Drug-Induced Interstitial Lung Disease: A Systematic Review

 , , ,
, , ,
Abstract
:1. Introduction
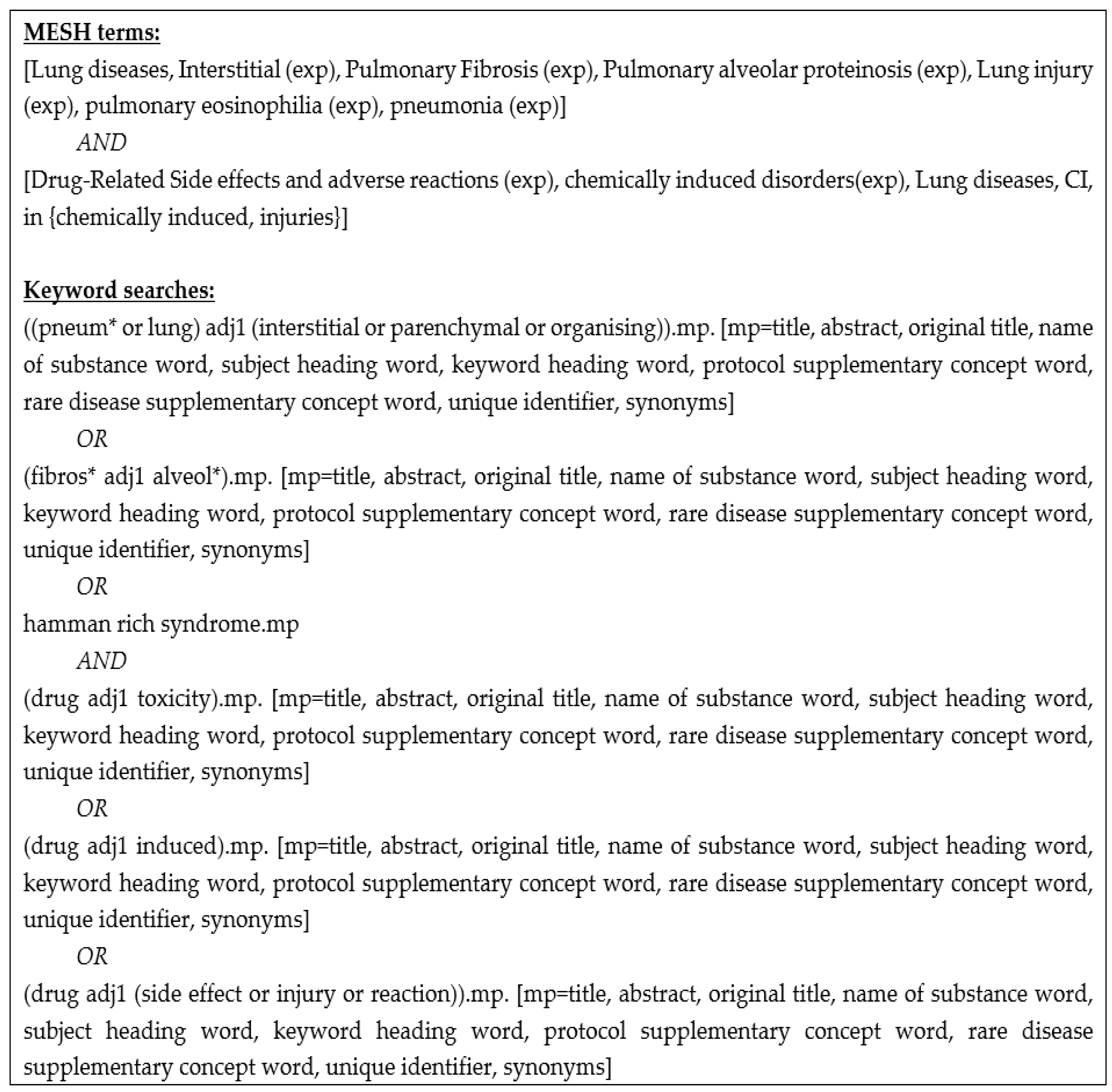
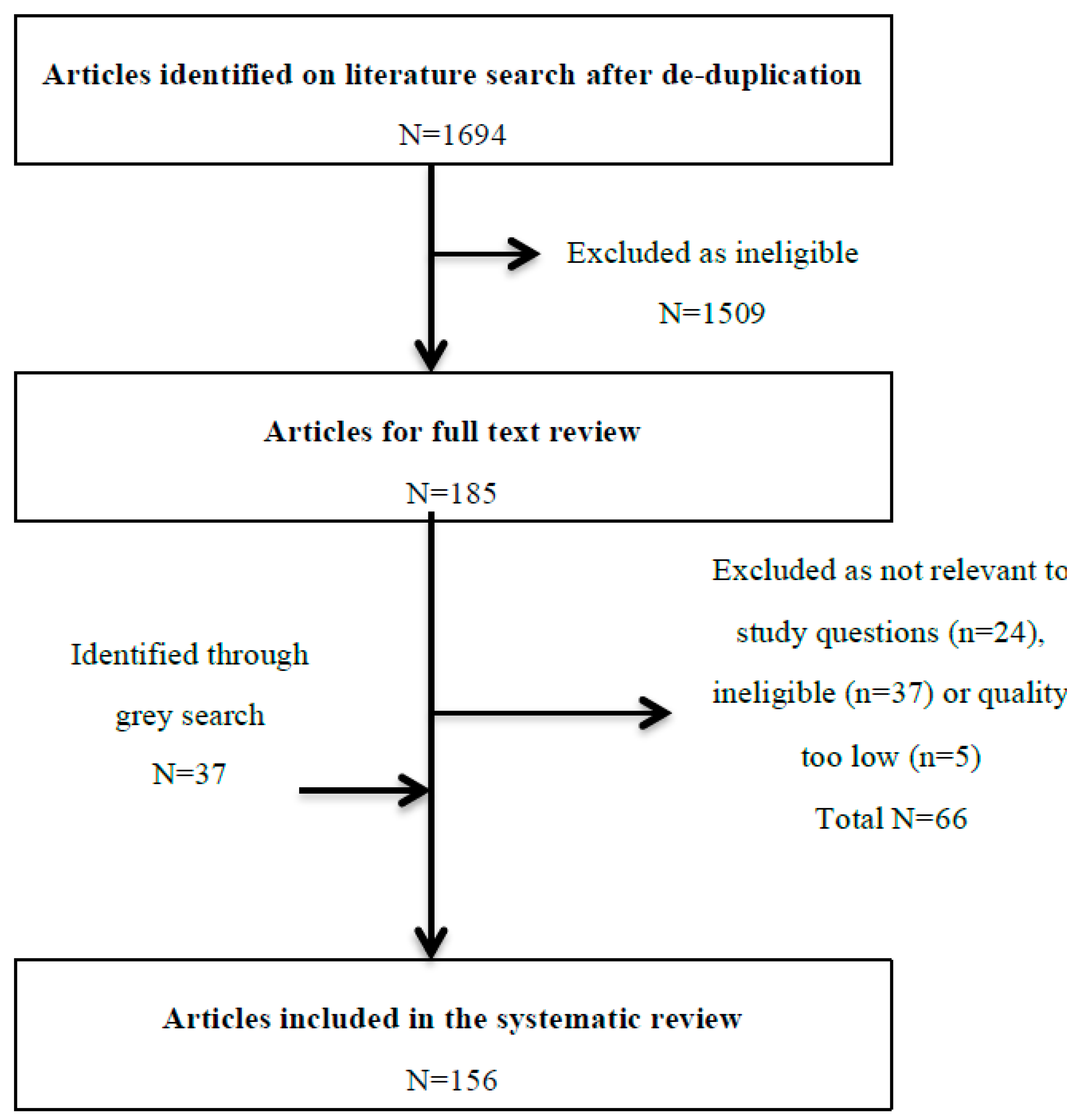
2. Methods
3. Results
3.1. Incidence and Prevalence
3.2. Common Causative Drugs
3.2.1. Cancer Therapy
Bleomycin
Gemcitabine
Epidermal Growth Factor Receptor (EGFR)-Targeted Agents
Mechanistic Target of Rapamycin Protein (MTOR) Inhibitors
Immune Checkpoint Inhibitors
3.2.2. Rheumatological Therapy
Methotrexate (MTX)
Leflunomide
Biological DMARDs
3.2.3. Other Drug Classes
Antibiotics
Amiodarone
3.3. Risk Factors for the Development of DIILD
3.4. Radiological Investigation of DIILD and Prevalent Radiopathological Patterns
3.5. Non-Imaging Diagnostic Investigations
3.5.1. Pulmonary Physiology
3.5.2. Bronchoalveolar Lavage (BAL)
3.5.3. Lung Biopsy
3.5.4. Circulating Biomarkers
3.6. The Role of Glucocorticoids (GCs) in the Treatment of DIILD
3.6.1. Efficacy
3.6.2. GC Dose and Duration
3.6.3. DIILD Subsets and GC Responses
3.7. Prognosis
Factors Predicting Mortality
4. Discussion
- (i)
- A standardised case definition for the study of DIILD to be used in clinical trials and observational studies.
- (ii)
- Validation of better biomarkers for detecting early DIILD and discriminating from other causes of ILD.
