
Characteristics and Patient Reported Outcome Measures in Lipedema Patients—Establishing a Baseline for Treatment Evaluation in a High-Volume Center

Abstract
:1. Introduction

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Diagnostic Criteria | Type of Lipedema | Location of Onset |
|---|---|---|
| Almost exclusive occurrence in women | 1 | Hips |
| Bilateral and symmetrical manifestation with minimal involvement of the feet | 2 | Hips and thighs |
| Persistent enlargement after elevation of the extremities or weight loss Arms are affected | 3 | Hips, thighs and shanks |
| Minimal pitting edema | 4 | Arms |
| Negative Kaposi–Stemmer sign | 5 | Shanks |
| Pain, tenderness on pressure |
2. Methods
2.1. Patient Selection
2.2. Structure of Questionnaire
2.3. Data Collection
3. Results
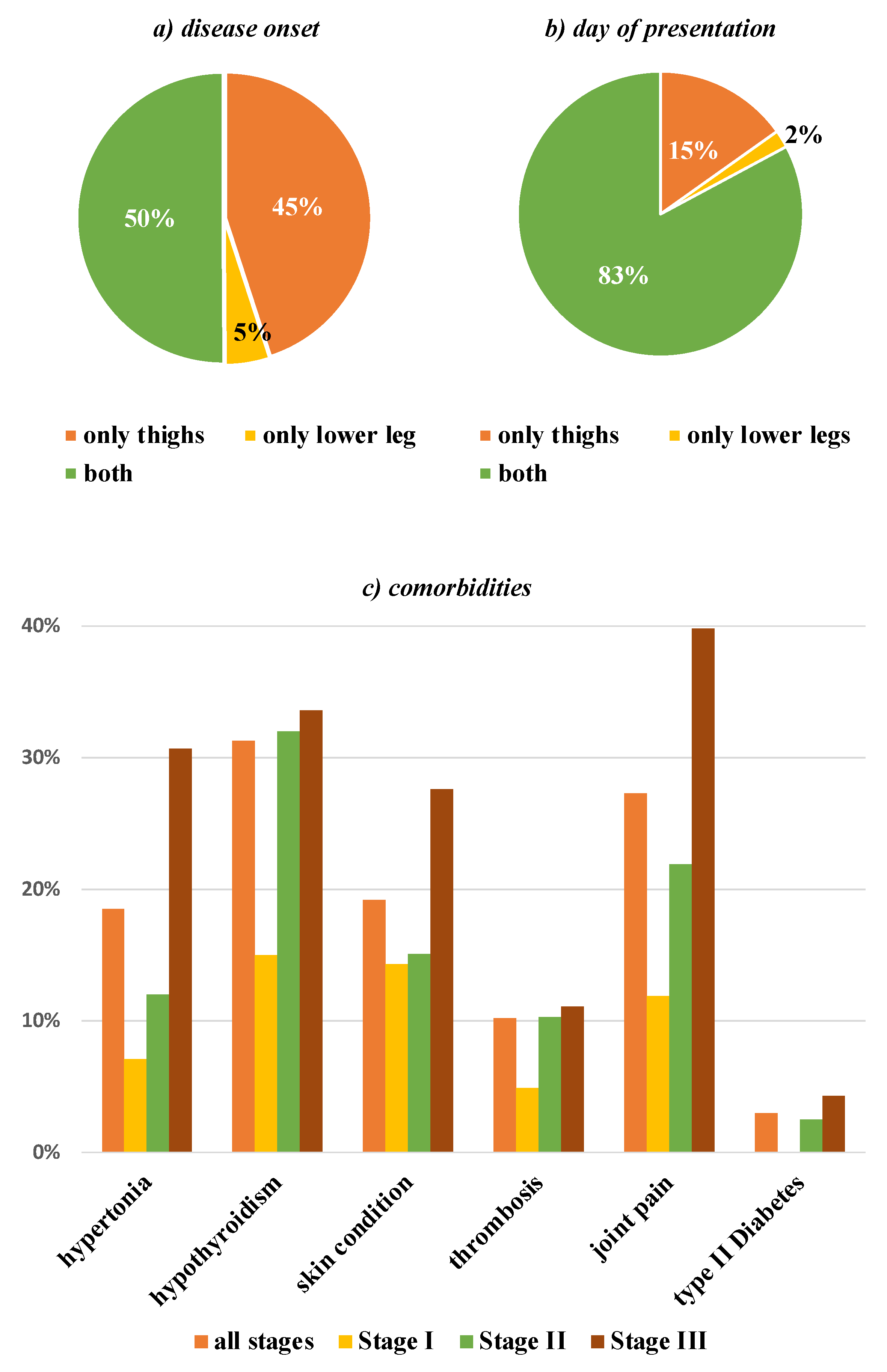
3.1. General Information
3.2. Comorbidities
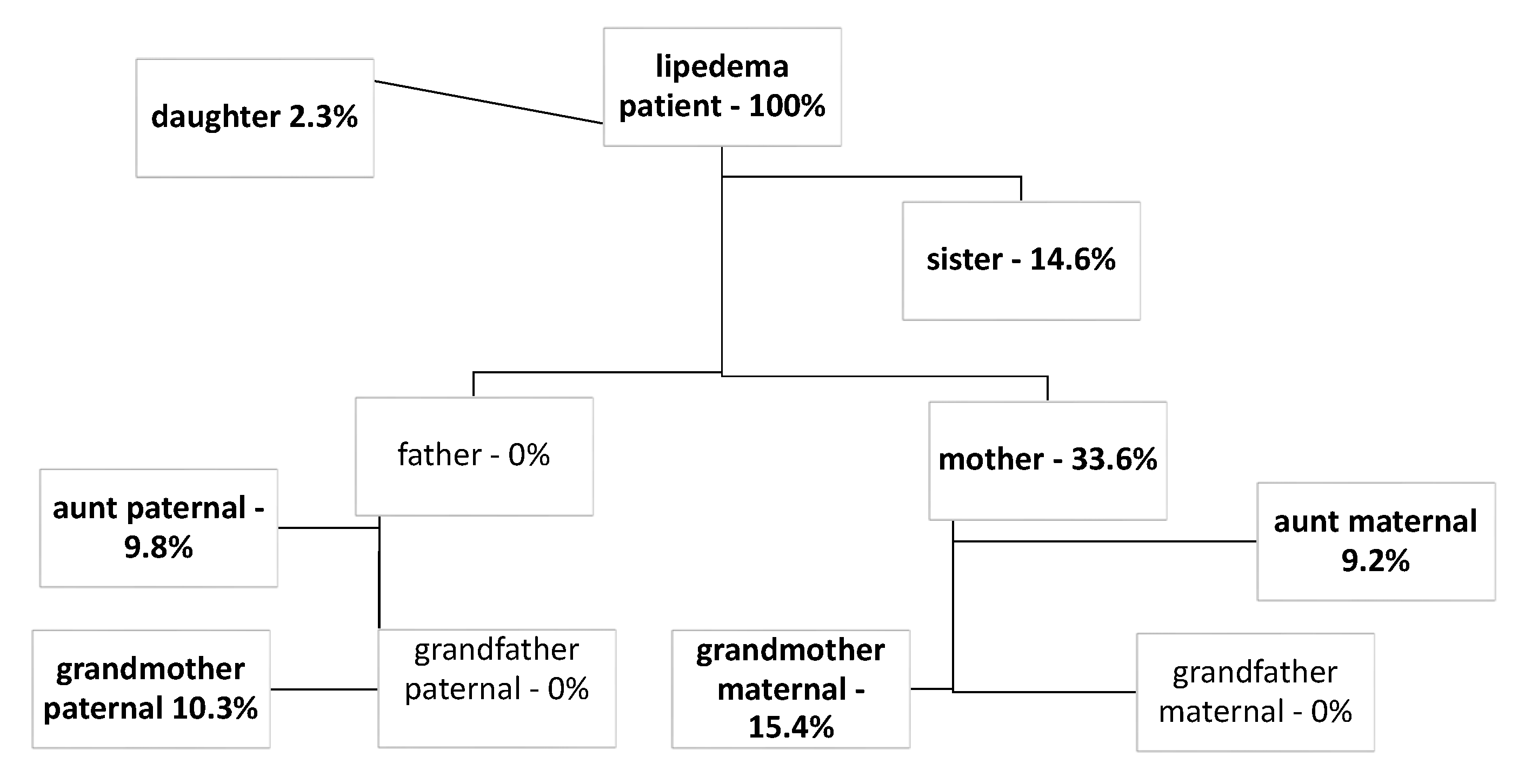
3.3. Familial Clustering
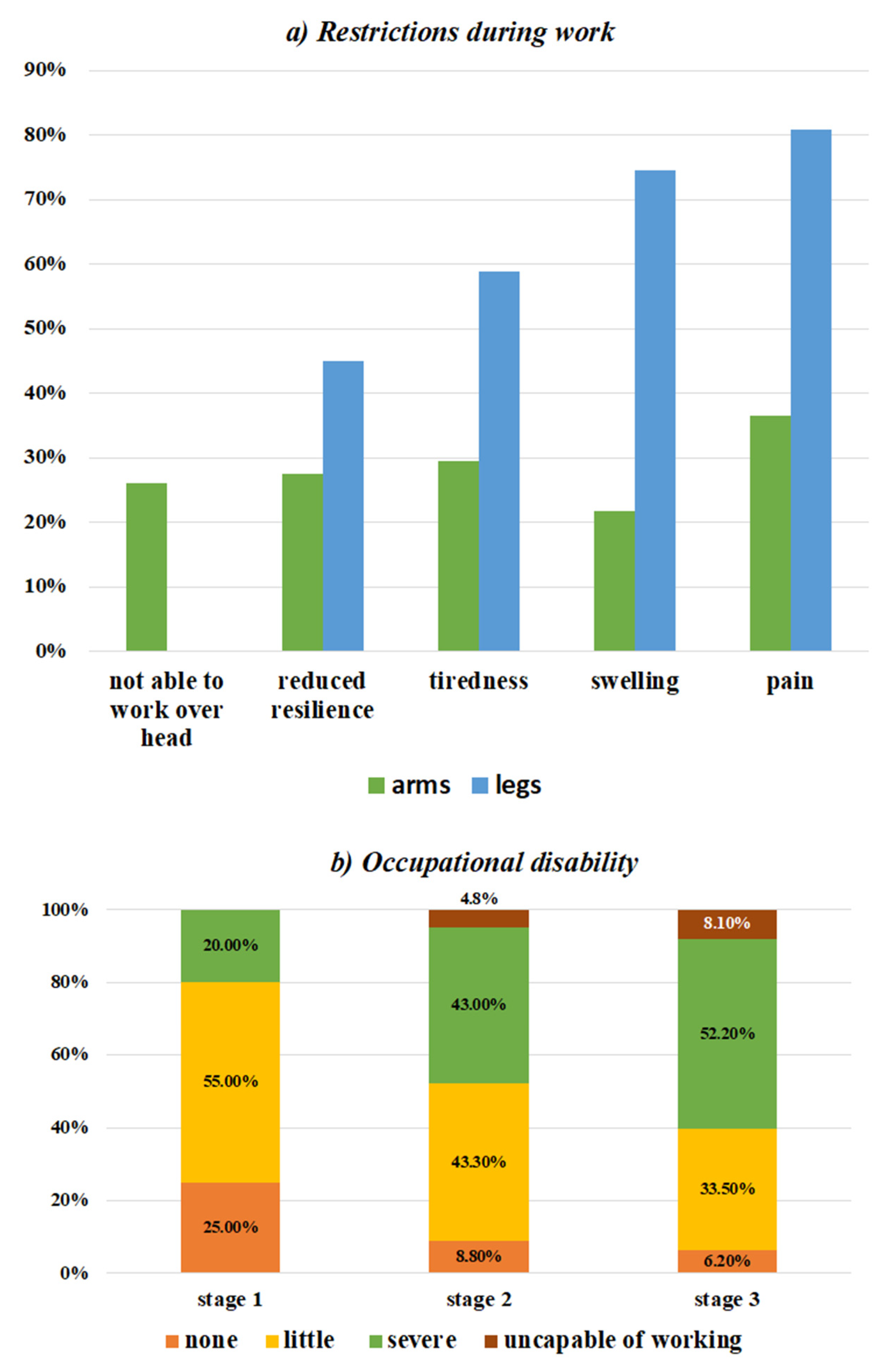
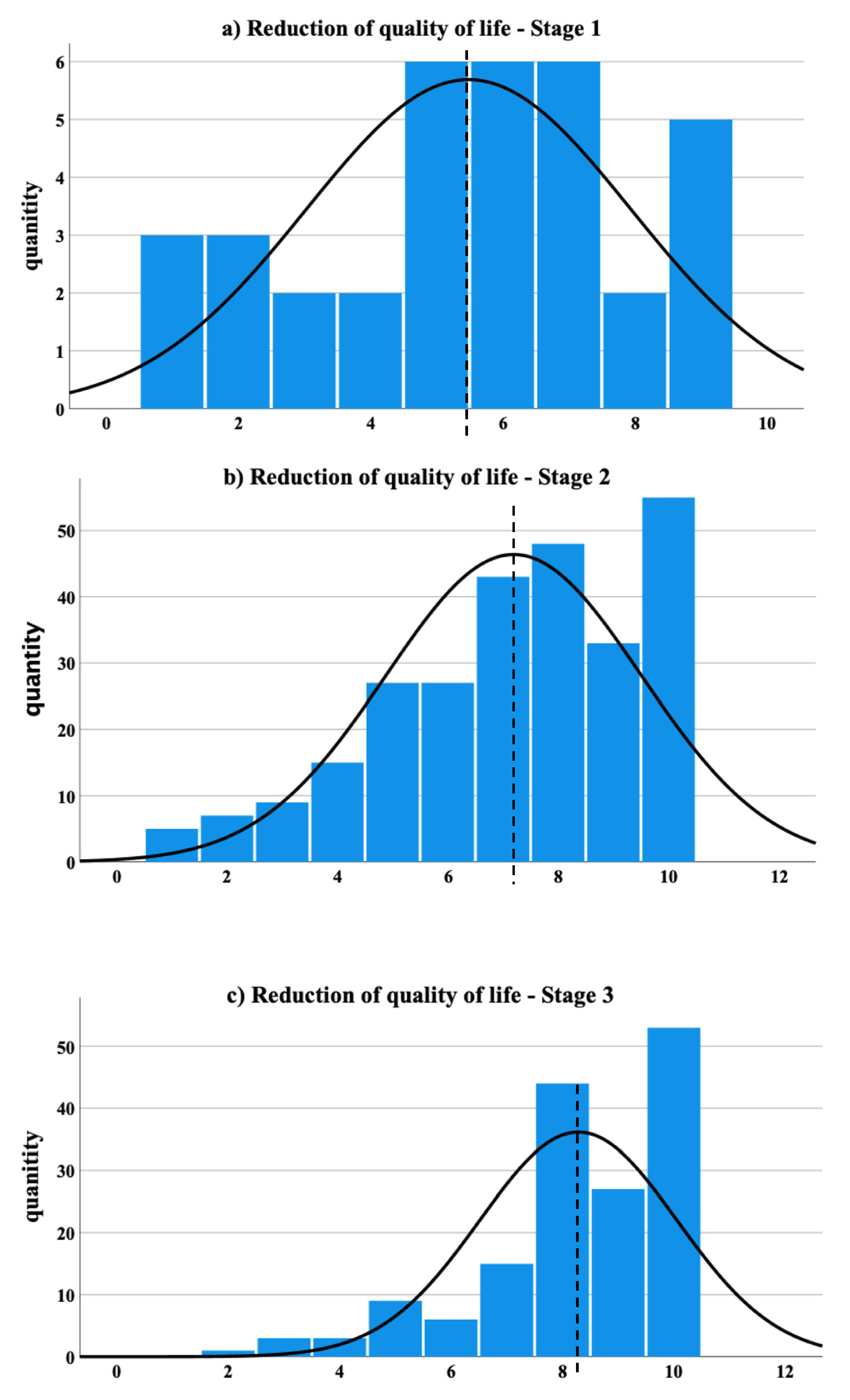
3.4. Symptoms
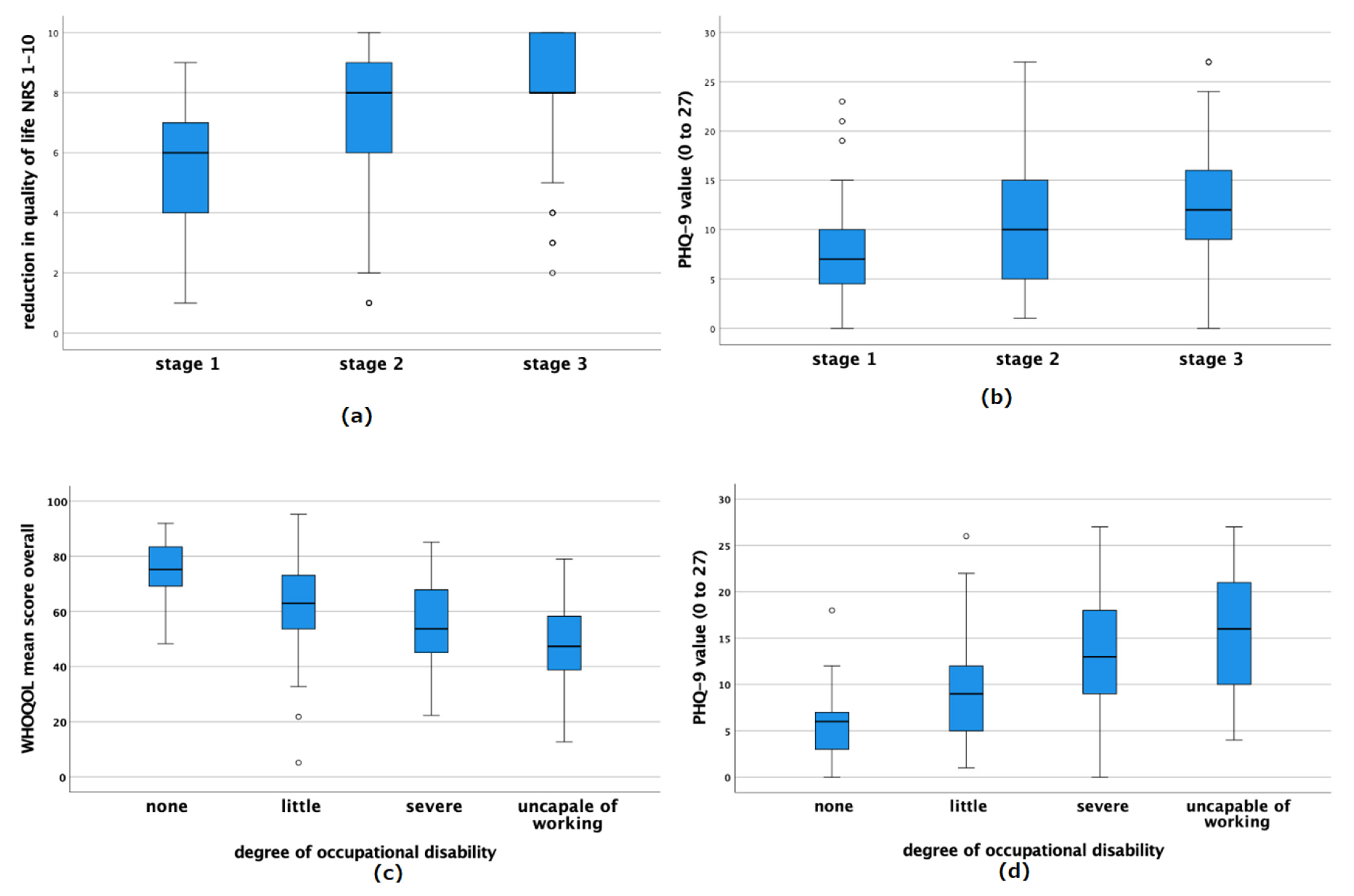
3.5. Effects on Daily Life
3.6. Mental State

4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A

| Name: | |
| Date of Birth: | |
