
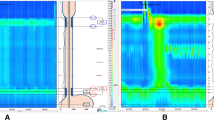
Background: The simultaneous occurrence of achalasia and morbid obesity is rare. Nevertheless, the surgical therapy of morbid obesity may be harmful, if undiagnosed achalasia were left untreated. We report the clinical presentation and response to treatment of achalasia in the context of morbid obesity. Methods: From 1998 to 2002, 638 patients underwent surgery for morbid obesity. Preoperative upper gastrointestinal radiography was performed in all patients. Three patients had manometric confirmation of achalasia. The characteristic symptoms were recurrent episodes of regurgitation, chronic cough and aspiration. No patient reported dysphagia or recent weight loss. Results: All patients had a duodenal switch procedure and in two a concurrent Heller myotomy was added. The other patient required a Heller myotomy after a duodenal switch had been performed, because the motility study was initially misinterpreted. All patients reported gradual resolution of presenting symptoms after myotomy. Conclusions: A careful symptomatic history focusing on aspiration, regurgitation and cough may identify the unusual combination of achalasia and morbid obesity. Treatment of morbid obesity alone may lead to progression of pulmonary symptoms.
Similar content being viewed by others

Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Almogy, G., Anthone, G.J. & Crookes, P.F. Achalasia in the Context of Morbid Obesity: a Rare but Important Association. OBES SURG 13, 896–900 (2003). https://doi.org/10.1381/096089203322618731
Published:
Issue Date:
DOI: https://doi.org/10.1381/096089203322618731