- (iii)
- An evidence base for the management of DIILD, including through clinical trials to the efficacy and optimal dosing of GCs in DIILD.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Travis, W.D.; Costabel, U.; Hansell, D.M.; King, T.E., Jr.; Lynch, D.A.; Nicholson, A.G.; Ryerson, C.J.; Ryu, J.H.; Selman, M.I.; Wells, A.U.; et al. An official American Thoracic Society/European Respiratory Society statement: Update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am. J. Respir. Crit. Care Med. 2013, 188, 733–748. [Google Scholar] [CrossRef] [PubMed]
- Cancer Therapy Evaluation Program DoCTaDNCINIoH. Common Terminology Criteria for Adverse Events [Internet]. Version 5.0. 27-11-2017. Available online: http://ctep.cancer.gov (accessed on 13 October 2018).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Schunemann, H.J.; Tugwell, P.; Knottnerus, A. GRADE guidelines: A new series of articles in the Journal of Clinical Epidemiology. J. Clin. Epidemiol. 2011, 64, 380–382. [Google Scholar] [CrossRef] [PubMed]
- Koo, L.C.; Clark, J.A.; Quesenberry, C.P.; Higenbottam, T.; Nyberg, F.; Wolf, M.K.; Steinberg, M.H.; Forsythe, B.H. National differences in reporting ‘pneumonia’ and ‘pneumonia interstitial’: An analysis of the WHO International Drug Monitoring Database on 15 drugs in nine countries for seven pulmonary conditions. Pharmacoepidemiol. Drug Saf. 2005, 14, 775–787. [Google Scholar] [CrossRef] [PubMed]
- Bate, A.; Evans, S.J. Quantitative signal detection using spontaneous ADR reporting. Pharmacoepidemiol. Drug Saf. 2009, 18, 427–436. [Google Scholar] [CrossRef] [PubMed]
- Amar, R.K.; Jick, S.S.; Rosenberg, D.; Maher, T.M.; Meier, C.R. Drug-/radiation-induced interstitial lung disease in the United Kingdom general population: Incidence, all-cause mortality and characteristics at diagnosis. Respirology 2012, 17, 861–868. [Google Scholar] [CrossRef] [PubMed]
- Duchemann, B.; Annesi-Maesano, I.; de Jacobe, N.C.; Sanyal, S.; Brillet, P.Y.; Brauner, M.; Kambouchner, M.; Huynh, S.; Naccache, J.M.; Borie, R.; et al. Prevalence and incidence of interstitial lung diseases in a multi-ethnic county of Greater Paris. Eur. Respir. J. 2017, 50, 1602419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coultas, D.B.; Zumwalt, R.E.; Black, W.C.; Sobonya, R.E. The epidemiology of interstitial lung diseases. Am. J. Respir. Crit. Care Med. 1994, 150, 967–972. [Google Scholar] [CrossRef] [PubMed]
- Roelandt, M.; Demedts, M.; Callebaut, W.; Coolen, D.; Slabbynck, H.; Bockaert, J.; Kips, J.; Brie, J.; Ulburghs, M.; de Boeck, K.; et al. Epidemiology of interstitial lung disease (ILD) in flanders: Registration by pneumologists in 1992–1994. Working group on ILD, VRGT. Vereniging voor Respiratoire Gezondheidszorg en Tuberculosebestrijding. Acta Clin. Belg. 1995, 50, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Hyldgaard, C.; Hilberg, O.; Muller, A.; Bendstrup, E. A cohort study of interstitial lung diseases in central Denmark. Respir. Med. 2014, 108, 793–799. [Google Scholar] [CrossRef] [PubMed]
- Kakugawa, T.; Yokota, S.; Ishimatsu, Y.; Hayashi, T.; Nakashima, S.; Hara, S.; Sakamoto, N.; Matsuoka, Y.; Kubota, H.; Mine, M.; et al. Serum heat shock protein 47 levels in patients with drug-induced lung disease. Respir. Res. 2013, 14, 133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tamura, M.; Saraya, T.; Fujiwara, M.; Hiraoka, S.; Yokoyama, T.; Yano, K.; Ishii, H.; Furuse, J.; Goya, T.; Takizawa, H.; et al. High-resolution computed tomography findings for patients with drug-induced pulmonary toxicity, with special reference to hypersensitivity pneumonitis-like patterns in gemcitabine-induced cases. Oncologist 2013, 18, 454–459. [Google Scholar] [CrossRef] [PubMed]
- Ohnishi, H.; Yokoyama, A.; Yasuhara, Y.; Watanabe, A.; Naka, T.; Hamada, H.; Abe, M.; Nishimura, K.; Higaki, J.; Ikezoe, J.; et al. Circulating KL-6 levels in patients with drug induced pneumonitis. Thorax 2003, 58, 872–875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piciucchi, S.; Romagnoli, M.; Chilosi, M.; Bigliazzi, C.; Dubini, A.; Beomonte, Z.B.; Gavelli, G.; Carloni, A.; Poletti, V. Prospective evaluation of drug-induced lung toxicity with high-resolution CT and transbronchial biopsy. Radiol. Med. 2011, 116, 246–263. [Google Scholar] [CrossRef] [PubMed]
- Romagnoli, M.; Bigliazzi, C.; Casoni, G.; Chilosi, M.; Carloni, A.; Dubini, A.; Gurioli, C.; Tomassetti, S.; Gurioli, C.; Poletti, V. The role of transbronchial lung biopsy for the diagnosis of diffuse drug-induced lung disease: A case series of 44 patients. Sarcoidosis Vasc. Diffuse Lung Dis. 2008, 25, 36–45. [Google Scholar] [PubMed]
- Akira, M.; Ishikawa, H.; Yamamoto, S. Drug-induced pneumonitis: Thin-section CT findings in 60 patients. Radiology 2002, 224, 852–860. [Google Scholar] [CrossRef] [PubMed]
- Blum, R.H.; Carter, S.K.; Agre, K. A clinical review of bleomycin—A new antineoplastic agent. Cancer 1973, 31, 903–914. [Google Scholar] [CrossRef]
- Delanoy, N.; Pecuchet, N.; Fabre, E.; Combe, P.; Juvin, K.; Pujade-Lauraine, E.; Oudard, S. Bleomycin-Induced Pneumonitis in the Treatment of Ovarian Sex Cord-Stromal Tumors: A Systematic Review and Meta-analysis. Int. J. Gynecol. Cancer 2015, 25, 1593–1598. [Google Scholar] [CrossRef] [PubMed]
- Hubbard, S.P.; Chabner, B.A.; Canellos, G.P.; Young, R.C.; DeVita, V.T., Jr. High dose intravenous bleomycin in the treatment of advanced lymphomas. Eur. J. Cancer 1975, 11, 623–626. [Google Scholar] [CrossRef]
- Ngeow, J.; Tan, I.B.; Kanesvaran, R.; Tan, H.C.; Tao, M.; Quek, R.; Lim, S.T. Prognostic impact of bleomycin-induced pneumonitis on the outcome of Hodgkin’s lymphoma. Ann. Hematol. 2011, 90, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Stamatoullas, A.; Brice, P.; Bouabdallah, R.; Mareschal, S.; Camus, V.; Rahal, I.; Franchi, P.; Lanic, H.; Tilly, H. Outcome of patients older than 60 years with classical Hodgkin lymphoma treated with front line ABVD chemotherapy: Frequent pulmonary events suggest limiting the use of bleomycin in the elderly. Br. J. Haematol. 2015, 170, 179–184. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, J.M.; Huddart, R.A.; Norman, A.R.; Nicholls, J.; Dearnaley, D.P.; Horwich, A. Predicting the risk of bleomycin lung toxicity in patients with germ-cell tumours. Ann. Oncol. 2003, 14, 91–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, P.; Federico, M.; Kirkwood, A.; Fossa, A.; Berkahn, L.; Carella, A.; d’Amore, F.; Enblad, G.; Franceschetto, A.; Fulham, M.; et al. Adapted Treatment Guided by Interim PET-CT Scan in Advanced Hodgkin’s Lymphoma. N. Engl. J. Med. 2016, 374, 2419–2429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Hu, G.F.; Zhang, Q.Q.; Tang, N.; Guo, J.; Liu, L.Y.; Han, X.; Wang, X.; Wang, Z. Efficacy and safety of gemcitabine plus erlotinib for locally advanced or metastatic pancreatic cancer: A systematic review and meta-analysis. Drug Des. Dev. Ther. 2016, 10, 1961–1972. [Google Scholar] [CrossRef] [PubMed]
- Sahin, I.H.; Geyer, A.I.; Kelly, D.W.; O’Reilly, E.M. Gemcitabine-Related Pneumonitis in Pancreas Adenocarcinoma—An Infrequent Event: Elucidation of Risk Factors and Management Implications. Clin. Colorectal. Cancer 2016, 15, 24–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Z.Y.; Yuan, J.Q.; Di, M.Y.; Zheng, D.Y.; Chen, J.Z.; Ding, H.; Wu, X.Y.; Huang, Y.-F.; Mao, C.; Tang, J.-L. Gemcitabine plus erlotinib for advanced pancreatic cancer: A systematic review with meta-analysis. PLoS ONE 2013, 8, e57528. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, S.; Hanna, N.; Ansari, R.; Pletcher, W.; Einhorn, L.; Ng, E.; Sandlere, A. A phase II study of weekly gemcitabine and paclitaxel in patients with previously untreated stage IIIb and IV non-small cell lung cancer. Lung Cancer 2002, 38, 73–77. [Google Scholar] [CrossRef]
