
Abstract
Introduction
Historically, the treatment of anorectal melanoma has been abdominoperineal resection (APR), but more recently local resection alone. Although treatment at melanoma centers has become less aggressive, the adoption of this approach and related outcomes across the USA is unknown.
Methods
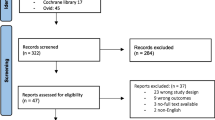
The Surveillance, Epidemiology, and End Results (SEER) database was queried to identify patients treated for anorectal melanoma (1973–2003). Treatment patterns and survival were studied. Frequency of treatment was compared using the chi-square test; survival was calculated using the Kaplan–Meier method.
Results
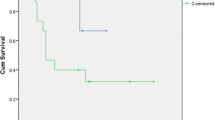
The 183 patients identified from the SEER database had a median age of 68 years. Of the 143 patients whose data were included, 51 underwent APR and 92 underwent transanal excision (TAE). Despite similar pathologic characteristics, median survival was similar in the two groups: 16 months for APR and 18 months for TAE (P = ns). Five-year survival also was similar in the two groups: 16.8% for APR and 19.3% for TAE (P = ns). The rate of APR was 27.0% between 1973 and 1996, as compared with 43.2% between 1997 and 2003 (P = ns).
Conclusion
This study, the largest series to analyze widespread practice patterns and outcomes for anorectal melanoma in the USA, did not reveal a survival difference comparing TAE with APR. Moreover, the study did not reveal a trend toward less aggressive surgical resection. Since the extent of surgical intervention did not correlate with survival or extent of primary tumor, APR should be reserved for selected patients in whom TAE is not technically feasible.

Similar content being viewed by others

References
Brady MS, Kavolius JP, Quan SH. Anorectal melanoma. A 64-year experience at Memorial Sloan-Kettering Cancer Center. Dis Colon Rectum. 1995;38:146–51.
Chang AE, Karnell LH, Menck HR. The National Cancer Data Base report on cutaneous and noncutaneous melanoma: a summary of 84,836 cases from the past decade. The American College of Surgeons Commission on Cancer and the American Cancer Society. Cancer. 1998;83:1664–78.
Wong JH, Cagle LA, Storm FK, Morton DL. Natural history of surgically treated mucosal melanoma. Am J Surg. 1987;154(1):54–7.
Quan SH, Deddish MR. Noncutaneous melanoma. Malignant melanoma of the anorectum. CA Cancer J Clin. 1966;16:111–4.
Pack GT, Oropeza R. A comparative study of melanoma and epidermoid carcinoma of the anal canal: A review of 20 melanomas and 29 epidermoid carcinomas (1930 to 1965). Dis Colon Rectum. 1967;10:161–76.
Cooper PH, Mills SE, Allen MS Jr. Malignant melanoma of the anus: report of 12 patients and analysis of 255 additional cases. Dis Colon Rectum. 1982;25:693–703.
Ross M, Pezzi C, Pezzi T, Meurer D, Hickey R, Balch C. Patterns of failure in anorectal melanoma. A guide to surgical therapy. Arch Surg. 1990;125:313–6.
Ballo MT, Gershenwald JE, Zagars GK, Lee JE, Mansfield PF, Strom EA, Bedikian AY, Kim KB, Papadopoulos NE, Prieto VG, Ross MI. Sphincter-sparing local excision and adjuvant radiation for anal-rectal melanoma. J Clin Oncol. 2002;20:4555–8.
Weyandt GH, Eggert AO, Houf M, Raulf F, Brocker EB, Becker JC. Anorectal melanoma: surgical management guidelines according to tumour thickness. Br J Cancer. 2003;89:2019–22.
Bullard KM, Tuttle TM, Rothenberger DA, Madoff RD, Baxter NN, Finne CO, Spencer MP. Surgical therapy for anorectal melanoma. J Am Coll Surg. 2003;196:206–11.
Yap LB, Neary P. A comparison of wide local excision with abdominoperineal resection in anorectal melanoma. Melanoma Res. 2004;14:147–50.
Pessaux P, Pocard M, Elias D, Duvillard P, Avril MF, Zimmerman P, Lasser P. Surgical management of primary anorectal melanoma. Br J Surg. 2004;91:1183–7.
Droesch JT, Flum DR, Mann GN. Wide local excision or abdominoperineal resection as the initial treatment for anorectal melanoma? Am J Surg. 2005;189:446–9.
Yeh JJ, Shia J, Hwu WJ, Busam KJ, Paty PB, Guillem JG, Coit DG, Wong WD, Weiser MR. The role of abdominoperineal resection as surgical therapy for anorectal melanoma. Ann Surg. 2006;244:1012–7.
Homsi J, Garrett C. Melanoma of the anal canal: a case series. Dis Colon Rectum. 2007;50:1004–10.
Iddings DM, Chen SL, Faries MB, Deacon L, Essner R, Morton DL. A new paradigm in the management of anorectal melanoma: trans-anal excision with sphincter preservation and sentinel node biopsy. J Clin Oncol. 2007;25(18S):Abstract 8513.
Podnos YD, Tsai NC, Smith D, Ellenhorn JD. Factors affecting survival in patients with anal melanoma. Am Surg. 2006;72:917–20.
Moozar KL, Wong CS, Couture J. Anorectal malignant melanoma: treatment with surgery or radiation therapy, or both. Can J Surg. 2003;46(5):345–9.
Acknowledgment
Supported by grant CA29605 from the National Cancer Institute and by funding from the Amyx Foundation, Inc. (Boise, ID), the Wayne and Gladys Valley Foundation (Oakland, CA), Mr. and Mrs. Louis Johnson, (Stanfield, AZ), Berton M. Kirshner (Los Angeles, CA), Todd Kirshner (Los Angeles, CA), Heather and Jim Murren (Las Vegas, NV), Mrs. Marianne Reis (Lake Forest, CA), the Wallis Foundation (Los Angeles, CA), the Harold J. McAlister Charitable Foundation (Los Angeles, CA), the Family of Robert Novick (Los Angeles, CA), the Weil Family Fund (Los Angeles, CA), and the Wrather Family Foundation (Los Alamos, CA).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Iddings, D.M., Fleisig, A.J., Chen, S.L. et al. Practice Patterns and Outcomes for Anorectal Melanoma in the USA, Reviewing Three Decades of Treatment: Is More Extensive Surgical Resection Beneficial in All Patients?. Ann Surg Oncol 17, 40–44 (2010). https://doi.org/10.1245/s10434-009-0705-0
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-009-0705-0