
Cardiovascular Safety Profile of Romosozumab: A Pharmacovigilance Analysis of the US Food and Drug Administration Adverse Event Reporting System (FAERS)

 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Data Source
2.2. Study Population
2.3. Outcomes of Interest
2.4. Statistical Analysis
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Appendix A
| Event of interest | All other events | |
| Romosozumab | a | b |
| All other drugs in FAERS | c | d |
| Information component (IC): | Reporting odds ratio (ROR): | |
| Equation 1. Formulas for disproportionality measures. Abbreviations: FAERS: Food and Drug Administration Adverse Event Reporting System, obs: observed, exp: expected, CI: confidence interaval. | ||
References
- Saag, K.G.; Petersen, J.; Brandi, M.L.; Karaplis, A.C.; Lorentzon, M.; Thomas, T.; Maddox, J.; Fan, M.; Meisner, P.D.; Grauer, A. Romosozumab or Alendronate for Fracture Prevention in Women with Osteoporosis. N. Engl. J. Med. 2017, 377, 1417–1427. [Google Scholar] [CrossRef] [Green Version]
- Cosman, F.; Crittenden, D.B.; Adachi, J.D.; Binkley, N.; Czerwinski, E.; Ferrari, S.; Hofbauer, L.C.; Lau, E.; Lewiecki, E.M.; Miyauchi, A.; et al. Romosozumab Treatment in Postmenopausal Women with Osteoporosis. N. Engl. J. Med. 2016, 375, 1532–1543. [Google Scholar] [CrossRef]
- Markham, A. Romosozumab: First Global Approval. Drugs 2019, 79, 471–476. [Google Scholar] [CrossRef]
- European Medicines Agency: Committee for Medicinal Products for Human Use (CHMP) Evenity Assessment Report. Available online: www.ema.europa.eu/contact (accessed on 5 February 2021).
- Government of Canada. Summary Basis of Decision-Evenity-Health Canada. Available online: https://hpr-rps.hres.ca/reg-content/summary-basis-decision-detailTwo.php?linkID=SBD00451#paatDiv (accessed on 5 February 2021).
- US Food and Drug Administration: Center for Drug Evaluation and Research. Other Action Letters: Evenity. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2019/761062Orig1s000OtherActionLtrs.pdf (accessed on 5 February 2021).
- Regulatory Decision Summary—Evenity—Health Canada. Available online: https://hpr-rps.hres.ca/reg-content/regulatory-decision-summary-detail.php?linkID=RDS00525 (accessed on 5 February 2021).
- FDA Approves New Treatment for Osteoporosis in Postmenopausal Women at High Risk of Fracture. Available online: https://www.fda.gov/news-events/press-announcements/fda-approves-new-treatment-osteoporosis-postmenopausal-women-high-risk-fracture (accessed on 5 February 2021).
- Evenity: European Medicines Agency. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/evenity (accessed on 5 February 2021).
- Pharmaceuticals and Medical Devices Agency. Summary of Investigation Results Romosozumab (Genetical Recombination); Pharmaceuticals and Medical Devices Agency: Tokyo, Japan, 2019.
- Revision of Precautions Romosozumab (Genetical Recombination) Therapeutic Category Hormones-Miscellaneous; Pharmaceuticals and Medical Devices Agency: Tokyo, Japan, 2019.
- US Food and Drug Administration. Center for Drug Evaluation and Research. Multi-Disciplinary Review: Evenity; US Food and Drug Administration: Silver Spring, MD, USA, 2020.
