoscopy 2014, 46, 799–815. [Google Scholar] [CrossRef] [Green Version]
- Testoni, P.A.; Mariani, A.; Aabakken, L.; Arvanitakis, M.; Bories, E.; Costamagna, G.; Devière, J.; Dinis-Ribeiro, M.; Dumonceau, J.M.; Giovannini, M.; et al. Papillary cannulation and sphincterotomy techniques at ERCP: European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline. Endoscopy 2016, 48, 657–683. [Google Scholar] [CrossRef]
- Farges, O.; Bendersky, N.; Truant, S.; Delpero, J.R.; Pruvot, F.R.; Sauvanet, A. The theory and practice of pancreatic surgery in France. Ann. Surg. 2017, 266, 797–804. [Google Scholar] [CrossRef]
- Nimptsch, U.; Krautz, C.; Weber, G.F.; Mansky, T.; Grützmann, R. Nationwide in-hospital mortality following pancreatic surgery in Germany is higher than anticipated. Ann. Surg. 2016, 264, 1082–1090. [Google Scholar] [CrossRef] [PubMed]
- Ito, K.; Fujita, N.; Noda, Y.; Kobayashi, G.; Horaguchi, J.; Takasawa, O.; Obana, T. Preoperative evaluation of ampullary neoplasm with EUS and transpapillary intraductal US: A prospective and histopathologically controlled study. Gastrointest. Endosc. 2007, 66, 740–747. [Google Scholar] [CrossRef] [PubMed]
- Mendonca, E.Q.; Bernardo, W.M.; Moura, E.G.H.; Chaves, D.M.; Kondo, A.; Pu, L.Z.; Baracat, F.I. Endoscopic versus surgical treatment of ampullary adenomas: A systematic review and meta-analysis. Clinics 2016, 71, 28–35. [Google Scholar] [CrossRef]
- Liu, M.; Shunrong, J.; Xu, W.; Liu, W.; Qin, Y.; Hu, Q.; Sun, Q.; Zhang, Z.; Yu, X.; Xu, X. Laparoscopic pancreaticoduodenectomy: Are the best times coming? World J. Surg. Oncol. 2019, 10, 1624–1626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marino, M.V.; Podda, M.; Ruiz, M.G.; Fernandez, C.G.; Guarrasi, D.; Fleitas, M.G. Robotic-assisted versus open pancreaticoduodenectomy: The results of a case-matched comparison. J. Robot. Surg. 2020, 14, 493–502. [Google Scholar] [CrossRef]
- Nickel, F.; Haney, C.M.; Kowalewski, K.F.; Probst, P.; Limen, E.F.; Kalkum, E.; Diener, M.K.; Strobel, O.; Müller-Stich, B.P.; Hackert, T. Laparoscopic versus open pancreaticoduodenectomy: A systematic review and meta-analysis of randomized controlled trials. Ann. Surg. 2020, 1, 54–66. [Google Scholar] [CrossRef]
- Van Hilst, J.; de Rooij, T.; Bosscha, K.; Brinkman, D.J.; van Dieren, S.; Dijkgraaf, M.G.; Gerhards, M.F.; de Hingh, I.H.; Karsten, T.M.; Lips, D.J.; et al. Laparoscopic versus open pancreatoduodenectomy for pancreatic or periampullary tumours (LEOPARD-2): A multicentre, patient-blinded, randomised controlled phase 2/3 trial. Lancet Gastroenterol. Hepatol. 2019, 4, 199–207. [Google Scholar] [CrossRef]
- Hollenbach, M.; Auriemma, F. Endoscopic vs. surgical ampullectomy vs. pancreatitcoduodenectomy (ESAP) for ampullary neoplasm—A Pancreas2000/EPC study group. Pancreatology 2019, 19, S166. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study 1st Author | Year | NOS-Score | Selection I.1 | Selection I.2 | Selection I.3 | Selection I.4 | Comparability II | Outcome III.1 | Outcome III.2 | Outcome III.3 |
|---|---|---|---|---|---|---|---|---|---|---|
