2.1. Participants and Procedures
All patients were referred for PR to the Zurich RehaCenter Klinik Wald, Switzerland after hospitalization between March and December 2020 following acute care phase of a COVID-19 infection. The data of these patients were prospectively analyzed according to performance and outcome during rehabilitation and were compared to the cohort of rehabilitation participants with different pulmonary diseases of the year 2019. Data of this patient group (lung diseases (LG)) were retrospectively analyzed to describe potential differences, performance, and outcome during PR of patients after severe COVID-19. In total, 92% of the patients of the control group participated in the PR program following severe exacerbation of their pulmonary disease requiring hospitalization. We used the German version of the program RehaTISTM by Softsolution, International AG, 15830 Lahti, Finland to record and control the individual rehabilitation process of each participant, including all therapies and procedures. The patient data and results of the assessments were stored and taken for evaluation out of the clinic information system PhoenixTM, CompuGroup Medical AG, 3007 Bern, Switzerland.
Post-COVID-19 patients were eligible for PR as soon as they were hemodynamically stable without the need of catecholamine or invasive ventilation and continuous monitoring. In the initial phase of the corona crisis in Switzerland, patients were admitted after being asymptomatic for 2 days and 10 days after onset of infection. Later on, patients were additionally required to have at least one negative swab before transfer, while between June and December, the swab strategy was dropped again, and the initial regulations were valid again. All patients gave written informed consent, and the local ethics committee approved the study protocol (BASEC-No 2020-01061). This study is registered at the German Clinical Trials Register (DRKS00024613).