- Michael Lewiecki, E.; Blicharski, T.; Goemaere, S.; Lippuner, K.; Meisner, P.D.; Miller, P.D.; Miyauchi, A.; Maddox, J.; Chen, L.; Horlait, S. A Phase III Randomized Placebo-Controlled Trial to Evaluate Efficacy and Safety of Romosozumab in Men with Osteoporosis. J. Clin. Endocrinol. Metab. 2018, 103, 3183–3193. [Google Scholar] [CrossRef] [Green Version]
- Kawaguchi, H. Serious Adverse Events with Romosozumab Use in Japanese Patients: Need for Clear Formulation of Contraindications Worldwide. J. Bone Miner. Res. 2020, 35, 994–995. [Google Scholar] [CrossRef]
- Miyauchi, A.; Hamaya, E.; Yang, W.; Nishi, K.; Libanati, C.; Tolman, C.; Shimauchi, J. Romosozumab followed by denosumab in Japanese women with high fracture risk in the FRAME trial. J. Bone Miner. Metab. 2020, 39, 278–288. [Google Scholar] [CrossRef]
- Cummings, S.R.; McCulloch, C. Explanations for the difference in rates of cardiovascular events in a trial of alendronate and romosozumab. Osteoporos. Int. 2020, 31, 1019–1021. [Google Scholar] [CrossRef] [Green Version]
- Kaveh, S.; Hosseinifard, H.; Ghadimi, N.; Vojdanian, M.; Aryankhesal, A. Efficacy and safety of Romosozumab in treatment for low bone mineral density: A systematic review and meta-analysis. Clin. Rheumatol. 2020, 39, 3261–3276. [Google Scholar] [CrossRef]
- Turk, J.R.; Deaton, A.M.; Yin, J.; Stolina, M.; Felx, M.; Boyd, G.; Bienvenu, J.G.; Varela, A.; Guillot, M.; Holdsworth, G.; et al. Nonclinical cardiovascular safety evaluation of romosozumab, an inhibitor of sclerostin for the treatment of osteoporosis in postmenopausal women at high risk of fracture. Regul. Toxicol. Pharmacol. 2020, 115, 104697. [Google Scholar] [CrossRef]
- Fixen, C.; Tunoa, J. Romosozumab: A Review of Efficacy, Safety, and Cardiovascular Risk. Curr. Osteoporos. Rep. 2021, 19, 15–22. [Google Scholar]
- MedWatch: The FDA Safety Information and Adverse Event Reporting Program FDA. Available online: https://www.fda.gov/safety/medwatch-fda-safety-information-and-adverse-event-reporting-program (accessed on 24 February 2021).
- FDA Adverse Events Reporting System (FAERS) Public Dashboard Sheets—Qlik Sense. Available online: https://fis.fda.gov/sense/app/d10be6bb-494e-4cd2-82e4-0135608ddc13/sheet/7a47a261-d58b-4203-a8aa-6d3021737452/state/analysis (accessed on 24 February 2021).
- EudraVigilance: European Medicines Agency. Available online: https://www.ema.europa.eu/en/human-regulatory/research-development/pharmacovigilance/eudravigilance (accessed on 9 March 2021).
- Uppsala Monitoring Centre VigiBase. Available online: https://www.who-umc.org/vigibase/vigibase/ (accessed on 5 February 2021).
- Vogel, U.; van Stekelenborg, J.; Dreyfus, B.; Garg, A.; Habib, M.; Hosain, R.; Wisniewski, A. Investigating Overlap in Signals from EVDAS, FAERS, and VigiBase®. Drug Saf. 2020, 43, 351–362. [Google Scholar] [CrossRef] [Green Version]
- Coloma, P.M.; Trifirò, G.; Patadia, V.; Sturkenboom, M. Postmarketing safety surveillance: Where does signal detection using electronic healthcare records fit into the big picture? Drug Saf. 2013, 36, 183–197. [Google Scholar] [CrossRef]
- FDA Adverse Event Reporting System (FAERS): Latest Quarterly Data Files FDA. Available online: https://www.fda.gov/drugs/questions-and-answers-fdas-adverse-event-reporting-system-faers/fda-adverse-event-reporting-system-faers-latest-quarterly-data-files (accessed on 24 February 2021).