| Date: | |
| Body size (in cm): | |
| Body weight currently (in kg): | |
| Former maximum weight (kg): | |
| Former minimum weight (kg): | |
| At what age were the first signs of increased fatty tissue on the legs? |
|
| At what age was the diagnosis of lipedema made? | |
| Which areas were affected first? |
|
| Which areas are affected now? |
|
| Who in your family suffers from lipedema or noticeably thick legs? |
|
| what do you do professionally? | |
| What discomfort do your legs give you during work? |
|
| What discomfort do your arms give you during work? |
|
| How would you rate the limitation of your ability to work due to lipedema? It affects me: |
Since: |
| Have you tried any dietary changes or diets? |
|
| If so, how many kg of weight did you lose: |
|
| Has help been sought for this? |
|
| Do you do any kind of sport? |
|
| Did you receive manual lymphatic drainage? |
|
| If yes, since when or in what period? How many times a week? |
|
| If so, does lymphatic drainage help or did it help? |
|
| Do you wear flat knit compression garments? |
|
| If yes, since when or during what period? |
|
| Have you already had liposuction?If yes, on which body region and how much? (Amount in liters) |
|
| Please provide information about your personal medical history. |
|
| Have you had a thrombosis or is thrombosis known to occur in relatives? |
|
| Do you take medications regularly, if so, which ones? | |
| Do you need to take pain medication due to pain from your lipedema? |
|
| Are allergies known? (especially to antibiotics and local anesthetics). | |
| Do you smoke? If yes, how much daily? |
|
| Mark Applicable Intensity with X | |
|---|---|
| Do you have pain in the affected areas? | none very strong ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ 1 2 3 4 5 6 7 8 9 10 |
| Pain in the lower legs: (leave blank if none) | none very strong ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ 1 2 3 4 5 6 7 8 9 10 |
| Pain in the thighs: (leave blank if none): | none very strong ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ 1 2 3 4 5 6 7 8 9 10 |
| Pain in the buttock: (leave blank if none): | none very strong ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ 1 2 3 4 5 6 7 8 9 10 |
| Pain in the belly: (leave blank if none): | none very strong ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ 1 2 3 4 5 6 7 8 9 10 |
| Pain in the arms: (leave blank if none): | none very strong ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ 1 2 3 4 5 6 7 8 9 10 |