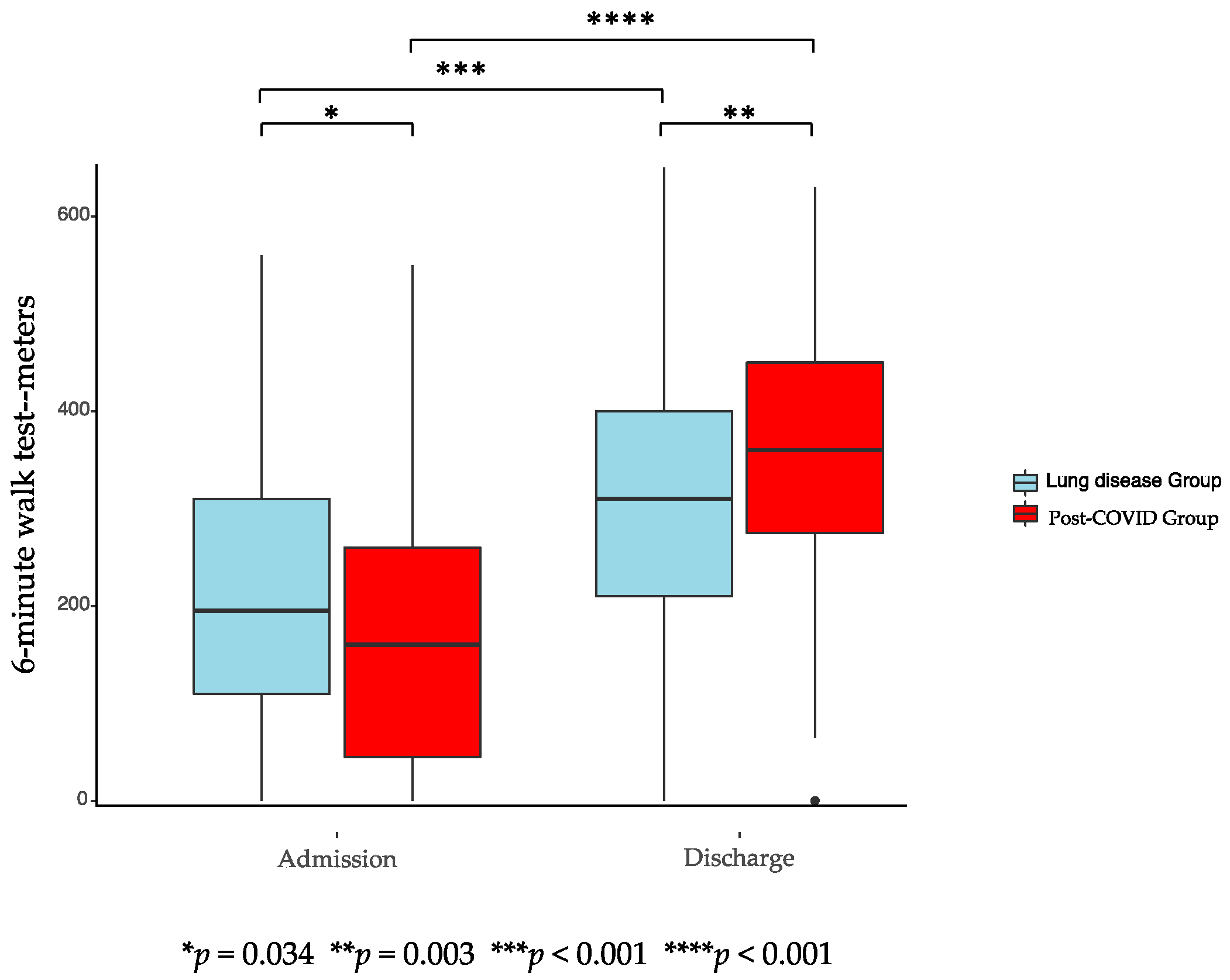
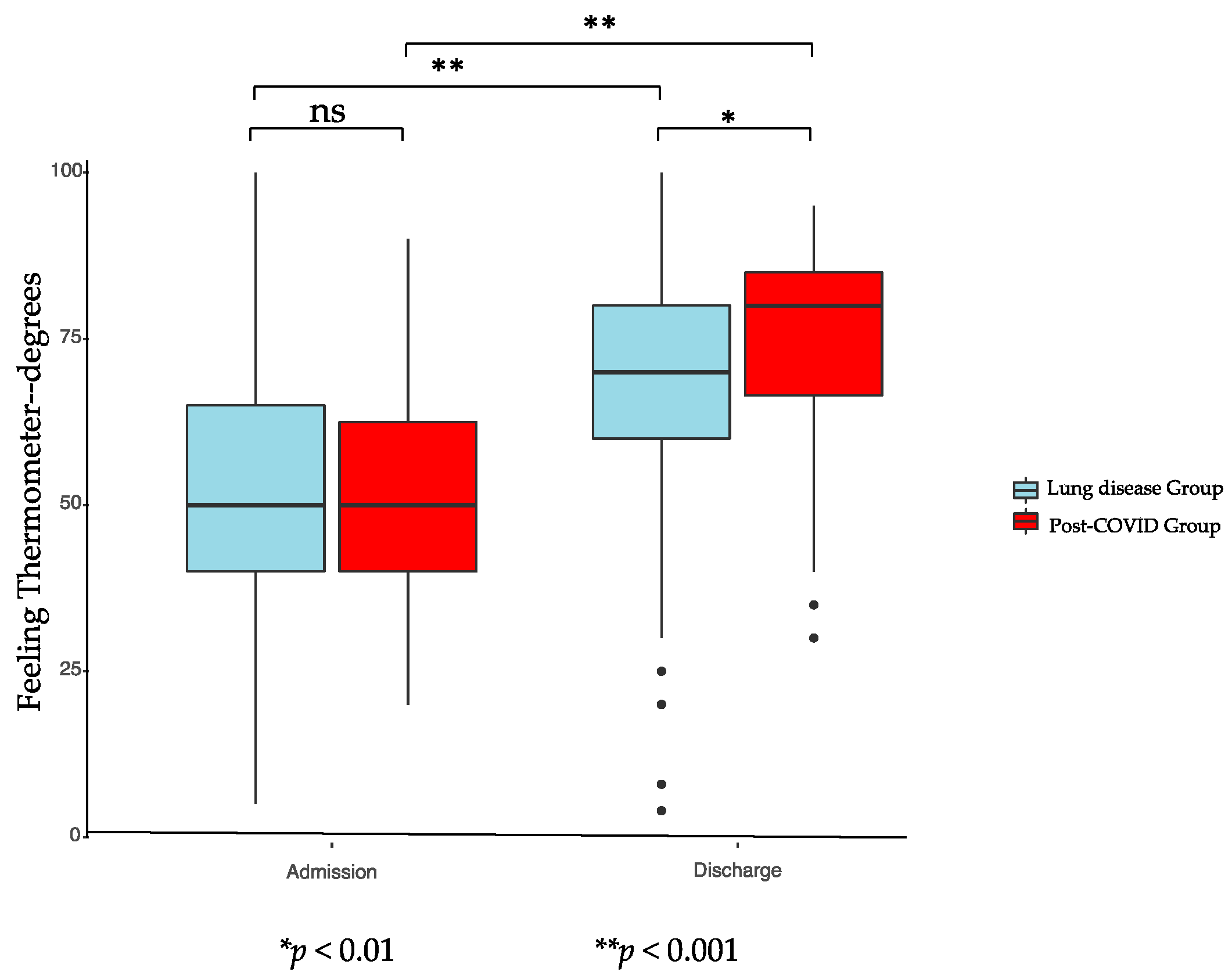
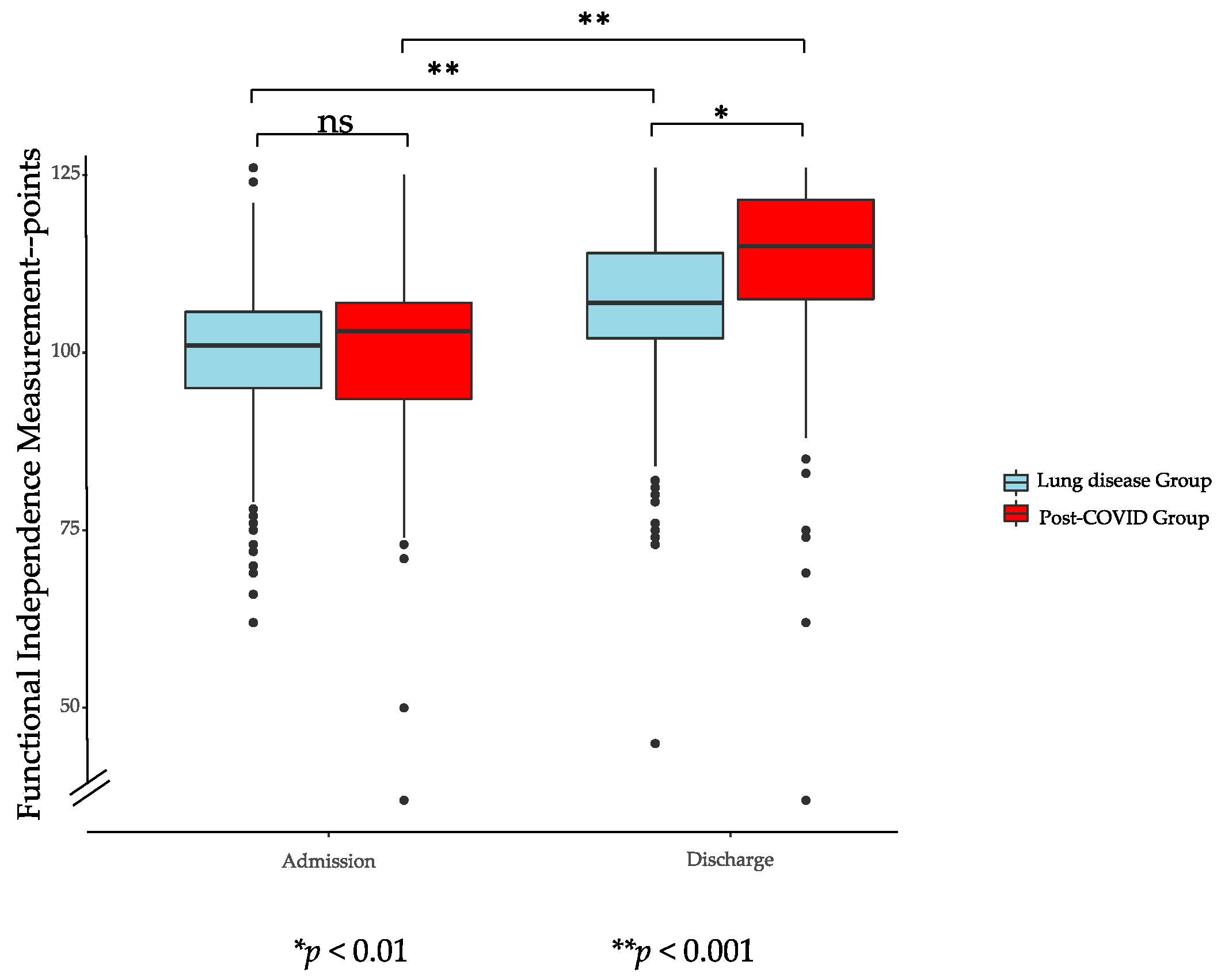
Within two days after admission for rehabilitation, all patients from the COVID-19 cohort and PR cohort of 2019 were assessed with questionnaires, such as Chronic Respiratory Disease Questionnaire (CRQ), Hospital Anxiety and Depression Scale (HADS), and Cumulative Illness Rating scale (CIRS) and Functional Independence Measure (FIM). To measure changes during rehabilitation, 6-min walk test (6-MWT) and Feeling Thermometer (FT) were performed on admission and before discharge. All patients were deemed cognitively able to provide valid responses to the questionnaires by treating physicians. Comorbidities, pulmonary function testing (PFT), and laboratory values including blood gas analysis were assessed.