- Bate, A.; Evans, S.J.W. Quantitative signal detection using spontaneous ADR reporting. Pharmacoepidemiol. Drug Saf. 2009, 18, 427–436. [Google Scholar]
- Montastruc, J.L.; Sommet, A.; Bagheri, H.; Lapeyre-Mestre, M. Benefits and strengths of the disproportionality analysis for identification of adverse drug reactions in a pharmacovigilance database. Br. J. Clin. Pharmacol. 2011, 72, 905–908. [Google Scholar] [CrossRef] [Green Version]
- Egberts, A.C.G.; Meyboom, R.H.B.; Van Puijenbroek, E.P. Use of measures of disproportionality in pharmacovigilance: Three Dutch examples. In Proceedings of the Drug Safety; Adis International Ltd.: Auckland, New Zealand, 2002; Volume 25, pp. 453–458. [Google Scholar]
- Vienna: R Foundation for Statistical Computing. R: A Language and Environment for Statistical Computing. Available online: https://www.r-project.org/ (accessed on 5 February 2021).
- GraphPad Prism Version 8.0.0. San Diego, CA: GraphPad Software. Available online: https://www.graphpad.com/ (accessed on 5 February 2021).
- Liu, Y.; Cao, Y.; Zhang, S.; Zhang, W.; Zhang, B.; Tang, Q.; Li, Z.; Wu, J. Romosozumab treatment in postmenopausal women with osteoporosis: A meta-analysis of randomized controlled trials. Climacteric 2018, 21, 189–195. [Google Scholar]
- Millett, E.R.C.; Peters, S.A.E.; Woodward, M. Sex differences in risk factors for myocardial infarction: Cohort study of UK Biobank participants. BMJ 2018, 363. [Google Scholar] [CrossRef] [Green Version]
- McClung, M.; Miller, P.; Recknor, C.; Mesenbrink, P.; Bucci-Rechtweg, C.; Benhamou, C.-L. Zoledronic acid for the prevention of bone loss in postmenopausal women with low bone mass: A randomized controlled trial. Obstet. Gynecol. 2009, 114, 999–1007. [Google Scholar] [CrossRef]