| Ahn | 2013 | 7 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 |
| Alvarez-Sanchez | 2017 | 7 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 |
| Amini | 2014 | 8 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Bellizzi | 2009 | 6 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 |
| Boix | 2009 | 5 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 0 |
| Catalano | 2004 | 7 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 |
| Ceppa | 2013 | 9 | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 |
| Chang | 2014 | 6 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 |
| Cheng | 2004 | 6 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 |
| Chung | 2018 | 6 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 0 |
| De Palma | 2015 | 7 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 |
| Demetriades | 2006 | 7 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 |
| Desilets | 2001 | 7 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 |
| Dixon | 2005 | 6 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 |
| Dubois | 2016 | 9 | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 |
| Gao | 2016 | 8 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Grobmyer | 2008 | 8 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Harano | 2011 | 7 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 |
| Hong | 2018 | 7 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 |
| Hyun | 2017 | 6 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 1 |
| Igarashi | 2010 | 6 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 |
| Irani | 2009 | 9 | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 |
| Ismail | 2014 | 6 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 |
| Jeanniard-Malet | 2011 | 6 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 |
| Jung | 2009 | 5 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 0 |
| Kahaleh | 2004 | 4 | 1 | 1 | 1 | 0 | 0 | 1 | 0 | 0 |
| Kang | 2017 | 6 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 |
| Katsinelos | 2006 | 6 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 |
| Kim a | 2013 | 6 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 |
| Kim c | 2017 | 8 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Kim b | 2011 | 8 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Klein | 2018 | 9 | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 |
| Lee a | 2016 | 7 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 |
| Lee b | 2016 | 8 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Ma | 2014 | 6 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 |
| Maguchi | 2003 | 6 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 |
| Mansukhani | 2017 | 7 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 |
| Napoleon | 2014 | 7 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 |
| Nguyen | 2010 | 7 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 |
| Norton | 2002 | 6 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 |
| Onkendi | 2014 | 8 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Ouaïssi | 2006 | 7 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 |