2.2. Pulmonary Rehabilitation
The standardized inpatient PR program had a duration of 3 weeks, including a total of 25–30 therapy sessions on 5–6 weekdays. The multimodal program mainly consisted of an individualized endurance exercise and strength training and was carried out according to a protocol adapted to the severity of the disease and functional physical limitations. Monday to Friday, patients participated in a maximum of 4 exercise sessions per day. On Saturday, one exercise session was offered, and Sunday was exercise-free. Exercise therapy consisted of endurance training (cycling and treadmill), gymnastics (3 levels), in- and outdoor walking (3 levels), and strength training.
For cycling exercise, a low-intensity interval program was chosen if the initial 6-MWT distance was <200 m. In this cohort, a walking distance of <200 m according to the initial 6-MWT was found in 58 patients. The duration of the higher and lower intensity intervals was set to 30–60 (55–70% of maximum heart rate) and 60 s, respectively. The rate of perceived exertion (RPE) measured by the adapted Borg Scale (1–10) was used to define and adapt exercise intensity with a goal of Borg 4–6 (dyspnea) during exercise [
16,
17,
18]. Since most patients were very weak on PR admission, exercise started at very low intensity and increased continuously according to the patients’ tolerance. RPE was assessed after each exercise session. Duration of cycling was titrated individually starting at 5–10 min at entry and increasing over time up to 30–35 min at discharge. Exercise duration was usually increased first, with the goal to reach 20 min. After that, intensity was increased as well. All patients were monitored using pulse oximetry during their exercise. Criteria for stopping or reducing exercise intensity were an oxygen saturation (SpO
2) < 88% and dyspnea symptoms (Borg ≥ 6). When a drop in SpO
2 was observed, oxygen was added with a maximum of 6–8 L per minute via nasal cannula to keep the SpO
2 > 90%. More than half of PG patients (
n = 58) had an initial 6-MWT distance < 200 m, which required an individual adaptation of training. Partially bedridden patients started with in-bed cycling and MOTO-Med
® (RECK-Technik GmbH & Co. KG Medizintechnik, Reckstraße 1–5, D-88422 Betzenweiler, Germany). This was followed by first walking attempts with walking aids until first cycling interval training was possible. For fitter patients (6-MWT distance > 200 m), endurance training was carried out either on the treadmill or cycle ergometer. The speed of treadmill training was calculated based on the result of the 6-MWT (80% of 6-MWT pace; 6-MWT distance × 0.008 = exercise speed in km/h) but was also symptom-limited (Borg ≥ 6).
Outdoor walking was offered at different levels, with level 1 at a slow pace with little incline of the terrain and level 3 at a faster pace with frequent inclines. To decide which level of gymnastics or outdoor walking suited a patient, the result of the 6MWD was used (gymnastics: 6-MWT < 200 m = level 1, >400 = level 3) or an individual outdoor test walk was performed.
Gymnastics was offered in three levels of intensity. Whereas exercises in gymnastics level 1 took place mostly in a sitting position with several breaks between exercises, level 3 consisted of exercise in a standing position or walking with only very few or no breaks at all between exercises. Gymnastics consisted of a mixture of exercises to improve endurance, strength, coordination, range of motion, and balance.
A physio- or sports therapist instructed strength exercise 3–4 times per week individually according to recent American Thoracic Society/European Respiratory Society recommendations [
17]. The modified Borg Scale was used to define exercise intensity with the goal of Borg 4–5. Usually, 3 series of 8–12 repetitions per exercise and 3–5 exercises for large muscle groups were chosen. In addition, patients received inspiratory muscle training and relaxation (progressive muscle relaxation).
Respiratory physiotherapy consisted of teaching breath control (pursed lip breathing, secretion mobilization, and diaphragmatic breathing), energy saving techniques, and controlled coughing exercises.
Twice a week (1 h each), all patients participated in educational sessions, including self-management, coping skills, self-medication, management of infections and exacerbations, dyspnea, use of oxygen, and nutrition interventions. If needed, patients took part in a structured smoking cessation program, received psychosocial support or diabetes advice.
Table 1 provides an overview of the different therapies and their respective durations.


 ,
, 



{kind=link}
{kind=link}
{kind=link}