| Is there sensitivity to touch or pressure pain? | none very strong ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ 1 2 3 4 5 6 7 8 9 10 |
| Are you prone to bruising (hematomas)? | none very strong ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ 1 2 3 4 5 6 7 8 9 10 |
| Is there a feeling of tension in the legs? | none very strong ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ 1 2 3 4 5 6 7 8 9 10 |
| Is there a feeling of warmth in the legs? | none very strong ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ 1 2 3 4 5 6 7 8 9 10 |
| Is there a feeling of cold in the legs? | none very strong ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ 1 2 3 4 5 6 7 8 9 10 |
| Do you have muscle cramps? | none very strong ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ 1 2 3 4 5 6 7 8 9 10 |
| Is there a feeling of heavy legs? | none very strong ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ 1 2 3 4 5 6 7 8 9 10 |
| Is there a feeling of tired legs? | none very strong ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ 1 2 3 4 5 6 7 8 9 10 |
| Does swelling occur? | none very strong ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ 1 2 3 4 5 6 7 8 9 10 |
| Do skin complications occur? | none very strong ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ 1 2 3 4 5 6 7 8 9 10 |
| Is there itching? | none very strong ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ 1 2 3 4 5 6 7 8 9 10 |
| Are there any restrictions on walking? | none very strong ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ 1 2 3 4 5 6 7 8 9 10 |
| How would you rate the reduction in your quality of life? | none very strong ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ 1 2 3 4 5 6 7 8 9 10 |
| How satisfied are you with the appearance of your legs? | Very satisfied very unsafisfied ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ ⬜ 1 2 3 4 5 6 7 8 9 10 |
References
- Wold, L.E.; Hines, E.A., Jr.; Allen, E.V. Lipedema of the legs; a syndrome characterized by fat legs and edema. Ann. Intern. Med. 1951, 34, 1243–1250. [Google Scholar] [CrossRef] [PubMed]
- Allen, E.V.; Hines, E.A. Lipedema of the Legs: A Syndrome Characterized by Fat Legs and Orthostatic Edema. Lipedema Project. 1940. Available online: https://lipedemaproject.org/mayo-clinic-staff-meetings-vascular-clinics-x-lipedema (accessed on 16 August 2020).
