Feasibility of a Culturally Adapted Dietary Weight-Loss Intervention among Ghanaian Migrants in Berlin, Germany: The ADAPT Study

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
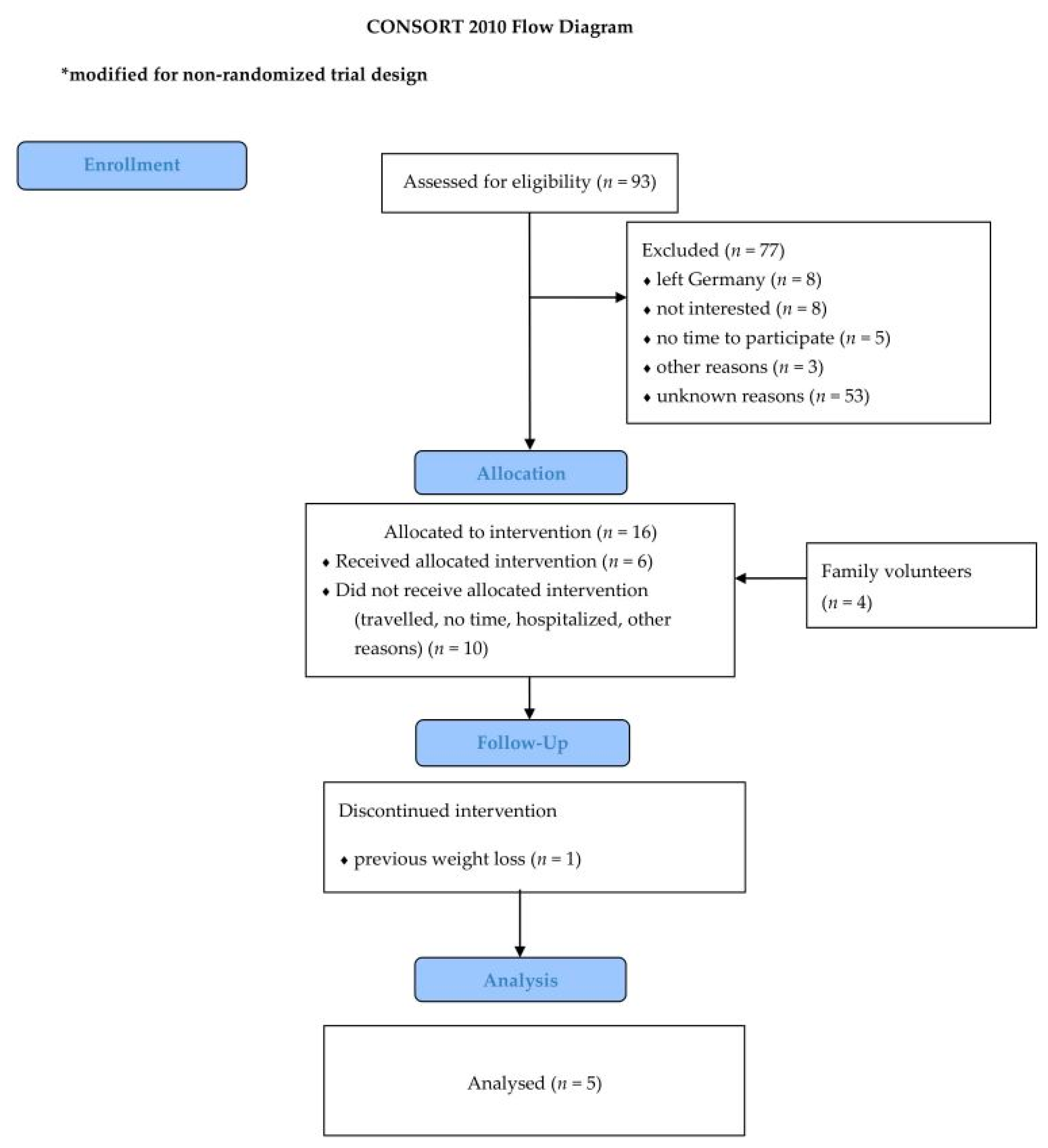
2.1. Study Population and Design
2.2. Ethics Statement
2.3. Intervention Program
2.4. Recruitment
2.5. Assessments of Demographics, Acceptability, and Lifestyle
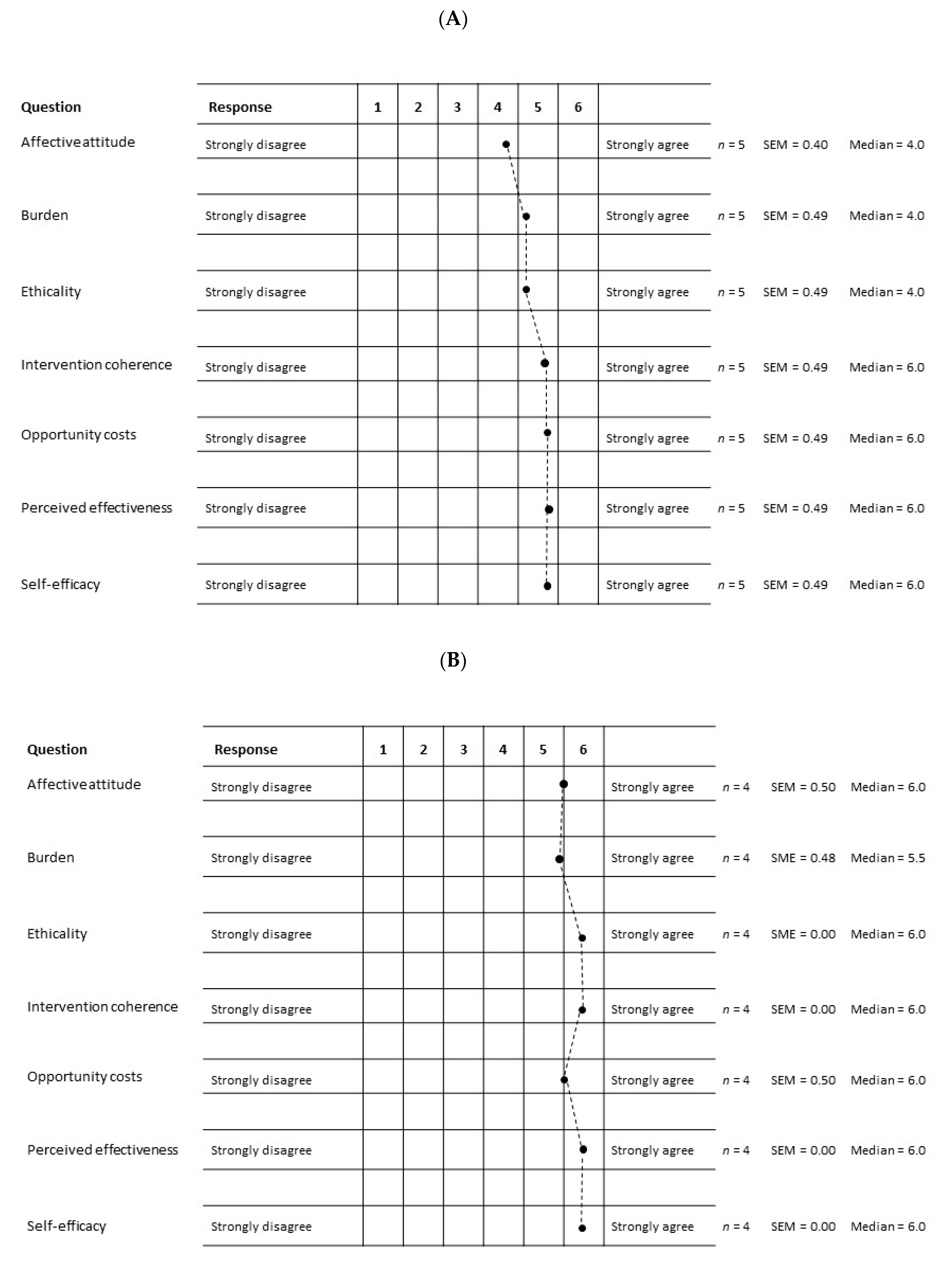
2.5.1. Acceptability
- Affective attitude: I enjoyed the diet and sports program;
- Burden: I easily integrated the diet and sports program in my daily life;
- Ethicality: The diet and sports program was important for me;
- Intervention coherence: I easily understood the diet and sports program;
- Opportunity costs: I am convinced by the diet and sports program;
- Perceived effectiveness: The diet and sports program will improve my health;
- Self-efficacy: The diet and sports program will help me to change my lifestyle.