| Patel | 2011 | 6 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 |
| Petrone | 2013 | 7 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 |
| Poincloux | 2014 | 7 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 |
| Ridtitid | 2014 | 6 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 |
| Salmi | 2012 | 7 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 |
| Schneider | 2016 | 7 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 |
| Shim | 2014 | 7 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 |
| Stiles | 2018 | 8 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Treitschke | 1999 | 7 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 |
| Tsuji | 2015 | 6 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 |
| Van der Wiel | 2018 | 6 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 |
| Will | 2013 | 6 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 |
| Yamamoto | 2018 | 7 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 |
| Yamao | 2010 | 6 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 |
| Yoon | 2005 | 7 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 |
| Yoon | 2007 | 8 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Zadorova | 2001 | 6 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 |
| Study 1st Author | Year | Country | Patients | Period Start | End | Design | Procedure |
|---|---|---|---|---|---|---|---|
| Ahn | 2013 | Korea | retrospective | 2006 | 2009 | monocentric | EA |
| Alvarez-Sanchez | 2017 | France | retrospective | 05/1999 | 09/2013 | monocentric | EA |
| Amini | 2014 | USA | retrospective | 2004 | 2010 | register, multicentric | EA, SA, PD |
| Bellizzi | 2009 | USA | retrospective | NA | NA | monocentric | EA |
| Boix | 2009 | Spain | retrospective | 01/1995 | 02/2007 | monocentric | EA |
| Catalano | 2004 | USA | retrospective | 1998 | 2001 | mulitcentric | EA |
| Ceppa | 2013 | USA | retrospective | 1991 | 2010 | monocentric | EA, SA |
| Chang | 2014 | Korea | retrospective | 08/2002 | 06/2011 | monocentric | EA |
| Cheng | 2004 | USA | retrospective | 1994 | 2003 | monocentric | EA |
| Chung | 2018 | Korea | retrospective | 03/2006 | 03/2014 | monocentric | EA |
| De Palma | 2015 | Italy | retrospective | 2008 | 2013 | monocentric | EA |
| Demetriades | 2006 | Greece | retrospective | 1990 | 2004 | monocentric | SA |
| Desilets | 2001 | USA | retrospective | 1991 | 2000 | monocentric | EA |
| Dixon | 2005 | Canada | retrospective | 1992 | 2002 | mulitcentric | SA |
| Dubois | 2016 | Switzerland | retrospective | 2005 | 2015 | monocentric | EA, SA |
| Gao | 2016 | China | retrospective | 01/2001 | 12/2014 | monocentric | SA, PD |
| Grobmyer | 2008 | USA | retrospective | 01/1991 | 12/2006 | monocentric | SA |
| Harano | 2011 | Japan | retrospective | 11/1995 | 07/2009 | monocentric | EA |
| Hong | 2018 | Korea | retrospective | 2004 | 2016 | monocentric | SA |
| Hyun | 2017 | Korea | prospective, randomized | 01/2014 | 12/2015 | multicentric | EA |
| Igarashi | 2010 | Japan | retrospective | 10/2002 | 03/2009 | monocentric | EA |