- Kouroussis, C.; Mavroudis, D.; Kakolyris, S.; Voloudaki, A.; Kalbakis, K.; Souglakos, J.; Agelaki, S.; Malas, K.; Bozionelou, V.; Georgoulias, V. High incidence of pulmonary toxicity of weekly docetaxel and gemcitabine in patients with non-small cell lung cancer: Results of a dose-finding study. Lung Cancer 2004, 44, 363–368. [Google Scholar] [CrossRef] [PubMed]
- Hamada, T.; Yasunaga, H.; Nakai, Y.; Isayama, H.; Matsui, H.; Fushimi, K.; Koike, K. Interstitial lung disease associated with gemcitabine: A Japanese retrospective cohort study. Respirology 2016, 21, 338–343. [Google Scholar] [CrossRef] [PubMed]
- Friedberg, J.W.; Neuberg, D.; Kim, H.; Miyata, S.; McCauley, M.; Fisher, D.C.; Takvorian, T.; Canellos, G.P. Gemcitabine added to doxorubicin, bleomycin, and vinblastine for the treatment of de novo Hodgkin disease: Unacceptable acute pulmonary toxicity. Cancer 2003, 98, 978–982. [Google Scholar] [CrossRef] [PubMed]
- Umemura, S.; Yamane, H.; Suwaki, T.; Katoh, T.; Yano, T.; Shiote, Y.; Takigawa, N.; Kiura, K.; Kamei, H. Interstitial lung disease associated with gemcitabine treatment in patients with non-small-cell lung cancer and pancreatic cancer. J. Cancer Res. Clin. Oncol. 2011, 137, 1469–1475. [Google Scholar] [CrossRef] [PubMed]
- Osawa, M.; Kudoh, S.; Sakai, F.; Endo, M.; Hamaguchi, T.; Ogino, Y.; Yoneoka, M.; Sakaguchi, M.; Nishimoto, H.; Gemma, A. Clinical features and risk factors of panitumumab-induced interstitial lung disease: A postmarketing all-case surveillance study. Int. J. Clin. Oncol. 2015, 20, 1063–1071. [Google Scholar] [CrossRef] [PubMed]
- Gemma, A.; Kudoh, S.; Ando, M.; Ohe, Y.; Nakagawa, K.; Johkoh, T.; Yamazaki, N.; Arakawa, H.; Inoue, Y.; Ebina, M.; et al. Final safety and efficacy of erlotinib in the phase 4 POLARSTAR surveillance study of 10,708 Japanese patients with non-small-cell lung cancer. Cancer Sci. 2014, 105, 1584–1590. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Tang, J.; Tong, L.; Liu, Z. Risk of interstitial lung disease with gefitinib and erlotinib in advanced non-small cell lung cancer: A systematic review and meta-analysis of clinical trials. Lung Cancer 2014, 83, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Qi, W.X.; Sun, Y.J.; Shen, Z.; Yao, Y. Risk of interstitial lung disease associated with EGFR-TKIs in advanced non-small-cell lung cancer: A meta-analysis of 24 phase III clinical trials. J. Chemother. 2015, 27, 40–51. [Google Scholar] [CrossRef] [PubMed]
- Kudoh, S.; Kato, H.; Nishiwaki, Y.; Fukuoka, M.; Nakata, K.; Ichinose, Y.; Tsuboi, M.; Yokota, S.; Nakagawa, K.; Suga, M.; et al. Interstitial lung disease in Japanese patients with lung cancer: A cohort and nested case-control study. Am. J. Respir. Crit. Care Med. 2008, 177, 1348–1357. [Google Scholar] [CrossRef] [PubMed]
- Ishiguro, M.; Watanabe, T.; Yamaguchi, K.; Satoh, T.; Ito, H.; Seriu, T.; Sakata, Y.; Sugihara, K. A Japanese post-marketing surveillance of cetuximab (Erbitux(R)) in patients with metastatic colorectal cancer. Jpn. J. Clin. Oncol. 2012, 42, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Boku, N.; Sugihara, K.; Kitagawa, Y.; Hatake, K.; Gemma, A.; Yamazaki, N.; Muro, K.; Hamaguchi, T.; Yoshino, T.; Yana, I.; et al. Panitumumab in Japanese patients with unresectable colorectal cancer: A post-marketing surveillance study of 3085 patients. Jpn. J. Clin. Oncol. 2014, 44, 214–223. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.T.; Chen, M.H.; Chen, J.S.; Chen, L.T.; Shan, Y.S.; Lu, C.H.; Su, Y.-L.; Ku, F.-C.; Chou, W.-C.; Chen, Y.-Y. The efficacy and safety of everolimus for the treatment of progressive gastroenteropancreatic neuroendocrine tumors: A multi-institution observational study in Taiwan. Asia Pac. J. Clin. Oncol. 2016, 12, 396–402. [Google Scholar] [CrossRef] [PubMed]
- Solazzo, A.; Botta, C.; Nava, F.; Baisi, A.; Bonucchi, D.; Cappelli, G. Interstitial Lung Disease After Kidney Transplantation and the Role of Everolimus. Transplant. Proc. 2016, 48, 349–351. [Google Scholar] [CrossRef] [PubMed]
- Nishino, M.; Brais, L.K.; Brooks, N.V.; Hatabu, H.; Kulke, M.H.; Ramaiya, N.H. Drug-related pneumonitis during mammalian target of rapamycin inhibitor therapy in patients with neuroendocrine tumors: A radiographic pattern-based approach. Eur. J. Cancer 2016, 53, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Nishino, M.; Boswell, E.N.; Hatabu, H.; Ghobrial, I.M.; Ramaiya, N.H. Drug-Related Pneumonitis During Mammalian Target of Rapamycin Inhibitor Therapy: Radiographic Pattern-Based Approach in Waldenstrom Macroglobulinemia as a Paradigm. Oncologist 2015, 20, 1077–1083. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duran, I.; Siu, L.L.; Oza, A.M.; Chung, T.B.; Sturgeon, J.; Townsley, C.A.; Pond, G.R.; Seymour, L.; Niroumand, M. Characterisation of the lung toxicity of the cell cycle inhibitor temsirolimus. Eur. J. Cancer 2006, 42, 1875–1880. [Google Scholar] [CrossRef] [PubMed]
- White, D.A.; Camus, P.; Endo, M.; Escudier, B.; Calvo, E.; Akaza, H.; Uemura, H.; Kpamegan, E.; Kay, A.; Robson, M.; et al. Noninfectious pneumonitis after everolimus therapy for advanced renal cell carcinoma. Am. J. Respir. Crit. Care Med. 2010, 182, 396–403. [Google Scholar] [CrossRef] [PubMed]
- Iacovelli, R.; Palazzo, A.; Mezi, S.; Morano, F.; Naso, G.; Cortesi, E. Incidence and risk of pulmonary toxicity in patients treated with mTOR inhibitors for malignancy. A meta-analysis of published trials. Acta Oncol. 2012, 51, 873–879. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maroto, J.P.; Hudes, G.; Dutcher, J.P.; Logan, T.F.; White, C.S.; Krygowski, M.; Cincotta, M.; Shapiro, M.; Duran, I.; Berkenblit, A. Drug-related pneumonitis in patients with advanced renal cell carcinoma treated with temsirolimus. J. Clin. Oncol. 2011, 29, 1750–1756. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Moreno, A.; Ridao, N.; Garcia-Ledesma, P.; Calvo, N.; Perez-Flores, I.; Marques, M.; Barrientos, A.; Sánchez-Fructuoso, A.I. Sirolimus and everolimus induced pneumonitis in adult renal allograft recipients: Experience in a center. Transplant. Proc. 2009, 41, 2163–2165. [Google Scholar] [CrossRef] [PubMed]
- Baas, M.C.; Struijk, G.H.; Moes, D.J.; Van den Berk, I.A.; Jonkers, R.E.; De Fijter, J.W.; van der Heide, J.J.H.; van Dijk, M.; ten Berge, I.J.M.; Bemelman, F.J. Interstitial pneumonitis caused by everolimus: A case-cohort study in renal transplant recipients. Transpl. Int. 2014, 27, 428–436. [Google Scholar] [CrossRef] [PubMed]
- Hodi, F.S.; O’Day, S.J.; McDermott, D.F.; Weber, R.W.; Sosman, J.A.; Haanen, J.B.; Gonzalez, R.; Robert, C.; Schadendorf, D.; Hassel, J.C.; et al. Improved survival with ipilimumab in patients with metastatic melanoma. N. Engl. J. Med. 2010, 363, 711–723. [Google Scholar] [CrossRef] [PubMed]
- Delaunay, M.; Cadranel, J.; Lusque, A.; Meyer, N.; Gounant, V.; Moro-Sibilot, D.; Michot, J.-M.; Raimbourg, J.; Girard, N.; Guisier, F.; et al. Immune-checkpoint inhibitors associated with interstitial lung disease in cancer patients. Eur. Respir. J. 2017, 50, 1700050. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khunger, M.; Rakshit, S.; Pasupuleti, V.; Hernandez, A.V.; Mazzone, P.; Stevenson, J.; Pennell, N.A.; Velcheti, V. Incidence of Pneumonitis with Use of Programmed Death 1 and Programmed Death-Ligand 1 Inhibitors in Non-Small Cell Lung Cancer: A Systematic Review and Meta-Analysis of Trials. Chest 2017, 152, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Nishino, M.; Giobbie-Hurder, A.; Hatabu, H.; Ramaiya, N.H.; Hodi, F.S. Incidence of Programmed Cell Death 1 Inhibitor-Related Pneumonitis in Patients with Advanced Cancer: A Systematic Review and Meta-analysis. JAMA Oncol. 2016, 2, 1607–1616. [Google Scholar] [CrossRef] [PubMed]
