Traction Therapy for Cervical Radicular Syndrome is Statistically Significant but not Clinically Relevant for Pain Relief. A Systematic Literature Review with Meta-Analysis and Trial Sequential Analysis


Abstract
:1. Introduction
2. Methods
2.1. Protocol and Registration
2.2. Search Strategies and Selection Criteria
2.3. Risk of Bias of Included Studies
2.4. Data Extraction
2.5. Data Synthesis
2.6. Trial Sequential Analysis
2.7. Quality of Evidence and Summary of Findings
3. Results
3.1. Study Selection
3.2. Study Characteristics
3.3. Risk of Bias
4. Synthesis of Results
4.1. Traction Versus Sham Traction
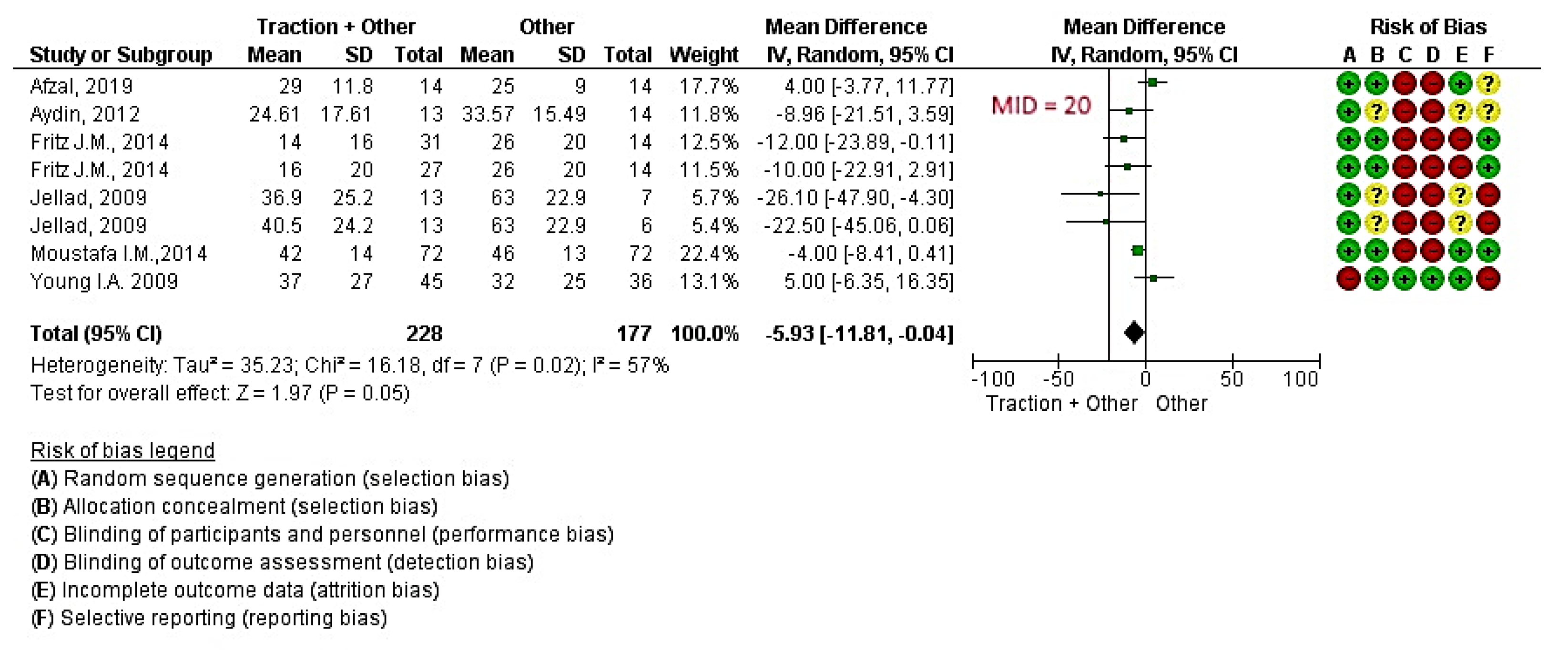
4.2. Traction in Addition to Other Treatments Versus Other Treatments
5. Additional Analysis
5.1. Subgroup Analysis
5.2. Mechanical and Manual Traction
5.3. Continuous Traction and Intermittent Traction
6. Discussion
7. Study Limitations
8. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
Appendix A. Medline Full Search Strategy
References
- Thoomes, E.J.; Scholten-Peeters, W.; Koes, B.; Falla, D.; Verhagen, A.P. The effectiveness of conservative treatment for patients with cervical radiculopathy: A systematic review. Clin. J. Pain. 2013, 29, 1073–1086. [Google Scholar] [CrossRef] [PubMed]
- Wong, J.J.; Côté, P.; Quesnele, J.J.; Stern, P.J.; Mior, S.A. The course and prognostic factors of symptomatic cervical disc herniation with radiculopathy: A systematic review of the literature. Spine J. 2014, 14, 1781–1789. [Google Scholar] [CrossRef] [PubMed]
- Slipman, C.W.; Plastaras, C.T.; Palmitier, R.A.; Huston, C.W.; Sterenfeld, E.B. Symptom provocation of fluoroscopically guided cervical nerve root stimulation. Are dynatomal maps identical to dermatomal maps? Spine 1998, 23, 2235–2242. [Google Scholar] [CrossRef] [PubMed]
- Boyles, R.; Toy, P.; Mellon, J.; Hayes, M.; Hammer, B. Effectiveness of manual physical therapy in the treatment of cervical radiculopathy: A systematic review. J. Man. Manip. Ther. 2011, 19, 135–142. [Google Scholar] [CrossRef] [Green Version]
- Wainner, R.S.; Fritz, J.M.; Irrgang, J.J.; Boninger, M.L.; Delitto, A.; Allison, S. Reliability and diagnostic accuracy of the clinical examination and patient self-report measures for cervical radiculopathy. Spine 2003, 28, 52–62. [Google Scholar] [CrossRef]
- Iyer, S.; Kim, H.J. Cervical radiculopathy. Curr. Rev. Musculoskelet Med. 2016, 9, 272–280. [Google Scholar] [CrossRef]
- Latka, D.; Miekisiak, G.; Jarmuzek, P.; Lachowski, M.; Kaczmarczyk, J. Treatment of degenerative cervical spondylosis with radiculopathy. Clinical practice guidelines endorsed by The Polish Society of Spinal Surgery. Neurol. Neurochir Pol. 2016, 50, 109–113. [Google Scholar] [CrossRef]