| Irani | 2009 | USA | retrospective | 1997 | 2007 | monocentric | EA |
| Ismail | 2014 | Finland | retrospective | 2000 | 2012 | monocentric | EA |
| Jeanniard-Malet | 2011 | France | retrospective | 12/2003 | 11/2008 | monocentric | EA |
| Jung | 2009 | Korea | retrospective | 07/2003 | 06/2008 | monocentric | EA |
| Kahaleh | 2004 | USA | retrospective | 03/2000 | 05/2003 | monocentric | EA |
| Kang | 2017 | Korea | retrospective | 01/2007 | 07/2014 | multicentric | EA |
| Katsinelos | 2006 | Greece | retrospective | 1998 | 2004 | monocentric | EA |
| Kim a | 2013 | Korea | retrospective | 09/2005 | 03/2012 | monocentric | EA |
| Kim b | 2011 | Korea | retrospective | 01/1999 | 12/2008 | monocentric | EA, SA |
| Kim c | 2017 | Korea | retrospective | 01/2001 | 09/2016 | monocentric | EA, SA |
| Klein | 2018 | Australia | retrospective | 2018 | 06/2017 | monocentric | EA |
| Lee a | 2016 | Korea | prospective randomized | 01/2012 | 07/2014 | multicentric | EA |
| Lee b | 2016 | Korea | retrospective | 09/1994 | 06/2013 | monocentric | SA, PD |
| Ma | 2014 | USA | retrospective | 1999 | 2010 | multicentric | EA |
| Maguchi | 2003 | Japan | retrospective | 04/1997 | 10/2002 | monocentric | EA |
| Mansukhani | 2017 | India | retrospective | 2009 | 2015 | monocentric | SA |
| Napoleon | 2014 | France | prospective | 09/2003 | 01/2006 | mulitcentric | EA |
| Nguyen | 2010 | USA | retrospective | NA | NA | monocentric | EA |
| Norton | 2002 | USA | retrospective | 09/1997 | 11/1999 | monocentric | EA |
| Onkendi | 2014 | USA | retrospective | 1994 | 2009 | monocentric | EA, SA, PD |
| Ouaïssi | 2006 | France | retrospective | 1981 | 2004 | monocentric | SA |
| Patel | 2011 | USA | retrospective | 05/1996 | 08/2009 | monocentric | EA |
| Petrone | 2013 | Italy | retrospective | 10/2000 | 06/2009 | monocentric | EA |
| Poincloux | 2014 | France | retrospective | 2004 | 2011 | monocentric | EA |
| Ridtitid | 2014 | USA | retrospective | 07/1995 | 07/2012 | monocentric | EA |
| Salmi | 2012 | France | retrospective | 02/2002 | 12/2008 | monocentric | EA |
| Schneider | 2016 | Germany | prospective | 2001 | 2014 | monocentric | SA |
| Shim | 2014 | Korea | retrospective | 09/2006 | 04/2012 | monocentric | EA |
| Stiles | 2018 | USA | retrospective | 2004 | 2014 | register, multicentre | SA, PD |
| Treitschke | 1999 | Germany | retrospective | 1983 | 1999 | monocentric | SA, PD |
| Tsuji | 2015 | Japan | retrospective | 05/1999 | 04/2014 | monocentric | EA |
| Van der Wiel | 2018 | The Netherlands | retrospective | 2002 | 2016 | monocentric | EA |
| Will | 2013 | Germany | prospective | NA | NA | multicentric | EA |
| Yamamoto | 2018 | Japan | retrospective | 05/1999 | 12/2016 | monocentric | EA |
| Yamao | 2010 | Japan | retrospective | 09/2000 | 06/2008 | monocentric | EA |
| Yoon | 2005 | Korea | retrospective | 1986 | 2002 | monocentric | PD |
| Yoon | 2007 | Korea | retrospective | 1996 | 2006 | monocentric | EA, SA |
| Zadorova | 2001 | Czech Republic | retrospective | 1994 | 1999 | monocentric | EA |