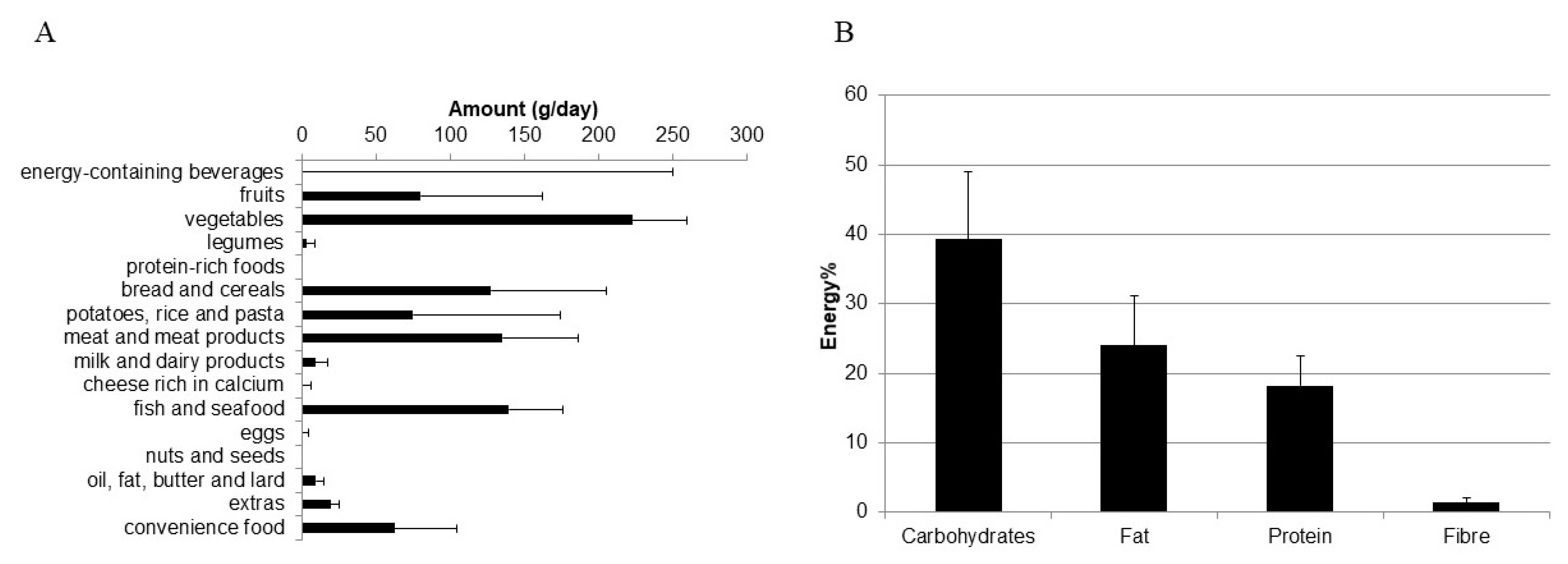
2.5.2. Dietary Behavior
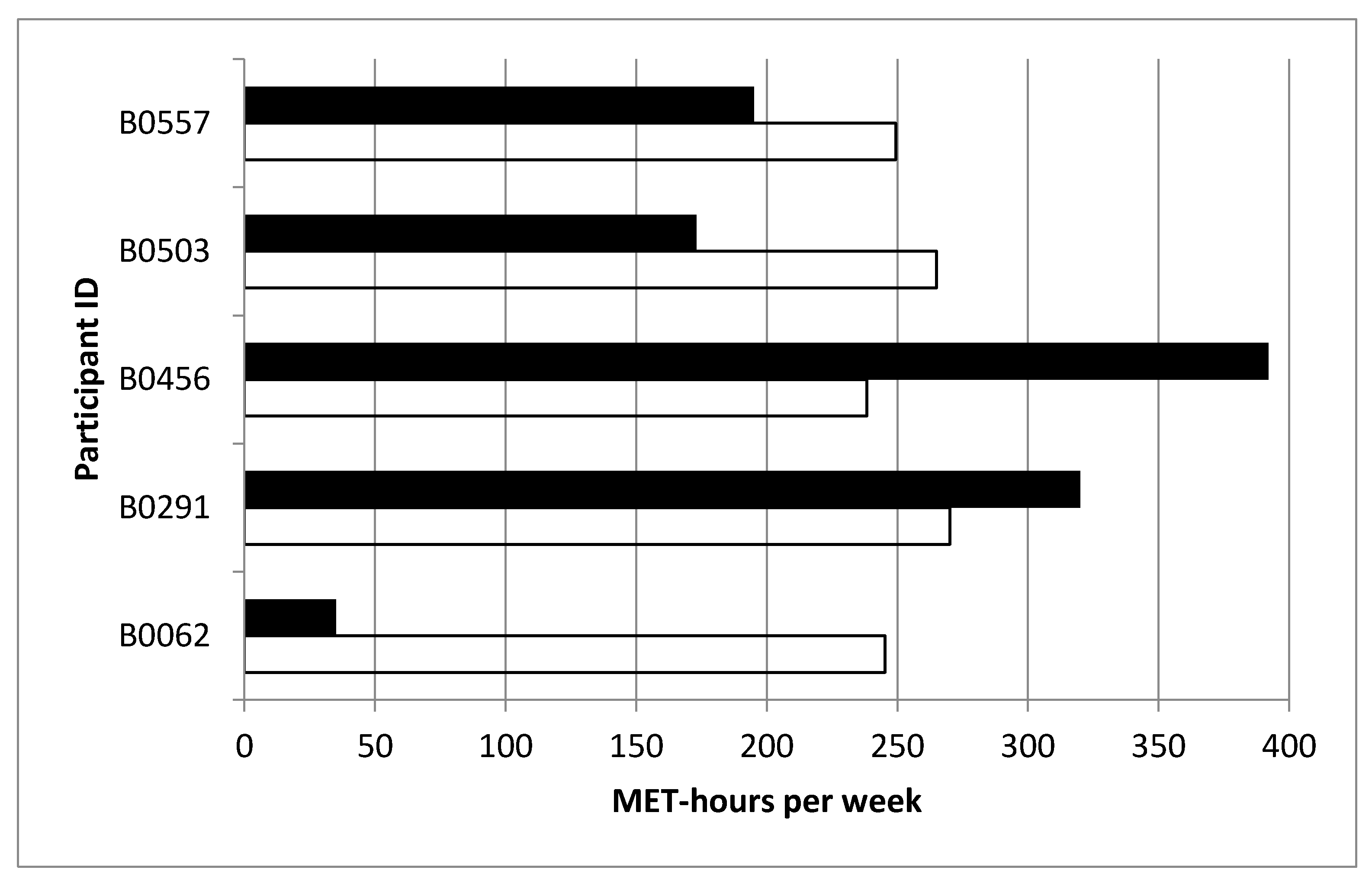
2.5.3. Physical Activity
2.6. Physical Examinations
2.7. Statistical Analysis
3. Results
3.1. Study Population
3.2. Practicability and Acceptability
3.3. Weight-Loss and Lifestyle Characteristics
4. Discussion
4.1. Practicability and Acceptability
4.2. Weight-Loss and Lifestyle
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef] [Green Version]
- Kelly, T.; Yang, W.; Chen, C.S.; Reynolds, K.; He, J. Global burden of obesity in 2005 and projections to 2030. Int. J. Obes. 2008, 32, 1431–1437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guh, D.P.; Zhang, W.; Bansback, N.; Amarsi, Z.; Birmingham, C.L.; Anis, A.H. The incidence of co-morbidities related to obesity and overweight: A systematic review and meta-analysis. BMC Public Health 2009, 9, 88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Must, A.; Spadano, J.; Coakley, E.H.; Field, A.E.; Colditz, G.; Dietz, W.H. The disease burden associated with overweight and obesity. JAMA 1999, 282, 1523–1529. [Google Scholar] [CrossRef]
- Misra, A.; Ganda, O.P. Migration and its impact on adiposity and type 2 diabetes. Nutrition 2007, 23, 696–708. [Google Scholar] [CrossRef]
- Agyemang, C.; Owusu-Dabo, E.; De Jonge, A.; Martins, D.; Ogedegbe, G.; Stronks, K. Overweight and obesity among Ghanaian residents in The Netherlands: How do they weigh against their urban and rural counterparts in Ghana? Public Health Nutr. 2009, 12, 909–916. [Google Scholar] [CrossRef] [Green Version]
- Organization for Economic Cooperation and Development (OECD). Key Indicators on International Migration. 2014. Available online: http://www.oecd.org/els/mig/keyindicatorsoninternationalmigration.htm (accessed on 24 October 2017).