- Dudek, J.E.; Białaszek, W.; Ostaszewski, P.; Smidt, T. Depression and appearance-related distress in functioning with lipedema. Psychol. Health Med. 2018, 23, 846–853. [Google Scholar] [CrossRef] [PubMed]
- Herpertz, U. Krankheitsspektrum des Lipödems an einer lyphologischen Fachklinik. Vasomed. Lymphologie 1997, 5, 301–307. [Google Scholar]
- Herpertz, U. Lipedema. Z Lymphologie 1995, 19, 1–7. [Google Scholar]
- Marshall, M.; Schwahn-Schreiber, C. Prävalenz des Lipödems bei berufstätigen Frauen in Deutschland: (Lipödem-3-Studie). Phlebologie 2011, 40, 127–134. [Google Scholar]
- Romeijn, J.R.M.; de Rooij, M.J.M.; Janssen, L.; Martens, H. Exploration of patient characteristics and quality of life in patients with lipoedema using a survey. Dermatol. Ther. 2018, 8, 303–311. [Google Scholar] [CrossRef] [Green Version]
- Bauer, A.T.; von Lukowicz, D.; Lossagk, K.; Aitzetmueller, M.; Moog, P.; Cerny, M.; Erne, H.; Schmauss, D.; Duscher, D.; Machens, H.G. New insights on lipedema: The enigmatic disease of the peripheral fat. Plast Reconstr Surg. 2019, 144, 1475–1484. [Google Scholar] [CrossRef]
- Tiwari, A.; Myint, F.; Hamilton, G. Management of lower limb lymphoedema in the United Kingdom. Eur. J. Vasc. Endovasc. Surg. 2006, 31, 311–315. [Google Scholar] [CrossRef] [Green Version]
- Herbst, K.L. Rare adipose disorders (RADs) masquerading as obesity. Acta Pharmacol. Sin. 2012, 33, 155–172. [Google Scholar] [CrossRef] [Green Version]
- Ghods, M.; Georgiou, I.; Schmidt, J.; Kruppa, P. Disease progression and comorbidities in lipedema patients: A 10-year retrospective analysis. Dermatol. Ther. 2020, 33, e14534. [Google Scholar] [CrossRef]
- Herbst, K.L.; Mirkovskaya, L.; Bharhagava, A.; Chava, Y.; Te, C.H.T. Lipedema fat and signs and symptoms of illness, increase with advancing stage. Arch. Med. 2015, 7, 8. [Google Scholar]
- Witte, T.; Dadras, M.; Heck, F.-C.; Heck, M.; Habermalz, B.; Welss, S.; Lehnhardt, M.; Behr, B. Water-jet-assisted liposuction for the treatment of lipedema: Standardized treatment protocol and results of 63 patients. J. Plast. Reconstr. Aesthetic Surg. 2020, 73, 1637–1644. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, A.; Hueppe, M.; Meier-Vollrath, I.; Schmeller, W. Improvements in patients with lipedema 4, 8 and 12 years after liposuction. Phlebol. J. Venous Dis. 2020, 36, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Dadras, M.; Mallinger, P.J.; Corterier, C.C.; Theodosiadi, S.; Ghods, M. Liposuction in the treatment of lipedema: A longitudinal study. Arch. Plast. Surg. 2017, 44, 324–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rapprich, S.; Dingler, A.; Podda, M. Liposuction is an effective treatment for lipedema-results of a study with 25 patients: Liposuction in lipedema. JDDG J. Dtsch. Dermatol. Ges. 2011, 9, 33–40. [Google Scholar] [PubMed]
- Dudek, J.E.; Białaszek, W.; Gabriel, M. Quality of life, its factors, and sociodemographic characteristics of Polish women with lipedema. BMC Womens Health 2021, 21, 27. [Google Scholar] [CrossRef] [PubMed]
- Meier-Vollrath, I.; Schneider, W.; Schmeller, W. Lipödem: Verbesserte Lebensqualität durch Therapiekombination. Dtsch. Ärztebl. 2005, 7, A1061–A1067. [Google Scholar]
- Schmeller, W.; Meier-Vollrath, I. Lipödem—Aktuelles zu einem weitgehend unbekannten Krankheitsbild. Aktuelle Dermatol. 2007, 33, 251–260. [Google Scholar] [CrossRef] [Green Version]
- Paling, I.; MacIntyre, L. Survey of lipoedema symptoms and experience with compression garments. Br. J. Community Nurs. 2020, 25, S17–S22. [Google Scholar] [CrossRef]
- Deri, G.; Weissleder, H. Vergleichende prä-und posttherapeutische Volumenmessungen in Beinsegmenten beim Lipödem. Lymph Forsch. 1997, 1, 35–37. [Google Scholar]
- Szolnoky, G.; Borsos, B.; Bársony, K.; Balogh, M.; Kemény, L. Complete decongestive physiotherapy with and without pneumatic compression for treatment of lipedema: A pilot study. Lymphology 2008, 41, 40–44. [Google Scholar] [PubMed]
- Schlosshauer, T.; Heiss, C.; von Hollen, A.; Spennato, S.; Rieger, U.M. Liposuction treatment improves disease-specific quality of life in lipoedema patients. Int. Wound J. 2021, 18, 923–931. [Google Scholar] [CrossRef] [PubMed]
- Berlim, M.T.; Pavanello, D.P.; Caldieraro, M.A.; Fleck, M.P.A. Reliability and validity of the WHOQOL BREF in a sample of Brazilian outpatients with major depression. Qual. Life Res. 2005, 14, 561–564. [Google Scholar] [CrossRef] [PubMed]
- Kalfoss, M.H.; Reidunsdatter, R.J.; Klöckner, C.A.; Nilsen, M. Validation of the WHOQOL-BREF: Psychometric properties and normative data for the Norwegian general population. Health Qual. Life Outcomes 2021, 19, 13. [Google Scholar] [CrossRef] [PubMed]
- Whoqol Group. Development of the World Health Organization WHOQOL-BREF quality of life assessment. Psychol. Med. 1998, 28, 551–558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gunzelmann, T.; Brähler, E.C.; Angermeyer, R.K.; Matschinger, H. Deutschsprachige Version der WHO Instrumente zur Erfassung von Lebensqualität WHOQOL-100 und WHOQOL-BREFM. 2002. Available online: https://www.semanticscholar.org/paper/C.-Angermeyer%2C-R.-Kilian-%26-H.-Matschinger%3A-Version-Gunzelmann-Br%C3%A4hler/725ce6eb69e18a7c5d1835cee58cf16e43ab26ea (accessed on 20 December 2021).