| Study 1st Author | Year | Type | Number | % Male | Age (y) | Lesion Size (mm) | R0 (%) | Recurrence % | Follow-Up (m) | Complications Overall | AP | Bleeding | Perforation | Infection | Stenosis | Leakage | Others | % Adenoma | % Adeno-Ca | Hereditary Syndroms | Asymptomatic % |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ahn | 2013 | EA | 43 | NA | N | 15 | 74 | 14 | 10.4 | 32.6 | 16.3 | 9.3 | NA | 4.7 | 2.3 | NA | NA | 100 | 0 | 0 | 100 |
| Alvarez-Sanchez | 2017 | EA | 28 | 61 | 71.3 | 18 | 43 | 58 | 28 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 0 | 100 |
| Bellizzi | 2009 | EA | 45 | 60 | 62.9 | NA | 34.8 | 73 | 12 | NA | NA | NA | NA | NA | NA | NA | NA | 9.1 | 0 | 0 | NA |
| Boix | 2009 | EA | 21 | 43 | 67.2 | NA | 28.6 | 16.7 | 15.9 | 23.8 | 19 | 4.8 | 0 | NA | 0 | NA | NA | 52.4 | 47.6 | 0 | 0 |
| Catalano | 2004 | EA | 103 | 48 | 53.1 | 22.8 | NA | 9.7 | 36 | 9.7 | 4.9 | 1.9 | NA | NA | 2.9 | NA | NA | 80.6 | 5.8 | 0 | NA |
| Ceppa | 2013 | EA | 68 | 47 | 57,8 | NA | 80 | NA | NA | 18 | 9 | 9 | NA | NA | NA | NA | NA | NA | NA | 0 | NA |
| Chang | 2014 | EA | 82 | 65.9 | 54.7 | 13 | 92.7 | 6.6 | 24.2 | NA | 9.8 | 12.2 | 0 | 0 | 1.2 | NA | NA | 91.5 | NA | 0 | 45 |
| Cheng | 2004 | EA | 55 | 40 | 59 | NA | 73.7 | 33.3 | 30 | 14.5 | 9.1 | 29.1 | 1.8 | NA | 3.6 | NA | NA | 100 | 0 | 52.4 | 29.1 |
| Chung | 2018 | EA | 122 | 53.3 | 58.2 | NA | 49.2 | 12.3 | 82 | NA | 13.9 | 8.2 | 1,6 | 4.1 | 4.9 | NA | NA | 95.9 | 2.5 | 0 | 52.5 |
| De Palma | 2015 | EA | 27 | 62.9 | 68 | 23 | 92.6 | 3.7 | 18.4 | 18.5 | 11.1 | 7.4 | NA | NA | NA | NA | NA | NA | NA | 0 | 25.9 |
| Desilets | 2001 | EA | 41 | 56 | 68 | 24.7 | 91.3 | 0 | 19 | 4.9 | 2,4 | 2.4 | 0 | 0 | 0 | 0 | NA | 41.5 | 36.6 | 0 | NA |
| Dubois | 2016 | EA | 11 | 63.6 | 65 | 15 | NA | NA | NA | 9.1 | NA | NA | NA | NA | NA | NA | NA | NA | 0 | 13.9 | NA |
| Harano | 2011 | EA | 28 | 61 | 66.6 | 170 | 79 | 0 | 66 | NA | 7 | 18 | 0 | 7 | NA | NA | NA | 17 | 39.3 | 0 | 100 |
| Hyun | 2017 | EA | 50 | 48 | 60.7 | 11 | 66 | 10.9 | 12 | NA | 20 | 44 | 2 | 2 | 4 | NA | NA | 100 | 0 | 0 | 100 |
| Igarashi | 2010 | EA | 36 | 50 | 66 | 16.3 | NA | 8.3 | NA | 55.6 | 30 | 17 | 0 | 2.8 | 5.6 | NA | NA | NA | NA | 0 | 100 |
| Irani | 2009 | EA | 102 | NA | NA | 24 | 84.3 | 7.8 | NA | 20.6 | 9.8 | 4.9 | 2 | 1 | 2.9 | NA | NA | NA | NA | 0 | NA |
| Ismail | 2014 | EA | 61 | 62.2 | NA | NA | 52.3 | NA | NA | 24.6 | 9.8 | 18 | 3.3 | NA | NA | NA | NA | 78.7 | 16.4 | 0 | 19.7 |
| Jeanniard-Malet | 2011 | EA | 42 | 54.8 | 63 | NA | 92.9 | 12.1 | 15 | 23.8 | 14.3 | 7.1 | NA | 2.4 | NA | NA | NA | 100 | NA | 0 | 61.9 |
| Jung | 2009 | EA | 22 | 41 | 58 | 18.4 | 54.5 | 16.7 | 5.6 | 22.7 | 18.2 | 4.5 | 4.5 | 9.1 | NA | NA | NA | 100 | 0 | 0 | NA |
| Kahaleh | 2004 | EA | 56 | 55 | 62 | 22.3 | 86 | NA | NA | NA | 7.1 | 3.6 | NA | 1.8 | NA | NA | NA | NA | NA | 0 | NA |
| Kang | 2017 | EA | 104 | 66 | 60.5 | 13.5 | 89.4 | 0 | 44.2 | 31.7 | 15.4 | 17.3 | 7.7 | NA | NA | NA | NA | 77.9 | 5.8 | 60.6 | 38.5 |
| Katsinelos | 2006 | EA | 14 | 57.1 | 62.6 | 14.4 | 78.6 | 18.2 | 28.4 | 14.3 | 7.1 | 7.1 | 0 | 0 | 0 | NA | NA | 100 | NA | 0 | 0 |