- Federal Office for Migration and Refugees (BAMF). Migration Report Germany 2013. 2014. Available online: https://www.bamf.de/SharedDocs/Anlagen/DE/Publikationen/Migrationsberichte/migrationsbericht-2013.html (accessed on 24 October 2017).
- Kohnert, D. African Migration to Europe: Obscured Responsibilities and Common Misconceptions; 2007; Available online: https://doi.org/10.2139/ssrn.989960 (accessed on 24 October 2017).
- German Technical Cooperation (GIZ). Die ghanaische Diaspora in Deutschland—Ihr Beitrag zur Entwicklung; GTZ: Eschborn, Germany, 2009. [Google Scholar]
- Tonah, S. Ghanaians Abroad and Their Ties Home. Cultural and Religious Dimensions of Transnational Migration. In Proceedings of the Transnationalisation and Development(s): Towards a North-South Perspective, Bielefeld, Germany, 31 May–1 June 2007. [Google Scholar]
- Agyemang, C.; Meeks, K.; Beune, E.; Owusu-Dabo, E.; Mockenhaupt, F.P.; Addo, J.; de Graft Aikins, A.; Bahendeka, S.; Danquah, I.; Schulze, M.B.; et al. Obesity and type 2 diabetes in sub-Saharan Africans—Is the burden in today’s Africa similar to African migrants in Europe? The RODAM study. BMC Med. 2016, 14, 166. [Google Scholar] [CrossRef] [Green Version]
- Jensen, M.D.; Ryan, D.H.; Apovian, C.M.; Ard, J.D.; Comuzzie, A.G.; Donato, K.A.; Hu, F.B.; Hubbard, V.S.; Jakicic, J.M.; Kushner, R.F.; et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. J. Am. Coll. Cardiol. 2014, 63 Pt B, 2985–3023. [Google Scholar] [CrossRef] [Green Version]
- Scott, P.; Rajan, L. Eating habits and reactions to dietary advice among two generations of Caribbean people: A South London study, part 1. Pract. Diabetes 2000, 17, 183–186. [Google Scholar] [CrossRef]
- Kong, A.; Tussing-Humphreys, L.M.; Odoms-Young, A.M.; Stolley, M.R.; Fitzgibbon, M.L. Systematic review of behavioural interventions with culturally adapted strategies to improve diet and weight outcomes in African American women. Obes. Rev. 2014, 15 (Suppl. 4), 62–92. [Google Scholar] [CrossRef] [Green Version]
- Nierkens, V.; Hartman, M.A.; Nicolaou, M.; Vissenberg, C.; Beune, E.J.; Hosper, K.; van Valkengoed, I.G.; Stronks, K. Effectiveness of cultural adaptations of interventions aimed at smoking cessation, diet, and/or physical activity in ethnic minorities. A systematic review. PLoS ONE 2013, 8, e73373. [Google Scholar]
- Tovar, A.; Renzaho, A.M.; Guerrero, A.D.; Mena, N.; Ayala, G.X. A Systematic Review of Obesity Prevention Intervention Studies among Immigrant Populations in the US. Curr. Obes. Rep. 2014, 3, 206–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agyemang, C.; Beune, E.; Meeks, K.; Owusu-Dabo, E.; Agyei-Baffour, P.; Aikins, A.D.G.; Dodoo, F.; Smeeth, L.; Addo, J.; Mockenhaupt, F.P.; et al. Rationale and cross-sectional study design of the Research on Obesity and type 2 Diabetes among African Migrants: The RODAM study. BMJ Open 2015, 4, e004877. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hauner, H.; Moss, A.; Berg, A.; Bischoff, S.C.; Colombo-Benkmann, M.; Ellrott, T.; Heintze, C.; Kanthak, U.; Kunze, D.; Stefan, N.; et al. Interdisziplinäre Leitlinie der Qualität S3 zur “Prävention und Therapie der Adipositas”. Adipositas-Ursachen Folgeerkrankungen Ther. 2014, 8, 179–221. [Google Scholar] [CrossRef] [Green Version]
- Bandura, A. Social Foundations of thought and Action: A Social Cognitive Theory; Prentice-Hall, Inc.: Englewood Cliffs, NJ, USA, 1986. [Google Scholar]
