
Abstract
Background
Elderly women (≥ 70 years old) form a significant proportion of patients affected by breast cancer (BC); however, the treatment decisions for this patient population are complicated, owing to the presence of comorbidities, limited life expectancy, reduced tolerability of therapy, and limited enrollment in clinical trials. A growing body of evidence suggests equivalent outcomes in elderly patients with hormone receptor-positive early-stage breast cancer receiving primary endocrine therapy only or surgery with subsequent endocrine therapy. Whether these results are reproduced in the larger BC population outside of a clinical trial currently remains unclear.
Patients and Methods
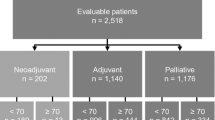
Women ≥ 70 years old diagnosed with early-stage invasive breast cancer between January 2008 and December 2013 with tumor size T1 or T2, minimal nodal involvement (N0 and N1), and estrogen and/or progesterone receptor positivity who started endocrine therapy within a year of diagnosis were identified using the Surveillance, Epidemiology, and End Results (SEER)–Medicare linked datasets. Endocrine therapy was identified using outpatient prescription fills for anastrozole, exemestane, fulvestrant, letrozole, raloxifene, tamoxifen, and toremifene; the first fill date was used as the treatment initiation date. Surgical intervention included either breast-conserving surgery or mastectomy. Women who received chemotherapy were excluded. Trends in the use of primary endocrine therapy only were assessed using Poisson regression. Multivariable Cox proportional hazard regression was used to estimate the association between undergoing surgery within a year of diagnosis and 5-year all-cause mortality, after adjusting for patient demographics, comorbidities, and clinical cancer characteristics. Similar methods were used to assess 5-year cancer-specific mortality, where noncancer mortality was treated as a competing risk.
Results
Overall, 8784 women were included in the analysis: 8006 (91%) received surgery with endocrine therapy and 778 (9%) received primary endocrine therapy alone. The proportion of women not receiving surgery remained consistent between 2008 and 2013 (p = 0.10). The 5-year mortality was 11% (n = 619), and 19% of all deaths were due to cancer causes (n = 117). After adjustment, 5-year mortality was lower among women undergoing surgery (HR 0.59, 95% CI 0.47–0.74, p < 0.0001). Similar results were found when looking at 5-year cancer-specific mortality (HR 0.52, 95% CI 0.30–0.90, p < 0.0001).
Conclusions
Elderly breast cancer patients with early-stage hormone-receptor-positive disease receiving primary surgical intervention plus endocrine therapy may have significantly improved survival than those receiving primary endocrine therapy alone. This study suggests the importance of surgical intervention for elderly breast cancer patients and warrants further investigation and comprehensive geriatric assessment to identify subsets of elderly breast cancer patients who may benefit significantly from surgical intervention.


Similar content being viewed by others


References
SEER Cancer Statistics Review, 1975-2015. https://seer.cancer.gov/csr/1975_2015/.
DeSantis C, Ma J, Bryan L, Jemal A. Breast cancer statistics, 2013. CA Cancer J Clin. 2014;64(1):52–62. https://doi.org/10.3322/caac.21203.
Jolly TA, Deal AM, Nyrop KA, et al. Geriatric assessment-identified deficits in older cancer patients with normal performance status. Oncologist. 2015;20(4):379–385.
Hurria A, Levit LA, Dale W, et al. Improving the evidence base for treating older adults with cancer: American Society of Clinical Oncology Statement. J Clin Oncol. 2015;33(32):3826–3833. https://doi.org/10.1200/jco.2015.63.0319.
Le Saux O, Falandry C, Gan HK, You B, Freyer G, Péron J. Inclusion of elderly patients in oncology clinical trials. Ann Oncol. 2016;27(9):1799–1804. https://doi.org/10.1093/annonc/mdw259.
Singh H, Kanapuru B, Smith C, et al. FDA analysis of enrollment of older adults in clinical trials for cancer drug registration: A 10-year experience by the U.S. Food and Drug Administration. J Clin Oncol. 2017;35(15_suppl):10009–10009. https://doi.org/10.1200/jco.2017.35.15_suppl.10009.
Syed BM, Green AR, Paish EC, et al. Biology of primary breast cancer in older women treated by surgery: with correlation with long-term clinical outcome and comparison with their younger counterparts. Br J Cancer. 2013;108(5):1042–1051.
Clark GM. The biology of breast cancer in older women. J Gerontol. 1992;47 Spec No:19–23.
Cummings FJ, Gray R, Tormey DC, et al. Adjuvant tamoxifen versus placebo in elderly women with node-positive breast cancer: long-term follow-up and causes of death. J Clin Oncol. 1993;11(1):29–35. https://doi.org/10.1200/jco.1993.11.1.29.
Mustacchi G, Scanni A, Capasso I, Farris A, Pluchinotta A, Isola G. Update of the Phase III trial “GRETA” of surgery and tamoxifen versus tamoxifen alone for early breast cancer in elderly women. Future Oncol. 2015;11(6):933–941. https://doi.org/10.2217/fon.14.266.
Willsher, P.C., Robertson JFR, Jackson L, Al-Hilaly M, Blarney RW. Investigation of primary tamoxifen therapy for elderly patients with operable breast cancer. Breast. 1997;6(3):150–154. https://doi.org/10.1016/s0960-9776(97)90557-9.
Chakrabarti J, Kenny FS, Syed BM, Robertson JFR, Blamey RW, Cheung KL. A randomised trial of mastectomy only versus tamoxifen for treating elderly patients with operable primary breast cancer—Final results at 20-year follow-up. Crit Rev Oncol Hematol. 2011;78(3):260–264.