- Nomura, K.; Takahashi, K.; Hinomura, Y.; Kawaguchi, G.; Matsushita, Y.; Marui, H.; Anzai, T.; Hashiguchi, M.; Mochizuki, M. Effect of database profile variation on drug safety assessment: An analysis of spontaneous adverse event reports of Japanese cases. Drug Des. Dev. Ther. 2015, 9, 3031–3041. [Google Scholar] [CrossRef] [Green Version]
- Bovijn, J.; Krebs, K.; Chen, C.Y.; Boxall, R.; Censin, J.C.; Ferreira, T.; Pulit, S.L.; Glastonbury, C.A.; Laber, S.; Millwood, I.Y.; et al. Evaluating the cardiovascular safety of sclerostin inhibition using evidence from meta-analysis of clinical trials and human genetics. Sci. Transl. Med. 2020, 12. [Google Scholar] [CrossRef]
- Tankó, L.B.; Christiansen, C.; Cox, D.A.; Geiger, M.J.; McNabb, M.A.; Cummings, S.R. Relationship Between Osteoporosis and Cardiovascular Disease in Postmenopausal Women. J. Bone Miner. Res. 2005, 20, 1912–1920. [Google Scholar] [CrossRef] [Green Version]
- Schneeweiss, S.; Gagne, J.J.; Glynn, R.J.; Ruhl, M.; Rassen, J.A. Assessing the comparative effectiveness of newly marketed medications: Methodological challenges and implications for drug development. Clin. Pharmacol. Ther. 2011, 90, 777–790. [Google Scholar] [CrossRef]



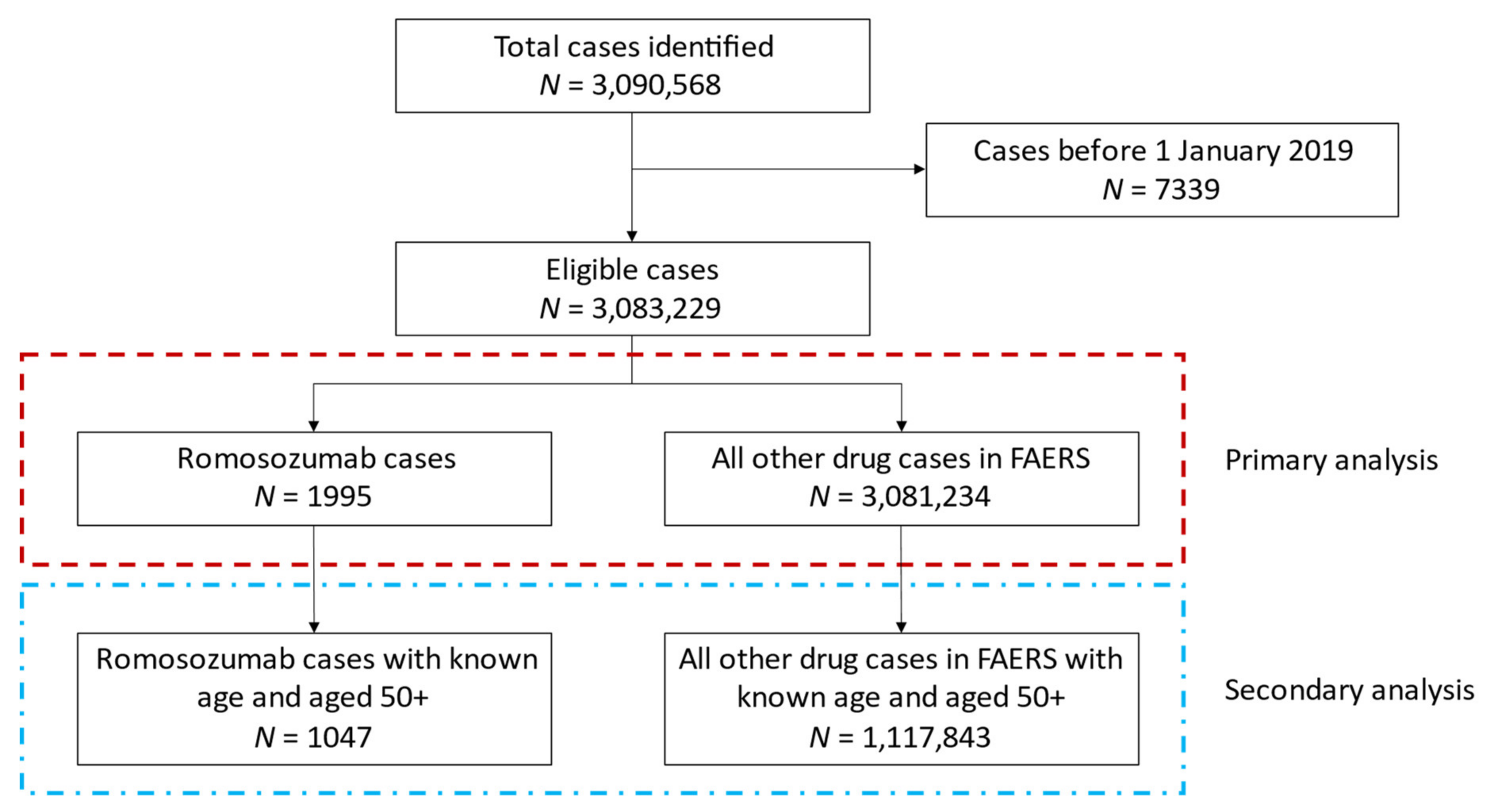{kind=link}
{kind=link}
| Total | United States | Japan | |
|---|---|---|---|
| 1995 | 787 (39.4%) | 1188 (59.5%) | |
| Sex | |||
| Female | 1518 (76.1%) | 833 (70.1%) † | 16 (80.0%) |
| Male | 177 (8.9%) | 154 (13.0%) † | <5 |
| Unknown | 300 (15.0%) | 201 (16.9%) | <5 |
| Age | |||
| Mean (SD) | 77.0 (10.2) | 71.7 (8.5) | 80.2 (9.5) † |