- Wolchok, J.D.; Chiarion-Sileni, V.; Gonzalez, R.; Rutkowski, P.; Grob, J.J.; Cowey, C.L.; Lao, C.D.; Wagstaff, J.; Schadendorf, D.; Ferrucci, P.F.; et al. Overall Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2017, 377, 1345–1356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conway, R.; Low, C.; Coughlan, R.J.; O’Donnell, M.J.; Carey, J.J. Methotrexate and lung disease in rheumatoid arthritis: A meta-analysis of randomized controlled trials. Arthritis Rheumatol. 2014, 66, 803–812. [Google Scholar] [CrossRef] [PubMed]
- Drosos, A.A.; Psychos, D.; Andonopoulos, A.P.; Stefanaki-Nikou, S.; Tsianos, E.B.; Moutsopoulos, H.M. Methotrexate therapy in rheumatoid arthritis: A two year prospective follow-up. Clin. Rheumatol. 1990, 9, 333–341. [Google Scholar] [CrossRef] [PubMed]
- Conway, R.; Low, C.; Coughlan, R.J.; O’Donnell, M.J.; Carey, J.J. Methotrexate use and risk of lung disease in psoriasis, psoriatic arthritis, and inflammatory bowel disease: Systematic literature review and meta-analysis of randomised controlled trials. BMJ 2015, 350, 1269. [Google Scholar] [CrossRef] [PubMed]
- Alarcon, G.S.; Kremer, J.M.; Macaluso, M.; Weinblatt, M.E.; Cannon, G.W.; Palmer, W.R.; St. Clair, E.W.; Sundy, J.S.; Alexander, R.W.; Smith, G.J.W.; et al. Risk factors for methotrexate-induced lung injury in patients with rheumatoid arthritis. A multicenter, case-control study. Methotrexate-Lung Study Group. Ann. Intern. Med. 1997, 127, 356–364. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Provenzale, D.; McKusick, A.; Kaplan, M.M. Interstitial pneumonitis after low-dose methotrexate therapy in primary biliary cirrhosis. Gastroenterology 1994, 107, 266–270. [Google Scholar] [CrossRef]
- Imokawa, S.; Colby, T.V.; Leslie, K.O.; Helmers, R.A. Methotrexate pneumonitis: Review of the literature and histopathological findings in nine patients. Eur. Respir. J. 2000, 15, 373–381. [Google Scholar] [CrossRef] [PubMed]
- Kremer, J.M.; Alarcon, G.S.; Weinblatt, M.E.; Kaymakcian, M.V.; Macaluso, M.; Cannon, G.W.; Palmer, W.R.; Sundy, J.S.; St Clair, E.W.; Alexander, R.W.; et al. Clinical, laboratory, radiographic, and histopathologic features of methotrexate-associated lung injury in patients with rheumatoid arthritis: A multicenter study with literature review. Arthritis Rheum. 1997, 40, 1829–1837. [Google Scholar] [CrossRef] [PubMed]
- Sawada, T.; Inokuma, S.; Sato, T.; Otsuka, T.; Saeki, Y.; Takeuchi, T.; Matsuda, T.; Takemura, T.; Sagawa, A.; On Behalf of the Study Committee for Leflunomide-induced Lung Injury, Japan College of Rheumatology. Leflunomide-induced interstitial lung disease: Prevalence and risk factors in Japanese patients with rheumatoid arthritis. Rheumatology 2009, 48, 1069–1072. [Google Scholar] [CrossRef] [PubMed]
- Chikura, B.; Lane, S.; Dawson, J.K. Clinical expression of leflunomide-induced pneumonitis. Rheumatology 2009, 48, 1065–1068. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sato, T.; Inokuma, S.; Sagawa, A.; Matsuda, T.; Takemura, T.; Otsuka, T.; Saeki, Y.; Takeuchi, T.; Sawada, T.; On Behalf of the Study Committee for Leflunomide-induced Lung Injury, Japan College of Rheumatology. Factors associated with fatal outcome of leflunomide-induced lung injury in Japanese patients with rheumatoid arthritis. Rheumatology 2009, 48, 1265–1268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suissa, S.; Hudson, M.; Ernst, P. Leflunomide use and the risk of interstitial lung disease in rheumatoid arthritis. Arthritis Rheum. 2006, 54, 1435–1439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conway, R.; Low, C.; Coughlan, R.J.; O’Donnell, M.J.; Carey, J.J. Leflunomide Use and Risk of Lung Disease in Rheumatoid Arthritis: A Systematic Literature Review and Metaanalysis of Randomized Controlled Trials. J. Rheumatol. 2016, 43, 855–860. [Google Scholar] [CrossRef] [PubMed]
- Roubille, C.; Haraoui, B. Interstitial lung diseases induced or exacerbated by DMARDS and biologic agents in rheumatoid arthritis: A systematic literature review. Semin. Arthritis Rheum. 2014, 43, 613–626. [Google Scholar] [CrossRef] [PubMed]
- Koike, T.; Harigai, M.; Ishiguro, N.; Inokuma, S.; Takei, S.; Takeuchi, T.; Yamanaka, H.; Tanaka, Y. Safety and effectiveness of adalimumab in Japanese rheumatoid arthritis patients: Postmarketing surveillance report of the first 3000 patients. Mod. Rheumatol. 2012, 22, 498–508. [Google Scholar] [CrossRef] [PubMed]
- Herrinton, L.J.; Harrold, L.R.; Liu, L.; Raebel, M.A.; Taharka, A.; Winthrop, K.L.; Solomon, D.H.; Curtis, J.R.; Lewis, J.D.; Saag, K.G. Association between anti-TNF-alpha therapy and interstitial lung disease. Pharmacoepidemiol. Drug Saf. 2013, 22, 394–402. [Google Scholar] [CrossRef] [PubMed]
- Curtis, J.R.; Sarsour, K.; Napalkov, P.; Costa, L.A.; Schulman, K.L. Incidence and complications of interstitial lung disease in users of tocilizumab, rituximab, abatacept and anti-tumor necrosis factor alpha agents, a retrospective cohort study. Arthritis Res. Ther. 2015, 17, 319. [Google Scholar] [CrossRef] [PubMed]
- Perez-Alvarez, R.; Perez-de-Lis, M.; Diaz-Lagares, C.; Pego-Reigosa, J.M.; Retamozo, S.; Bove, A.; Brito-Zeron, P.; Bosch, X.; Ramos-Casals, M. Interstitial lung disease induced or exacerbated by TNF-targeted therapies: Analysis of 122 cases. Semin. Arthritis Rheum. 2011, 41, 256–264. [Google Scholar] [CrossRef] [PubMed]
- Hadjinicolaou, A.V.; Nisar, M.K.; Bhagat, S.; Parfrey, H.; Chilvers, E.R.; Ostor, A.J. Non-infectious pulmonary complications of newer biological agents for rheumatic diseases—A systematic literature review. Rheumatology 2011, 50, 2297–2305. [Google Scholar] [CrossRef] [PubMed]
- Liote, H.; Liote, F.; Seroussi, B.; Mayaud, C.; Cadranel, J. Rituximab-induced lung disease: A systematic literature review. Eur. Respir. J. 2010, 35, 681–687. [Google Scholar] [CrossRef] [PubMed]
- Wagner, S.A.; Mehta, A.C.; Laber, D.A. Rituximab-induced interstitial lung disease. Am. J. Hematol. 2007, 82, 916–919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Penn, R.G.; Griffin, J.P. Adverse reactions to nitrofurantoin in the United Kingdom, Sweden, and Holland. Br. Med. J. 1982, 284, 1440–1442. [Google Scholar] [CrossRef]
- Holmberg, L.; Boman, G.; Bottiger, L.E.; Eriksson, B.; Spross, R.; Wessling, A. Adverse reactions to nitrofurantoin. Analysis of 921 reports. Am. J. Med. 1980, 69, 733–738. [Google Scholar] [CrossRef]
- Sovijarvi, A.R.; Lemola, M.; Stenius, B.; Idanpaan-Heikkila, J. Nitrofurantoin-induced acute, subacute and chronic pulmonary reactions. Scand. J. Respir. Dis. 1977, 58, 41–50. [Google Scholar] [PubMed]
- Santos, J.M.; Batech, M.; Pelter, M.A.; Deamer, R.L. Evaluation of the Risk of Nitrofurantoin Lung Injury and Its Efficacy in Diminished Kidney Function in Older Adults in a Large Integrated Healthcare System: A Matched Cohort Study. J. Am. Geriatr. Soc. 2016, 64, 798–805. [Google Scholar] [CrossRef] [PubMed]
- Durante-Mangoni, E.; Andini, R.; Parrella, A.; Mattucci, I.; Cavezza, G.; Senese, A.; Trojaniello, C.; Caprioli, R.; Diana, M.V.; Utili, R. Safety of treatment with high-dose daptomycin in 102 patients with infective endocarditis. Int. J. Antimicrob. Agents 2016, 48, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Mankikian, J.; Favelle, O.; Guillon, A.; Guilleminault, L.; Cormier, B.; Jonville-Bera, A.P.; Perrotin, D.; Diot, P.; Marchand-Adam, S. Initial characteristics and outcome of hospitalized patients with amiodarone pulmonary toxicity. Respir. Med. 2014, 108, 638–646. [Google Scholar] [CrossRef] [PubMed]