- Prochaska, J.O.; DiClemente, C.C. Transtheoretical therapy: Toward a more integrative model of change. Psychother. Theory Res. Pract. 1982, 19, 276. [Google Scholar] [CrossRef]
- Ahluwalia, J.; Baranowski, T.; Braithwaite, R.; Resnicow, K. Cultural sensitivity in public health: Defined and demystified. Ethn. Dis. 1999, 9, 10–21. [Google Scholar]
- Renzaho, A.M.; Mellor, D.; Boulton, K.; Swinburn, B. Effectiveness of prevention programmes for obesity and chronic diseases among immigrants to developed countries—A systematic review. Public Health Nutr. 2010, 13, 438–450. [Google Scholar] [CrossRef] [Green Version]
- Bhopal, R.S.; Douglas, A.; Wallia, S.; Forbes, J.F.; Lean, M.E.; Gill, J.M.; McKnight, J.A.; Sattar, N.; Sheikh, A.; Wild, S.H.; et al. Effect of a lifestyle intervention on weight change in south Asian individuals in the UK at high risk of type 2 diabetes: A family-cluster randomised controlled trial. Lancet Diabetes Endocrinol. 2014, 2, 218–227. [Google Scholar] [CrossRef]
- Sekhon, M.; Cartwright, M.; Francis, J.J. Acceptability of healthcare interventions: An overview of reviews and development of a theoretical framework. BMC Health Serv. Res. 2017, 17, 88. [Google Scholar] [CrossRef] [Green Version]
- Galbete, C.; Nicolaou, M.; Meeks, K.A.; Aikins, A.D.-G.; Addo, J.; Amoah, S.K.; Smeeth, L.; Owusu-Dabo, E.; Klipstein-Grobusch, K.; Bahendeka, S.K.; et al. Food consumption, nutrient intake, and dietary patterns in Ghanaian migrants in Europe and their compatriots in Ghana. Food Nutr. Res. 2017, 61, 1341809. [Google Scholar] [CrossRef] [Green Version]
- Conway, J.M.; Ingwersen, L.A.; Vinyard, B.T.; Moshfegh, A.J. Effectiveness of the US Department of Agriculture 5-step multiple-pass method in assessing food intake in obese and nonobese women. Am. J. Clin. Nutr. 2003, 77, 1171–1178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. The WHO STEPwise Approach to Noncommunicable Disease Risk Factor Surveillance (STEPS); World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- George, S.; Duran, N.; Norris, K. A systematic review of barriers and facilitators to minority research participation among African Americans, Latinos, Asian Americans, and Pacific Islanders. Am. J. Public Health 2014, 104, e16–e31. [Google Scholar] [CrossRef] [PubMed]
- Wallia, S.; Bhopal, R.S.; Douglas, A.; Sharma, A.; Hutchison, A.; Murray, G.; Gill, J.; Sattar, N.; Lawton, J.; Tuomilehto, J.; et al. Culturally adapting the prevention of diabetes and obesity in South Asians (PODOSA) trial. Health Promot. Int. 2013, 29, 768–779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agyemang, C.; Nicolaou, M.; Boateng, L.; Dijkshoorn, H.; Van De Born, B.-J.; Stronks, K. Prevalence, awareness, treatment, and control of hypertension among Ghanaian population in Amsterdam, the Netherlands: The GHAIA study. Eur. J. Prev. Cardiol. 2013, 20, 938–946. [Google Scholar] [CrossRef] [PubMed]
- Elam, G.; McMunn, A.; Nazroo, J. Feasibility Study for Health Surveys among Black African People Living in England: Final Report—Implications for the Health Surveys for England; Department of Health: London, UK, 2001. [Google Scholar]
- Beune, E.J.A.J.; Haafkens, J.A.; Schuster, J.S.; Bindels, P.J.E. ‘Under pressure’: How Ghanaian, African-Surinamese and Dutch patients explain hypertension. J. Hum. Hypertens. 2006, 20, 946–955. [Google Scholar] [CrossRef] [PubMed]
- Tuoyire, D.A.; Kumi-Kyereme, A.; Doku, D.T.; Amo-Adjei, J. Perceived ideal body size of Ghanaian women: “Not too skinny, but not too fat”. Women Health 2018, 58, 583–597. [Google Scholar]