| Kim a | 2013 | EA | 72 | 56.9 | 56.4 | 8.7 | 90.3 | 7.7 | 23.7 | 25 | 8.3 | 16.7 | 0 | NA | NA | NA | NA | 100 | NA | 0 | NA |
| Kim b | 2011 | EA | 22 | NA | NA | NA | 86 | 27 | 10 | 50 | 27.3 | 13.6 | 4.5 | NA | 4.5 | NA | NA | NA | NA | 0 | 0 |
| Kim c | 2017 | EA | 10 | 70 | 64 | 8 | 100 | 10 | 15 | 50 | NA | 30 | 10 | 0 | 0 | 0 | 10 | NA | NA | 0 | NA |
| Klein | 2018 | EA | 125 | 50.4 | 64 | 20 | 97.6 | 17 | 18.5 | NA | 7.2 | 44.8 | 0.8 | NA | NA | NA | NA | NA | NA | 37 | NA |
| Lee a | 2016 | EA | 45 | 55.6 | 56 | NA | 84.4 | 4.4 | NA | 26.7 | 15.6 | 6.7 | 2.2 | 0 | 2.2 | NA | NA | NA | NA | 0 | NA |
| Ma | 2014 | EA | 26 | 34.6 | 27.8 | 9.9 | 38.5 | 58.3 | 84.5 | 30.8 | 19.2 | 3.8 | NA | NA | 15.4 | NA | NA | NA | NA | 34.6 | NA |
| Maguchi | 2003 | EA | 12 | 58.3 | 65.7 | 21.6 | 100 | 0 | NA | 41.7 | 25 | 25 | 8.3 | NA | NA | NA | NA | NA | NA | 0 | NA |
| Napoleon | 2014 | EA | 93 | 47.3 | 57 | NA | NA | 5.4 | 36 | 42 | 23.7 | 11.8 | 4.3 | 8.6 | 2.2 | NA | NA | NA | NA | 0 | 100 |
| Nguyen | 2010 | EA | 36 | 52.8 | 63 | 23.9 | 72,2 | 5.6 | NA | NA | 0 | 30.6 | NA | NA | NA | NA | NA | 88.9 | 11.1 | 0 | 100 |
| Norton | 2002 | EA | 28 | 54 | 42 | NA | 46,2 | 9.5 | 13 | NA | 15.4 | 7.7 | 3.8 | NA | 9.5 | NA | NA | NA | NA | 0 | 0 |
| Onkendi | 2014 | EA | 130 | 52.3 | NA | 17 | NA | 32 | NA | 29 | 14.6 | 13.1 | 0.7 | NA | NA | NA | 0.7 | NA | NA | 0 | NA |
| Patel | 2011 | EA | 38 | 42 | 54.3 | 17.3 | 81 | 15.8 | 17.2 | 15.8 | 7.9 | 5.3 | 0 | 2.6 | 0 | NA | NA | 100 | 0 | 0 | 55.3 |
| Petrone | 2013 | EA | 14 | 50 | 74.6 | 15.3 | 57,1 | 57.1 | 29.6 | NA | NA | NA | NA | NA | NA | NA | NA | NA | 33.3 | 73.3 | NA |
| Poincloux | 2014 | EA | 56 | 57.1 | 64 | 16 | 96,4 | 21.4 | 24 | 19.5 | 10.7 | 7.1 | 1.8 | 1.8 | NA | NA | 1.8 | 76.8 | 23.2 | 0 | 100 |
| Ridtitid | 2014 | EA | 182 | 48.4 | 61.4 | 16.6 | 73,6 | 15 | 190 | 18.7 | 3.8 | 12.6 | 1.6 | NA | 3.8 | NA | 0.5 | 75.8 | 6.6 | 0 | 39 |
| Salmi | 2012 | EA | 61 | 45 | 64 | NA | NA | 5 | 36 | 11 | 10 | 5 | 3 | NA | NA | NA | NA | 53 | 16 | 0 | NA |
| Shim | 2014 | EA | 39 | 61 | 62 | 13.9 | 74,3 | 7.7 | 15 | 71.8 | 17.9 | 10.3 | 5.1 | NA | NA | NA | 5.1 | 81.6 | 7.7 | 0 | 100 |
| Tsuji | 2015 | EA | 115 | 65.2 | 64.5 | 16.2 | 80,9 | NA | NA | NA | 10.4 | 18.2 | 2.6 | 1.7 | 4.3 | NA | NA | 90.4 | 9.6 | 0 | NA |
| Van der Wiel | 2018 | EA | 87 | 51.7 | 65 | 27.7 | 77 | 10.7 | 60 | 25.3 | 3.4 | 12.6 | 8.1 | 1.1 | 0 | NA | NA | 100 | 0 | 0 | 71 |
| Will | 2013 | EA | 54 | 46.3 | 64.6 | NA | 79,2 | 11.8 | NA | 18.5 | 13 | 5.6 | 1.9 | NA | NA | NA | NA | 44.4 | 33.3 | 0 | 79.6 |
| Yamamoto | 2018 | EA | 177 | 61 | 62.7 | 14.4 | 74,6 | 0 | 30 | 40.7 | 10.2 | 20.3 | 2.8 | 2.8 | 6.8 | NA | NA | 93.2 | 6.8 | 0 | NA |
| Yamao | 2010 | EA | 36 | 58.3 | 66 | 14.3 | 80,6 | 3.4 | 17.9 | NA | 8.3 | 8.3 | 0 | 0 | 2.8 | NA | NA | 100 | 0 | 0 | 100 |
| Yoon | 2007 | EA | 23 | NA | NA | 18 | 100 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 66.2 | 33.8 | 0 | NA |
| Zadorova | 2001 | EA | 16 | 56.3 | 68 | NA | NA | 11.1 | NA | 14.8 | 7.4 | 7.4 | NA | NA | NA | NA | NA | 100 | NA | 0 | 100 |
| Amini | 2014 | SA | 41 | 49 | 74 | 17 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 0 | 100 | 0 | NA |