- Bongard, V.; Marc, D.; Philippe, V.; Jean-Louis, M.; Maryse, L.M. Incidence rate of adverse drug reactions during long-term follow-up of patients newly treated with amiodarone. Am. J. Ther. 2006, 13, 315–319. [Google Scholar] [CrossRef] [PubMed]
- Tisdale, J.E.; Follin, S.L.; Ordelova, A.; Webb, C.R. Risk factors for the development of specific noncardiovascular adverse effects associated with amiodarone. J. Clin. Pharmacol. 1995, 35, 351–356. [Google Scholar] [CrossRef] [PubMed]
- Pollak, P.T.; Sharma, A.D.; Carruthers, S.G. Relation of amiodarone hepatic and pulmonary toxicity to serum drug concentrations and superoxide dismutase activity. Am. J. Cardiol. 1990, 65, 1185–1191. [Google Scholar] [CrossRef]
- Kang, I.S.; Kim, K.J.; Kim, Y.; Park, S.H. The diagnostic utility of chest computed tomography scoring for the assessment of amiodarone-induced pulmonary toxicity. Korean J. Intern. Med. 2014, 29, 746–753. [Google Scholar] [CrossRef] [PubMed]
- Yamada, Y.; Shiga, T.; Matsuda, N.; Hagiwara, N.; Kasanuki, H. Incidence and predictors of pulmonary toxicity in Japanese patients receiving low-dose amiodarone. Circ. J. 2007, 71, 1610–1616. [Google Scholar] [CrossRef] [PubMed]
- Dusman, R.E.; Stanton, M.S.; Miles, W.M.; Klein, L.S.; Zipes, D.P.; Fineberg, N.S.; Heger, J.J. Clinical features of amiodarone-induced pulmonary toxicity. Circulation 1990, 82, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Dean, P.J.; Groshart, K.D.; Porterfield, J.G.; Iansmith, D.H.; Golden, E.B., Jr. Amiodarone-associated pulmonary toxicity. A clinical and pathologic study of eleven cases. Am. J. Clin. Pathol. 1987, 87, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Kupferschmid, J.P.; Rosengart, T.K.; McIntosh, C.L.; Leon, M.B.; Clark, R.E. Amiodarone-induced complications after cardiac operation for obstructive hypertrophic cardiomyopathy. Ann. Thorac. Surg. 1989, 48, 359–364. [Google Scholar] [CrossRef]
- Logan, P.M.; Primack, S.L.; Staples, C.; Miller, R.R.; Muller, N.L. Acute lung disease in the immunocompromised host. Diagnostic accuracy of the chest radiograph. Chest 1995, 108, 1283–1287. [Google Scholar] [CrossRef] [PubMed]
- Kawase, S.; Hattori, N.; Ishikawa, N.; Horimasu, Y.; Fujitaka, K.; Furonaka, O.; Isobe, T.; Miyoshi, S.; Hamada, H.; Yamane, T.; et al. Change in serum KL-6 level from baseline is useful for predicting life-threatening EGFR-TKIs induced interstitial lung disease. Respir. Res. 2011, 12, 97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tirumani, S.H.; Ramaiya, N.H.; Keraliya, A.; Bailey, N.D.; Ott, P.A.; Hodi, F.S.; Nishino, M. Radiographic Profiling of Immune-Related Adverse Events in Advanced Melanoma Patients Treated with Ipilimumab. Cancer Immunol. Res. 2015, 3, 1185–1192. [Google Scholar] [CrossRef] [PubMed]
- Nishino, M.; Ramaiya, N.H.; Awad, M.M.; Sholl, L.M.; Maattala, J.A.; Taibi, M.; Hatabu, H.; Ott, P.A.; Armand, P.; Hodi, F.S. PD-1 Inhibitor-Related Pneumonitis in Advanced Cancer Patients: Radiographic Patterns and Clinical Course. Clin. Cancer Res. 2016, 22, 6051–6060. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshii, N.; Suzuki, T.; Nagashima, M.; Kon, A.; Kakihata, K.; Gemma, A. Clarification of clinical features of interstitial lung disease induced by irinotecan based on postmarketing surveillance data and spontaneous reports. Anti-Cancer Drugs 2011, 22, 563–568. [Google Scholar] [CrossRef] [PubMed]
- Ohnishi, K.; Sakai, F.; Kudoh, S.; Ohno, R. Twenty-seven cases of drug-induced interstitial lung disease associated with imatinib mesylate. Leukemia 2006, 20, 1162–1164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomii, K.; Kato, T.; Takahashi, M.; Noma, S.; Kobashi, Y.; Enatsu, S.; Okubo, S.; Kobayashi, N.; Kudoh, S. Pemetrexed-related interstitial lung disease reported from post marketing surveillance (malignant pleural mesothelioma/non-small cell lung cancer). Jpn. J. Clin. Oncol. 2017, 47, 350–356. [Google Scholar] [CrossRef] [PubMed]
- Iki, S.; Yoshinaga, K.; Ohbayashi, Y.; Urabe, A. Cytotoxic drug-induced pneumonia and possible augmentation by G-CSF—Clinical attention. Ann. Hematol. 1993, 66, 217–218. [Google Scholar] [CrossRef] [PubMed]
- Koike, T.; Harigai, M.; Inokuma, S.; Ishiguro, N.; Ryu, J.; Takeuchi, T.; Tanaka, Y.; Yamanaka, H.; Fujii, K.; Yoshinaga, T.; et al. Postmarketing surveillance of safety and effectiveness of etanercept in Japanese patients with rheumatoid arthritis. Mod. Rheumatol. 2011, 21, 343–351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramos-Casals, M.; Brito-Zeron, P.; Munoz, S.; Soria, N.; Galiana, D.; Bertolaccini, L.; Cuadrado, M.-J.; Khamashta, M.A. Autoimmune diseases induced by TNF-targeted therapies: Analysis of 233 cases. Medicine 2007, 86, 242–251. [Google Scholar] [CrossRef] [PubMed]
- Israel-Biet, D.; Venet, A.; Caubarrere, I.; Bonan, G.; Danel, C.; Chretien, J.; Hance, A.J. Bronchoalveolar lavage in amiodarone pneumonitis. Cellular abnormalities and their relevance to pathogenesis. Chest 1987, 91, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Waxman, H.L.; Groh, W.C.; Marchlinski, F.E.; Buxton, A.E.; Sadowski, L.M.; Horowitz, L.N.; Josephson, M.E.; Kastor, J.A. Amiodarone for control of sustained ventricular tachyarrhythmia: Clinical and electrophysiologic effects in 51 patients. Am. J. Cardiol. 1982, 50, 1066–1074. [Google Scholar] [CrossRef]
- Van, M.W.; Coolen, L.; Malysse, I.; Lacquet, L.M.; Deneffe, G.J.; Demedts, M.G. Amiodarone and the development of ARDS after lung surgery. Chest 1994, 105, 1642–1645. [Google Scholar]
- Yamasaki, K.; Yatera, K.; Noguchi, S.; Oda, K.; Akata, K.; Nishida, C.; Kawanami, T.; Kawanami, Y.; Ishimoto, H.; Ono, S.; et al. Incidence and outcomes of bepridil-induced interstitial pneumonia. Respir. Med. 2013, 107, 2088–2091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandez, A.B.; Karas, R.H.; Alsheikh-Ali, A.A.; Thompson, P.D. Statins and interstitial lung disease: A systematic review of the literature and of food and drug administration adverse event reports. Chest 2008, 134, 824–830. [Google Scholar] [CrossRef] [PubMed]
- Hardak, E.; Berger, G.; Krivoy, N.; Solomonov, A.; Yigla, M. Nitrofurantoin pulmonary toxicity: Neglected threat. Curr. Drug Saf. 2010, 5, 125–128. [Google Scholar] [CrossRef] [PubMed]
- Kim, P.W.; Sorbello, A.F.; Wassel, R.T.; Pham, T.M.; Tonning, J.M.; Nambiar, S. Eosinophilic pneumonia in patients treated with daptomycin: Review of the literature and US FDA adverse event reporting system reports. Drug Saf. 2012, 35, 447–457. [Google Scholar] [CrossRef] [PubMed]
- Slavenburg, S.; Heijdra, Y.F.; Drenth, J.P. Pneumonitis as a consequence of (peg) interferon-ribavirin combination therapy for hepatitis C: A review of the literature. Dig. Dis. Sci. 2010, 55, 579–585. [Google Scholar] [CrossRef] [PubMed]
- Minami-Shimmyo, Y.; Ohe, Y.; Yamamoto, S.; Sumi, M.; Nokihara, H.; Horinouchi, H.; Yamamoto, N.; Sekine, I.; Kubota, K.; Tamura, T. Risk factors for treatment-related death associated with chemotherapy and thoracic radiotherapy for lung cancer. J. Thorac. Oncol. 2012, 7, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Sakurada, T.; Kakiuchi, S.; Tajima, S.; Horinouchi, Y.; Okada, N.; Nishisako, H.; Nakamura, T.; Teraoka, K.; Kawazoe, K.; Yanagawa, H.; et al. Characteristics of and risk factors for interstitial lung disease induced by chemotherapy for lung cancer. Ann. Pharmacother. 2015, 49, 398–404. [Google Scholar] [CrossRef] [PubMed]