- Bono, C.M.; Ghiselli, G.; Gilbert, T.J.; Kreiner, D.S.; Reitman, C.; Summers, J.T.; Jamie, L.; Baisden, M.D.; John Easa, M.D.; Robert Fernand, M.D.; et al. An evidence-based clinical guideline for the diagnosis and treatment of cervical radiculopathy from degenerative disorders. Spine J. 2011, 11, 64–72. [Google Scholar] [CrossRef]
- Liu, W.-J.; Hu, L.; Chou, P.-H.; Wang, J.-W.; Kan, W.-S. Comparison of Anterior Cervical Discectomy and Fusion versus Posterior Cervical Foraminotomy in the Treatment of Cervical Radiculopathy: A Systematic Review. Orthop. Surg. 2016, 8, 425–431. [Google Scholar] [CrossRef]
- Saal, J.S.; Saal, J.A.; Yurth, E.F. Nonoperative Management of Herniated Cervical Intervertebral Disc with Radiculopathy. Spine 1996, 21, 1877–1883. [Google Scholar] [CrossRef] [Green Version]
- Salt, E.; Wright, C.; Kelly, S.; Dean, A. A systematic literature review on the effectiveness of non-invasive therapy for cervicobrachial pain. Man. Ther. 2011, 16, 53–65. [Google Scholar] [CrossRef] [PubMed]
- Fritz, J.M.; Thackeray, A.; Brennan, G.P.; Childs, J.D. Exercise only, exercise with mechanical traction, or exercise with over-door traction for patients with cervical radiculopathy, with or without consideration of status on a previously described subgrouping rule: A randomized clinical trial. J. Orthop. Sports Phys. Ther. 2014, 44, 45–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jellad, A.; Ben Salah, Z.; Boudokhane, S.; Migaou, H.; Bahri, I.; Rejeb, N. The value of intermittent cervical traction in recent cervical radiculopathy. Ann. Phys. Rehabil. Med. 2009, 52, 638–652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, I.A.; Michener, L.A.; Cleland, J.A.; Aguilera, A.J.; Snyder, A.R. Manual therapy, exercise, and traction for patients with cervical radiculopathy: A randomized clinical trial. Phys. Ther. 2009, 89, 632–642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joghataei, M.T.; Arab, A.M.; Khaksar, H. The effect of cervical traction combined with conventional therapy on grip strength on patients with cervical radiculopathy. Clin. Rehabil. 2004, 18, 879–887. [Google Scholar] [CrossRef] [PubMed]
- Moustafa, I.M.; Diab, A.A. Multimodal treatment program comparing 2 different traction approaches for patients with discogenic cervical radiculopathy: A randomized controlled trial. J. Chiropr. Med. 2014, 13, 157–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bukhari, S.R.I.; Shakil-Ur-Rehman, S.; Ahmad, S.; Naeem, A. Comparison between effectiveness of Mechanical and Manual Traction combined with mobilization and exercise therapy in Patients with Cervical Radiculopathy. Pak. J. Med. Sci. 2016, 32, 31–34. [Google Scholar] [PubMed] [Green Version]
- Aydin, N.A.; Yazicioglu, K. Cervical Intermittent Traction: Does it Really Work in Cervical Radiculopathy Due to Herniated Disc? Turk. Fiz. Tip ve Rehabil. Derg. 2012, 58, 277–282. [Google Scholar]