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Arroll, B.; Goodyear-Smith, F.; Crengle, S.; Gunn, J.; Kerse, N.; Fishman, T.; Falloon, K.; Hatcher, S. Validation of PHQ-2 and PHQ-9 to screen for major depression in the primary care population. Ann. Fam. Med. 2010, 8, 348–353. [Google Scholar] [CrossRef] [Green Version]
- Dudek, J.E.; Białaszek, W.; Ostaszewski, P. Quality of life in women with lipoedema: A contextual behavioral approach. Qual. Life Res. 2015, 25, 401–408. [Google Scholar] [CrossRef]
- Wollina, U.; Heinig, B. Treatment of lipedema by low-volume micro-cannular liposuction in tumescent anesthesia: Results in 111 patients. Dermatol. Ther. 2019, 32, e12820. [Google Scholar] [CrossRef]
- Sanyal, D.; Raychaudhuri, M. Hypothyroidism and obesity: An intriguing link. Indian J. Endocrinol. Metab. 2016, 20, 554–557. [Google Scholar] [CrossRef]
- Taylor, P.N.; Albrecht, D.; Scholz, A.; Gutierrez-Buey, G.; Lazarus, J.H.; Dayan, C.M.; Okosieme, O.E. Global epidemiology of hyperthyroidism and hypothyroidism. Nat. Rev. Endocrinol. 2018, 14, 301–316. [Google Scholar] [CrossRef]
- Gouda, P.; Zheng, S.; Peters, T.; Fudim, M.; Randhawa, V.K.; Ezekowitz, J.; Mavrakanas, T.A.; Giannetti, N.; Tsoukas, M.; Lopes, R.; et al. Clinical phenotypes in patients with type 2 diabetes mellitus: Characteristics, cardiovascular outcomes and treatment strategies. Curr. Heart Fail. Rep. 2021, 18, 253–263. [Google Scholar] [CrossRef] [PubMed]
- Al-Goblan, A.S.; Al-Alfi, M.A.; Khan, M.Z. Mechanism linking diabetes mellitus and obesity. Diabetes Metab. Syndr. Obes. Targets Ther. 2014, 7, 587–591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keith, L.; Seo, C.; Rowsemitt, C.; Pfeffer, M.; Wahi, M.; Staggs, M.; Dudek, J.; Gower, B.; Carmody, M. Ketogenic diet as a potential intervention for lipedema. Med. Hypotheses 2020, 146, 110435. [Google Scholar] [CrossRef]
- Di Renzo, L.; Cinelli, G.; Romano, L.; Zomparelli, S.; De Santis, G.L.; Nocerino, P.; Bigioni, G.; Arsini, L.; Cenname, G.; Pujia, A.; et al. Potential effects of a modified mediterranean diet on body composition in lipoedema. Nutrients 2021, 13, 358. [Google Scholar] [CrossRef]
- Macias, N.; Alemán-Mateo, H.; Esparza-Romero, J.; Valencia, M.E. Body fat measurement by bioelectrical impedance and air displacement plethysmography: A cross-validation study to design bioelectrical impedance equations in Mexican adults. Nutr. J. 2007, 6, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sartorio, A.; Malavolti, M.; Agosti, F.; Marinone, P.G.; Caiti, O.; Battistini, N.; Bedogni, G. Body water distribution in severe obesity and its assessment from eight-polar bioelectrical impedance analysis. Eur. J. Clin. Nutr. 2004, 59, 155–160. [Google Scholar] [CrossRef] [Green Version]
- Utter, A.C.; Lambeth, P.G. Evaluation of multifrequency bioelectrical impedance analysis in assessing body composition of wrestlers. Med. Sci. Sports Exerc. 2010, 42, 361–367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gibson, A.L.; Holmes, J.C.; Desautels, R.L.; Edmonds, L.B.; Nuudi, L. Ability of new octapolar bioimpedance spectroscopy analyzers to predict 4-component-model percentage body fat in Hispanic, black, and white adults. Am. J. Clin. Nutr. 2008, 87, 332–338. [Google Scholar] [CrossRef] [Green Version]
- Child, A.H.; Gordon, K.D.; Sharpe, P.; Brice, G.; Ostergaard, P.; Jeffery, S.; Mortimer, P.S. Lipedema: An inherited condition. Am. J. Med. Genet. Part A 2010, 152, 970–976. [Google Scholar] [CrossRef]
- Michelini, S.; Chiurazzi, P.; Marino, V.; Dell’Orco, D.; Manara, E.; Baglivo, M.; Fiorentino, A.; Maltese, P.E.; Pinelli, M.; Herbst, K.L.; et al. Aldo-Keto reductase 1C1 (AKR1C1) as the first mutated gene in a family with nonsyndromic primary lipedema. Int. J. Mol. Sci. 2020, 21, 6264. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, A.; Hueppe, M.; Schmeller, W. Long-term benefit of liposuction in patients with lipoedema: A follow-up study after an average of 4 and 8 years. Br. J. Dermatol. 2015, 174, 1061–1067. [Google Scholar] [CrossRef]