- Johkoh, T.; Sakai, F.; Kusumoto, M.; Arakawa, H.; Harada, R.; Ueda, M.; Kudoh, S.; Fukuoka, M. Association between baseline pulmonary status and interstitial lung disease in patients with non-small-cell lung cancer treated with erlotinib—A cohort study. Clin. Lung Cancer 2014, 15, 448–454. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, K.; Kudoh, S.; Ohe, Y.; Johkoh, T.; Ando, M.; Yamazaki, N.; Seki, A.; Takemoto, S.; Fukuoka, M. Postmarketing surveillance study of erlotinib in Japanese patients with non-small-cell lung cancer (NSCLC, an interim analysis of 3488 patients (POLARSTAR). J. Thorac. Oncol. 2012, 7, 1296–1303. [Google Scholar] [CrossRef] [PubMed]
- Shidara, K.; Hoshi, D.; Inoue, E.; Yamada, T.; Nakajima, A.; Taniguchi, A.; Hara, M.; Momohara, S.; Kamatani, N.; Yamanaka, H. Incidence of and risk factors for interstitial pneumonia in patients with rheumatoid arthritis in a large Japanese observational cohort, IORRA. Mod. Rheumatol. 2010, 20, 280–286. [Google Scholar] [CrossRef] [PubMed]
- Ando, M.; Okamoto, I.; Yamamoto, N.; Takeda, K.; Tamura, K.; Seto, T.; Ariyoshi, Y.; Fukuoka, M. Predictive factors for interstitial lung disease, antitumor response, and survival in non-small-cell lung cancer patients treated with gefitinib. J. Clin. Oncol. 2006, 24, 2549–2556. [Google Scholar] [CrossRef] [PubMed]
- Wijnen, P.A.; Drent, M.; Nelemans, P.J.; Kuijpers, P.M.; Koek, G.H.; Neef, C.; Haenen, G.R.M.M.; Bekers, O. Role of cytochrome P450 polymorphisms in the development of pulmonary drug toxicity: A case-control study in The Netherlands. Drug Saf. 2008, 31, 1125–1134. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, M.; Toyoda, M.; Takenaka, K.; Imamura, Y.; Chayahara, N.; Kiyota, N.; Mukohara, T.; Kotake, T.; Tsuji, A.; Saito, K.; et al. The combination of HLA-B*15:01 and DRB1*15:01 is associated with gemcitabine plus erlotinib-induced interstitial lung disease in patients with advanced pancreatic cancer. Cancer Chemother. Pharmacol. 2016, 77, 1165–1170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weiner, S.M.; Sellin, L.; Vonend, O.; Schenker, P.; Buchner, N.J.; Flecken, M.; Viebahn, R.; Rump, L.C. Pneumonitis associated with sirolimus: Clinical characteristics, risk factors and outcome—A single-centre experience and review of the literature. Nephrol. Dial. Transplant. 2007, 22, 3631–3637. [Google Scholar] [CrossRef] [PubMed]
- Chap, L.; Shpiner, R.; Levine, M.; Norton, L.; Lill, M.; Glaspy, J. Pulmonary toxicity of high-dose chemotherapy for breast cancer: A non-invasive approach to diagnosis and treatment. Bone Marrow Transplant. 1997, 20, 1063–1067. [Google Scholar] [CrossRef] [PubMed]
- Padley, S.P.; Adler, B.; Hansell, D.M.; Muller, N.L. High-resolution computed tomography of drug-induced lung disease. Clin. Radiol. 1992, 46, 232–236. [Google Scholar] [CrossRef]
- Potente, G.; Bellelli, A.; Nardis, P. Specific diagnosis by CT and HRCT in six chronic lung diseases. Comput. Med. Imaging Graph. 1992, 16, 277–282. [Google Scholar] [CrossRef]
- Cleverley, J.R.; Screaton, N.J.; Hiorns, M.P.; Flint, J.D.; Muller, N.L. Drug-induced lung disease: High-resolution CT and histological findings. Clin. Radiol. 2002, 57, 292–299. [Google Scholar] [CrossRef] [PubMed]
- Patz, E.F., Jr.; Peters, W.P.; Goodman, P.C. Pulmonary drug toxicity following high-dose chemotherapy with autologous bone marrow transplantation: CT findings in 20 cases. J. Thorac. Imaging 1994, 9, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, K.; Kato, M.; Shukuya, T.; Mori, K.; Sekimoto, Y.; Ihara, H.; Kanemaru, R.; Ko, R.; Shibayama, R.; Tajima, K.; et al. Surfactant protein-D predicts prognosis of interstitial lung disease induced by anticancer agents in advanced lung cancer: A case control study. BMC Cancer 2017, 17, 302. [Google Scholar] [CrossRef] [PubMed]
- Takatani, K.; Miyazaki, E.; Nureki, S.; Ando, M.; Ueno, T.; Okubo, T.; Takenaka, R.; Hiroshige, S.; Kumamoto, T. High-resolution computed tomography patterns and immunopathogenetic findings in drug-induced pneumonitis. Respir. Med. 2008, 102, 892–898. [Google Scholar] [CrossRef] [PubMed]
- Johkoh, T.; Itoh, H.; Muller, N.L.; Ichikado, K.; Nakamura, H.; Ikezoe, J.; Akira, M.; Nagareda, T. Crazy-paving appearance at thin-section CT: Spectrum of disease and pathologic findings. Radiology 1999, 211, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.B.; Matthes, S.; Shpall, E.J.; Fisher, J.H.; Stemmer, S.M.; Dufton, C.; Stephens, J.K.; Bearman, S.I. Acute lung injury following treatment with high-dose cyclophosphamide, cisplatin, and carmustine: Pharmacodynamic evaluation of carmustine. J. Natl. Cancer Inst. 1993, 85, 640–647. [Google Scholar] [CrossRef] [PubMed]
- Akoun, G.M.; Cadranel, J.L.; Milleron, B.J.; D’Ortho, M.P.; Mayaud, C.M. Bronchoalveolar lavage cell data in 19 patients with drug-associated pneumonitis (except amiodarone). Chest 1991, 99, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Allen, J.N.; Davis, W.B.; Pacht, E.R. Diagnostic significance of increased bronchoalveolar lavage fluid eosinophils. Am. Rev. Respir. Dis. 1990, 142, 642–647. [Google Scholar] [CrossRef] [PubMed]
- White, D.A.; Rankin, J.A.; Stover, D.E.; Gellene, R.A.; Gupta, S. Methotrexate pneumonitis. Bronchoalveolar lavage findings suggest an immunologic disorder. Am. Rev. Respir. Dis. 1989, 139, 18–21. [Google Scholar] [CrossRef] [PubMed]
- Fuhrman, C.; Parrot, A.; Wislez, M.; Prigent, H.; Boussaud, V.; Bernaudin, J.F.; Mayaud, C.; Cadranel, J. Spectrum of CD4 to CD8 T-cell ratios in lymphocytic alveolitis associated with methotrexate-induced pneumonitis. Am. J. Respir. Crit. Care Med. 2001, 164, 1186–1191. [Google Scholar] [CrossRef] [PubMed]
- Akoun, G.M.; Mayaud, C.M.; Touboul, J.L.; Denis, M.F.; Milleron, B.J.; Perrot, J.Y. Use of bronchoalveolar lavage in the evaluation of methotrexate lung disease. Thorax 1987, 42, 652–655. [Google Scholar] [CrossRef] [PubMed]
- Schnabel, A.; Richter, C.; Bauerfeind, S.; Gross, W.L. Bronchoalveolar lavage cell profile in methotrexate induced pneumonitis. Thorax 1997, 52, 377–379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, M.S.; Colby, T.V.; Goellner, J.R.; Martin, W.J., Jr. Utility of bronchoalveolar lavage in the diagnosis of drug-induced pulmonary toxicity. Acta Cytol. 1989, 33, 533–538. [Google Scholar] [PubMed]
- Lim, K.H.; Yoon, H.I.; Kang, Y.A.; Lee, K.W.; Kim, J.H.; Bang, S.M.; Lee, J.H.; Lee, C.-T.; Lee, J.S. Severe pulmonary adverse effects in lymphoma patients treated with cyclophosphamide, doxorubicin, vincristine, and prednisone (CHOP) regimen plus rituximab. Korean J. Intern. Med. 2010, 25, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Rebattu, P.; Quantin, X.; Ardiet, C.; Morere, J.F.; Azarian, M.R.; Schuller-Lebeau, M.P.; Pujol, J.-L. Dose-finding, pharmacokinetic and phase II study of docetaxel in combination with gemcitabine in patients with inoperable non-small cell lung cancer. Lung Cancer 2001, 33, 277–287. [Google Scholar] [CrossRef]
- Ki, K.D.; Lee, J.M.; Lee, S.K.; Tong, S.Y.; Huh, C.Y.; Ryu, J.K.; Kim, K.-Y. Pulmonary toxicity after a quick course of combinatorial vincristine, bleomycin, and cisplatin neoadjuvant chemotherapy in cervical cancer. J. Korean Med. Sci. 2010, 25, 240–244. [Google Scholar] [CrossRef] [PubMed]
- Vial-Dupuy, A.; Sanchez, O.; Douvry, B.; Guetta, L.; Juvin, K.; Wermert, D.; Guérot, E.; Israël-Biet, D. Outcome of patients with interstitial lung disease admitted to the intensive care unit. Sarcoidosis Vasc. Diffuse Lung Dis. 2013, 30, 134–142. [Google Scholar] [PubMed]