| 18–59 | 46 (2.3%) | 29 (3.7%) | 16 (1.4%) † |
| 60–69 | 175 (16.6%) | 117 (14.9%) | 55 (4.6%) † |
| 70–79 | 385 (36.4%) | 167 (21.2%) | 211 (17.8%) |
| 80+ | 451 (42.7%) | 70 (8.9%) | 380 (32.0%) † |
| Unknown age | 938 (47.0%) | 404 (51.3%) | 526 (44.3%) † |
| Seriousness Criteria | |||
| Death | 176 (8.8%) | 18 (2.3%) | 158 (13.3%) † |
| Hospitalized or Required Intervention | 660 (33.1%) | 67 (8.5%) | 589 (49.6%) † |
| Life Threatening | 48 (2.4%) | 6 (0.8%) | 41 (3.5%) † |
| Disabled | 22 (1.1%) | 6 (0.8%) | 16 (1.3%) |
| Outcomes of Interest | |||
| Major Cardiovascular Event | 206 (10.3%) | 41 (5.2%) | 164 (13.8%) † |
| Myocardial Infarction | 42 (2.1%) | 13 (1.7%) | 28 (2.4%) |
| Stroke | 84 (4.2%) | 27 (3.4%) | 57 (4.8%) |
| Cardiovascular Death | 86 (4.3%) | <5 | 83 (7.0%) † |
| Other Cardiovascular Event | 58 (2.9%) | 16 (2.0%) | 42 (3.5%) |
| General cardiac events | 16 (0.8%) | 6 (0.8%) | 10 (0.8%) |
| Bleeding | 19 (1.0%) | -- | 19 (1.6%) |
| Thrombosis | 23 (1.2%) | 10 (1.3%) | 13 (1.1%) |
| Other reported cardiovascular drugs | |||
| Anticoagulants | 38 (1.9%) | 9 (1.1%) | 29 (2.4%) |
| Antiplatelets | 60 (3.0%) | 12 (1.5%) | 47 (4.0%) † |
| ACE inhibitors | 14 (0.7%) | 11 (1.4%) | <5 |
| Angiotensin receptor blockers | 65 (3.3%) | <5 | 61 (5.1%) |
| Beta-blockers | 47 (2.4%) | 14 (1.8%) | 33 (2.8%) |
| Calcium channel blockers | 99 (5.0%) | 8 (1.0%) | 91 (7.7%) † |
| Non-Cardiovascular | MACE | Other Cardiovascular | Any Cardiovascular * | |
|---|---|---|---|---|
| 1740 | 206 | 58 | 255 | |
| Sex | ||||
| Female | 1323 (76.0%) | 159 (77.2%) † | 43 (74.1%) | 195 (76.5%) |
| Male | 143 (8.2%) | 30 (14.6%) † | 5 (8.6%) | 34 (13.3%) |
| Unknown | 274 (15.7%) | 17 (8.3%) † | 10 (17.2%) | 26 (10.2%) |