Hind D, Wyld L, Beverley CB, Reed MW. Surgery versus primary endocrine therapy for operable primary breast cancer in elderly women (70 years plus). Cochrane Database Syst Rev. 2006;(1):CD004272. https://doi.org/10.1002/14651858.cd004272.pub2.
Pepping RMC, Portielje JEA, van de Water W, de Glas NA. Primary endocrine therapy in older women with breast cancer. Curr Geriatr Rep. 2017;6(4):239–246.
Healthcaredelivery.Cancer.Gov. https://healthcaredelivery.cancer.gov. Accessed February 10, 2019.
Warren JL, Brown ML, Fay MP, Schussler N, Potosky AL, Riley GF. Costs of treatment for elderly women with early-stage breast cancer in fee-for-service settings. J Clin Oncol. 2002;20(1):307–316. https://doi.org/10.1200/jco.2002.20.1.307.
Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol. 1992;45(6):613–619.
Simon R, Latreille J, Matte C, Desjardins P, Bergeron E. Adherence to adjuvant endocrine therapy in estrogen receptor-positive breast cancer patients with regular follow-up. Can J Surg. 2014;57(1):26-32.
Chlebowski RT, Kim J, Haque R. Adherence to endocrine therapy in breast cancer adjuvant and prevention settings. Cancer Prevention Research. 2014;7(4):378–387. https://doi.org/10.1158/1940-6207.capr-13-0389.
Muss HB, Tu D, Ingle JN, et al. Efficacy, toxicity, and quality of life in older women with early-stage breast cancer treated with letrozole or placebo after 5 years of tamoxifen: NCIC CTG intergroup trial MA.17. J Clin Oncol. 2008;26(12):1956–1964. https://doi.org/10.1200/jco.2007.12.6334.
Amir E, Seruga B, Niraula S, Carlsson L, Ocana A. Toxicity of adjuvant endocrine therapy in postmenopausal breast cancer patients: a systematic review and meta-analysis. J Natl Cancer Inst. 2011;103(17):1299–1309. https://doi.org/10.1093/jnci/djr242.
Kardas P, Lewek P, Matyjaszczyk M. Determinants of patient adherence: a review of systematic reviews. Front Pharmacol. 2013;4:91. https://doi.org/10.3389/fphar.2013.00091.
Lee S-Y, Seo JH. Current strategies of endocrine therapy in elderly patients with breast cancer. Biomed Res Int. 2018;2018:6074808–6074808.
Wanebo HJ, Cole B, Chung M, et al. Is surgical management compromised in elderly patients with breast cancer? Ann Surg. 1997;225(5):579–86–discussion586–9.
Malik MK, Tartter PI, Belfer R. Undertreated breast cancer in the elderly. J Cancer Epidemiol. 2013;2013:893104.
Bouchardy C, Rapiti E, Fioretta G, et al. Undertreatment strongly decreases prognosis of breast cancer in elderly women. J Clin Oncol. 2003;21(19):3580–3587.
Gazet JC, Sutcliffe R. A randomised trial comparing tamoxifen vs. surgery in patients over the age of 70 with operable breast cancer - Final results after 28 years of follow-up. Eur J Surg Oncol (EJSO). 2011;37(9):754–757. https://doi.org/10.1016/j.ejso.2011.06.011.
Mustacchi G, Ceccherini R, Milani S, et al. Tamoxifen alone versus adjuvant tamoxifen for operable breast cancer of the elderly: long-term results of the phase III randomized controlled multicenter GRETA trial. Ann Oncol. 2003;14(3):414–420.
Fennessy M, Bates T, MacRae K, Riley D, Houghton J, Baum M. Late follow-up of a randomized trial of surgery plus tamoxifen versus tamoxifen alone in women aged over 70 years with operable breast cancer. Br J Surg. 2004;91(6):699–704. https://doi.org/10.1002/bjs.4603.
Acknowledgements
The collection of cancer incidence data used in this study was supported by the California Department of Public Health as part of the statewide cancer reporting program mandated by California Health and Safety Code Section 103885; the National Cancer Institute’s Surveillance, Epidemiology and End Results. Program under contract HHSN261201000140C awarded to the Cancer Prevention Institute of California, contract HHSN261201000035C awarded to the University of Southern California, and contract HHSN261201000034C awarded to the Public Health Institute; and the Centers for Disease Control and Prevention’s National Program of Cancer Registries, under agreement # U58DP003862-01 awarded to the California Department of Public Health. The ideas and opinions expressed herein are those of the author(s), and endorsement by the State of California Department of Public Health, the National Cancer Institute, and the Centers for Disease Control and Prevention or their contractors and subcontractors is not intended nor should be inferred. The authors acknowledge the efforts of the National Cancer Institute; the Office of Research, Development and Information, CMS; Information Management Services (IMS), Inc.; and the Surveillance, Epidemiology, and End Results (SEER) Program tumor registries in the creation of the SEER-Medicare database. The database infrastructure used for this project was funded by the CER Strategic Initiative of UNC’s Clinical and Translational Science Award (UL1TR001111) and the UNC School of Medicine. Additional funding for the SEER-Medicare data was provided by the UNC Lineberger Comprehensive Cancer Center’s University Cancer Research Fund (UCRF) via the State of North Carolina.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosure
None of the authors have any disclosure relevant to the material in this paper. No outside funding was received for this study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Nayyar, A., Strassle, P.D., Iles, K. et al. Survival Outcomes of Early-Stage Hormone Receptor-Positive Breast Cancer in Elderly Women. Ann Surg Oncol 27, 4853–4860 (2020). https://doi.org/10.1245/s10434-020-08945-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-020-08945-1