- Park, S.Y.; Lim, S.Y.; Um, S.W.; Koh, W.J.; Chung, M.P.; Kim, H.; Kwon, O.J.; Park, H.K.; Kim, S.J.; Im, Y.H.; et al. Outcome and predictors of mortality in patients requiring invasive mechanical ventilation due to acute respiratory failure while undergoing ambulatory chemotherapy for solid cancers. Support. Care Cancer 2013, 21, 1647–1653. [Google Scholar] [CrossRef] [PubMed]
- Delorme, S.; Keller-Reichenbecher, M.A.; Zuna, I.; Schlegel, W.; Van, K.G. Usual interstitial pneumonia. Quantitative assessment of high-resolution computed tomography findings by computer-assisted texture-based image analysis. Investig. Radiol. 1997, 32, 566–574. [Google Scholar] [CrossRef]
- Wild, J.M. Imaging pathophysiological changes in the lungs in IPF with xenon magnetic resonance imaging. Thorax 2018, 73, 1. [Google Scholar] [CrossRef] [PubMed]
- Morgan, A.R.; Parker, G.J.; Roberts, C.; Buonaccorsi, G.A.; Maguire, N.C.; Hubbard Cristinacce, P.L.; Singh, D.; Vestbo, J.; Bjermer, L.; Jögi, J.; et al. Feasibility assessment of using oxygen-enhanced magnetic resonance imaging for evaluating the effect of pharmacological treatment in COPD. Eur. J. Radiol. 2014, 83, 2093–2101. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Grade 1 (mild) | Asymptomatic, radiographic findings only |
| Grade 2 (moderate) | Symptomatic, not interfering with activities of daily living |
| Grade 3 (severe) | Symptomatic, interfering with activities of daily living or oxygen indicated |
| Grade 4 (life-threatening or disabling) | Life-threatening, or ventilator support required |
| Grade 5 (fatal) |
| Drug/Class | Number of Studies | Quality | Study Design | Patient Population | Sample Size (Range) | Case Definition of DIILD | Estimated Incidence (Range) | Estimated Mortality in Those with DIILD (Range) |
|---|---|---|---|---|---|---|---|---|
| Cancer Therapies | ||||||||
| Bleomycin [18,19,20,21,22,23,24] | 7 | Moderate = 3 Low = 3 Very low = 1 | Meta-analysis = 2 Observational studies = 5 | Various cancers (1 meta-analysis in ovarian sex cord stromal tumours and 1 in all cancer RCT data) | 22–1147 | variable | Meta-analyses: 6.8–15% Other studies: 6.8–21% | Meta-analyses: 8.1–23% Other studies: 0–48% |
| Gemcitabine [13,25,26,27,28,29,30,31,32] | 9 | Moderate = 2 Low = 6 Very low = 1 | Meta-analysis = 2 Clinical trial = 3 Observational = 4 | Cancer (predominantly pancreatic and non-small cell lung cancer but also others) | Meta-analysis: 1308–1742 Others: 26–2440 | variable | 1.1–3.9% | 0–22% |
| Epidermal growth factor receptor-targeted therapies (EGFR) | ||||||||
| Erlotinib [34,35,36,89,90] | 5 | Moderate = 2 Low = 3 | Meta-analysis = 2 Post marketing surveillance = 2 Observational = 1 | Non-small cell lung cancer | 341–9909 | variable | 0.9–5.9% | 31–45% |
| Gefitinib [34,35,36,37] | 4 | Moderate = 2 Low = 2 | Meta-analysis = 2 Post marketing surveillance = 2 | Non-small cell lung, breast and colorectal cancer | 70–5468 | variable | 1.9–3.5% | 18–44% |
| Panitumumab [33,39] | 2 (but reporting from same cohort) | Moderate = 2 | Post marketing surveillance | Colorectal cancer | 3085 | Expert case review | 1.3% | 51.3% |
| Cetuximab [38] | 1 | Moderate = 3 | Post marketing surveillance | Colorectal cancer | 2006 | Physician reported | 1.2% | 41.6% |
| Mechanistic target of rapamycin protein (MTOR) inhibitors | ||||||||
| Everolimus [40,41,42,43,45,46,48,49] | 8 | Moderate = 3 Low = 3 Very low = 2 | Meta-analysis = 1 Clinical trial = 2 (same trial 2 separate published analyses) Observational = 5 | Neuroendocrine cancer Renal cell cancer Renal transplant | 40–2261 | Variable, including radiographic signs of DIILD | 2.8–58% | 5.4–20% |
| Temsirolimus [44,47] | 2 | Low = 2 | Meta-analysis = 1 Clinical trial = 1 Observational study = 1 | Neuroendocrine cancer Endometrial cancer Renal cell cancer | 22–408 | Variable | 29–36% | n/a |
| Sirolimus [48] | 1 | Very low = 1 | Observational | Renal/pancreas transplant | 115 | Physician reported | 9.5% | 0% |
| Check point inhibitors (CPI) | ||||||||
| All CPIs [51,52,53] | 3 | High = 2 Moderate = 1 | Meta-analysis = 2 Observational = 1 | Non-small cell lung cancer | 1826–3232 | variable | 1.1–3.6% | 8–9.4% |
| Ipilimumab [91] | Low = 1 | Observational = 1 | Melanoma | 146 | Radiographic evidence of DIILD | 5.44% | n/a | |
| Nivolumab [92] | 1 | Low = 1 | Post hoc pooled clinical trial analysis = 1 | Cancer (various types) | 170 | Physician reported events | 11.7% | 0% |
| Other agents identified | ||||||||
| Irinotecan [93] | 1 | Low = 1 | Post marketing surveillance | Cancer (various types) | 8864 | Physician reported | 0.74% | 24% |
| Rituximab [67,72,73,74] | 4 | Very low = 4 | Systematic reviews = 3 Case series = 1 | Predominantly cancer but other indications included | 16–52 | Variable | n/a | n/a |
| Imatinib [94] | 1 | Low = 1 | Post marketing surveillance | Leukaemia | 6 | Physician reported | n/a | 6/6 resolved |
| Pemetrexed [95] | 1 | Moderate = 1 | Post marketing surveillance | Mesothelioma Non-small cell lung cancer | 903 | Expert committee review | 1.8% | |
| Granulocyte colony stimulating factor [96] | 1 | Low = 1 | Observational | In conjunction with chemotherapy | 40 treated vs. 25 with chemotherapy along | Physician reported | 0.2% vs. 0% in the control group | n/a |
| Rheumatology drugs | ||||||||
| Methotrexate [55,56,57,58,59,60,61,67] | 8 | Moderate = 3 Low = 4 Very low = 1 | Meta-analysis = 2 Clinical trial = 3 Observational = 2 Case series = 1 | Rheumatoid arthritis Psoriasis, psoriatic arthritis or inflammatory bowel Primary biliary cirrhosis | 29–3188 | variable | 0.06–15% | 10–33% |
| Tumour necrosis factor inhibitors [67,68,69,70,71,72,97,98] | 8 | Moderate = 4 Low = 1 Very low = 3 | Post marketing surveillance = 3 (2 papers report on 1 study) Observational study = 3 Systematic review of case reports = 3 | Predominantly rheumatoid arthritis but cases in other diseases | 233–13,894 | variable | 0.6% | 32% |
| Leflunomide [62,63,64,65,66] | 5 | Moderate = 1 Low = 3 Very low = 1 | Meta-analysis of RCTs = 1 Case control via claims database = 1 Post marketing surveillance = 2 Case series = 1 | Rheumatoid arthritis | 2274–62,734 | variable | 0–1.2% | 19–41% |
| Cardiology drugs | ||||||||
| Amiodarone [80,81,82,83,84,85,86,87,88,99,100,101] | 12 | Moderate = 2 Low = 5 Very low = 5 | Observational = 7 Case series = 5 | Cardiovascular disease | 13–500 | Variable, often not restricted to DIILD | 1.2–8.8% | 0–41% |
| Bepridil [102] | 1 | Low = 1 | Observational | Cardiovascular disease | 222 | Standardised definition | 6.3% | 0% |
| Statins [103] | 1 | Very low = 1 | Observational (Adverse events reporting database) | Cardiovascular disease/prevention | 1/40 adverse event reports for statins were ILD | n/a | ||
| Anti-infection agents | ||||||||
| Nitrofurantoin [75,76,77,78,104] | 5 | Low = 3 Very low = 2 | Case-control study = 1 Registry study = 1 Post marketing surveillance = 1 Case series = 2 | Chronic and acute treatment of urinary tract infection | 10–70,804 | Variable, some used “any ILD” after use of drug | 3.65% | 1.34% |
| Daptomycin [79,105] | 2 | Low = 2 | Observational study = 1 Post marketing surveillance = 1 | Infection (one study specifically infective endocarditis) | 58–102 | Variable | 2.9% | n/a |
| Interferon [106] | 1 | Very low = 1 | Systematic review of case reports | Hepatitis C | 25 | Variable | n/a | n/a |
| Author | Drug | Patient Population | Sample Size | Glucocorticoids Dose (Oral or IV) | Response |
|---|---|---|---|---|---|