| Ceppa | 2013 | SA | 41 | 40 | 56.5 | NA | 90 | NA | NA | 42 | 10 | NA | NA | 15 | NA | NA | 17 | 56 | 12 | 0 | NA |
| Demetriades | 2006 | SA | 20 | 60 | 68.5 | 13 | 100 | 25 | 85 | 10 | 0 | 0 | 0 | 10 | 0 | 0 | 0 | 8 | 12 | 0 | 100 |
| Dixon | 2005 | SA | 19 | 53 | 64.2 | 27 | 63 | 28 | 48.6 | 37 | 0 | 0 | 0 | 5 | 0 | 5 | 27 | 63 | 37 | 0 | 100 |
| Dubois | 2016 | SA | 19 | 37 | 69 | 14 | NA | NA | NA | 68 | NA | NA | NA | NA | NA | NA | NA | 63 | 26 | 5.3 | NA |
| Gao | 2016 | SA | 21 | 59 | 68 | 12 | 100 | 31.8 | 75 | 13.6 | NA | 23.8 | NA | 14.3 | NA | NA | 0 | 0 | 100 | 0 | 0 |
| Grobmyer | 2008 | SA | 29 | NA | 63 | 20 | NA | 10 | 16 | 45 | 10 | 0 | 0 | 41 | 0 | 14 | 35 | 90 | 14 | 4 | NA |
| Hong | 2018 | SA | 26 | 50 | 60.2 | 20 | 100 | 9.1 | 72 | 30.8 | 0 | 3.8 | 0 | 7.7 | 3.8 | 0 | 15.5 | 88,5 | 11,5 | 0 | NA |
| Kim b | 2011 | SA | 21 | NA | NA | NA | NA | 4.7 | 18 | 23.8 | 9.5 | NA | NA | NA | NA | NA | 9.4 | 38 | 14,3 | 0 | 45 |
| Kim c | 2017 | SA | 21 | 57.1 | 61 | 15 | 100 | 0 | 8 | 23.8 | NA | 4.76 | 0 | 9.5 | 4.7 | 4.7 | 0 | 61,9 | 19 | 0 | 29.1 |
| Lee b | 2016 | SA | 18 | 50 | 59 | 16 | 89 | 11.1 | 50 | 33 | 0 | 0 | 0 | 23 | 6 | 6 | 0 | 0 | 100 | 0 | 52.5 |
| Mansukhani | 2017 | SA | 11 | NA | 56 | NA | 100 | 9 | 34 | 9 | 0 | 0 | 0 | 0 | 0 | 0 | 9 | 64 | 36 | 0 | 25.9 |
| Ouaïssi | 2006 | SA | 26 | 58 | 59 | 20 | 96 | 15 | 86 | 7.7 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 58 | 15 | 30 | NA |
| Schneider | 2016 | SA | 44 | 36 | 67 | NA | 100 | 8.1 | 54 | 36 | 4.3 | NA | NA | 3.3 | NA | 2.2 | 24.9 | 100 | 0 | 0 | NA |
| Treitschke | 1999 | SA | 36 | 41 | 59 | NA | NA | 0 | 42 | NA | NA | NA | NA | NA | NA | NA | NA | 86 | 0 | 0 | 100 |
| Amini | 2014 | PD | 136 | 52 | 72 | 13 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 0 | 100 | 0 | 100 |
| Gao | 2016 | PD | 22 | 52 | 67 | 12 | 100 | 23.8 | 75 | 42.8 | NA | 4.5 | NA | 9.1 | NA | NA | 19 | 0 | 100 | 0 | 100 |
| Lee b | 2016 | PD | 119 | 46 | 62 | 18 | 98.3 | 11.8 | 50 | 43 | 0 | 4 | 0 | 7 | 0 | 8 | 17 | 0 | 100 | 0 | NA |
| Stiles | 2018 | PD | 434 | 55.1 | 62.9 | 18 | 99.1 | NA | 29.4 | NA | NA | NA | NA | NA | NA | NA | NA | 0 | 100 | 0 | 19.7 |
| Yoon | 2005 | PD | 67 | 58 | 56.7 | 18 | 95.5 | 18.2 | 58.9 | 49.3 | NA | 6 | 0 | 16.4 | 0 | 19.4 | 13.4 | 0 | 100 | 0 | 61.9 |
| Study 1st Author | Year | EUS Performed | Patients with EUS (%) | Prior ERCP | Paitents with Prior ERCP (%) | Implantation of Stents | Submucosal Injection | Additional Intervention |
|---|---|---|---|---|---|---|---|---|
| Ahn | 2013 | YES | 100 | YES | 100 | PD | YES | EA |
| Alvarez-Sanchez | 2017 | YES | 100 | YES | 100 | NA | NA | Surg |
| Bellizzi | 2009 | NO | 0 | NO | 0 | NO | NO | NA |
| Boix | 2009 | YES | NA | NA | NA | NO | YES | APC |
| Catalano | 2004 | YES | NA | NA | NA | BD + PD | NO | Surg + RFA |
| Ceppa | 2013 | NA | NA | NA | NA | NO | NO | NA |
| Chang | 2014 | YES | 45 | YES | 100 | BD + PD | YES | Surg |
| Cheng | 2004 | YES | 29.1 | NA | NA | PD | YES | NA |
| Chung | 2018 | YES | 52.5 | YES | 100 | BD + PD | YES | Surg + APC |