| Age | ||||
| Mean (SD) | 76.4 (9.9) | 81.2 (9.5) † | 79.0 (7.3) | 81.1 (9.9) |
| 18–59 | 41 (2.3%) | 5 (2.4%) | -- | 5 (2.0%) |
| 60–69 | 165 (9.5%) | 6 (2.9%) † | 4 (6.9%) | 10 (3.9%) |
| 70–79 | 324 (18.6%) | 53 (25.7%) † | 12 (20.7%) | 61 (23.9%) |
| 80+ | 335 (19.3%) | 98 (47.6%) † | 20 (34.5%) | 116 (45.5%) |
| Unknown age | 875 (50.3%) | 44 (21.4%) † | 22 (37.9%) | 63 (24.7%) |
| Region of reporting | ||||
| United States | 731 (42.0%) | 41 (19.9%) † | 16 (27.6%) | 56 (22.0%) |
| Japan | 990 (56.9%) | 164 (79.6%) † | 42 (72.4%) | 198 (77.6%) |
| Other | 19 (1.1%) | <5 | -- | <5 |
| Seriousness | ||||
| Death | 117 (6.7%) | 54 (26.2%) † | 7 (12.1%) | 59 (23.1%) |
| Hospitalized or Required Intervention | 526 (30.2%) | 117 (56.8%) † | 21 (36.2%) | 134 (52.5%) |
| Life Threatening | 19 (1.1%) | 24 (11.7%) † | 6 (10.3%) | 29 (11.4%) |
| Disabled | 10 (0.6%) | 12 (5.8%) † | -- | 12 (4.7%) |
| Other co-reported cardiovascular drugs | ||||
| Anticoagulants | 21 (1.2%) | 13 (6.3%) † | 4 (6.9%) | 17 (6.7%) |
| Antiplatelets | 34 (2.0%) | 22 (10.7%) † | 8 (13.8%) | 26 (10.2%) |
| ACE inhibitors | 9 (0.5%) | <5 | <5 | 5 (2.0%) |
| Angiotensin receptor blockers | 40 (2.3%) | 22 (10.7%) † | 5 (8.6%) | 25 (9.8%) |
| Beta-blockers | 25 (1.4%) | 20 (9.7%) † | <5 | 22 (8.6%) |
| Calcium channel blockers | 60 (3.4%) | 34 (16.5%) † | 6 (10.3%) | 39 (15.3%) |
| Romosozumab | Romosozumab | All other Drugs | All other Drugs | ||||
|---|---|---|---|---|---|---|---|
| Event | No Event | Event | No Event | ROR (95% CI) | IC | IC025 | |
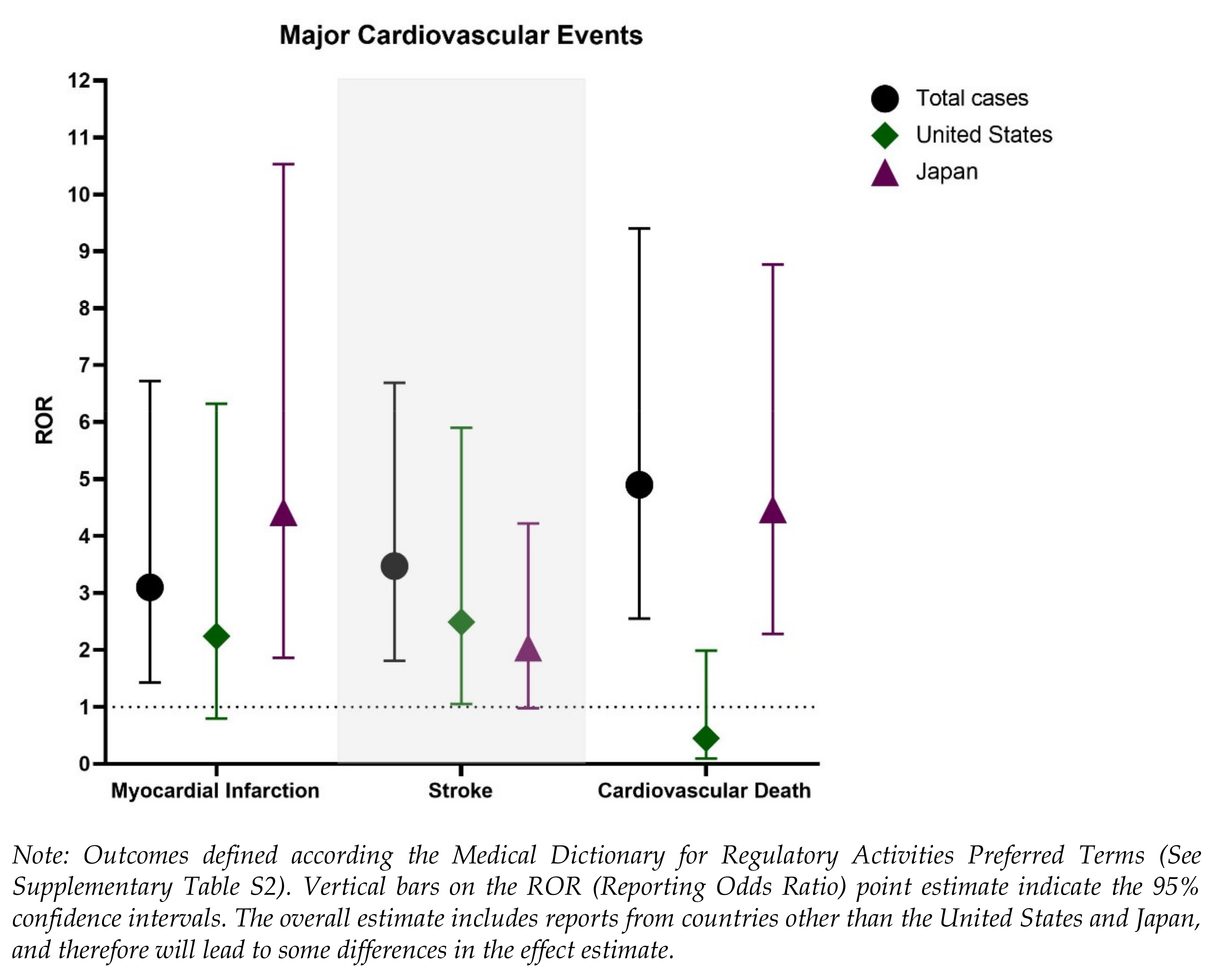
| MACE | 206 | 1789 | 84,723 | 2,996,511 | 4.07 (2.39–6.93) | 1.90 | 1.67 |