- Yu, H. Clinical Observation on Treatment of Cervical Spondylotic Radiculopathy with Combined Electroacupuncture Tuina and Traction. J. Acupunct. Tuina Sci. 2009, 7, 156–158. [Google Scholar]
- Elnaggar, I.M.; Elhabashy, H.R.; Abd El-Menam, E.M. Influence of Spinal Traction in Treatment of Cervical Radiculopathy. Egypt J. Neurol. Psychiat. Neurosurg. 2009, 46, 455–461. [Google Scholar]
- Atteya, A.A. Biofeedback traction versus conventional traction in cervical radiculopathy. Neurosciences 2004, 9, 91–93. [Google Scholar]
- Klaber Moffett, J.A.; Hughes, G.I.; Griffiths, P. An investigation of the effects of cervical traction. Part 1: Clinical effectiveness. Clin. Rehabil. 1990, 4, 205–211. [Google Scholar] [CrossRef]
- Thoomes, E.J. Effectiveness of manual therapy for cervical radiculopathy, a review. Chiropr. Man. Therap. 2016, 24, 45. [Google Scholar] [CrossRef] [Green Version]
- Rodine, R.J.; Vernon, H. Cervical radiculopathy: A systematic review on treatment by spinal manipulation and measurement with the Neck Disability Index. J. Can. Chiropr. Assoc. 2012, 56, 18–28. [Google Scholar]
- Zhu, L.; Wei, X.; Wang, S. Does cervical spine manipulation reduce pain in people with degenerative cervical radiculopathy? A systematic review of the evidence, and a meta-analysis. Clin. Rehabil. 2016, 30, 145–155. [Google Scholar] [CrossRef] [PubMed]
- Muhammad, U.; Naeem, A.; Badshah, M.; Amjad, I. Effectiveness of cervical traction combined with core muscle strengthening exercises in cervical radiculopathy. J. Public Health Biol. Sci. 2012, 1, 115–120. [Google Scholar]
- Leininger, B.; Bronfort, G.; Evans, R.; Reiter, T. Spinal manipulation or mobilization for radiculopathy: A systematic review. Phys. Med. Rehabil. Clin. 2011, 22, 105–125. [Google Scholar] [CrossRef]
- Afzal, R.; Ghous, M.; Shakil Ur Rehman, S.; Masood, T. Comparison between Manual Traction, Manual Opening technique and Combination in Patients with cervical radiculopathy: Randomized Control Trial. J. Pak. Med. Assoc. 2019, 69, 1237–1241. [Google Scholar]
- Raney, N.H.; Petersen, E.J.; Smith, T.A.; James, E.; Cowan, J.E.; Daniel, D.G.; Childs, J.D. Development of a clinical prediction rule to identify patients with neck pain likely to benefit from cervical traction and exercise. Eur. Spine J. 2009, 18, 382–391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graham, N.; Gross, A.R.; Goldsmith, C.; BHScPT, A.R.G. Mechanical traction for mechanical neck disorders: A systematic review. J. Rehabil. Med. 2006, 38, 145–152. [Google Scholar] [CrossRef] [Green Version]
- Graham, N.; Gross, A.; Goldsmith, C.H.; Klaber Moffett, J.; Haines, T.; Burnie, S.J.; Peloso, P.M.J. Mechanical traction for neck pain with or without radiculopathy. Cochrane Database Syst. Rev. 2008, 16, CD006408. [Google Scholar] [CrossRef] [PubMed]