- Symmank, C.; Mai, R.; Hoffmann, S.; Stok, F.M.; Renner, B.; Lien, N.; Rohm, H. Predictors of food decision making: A systematic interdisciplinary mapping (SIM) review. Appetite 2017, 110, 25–35. [Google Scholar] [CrossRef]
- Walker, R.J.; Smalls, B.L.; Bonilha, H.S.; Campbell, J.A.; Egede, L.E. Behavioral interventions to improve glycemic control in African Americans with type 2 diabetes: A systematic review. Ethn. Dis. 2013, 23, 401–408. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | German Society of Adiposity (DAG) Guidelines | ADAPT Intervention | Reasons for Adaptation |
|---|---|---|---|
| Participants | Individuals with adiposity | Ghanaian adult migrants (defined as born in Ghana or both parents born in Ghana) with either general overweight/obesity or abdominal overweight/obesity and one adult family volunteer. Main cook agrees to co-operate. | Recruit Ghanaian migrants with high prevalence rates of adiposity; encourage support from family members, particularly from those who are responsible for the family meals; encourage healthier lifestyle in the entire family |
| Inclusion criteria | Body mass index (BMI) ≥ 30.0 kg/m2 or waist circumference ≥ 88 cm for women and ≥102 cm for men, if BMI 25.0 < 30.0 kg/m2 | Body mass index (BMI) ≥ 30.0 kg/m2 or waist circumference ≥ 88 cm for women and ≥102 cm for men, if BMI 25.0 < 30.0 kg/m2 | Potential recruits may have central obesity, but have a low BMI; acknowledge the important role of central body fat accumulation |
| Setting | General practitioner | Community for recruitment, ethnically matched practitioner for examination, home setting for intervention | Encourage community and family involvement; increase compliance; reduce attrition |
| Duration of the intervention | 3 months | 3 months intensive intervention period with 1 group contact, 3 family-based contacts and weekly mobile phone reminders | Facilitate motivation, compliance, self-efficacy, family involvement, and sustainability |
| Weight loss goal | ≥5% of initial body weight, if BMI 25.0 < 30.0 kg/m2; ≥10% of initial body weight, if BMI ≥ 30.0 kg/m2 | ≥2.5 kg in the intervention group | Realistic for Ghanaian migrants and still relevant to improve the cardio-metabolic profile |
| Physical activity (PA) | >30 min/day (≈ 1200–1800 kcal/week); mainly endurance sports; for individuals with BMI ≥ 30.0 kg/m2, increase PA in daily routine (e.g., walking, taking stairs); PA counselling: health-beneficial effects of physical activity beyond weight loss and PA goal setting | >30 min/day (≈ 1200–1800 kcal/week); increase PA in daily routine (e.g., brisk walking, taking stairs); Group counselling and lifestyle poster: health-beneficial effects of physical activity beyond weight loss; PA goal setting: pedometer; PA self-contracting: weekly mobile phone text messages | Most relevant; achievable recommendations, accounting for work load and family time; encouragement of self-chosen outdoor or gym activity in a group or alone; incorporates goal setting, behavioral contracting, and tailored health communication |