| Myocardial infarction | 42 | 1953 | 21,253 | 3,059,981 | 3.10 (1.43–6.72) | 1.57 | 1.06 |
| Stroke | 84 | 1911 | 38,489 | 3,042,745 | 3.47 (1.81–6.69) | 1.73 | 1.37 |
| Cardiovascular death | 86 | 1909 | 28,070 | 3,053,164 | 4.90 (2.55–9.40) | 2.21 | 1.85 |
| Other cardiovascular event | 58 | 1937 | 56,239 | 3,024,995 | 1.61 (0.79–3.29) | 0.66 | 0.23 |
| General cardiac events | 16 | 1979 | 16,880 | 3,064,354 | 1.47 (0.55–3.92) | 0.53 | −0.31 |
| Bleeding | 19 | 1976 | 20,699 | 3,060,535 | 1.42 (0.55–3.64) | 0.49 | −0.28 |
| Thrombosis | 23 | 1972 | 19,753 | 3,061,481 | 1.81 (0.74–4.44) | 0.82 | 0.12 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vestergaard Kvist, A.; Faruque, J.; Vallejo-Yagüe, E.; Weiler, S.; Winter, E.M.; Burden, A.M. Cardiovascular Safety Profile of Romosozumab: A Pharmacovigilance Analysis of the US Food and Drug Administration Adverse Event Reporting System (FAERS). J. Clin. Med. 2021, 10, 1660. https://doi.org/10.3390/jcm10081660
Vestergaard Kvist A, Faruque J, Vallejo-Yagüe E, Weiler S, Winter EM, Burden AM. Cardiovascular Safety Profile of Romosozumab: A Pharmacovigilance Analysis of the US Food and Drug Administration Adverse Event Reporting System (FAERS). Journal of Clinical Medicine. 2021; 10(8):1660. https://doi.org/10.3390/jcm10081660
Chicago/Turabian StyleVestergaard Kvist, Annika, Junaid Faruque, Enriqueta Vallejo-Yagüe, Stefan Weiler, Elizabeth M. Winter, and Andrea M. Burden. 2021. "Cardiovascular Safety Profile of Romosozumab: A Pharmacovigilance Analysis of the US Food and Drug Administration Adverse Event Reporting System (FAERS)" Journal of Clinical Medicine 10, no. 8: 1660. https://doi.org/10.3390/jcm10081660