| Mankikian et al. [80] | Amiodarone | DIILD | 46 | Median dose of 1 mg/kg 15 surviving patients followed and 9 (60%) received glucocorticoids for 3–29 months. All surviving patients successfully had glucocorticoids withdrawn | 76% got glucocorticoids but no obvious difference in survival outcomes. Three patients treated for <3 months relapsed and glucocorticoids restarted. No relapse in patients treated for >6 months |
| Kakugawa et al. [12] | Various | DIILD | 47 | 29 of 47 patients received glucocorticoid therapy. Decision on glucocorticoid therapy was physician-based rather than protocol-based. No dosing information available | None of the patients with a DAD pattern on HRCT improved with glucocorticoid treatment, and DAD group had a 37.5% mortality. 75% of those with OP pattern on HRCT (3 of 4) improved with glucocorticoid treatment. With an NSIP pattern, 45.8% (11 of 24 patients) improved with glucocorticoid treatment. Hypersensitivity pneumonitis (HP) pattern was associated with a 36.4% response to glucocorticoid therapy. |
| Ki et al. [134] | Bleomycin with cisplatin and vincristine | Cervical cancer patients treated with prior mentioned agents [59] | 61 (7 cases of DIILD) | 4 with bleomycin injury received glucocorticoid Different regimens within the study. 1 patient who improved received 40 mg/day methylprednisolone, followed by 10 mg daily. 2 acutely ill patients received IV methylprednisolone 500 mg/day × 3 days. 1 patient received 1 mg/kg/day prednisolone, then 0.5 mg/kg | Of these 4 patients, 2 died, 1 improved, 1 non-responder. Insulin-dependent diabetes developed in 2 patients |
| Kim et al. [105] | Daptomycin | Suspected DIILD | 58 (7 definite DIILD cases, 13 probable cases) | No dosing information Definite cases: 5 of 7 received glucocorticoid (1 intravenous) Probable cases: 9 of 13 received glucocorticoid | No deaths 1 required long-term treatment |
| Rebattu et al. [133] | Gemcitabine with docetaxel | NSCLC patients treated with prior mentioned agents | 49 (6 DIILD cases) | 6/6 received glucocorticoids | All recovered |
| Ohnishi et al. [94] | Imatinib | DIILD | 27 | 19/27 received high dose glucocorticoids 5/27 moderate dose glucocorticoids3/27 no treatment | 7/27 resolved 16/27 improved 4/27 no improvement |
| Sharma et al. [59] | Methotrexate | Primary biliary cirrhosis patients treated with methotrexate | 43 (6 DIILD cases) | 5/6 received prednisolone 60 mg IV daily Duration of intravenous route and glucocorticoids taper unclear | 4/5 given glucocorticoids responded, 1 patient died from liver decompensation |
| White et al. [45] | Everolimus | Advanced renal cell cancer patients treated with everolimus | 416 (37 DIILD cases) | 16/37 patients received glucocorticoids All 10 patients with grade 3 pneumonitis received glucocorticoids | 10 patients with grade 3 pneumonitis who received glucocorticoids 3/10 continued everolimus: 1 died and 2 recovered 7/10 discontinued: 5 recovered, 1 had ongoing disease, 1 died |
| Tomii et al. [95] | Pemetrexed | Mesothelioma and NSCLC DIILD patients | 1586 (10 DIILD cases) | 10 cases, all of which received glucocorticoids | 5/10 patients deemed glucocorticoids responsive, 1 indeterminate, 4 non-glucocorticoids responders died |
| Osawa et al. [33] | Panitumumab | Colorectal cancer patients treated with panitumumab | 3085 (39 DIILD cases) | No dosing information available | Minimal information on glucocorticoid impact other than statement that most of the 20 patients who died had received glucocorticoids |
| Yoshii et al. [93] | Irinotecan | Cancer patients treated with irinotecan | 8864 (153 DIILD cases, 83 with clinical information) | 75/83 patients received glucocorticoids No dosing information available | 46/75 of those treated recovered or improved, 5/75 no response, 22/75 died, 2/75 unknown outcome DAD pattern associated with lack of response to glucocorticoids |
| Liote et al. [73] | Rituximab | DIILD | 45 | 27/45 cases of rituximab DIILD received glucocorticoid. Dosing unclear. Some patients received 1 mg/kg of body weight concomitantly with re-challenge. | No recurrence of rituximab injury in 3 patients receiving re-challenge with rituximab and concomitant 1 mg/kg methylprednisolone Early onset acute presentation: 5 patients all received glucocorticoids, 2 died Late onset chronic presentation in 3 patients who recovered with glucocorticoid therapy Authors recommend longer period of glucocorticoids usage rather than just boluses at each rituximab infusion, and a gradual taper to avoid rebound |
| Takatani et al. [122] | Various | DIILD | DAD group received median cumulative glucocorticoids dose of 5240 mg, range 1000–9195 mg; NSIP group median of 264, range 0–735 mg; HP group median 415, range 0–4470 mg; OP group median 2722, range 0–7835 mg | Days of oxygen therapy correlated well with cumulative doses of glucocorticoid therapy, i.e., the sicker patients received more glucocorticoids. OP pattern patients showed full recovery with glucocorticoids. No deaths in this group of 34 non-chemotherapy DIILD pts. 11 pts recovered fully without glucocorticoids | |
| Chap et al. [116] | Cyclophosphamide, cisplatin and BCNU | Breast cancer patients treated with prior mentioned | 64 (37 cases of DIILD) | 37/37 treated with prednisolone 60 mg oral twice daily × 10 days, then 30 mg/day × 1 week, 20 mg/day × 1 week, 15 mg/day × 1 week, followed by 5 mg taper on daily dose each week. Initiation of prednisolone based on scoring system; crackles on lung auscultation = 2, drop in DLCO by >10% from baseline = 3, drop in O2 saturation ≥4% with 2 min walk = 3, interstitial infiltrates on CXR = 3. Patients with a score ≥6 received prednisolone as above. | Glucocorticoid therapy associated with rapid clinical improvement in “most patients” (absolute numbers not available). 11 patients required prolonged prednisolone therapy (4–8 months), having experienced exacerbation of symptoms when prednisolone reduced to 15–20 mg/day |
| Hamada et al. [30] | Gemcitabine | pancreatic, lung, urothelial, breast, ovarian | 25,924 (428 cases of ILD not verified as DIILD) | 363/428 (84%) patients with ILD received either oral or intravenous glucocorticoids | 20% of hospitalised DIILD patients with severe disease died, no data on glucocorticoid-treated group outcome versus non-glucocorticoid-treated patients |
| What is the incidence and prevalence of DIILD? |
|
| What drugs are commonly associated with DIILD? |
|
| What are the risk factors for developing DIILD? |
|
| Radiological investigation of DIILD and the prevalent radiopathological patterns |
|
| What is the role of non-imaging diagnostic investigations? |
|
| What is the impact of glucocorticoid (GC) therapy on DIILD outcome? |
|
| What if any factors predict prognosis? |
|
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Skeoch, S.; Weatherley, N.; Swift, A.J.; Oldroyd, A.; Johns, C.; Hayton, C.; Giollo, A.; Wild, J.M.; Waterton, J.C.; Buch, M.; et al. Drug-Induced Interstitial Lung Disease: A Systematic Review. J. Clin. Med. 2018, 7, 356. https://doi.org/10.3390/jcm7100356
Skeoch S, Weatherley N, Swift AJ, Oldroyd A, Johns C, Hayton C, Giollo A, Wild JM, Waterton JC, Buch M, et al. Drug-Induced Interstitial Lung Disease: A Systematic Review. Journal of Clinical Medicine. 2018; 7(10):356. https://doi.org/10.3390/jcm7100356
Chicago/Turabian StyleSkeoch, Sarah, Nicholas Weatherley, Andrew J. Swift, Alexander Oldroyd, Christopher Johns, Conal Hayton, Alessandro Giollo, James M. Wild, John C. Waterton, Maya Buch, and et al. 2018. "Drug-Induced Interstitial Lung Disease: A Systematic Review" Journal of Clinical Medicine 7, no. 10: 356. https://doi.org/10.3390/jcm7100356