- Schmeller, W.; Hueppe, M.; Meier-Vollrath, I. Tumescent liposuction in lipoedema yields good long-term results: Tumescent liposuction in lipoedema. Br. J. Dermatol. 2012, 166, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Schmeller, W.; Meier-Vollrath, I. Tumescent liposuction: A new and successful therapy for lipedema. J. Cutan. Med. Surg. 2006, 10, 7–10. [Google Scholar] [CrossRef]




| Age at Presentation | Mean 40.16 (±12.45) |
|---|---|
| Weight at presentation | mean 96.16 kg (±23.11) |
| BMI at presentation | mean 33.13 (±7.8) |
| BMI < 18.5 | 0.0% |
| BMI 18.5 to 24.99 | 11.7% |
| BMI 25 to 29.99 | 23.2% |
| BMI 30 to 34.99 (obesity I°) | 24.2% |
| BMI 35 to 39.99 (obesity II°) | 19.6% |
| BMI > 40 (obesity III°) | 20.2% |
| Age at onset of symptoms | mean 19.66 (±10.00) |
| Age at diagnosis | mean 36.69 (±11.79) |
| years between onset and diagnosis | mean 16.11 (±11.39) |
| BMI stage I | mean 24.71 ± 3.61 |
| BMI stage II | mean 32.11 ± 6.00 |
| BMI stage III | mean 39.33 ± 7.53 |
| Stage I legs (at presentation) | 8.6% |
| Stage II legs | 57.8% |
| Stage III legs | 33.6% |
| Stage I arms | 11.8% |
| Stage II arms | 36.0% |
| Stage III arms | 9.9% |
| Stage 0 arms | 42.3% |
| Smoking behavior | 87.2%—nonsmoker 6.4%—<5 per day 3.4%—5–10 per day 1.8%—11–15 per day 1.2%—16–20 per day |
| Comorbidities | 75.9% |
| hypothyroidism | 31.3% |
| joint pain | 27.3% |
| Skin problems | 19.2% |
| Hypertonia | 18.5% |
| 10.2% patient | |
| thrombosis | 9.3% only family member |
| Type 2 diabetes | 3.0% |
| Symptoms | mean (±SD) (n = 511) |
| Feeling of “heavy” legs | 8.21 (±1.95) |
| Feeling of tired legs | 7.79 (±2.17) |
| Bruising (hematomas) | 7.63 (±2.31) |
| Feeling of tension in the legs | 7.49 (±2.19) |
| Hypersensitivity to touch | 7.32 (±2.42) |
| Swelling | 7.04 (±2.41) |
| Pain in the affected areas | 6.68 (±2.32) |
| Impairment in walking | 6.45 (±2.78) |
| Pain in thighs: | 6.34 (±2.5) |
| Pain in lower legs: | 6.18 (±2.53) |
| Pain in arms: | 5.33 (±2.72) |
| Feeling of cold in the legs | 5.11 (±3.21) |
| Feeling of warmth in the legs | 4.92 (±3.01) |
| Itching | 4.78 (±3.00) |
| Pain in buttock: | 4.65 (±2.62) |
| muscle cramps | 4.63 (±2.86) |
| Skin complications | 4.11 (±2.98) |
| Pain in belly: | 4.00 (±2.72) |
| Family Member | Affected (n = 511) |
|---|---|
| mother | 33.6% |
| grandmother (in general) | 28.4% |
| grandmother maternal | 15.4% |
| sister | 14.6% |
| grandmother paternal | 10.3% |
| aunt paternal | 9.8% |
| aunt maternal | 9.2% |
| daughter | 2.3% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hamatschek, M.; Knors, H.; Klietz, M.-L.; Wiebringhaus, P.; Aitzetmueller, M.; Hirsch, T.; Kueckelhaus, M. Characteristics and Patient Reported Outcome Measures in Lipedema Patients—Establishing a Baseline for Treatment Evaluation in a High-Volume Center. J. Clin. Med. 2022, 11, 2836. https://doi.org/10.3390/jcm11102836
Hamatschek M, Knors H, Klietz M-L, Wiebringhaus P, Aitzetmueller M, Hirsch T, Kueckelhaus M. Characteristics and Patient Reported Outcome Measures in Lipedema Patients—Establishing a Baseline for Treatment Evaluation in a High-Volume Center. Journal of Clinical Medicine. 2022; 11(10):2836. https://doi.org/10.3390/jcm11102836
Chicago/Turabian StyleHamatschek, Matthias, Henning Knors, Marie-Luise Klietz, Philipp Wiebringhaus, Matthias Aitzetmueller, Tobias Hirsch, and Maximilian Kueckelhaus. 2022. "Characteristics and Patient Reported Outcome Measures in Lipedema Patients—Establishing a Baseline for Treatment Evaluation in a High-Volume Center" Journal of Clinical Medicine 11, no. 10: 2836. https://doi.org/10.3390/jcm11102836