| De Palma | 2015 | YES | 25.9 | YES | 100 | PD | NO | NA |
| Desilets | 2001 | NO | 0 | YES | 100 | BD + PD | YES | APC |
| Dubois | 2016 | NA | NA | NA | NA | NO | NO | NA |
| Harano | 2011 | YES | 100 | YES | 100 | BD + PD | YES | EA |
| Hyun | 2017 | YES | 100 | NA | NA | BD + PD | YES | Surg |
| Igarashi | 2010 | YES | 100 | YES | 100 | BD + PD | NO | APC |
| Irani | 2009 | YES | 42 | NA | NA | NA | NA | NA |
| Ismail | 2014 | YES | 19.7 | NA | NA | PD | NO | NA |
| Jeanniard-Malet | 2011 | YES | 61.9 | NO | 0 | BD + PD | NO | Surg |
| Jung | 2009 | NO | 0 | YES | 100 | BD + PD | YES | Surg |
| Kahaleh | 2004 | YES | NA | NO | 0 | PD | NO | NA |
| Kang | 2017 | YES | 38.5 | YES | 79.8 | BD + PD | YES | EA + Surg |
| Katsinelos | 2006 | NO | 0 | YES | 100 | BD + PD | YES | Surg |
| Kim a | 2013 | NO | 0 | NO | 0 | PD | NO | NA |
| Kim b | 2011 | NA | NA | NA | NA | NA | NA | NA |
| Kim c | 2017 | NA | NA | NA | NA | NA | NA | NA |
| Klein | 2018 | YES | NA | YES | 100 | BD + PD | YES | Surg |
| Lee a | 2016 | YES | NA | YES | NA | PD | NO | EA + Surg |
| Ma | 2014 | NO | 0 | NA | NA | BD + PD | YES | EA + Surg |
| Maguchi | 2003 | NO | 0 | NO | 0 | BD + PD | NO | NA |
| Napoleon | 2014 | YES | 100 | NO | 0 | PD | YES | RFA |
| Nguyen | 2010 | YES | 100 | NO | 0 | PD | NO | Surg |
| Norton | 2002 | NO | 0 | YES | 100 | BD + PD | NO | Surg |
| Onkendi | 2014 | YES | 27.8 | YES | 49.4 | NA | NA | NA |
| Patel | 2011 | YES | 55-3 | YES | 100 | PD | NO | NA |
| Petrone | 2013 | NO | 0 | YES | 100 | PD | NO | APC |
| Poincloux | 2014 | YES | 100 | YES | 100 | PD | YES | Surg + APC + RCT |
| Ridtitid | 2014 | YES | 39 | YES | 100 | PD | YES | Caut |
| Salmi | 2012 | NA | NA | NA | NA | BD + PD | YES | EA |
| Shim | 2014 | YES | 100 | YES | 100 | BD + PD | YES | EA+APC |
| Tsuji | 2015 | NO | 0 | NO | 0 | NO | NO | Surg |
| Van der Wiel | 2018 | YES | 71 | YES | 100 | PD | YES | APC |
| Will | 2013 | YES | 79.6 | YES | 44.8 | NA | NA | NA |
| Yamamoto | 2018 | YES | NA | NA | NA | NO | NO | NA |
| Yamao | 2010 | YES | 100 | YES | 100 | BD + PD | NO | APC |
| Yoon | 2007 | NA | NA | NA | NA | NA | NA | NA |
| Zadorova | 2001 | YES | 100 | YES | 93.6 | BD + PD | NO | APC |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heise, C.; Abou Ali, E.; Hasenclever, D.; Auriemma, F.; Gulla, A.; Regner, S.; Gaujoux, S.; Hollenbach, M. Systematic Review with Meta-Analysis: Endoscopic and Surgical Resection for Ampullary Lesions. J. Clin. Med. 2020, 9, 3622. https://doi.org/10.3390/jcm9113622
Heise C, Abou Ali E, Hasenclever D, Auriemma F, Gulla A, Regner S, Gaujoux S, Hollenbach M. Systematic Review with Meta-Analysis: Endoscopic and Surgical Resection for Ampullary Lesions. Journal of Clinical Medicine. 2020; 9(11):3622. https://doi.org/10.3390/jcm9113622
Chicago/Turabian StyleHeise, Christian, Einas Abou Ali, Dirk Hasenclever, Francesco Auriemma, Aiste Gulla, Sara Regner, Sébastien Gaujoux, and Marcus Hollenbach. 2020. "Systematic Review with Meta-Analysis: Endoscopic and Surgical Resection for Ampullary Lesions" Journal of Clinical Medicine 9, no. 11: 3622. https://doi.org/10.3390/jcm9113622