- Clarke, J.A.; van Tulder, M.W.; Blomberg, S.E.I.; de Vet, H.C.W.; van der Heijden, G.J.M.G.; Bronfort, G. Traction for low-back pain with or without sciatica. Cochrane Database Syst. Rev. 2005, 19, CD003010. [Google Scholar]
- Romeo, A.; Vanti, C.; Boldrini, V.; Ruggeri, M.; Guccione, A.A.; Pillastrini, P.; Bertozzi, L. Cervical Radiculopathy: Effectiveness of Adding Traction to Physical Therapy. A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Phys. Ther. 2018, 98, 231–242. [Google Scholar] [CrossRef]
- GRADEpro GDT: GRADEpro Guideline Development Tool [Software]. McMaster University, 2020 (developed by Evidence Prime, Inc.). Available online: gradepro.org (accessed on 20 May 2020).
- Ryan, R.; Hill, S. How to GRADE the Quality of the Evidence. Cochrane Consumers and Communication Group. Version 3.0. 2016. Available online: http://cccrg.cochrane.org/author-resources (accessed on 20 May 2020).
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Rind, D.; Devereaux, P.J.; Montorih, V.M.; Freyschuss, B.; Vist, G.; et al. GRADE guidelines 6. Rating the quality of evidence--imprecision. J. Clin. Epidemiol. 2011, 64, 1283–1293. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Altman, D.G.; Sterne, J.A.C. Chapter 8: Assessing risk of bias in included studies. In Higgins JPT; Green, S., Ed.; The Cochrane Collaboration; John Wiley & Sons: New York, NY, USA, 2011; Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0.; Available online: www.cochrane-handbook.org (accessed on 16 March 2020).
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deeks, J.J.; Higgins, J.P.T.; Altman, D.G. Chapter 9: Analysing data and undertaking meta-analyses. In Higgins JPT; Green, S., Ed.; The Cochrane Collaboration; John Wiley & Sons: New York, NY, USA, 2011; pp. 229–240. [Google Scholar]
- Deeks, J.J.; Altman, D.G. Chapter 16: Special Topics in Statistics; Deeks, J.J., Altman, D.G., Eds.; The Cochrane Collaboration; John Wiley & Sons: New York, NY, USA, 2011; pp. 433–449. [Google Scholar]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials. 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Review Manager (RevMan) Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014. Available online: https://training.cochrane.org/sites/training.cochrane.org/files/public/uploads/resources/downloadable_resources/English/RevMan_5.3_User_Guide.pdf (accessed on 20 May 2020).
- Thorlund, K.; Wetterslev, J.; Awad, T.; Thabane, L.; Gluud, C. Comparison of statistical inferences from the DerSimonian-Laird and alternative random-effects model meta-analyses—an empirical assessment of 920 Cochrane primary outcome meta-analyses. Res. Synth. Methods 2011, 2, 238–253. [Google Scholar] [CrossRef]
- Thorlund, K.E.J.; Wetterslev, J.; Brok, J.; Imberger, G.; Gluud, C. User Manual for Trial Sequential Analysis (TSA). 2011. Available online: http://www.ctu.dk/tsa/files/tsa_manual.pdf (accessed on 25 May 2020).