| Dietary intervention and targets | Dietary advice by general practitioner: daily energy deficit of 500 kcal; reduction of total fat and/or reduction of carbohydrates | Group counselling, lifestyle poster: reduced energy intake, not specific in nutrients; consultation with a dietician in the language of choice (German, English, local Ghanaian); reducing the intakes of frequently consumed foods that are rich in fats and carbohydrates; 3 home-based cooking sessions focusing on cooking methods, portion sizes, food choices, and fat amount for cooking; diet goal setting: 24-h dietary recall protocols; diet self-contracting: weekly mobile phone text messages | Bilingual dietary counselling available; Achievable and comprehensible approach, given the low level of formal education and health literacy in the study population; Engage the available family in a domestic setting especially those who prepare the family meals; Incorporates goal setting, behavioral contracting, and tailored health communication |
| Week | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Examinations | ||||||||||||
| Anthropometry | X | X | ||||||||||
| Oral glucose tolerance test | X | X | ||||||||||
| Blood pressure | X | X | ||||||||||
| Laboratory analyses | ||||||||||||
| Blood glucose (0, 30, 120 min) | X | X | ||||||||||
| C-Peptide, Insulin (0, 30, 120 min) | X | X | ||||||||||
| HbA1c | X | X | ||||||||||
| Fasting blood lipids | X | X | ||||||||||
| Intervention | ||||||||||||
| Group counselling | X | |||||||||||
| Info poster | X | |||||||||||
| Cooking session | X | X | X | |||||||||
| Smartphone reminder | X | X | X | X | X | X | X | X | X | X | ||
| ActivPAL set | X | X | X | |||||||||
| ActivPAL collect | X | X | X | |||||||||
| 24 h dietary recall | X | X | ||||||||||
| WHO STEPS activity questionnaire | X | X | ||||||||||
| Acceptability questionnaire | X | X |
| Characteristics | 2014 | 2017 | ||
|---|---|---|---|---|
| Median/Percentage | Range/Number | Median/Percentage | Range/Number | |
| n | 100% | 6 | 100% | 6 |
| Age (years) | 47.5 | 22.0–58.0 | 50.6 | 25.0–61.5 |
| Sex (male) | 33.3% | 2 | 33.3% | 2 |
| Weight (kg) | 75.5 | 64.0–83.9 | 77.4 | 62.8–87.6 |
| Body mass index (kg/m2) | 29.7 | 25.7–31.3 | 29.9 | 23.3–35.1 |
| Waist circumference (cm) | 92.2 | 83.1–105.1 | 98.3 | 86.0–100.0 |
| Physical activity (MET-h/week) | 195 | 0.0–392 | ||
| Energy intake (kcal/d) * | 2384 | 922–3361 | ||
| Characteristics. | Median/Percentage | Range/Number |
|---|---|---|
| Anthropometry | ||
| ∆ weight (kg) | −0.6 | 0.5, −3.6 |
| ∆ body mass index (kg/m2) | −0.3 | 0.2, −1.2 |
| ∆ waist circumference (cm) | −1.3 | 4.1, −4.5 |
| Lifestyle characteristics | ||
| ∆ physical activity (MET-h/week) | 65 | −24, 249 |
| ∆ energy intake (kcal/d) * | −1480 | −3300, −127 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amoah, S.; Ennin, R.; Sagoe, K.; Steinbrecher, A.; Pischon, T.; Mockenhaupt, F.P.; Danquah, I. Feasibility of a Culturally Adapted Dietary Weight-Loss Intervention among Ghanaian Migrants in Berlin, Germany: The ADAPT Study. Int. J. Environ. Res. Public Health 2021, 18, 510. https://doi.org/10.3390/ijerph18020510
Amoah S, Ennin R, Sagoe K, Steinbrecher A, Pischon T, Mockenhaupt FP, Danquah I. Feasibility of a Culturally Adapted Dietary Weight-Loss Intervention among Ghanaian Migrants in Berlin, Germany: The ADAPT Study. International Journal of Environmental Research and Public Health. 2021; 18(2):510. https://doi.org/10.3390/ijerph18020510
Chicago/Turabian StyleAmoah, Stephen, Ruth Ennin, Karen Sagoe, Astrid Steinbrecher, Tobias Pischon, Frank P. Mockenhaupt, and Ina Danquah. 2021. "Feasibility of a Culturally Adapted Dietary Weight-Loss Intervention among Ghanaian Migrants in Berlin, Germany: The ADAPT Study" International Journal of Environmental Research and Public Health 18, no. 2: 510. https://doi.org/10.3390/ijerph18020510