- Ostelo, R.W.J.G.; Deyo, R.A.; Stratford, P.; Waddell, G.; Croft, P.; Von Korff, M.; Bouter, L.M.; de Vet, H.C. Interpreting change scores for pain and functional status in low back pain: Towards international consensus regarding minimal important change. Spine 2008, 33, 90–94. [Google Scholar] [CrossRef] [Green Version]
- Copenhagen Trial Unit; Thorlund, K.; Engstrøm, J.; Wetterslev, J.; Brok, J.; Imberger, G.; Gluud, C. Software for Trial Sequential Analysis (TSA) ver. 0.9.5.5 Beta. Copenhagen Trial Unit, Centre for Clinical Intervention Research, Copenhagen, Denmark, Free-Ware. Available online: http://www.ctu.dk/tsa/ (accessed on 2 June 2018).
- Schünemann, H.J.; Oxman, A.D.; Higgins, J.P.T.; Vist, G.E.; Glasziou, P.; Guyatt, G.H. Chapter 11: Presenting results and ‘Summary of findings’ tables. In Higgins JPT; Green, S., Ed.; The Cochrane Collaboration, 2011; Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011); Available online: www.handbook.cochrane.org (accessed on 25 May 2020).
- Goldsmith, E.S.; Taylor, B.C.; Greer, N.; Murdoch, M.; MacDonald, R.; McKenzie, L.; Rosebush, C.E.; Wilt MD, T.J. Focused Evidence Review: Psychometric Properties of Patient-Reported Outcome Measures for Chronic Musculoskeletal Pain. J. Gen. Intern. Med. 2018, 33 (Suppl. 1), 61–70. [Google Scholar] [CrossRef] [Green Version]
- Boutron, I.; Altman, D.G.; Moher, D.; Schulz, K.F.; Ravaud, P. CONSORT Statement for Randomized Trials of Nonpharmacologic Treatments: A 2017 Update and a CONSORT Extension for Nonpharmacologic Trial Abstracts. Ann. Intern. Med. 2017, 167, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Woolf, C.J. Central sensitization: Implications for the diagnosis and treatment of pain. Pain 2011, 152 (Suppl. 3), S2–S15. [Google Scholar] [CrossRef] [PubMed]
- Matre, D.; Knardahl, S. Central sensitization in chronic neck/shoulder pain. Scand. J. Pain 2012, 3, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Graven-Nielsen, T.; Arendt-Nielsen, L. Peripheral and central sensitization in musculoskeletal pain disorders: An experimental approach. Curr. Rheumatol. Rep. 2002, 4, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Del Grande, F.; Maus, T.P.; Carrino, J.A. Imaging the intervertebral disk: Age-related changes, herniations, and radicular pain. Radiol. Clin. North Am. 2012, 50, 629–649. [Google Scholar] [CrossRef] [PubMed]
- Hróbjartsson, A.; Kaptchuk, T.J.; Miller, F.G. Placebo effect studies are susceptible to response bias and to other types of biases. J. Clin. Epidemiol. 2011, 64, 1223–1229. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | Study Design | Country | Diagnostic Criteria | Intervention Group | Control Group | Outcome Measure Considered (Follow Up) | Sample Size (Drop Out) |
|---|---|---|---|---|---|---|---|
| Afzal R., 2019 | RCT | Pakistan | Clinic criteria: unilateral upper extremity pain, paresthesia, or numbness, and at least 3/4 positive test of Wainner’s cluster. Imaging: MR diagnosis of radiculopathy. | I1: Manual opening technique + manual intermittent traction 10 min, 25° cervical flexion, 10 s tension/5 s relaxation. I2: Manual intermittent traction 10 min, 25° cervical flexion, 10 s tension/5 s relaxation. | C: Manual opening technique pull the neck to rotation at the restriction improving rotation and performing opening 3 sets of 10 repetitions | NPRS 0–10 (3 weeks) | 40 (1) |
| Fritz J.M., 2014 | RCT | Utah, USA | Clinic criteria: neck pain associated with pain or numbness distally to a/c joint or caudal to superior edge of scapulae. | I1: Physiotherapy + mechanical intermittent traction 15 min, 15° cervical flexion, 60 s tension/20 s relaxation. I2: Physiotherapy + over-door mechanical continuous traction 15 min, sitting. | C: Physiotherapy scapular strengthening 3 × 10 rep., cranio-cervical strengthening 10 × 10 s | NPRS 0–10 (4 weeks) | 86 (32) |
| Young I.A., 2009 | RCT | Georgia | Clinic criteria: pain, numbness to an arm and at least 3/4 positive test of Wainner’s cluster. | I1: Physiotherapy + mechanical intermittent traction-dorsal thrust mid and high, P-A glide, retraction, rotation, lateral glide in ULTT1, P-A glide, strengthening exercise-traction 15 min, 15° cervical flexion, 50 s tension/10 s relaxation. | C: Physiotherapy + sham traction-dorsal thrust mid and high, P-A glide, retraction, rotation, lateral glide in ULTT1, P-A glide, strengthening exercise-sham traction. | NPRS 0–10 (4 weeks) | 81 (12) |
| Moustafa I.M., 2014 | RCT | Egypt | Clinic criteria: neurological exams, exacerbated symptoms in flexion, protraction and reduction of symptoms in retraction, extension, side homolateral side-bending and positive Wainner’s cluster (4/4). Imaging: unilateral hernia C5-C6, C6-C7 confirmed by MR and CT. | I1: Physiotherapy, MT + mechanical intermittent traction, 50 s tension/10 s relaxation 24° flexion. I2: Physiotherapy, MT + FCR H reflex traction. | C: Physiotherapy, TM (laser, TENS, STM, Dorsal thrust, cervical flexor and scapular muscle strengthening. | VAS 0–10 (4 weeks) | 216 (27) |
| Aydin, 2012 | RCT | Turkey | Clinic criteria: neurological exam and positive neurotension and spurling test. Imaging: MR. | I1: Physiotherapy + mechanical intermittent traction 7 s tension, 5 s relaxation. | C: Physiotherapy, US, hot packs, TENS, isometric exercise for cervical extensor and flexor, stretching. | VAS 0–100 (3 weeks) | 27 (/) |
| Klaber Moffet J.A., 1990 | RCT | England | Clinic criteria: typical symptomatology: | I1: Mechanical continuous traction 25° flexion. | C: Sham traction. | NPRS 0–10 (4 weeks) | 100 (/) |
| Jellad, 2009 | RCT | Tunisia | Clinic criteria: typical symptomatology. Imaging: involvement of spinal nerve with herniated disc and/or intervertebral disc degeneration by CT or MR. | I1: Physiotherapy + manual intermittent traction 20 repetitions, 20 s tension/10 s relaxation, most pain-free position. I2: Physiotherapy + mechanical continuous traction 2 sessions of 25 min, 10 min rest intra-session, most pain-free position. | C: Physiotherapy US, infrared, massage, cervical spine mobilization, muscle strengthening via isometric contraction of flexor and extensor muscles, stretching exercises. | VAS 0–100 (4 weeks) | 39 (/) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colombo, C.; Salvioli, S.; Gianola, S.; Castellini, G.; Testa, M. Traction Therapy for Cervical Radicular Syndrome is Statistically Significant but not Clinically Relevant for Pain Relief. A Systematic Literature Review with Meta-Analysis and Trial Sequential Analysis. J. Clin. Med. 2020, 9, 3389. https://doi.org/10.3390/jcm9113389
Colombo C, Salvioli S, Gianola S, Castellini G, Testa M. Traction Therapy for Cervical Radicular Syndrome is Statistically Significant but not Clinically Relevant for Pain Relief. A Systematic Literature Review with Meta-Analysis and Trial Sequential Analysis. Journal of Clinical Medicine. 2020; 9(11):3389. https://doi.org/10.3390/jcm9113389
Chicago/Turabian StyleColombo, Claudio, Stefano Salvioli, Silvia Gianola, Greta Castellini, and Marco Testa. 2020. "Traction Therapy for Cervical Radicular Syndrome is Statistically Significant but not Clinically Relevant for Pain Relief. A Systematic Literature Review with Meta-Analysis and Trial Sequential Analysis" Journal of Clinical Medicine 9, no. 11: 3389. https://doi.org/10.3390/jcm9113389