Article Text

Abstract
Background A European League Against Rheumatism (EULAR) taskforce was convened to develop recommendations for lifestyle behaviours in rheumatic and musculoskeletal diseases (RMDs). This paper reviews the literature on the effects of physical exercise and body weight on disease-specific outcomes of people with RMDs.
Methods Three systematic reviews were conducted to summarise evidence related to exercise and weight in seven RMDs: osteoarthritis, rheumatoid arthritis, systemic lupus erythematosus, axial spondyloarthritis (axSpA), psoriatic arthritis, systemic sclerosis and gout. Systematic reviews and original studies were included if they assessed exercise or weight in one of the above RMDs, and reported results regarding disease-specific outcomes (eg, pain, function, joint damage). Systematic reviews were only included if published between 2013–2018. Search strategies were implemented in the Medline, Embase, Cochrane Library of systematic reviews and CENTRAL databases.
Results 236 articles on exercise and 181 articles on weight were included. Exercise interventions resulted in improvements in outcomes such as pain and function across all the RMDs, although the size of the effect varied by RMD and intervention. Disease activity was not influenced by exercise, other than in axSpA. Increased body weight was associated with worse outcomes for the majority of RMDs and outcomes assessed. In general, study quality was moderate for the literature on exercise and body weight in RMDs, although there was large heterogeneity between studies.
Conclusion The current literature supports recommending exercise and the maintenance of a healthy body weight for people with RMDs.
- epidemiology
- arthritis
- patient reported outcome measures
- physical therapy modalities
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Body weight and physical exercise are important for health.
It is unclear whether body weight or change in body weight and exercise influence outcomes in rheumatic and musculoskeletal diseases (RMDs).
What does this study add?
This study summarises the literature on the association between exercise and weight with disease outcomes of seven RMDs, concluding that performing exercise and a healthy weight are associated with better outcomes in people with RMDs.
How might this impact on clinical practice or further developments?
People with RMDs should be encouraged to perform exercise if they do not currently perform exercise, or maintain exercise if performing sufficient quantities.
People with RMDs should be encouraged and supported to attain and maintain a healthy body weight.
Introduction
Rheumatic and musculoskeletal diseases (RMDs) comprise a wide range of conditions characterised by pain, disability and poorer quality of life (QoL).1–3 Globally, these conditions comprise a significant burden which is continuing to increase. For instance, the Global Burden of Disease study reported that the percentage increase of disability adjusted life years driven by RMDs (other than lower back pain) was 128.9% (95% CI 122.0% to 136.3%) between 1990 and 2019 across all age groups.4 While some RMDs have many effective pharmacological treatments (eg, rheumatoid arthritis (RA)5), for some the treatment options are limited (eg, systemic lupus erythematosus (SLE)6) and for others there are no effective disease modifying treatments (eg, osteoarthritis (OA)7). However, there is room for additional improvements in outcomes in all RMDs, potentially through modification of lifestyle behaviour.
Physical activity (including exercise)8 is clearly beneficial for health, regardless of the presence of chronic diseases such as RMDs. The WHO and American institutions recommend that all adults aged 18–65 years should participate in at least 150 min per week of moderate-intensity aerobic physical activity, or do at least 75 min of vigorous-intensity aerobic physical activity, or an equivalent combination of moderate- and vigorous-intensity activity (moderate intensity=3.0 to <6.0 METs (metabolic equivalent of task), vigorous intensity =≥6 METs, where 1 MET is the rate of energy expenditure at rest). Additionally, all adults aged 18–65 years should perform muscle-strengthening activities (eg, resistance training and weight lifting) involving major muscle groups on two or more days a week.9 10 In 2018, the European League Against Rheumatism (EULAR) recommended physical activity for people with inflammatory arthritis and OA,11 after a systematic review illustrating the benefits of exercise on strength, flexibility and cardiovascular fitness.12 Furthermore, exercise is closely linked to body weight. The prevalence of global obesity is increasing and obesity, as well as physical inactivity, is associated with poor health, comorbidity (eg, cardiovascular disease,13 diabetes,14) and increased risk of mortality.13 Therefore, there is an urgent need for strategies to ameliorate the obesity epidemic for the benefit of global health.
However, it is unclear whether exercise is effective at improving RMD-specific outcomes (eg, pain, disability), or whether excess weight is associated with worse RMD outcomes. Therefore, a EULAR taskforce was convened in 2018 to develop recommendations for lifestyle improvements in RMDs, with the focus on lifestyles that affect disease progression. The taskforce decided to focus on six lifestyle factors: diet, exercise, body weight, alcohol, smoking and (paid) work-participation, in seven diseases: RA, OA, SLE, axial spondyloarthritis (axSpA), psoriatic arthritis (PsA), systemic sclerosis (SSc) and gout (henceforth referred to collectively as RMDs). For each of these lifestyle factors, systematic reviews were performed, aiming to collate all relevant literature on each factor in order to formulate evidence-based recommendations. This article presents the results of the systematic reviews assessing the impact of exercise and body weight on the disease-specific outcomes of people with RMDs.
Methods
Design
These reviews were conducted following EULAR’s standard operating procedure for EULAR endorsed recommendations15 and are reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.16
Search strategy
A two-step process was used to identify studies to include in each review. Initially, a review of systematic reviews was conducted using the MEDLINE, EMBASE and Cochrane Library databases, aiming to identify existing systematic reviews on the included exposures and RMD progression (online supplemental tables 1 and 2, defined a priori by the study team) that were published from 1 January 2013 to 18 September 2018. Two reviewers screened the titles and abstracts (JMG and MW) and then a team of four reviewers screened the eligible full texts (JMG, MW, JR-C and GC; each full text screened by two reviewers). Only existing systematic reviews relating to exercise and weight are presented here.
Supplemental material
Following this, separate systematic reviews of original studies of exercise and weight in RMDs were conducted (from inception to search date). It was decided that there were sufficient numbers of published systematic reviews regarding exercise and OA and therefore OA was not included in the systematic review of original studies of exercise. Search strategies for each review were developed based on a predefined PICO strategy (participants, intervention/exposure, comparison, outcome) (online supplemental tables 3 and 4 for search strategies) and implemented in the MEDLINE, EMBASE and CENTRAL databases (dates when strategies were implemented: exercise: 18 March 2019; weight: 14 March 2019). Titles and abstracts, followed by full texts, were screened by two reviewers (exercise: JMG and GC; weight: JMG and SMMV).
Inclusion and exclusion criteria
Systematic reviews were included if they:
Included adults with an RMD (OA, RA, SLE, axSpA, PsA, SSc, gout).
Studied the relationship between exercise or weight and disease-specific outcomes (online supplemental table 5 for list of included outcomes).
Published in English, French, Spanish or Italian.
No restrictions were implemented regarding the included study designs of studies in systematic reviews.
Original studies were included if they:
Used a longitudinal study design (randomised controlled trials (RCTs), non-randomised trials, single-arm intervention studies, longitudinal observational studies)
Included adults with an RMD (RA, SLE, axSpA, PsA, SSc, gout (and OA for the weight review)).
Studied the relationship between exercise or weight and outcomes (online supplemental table 5 for list of included outcomes).
Published in English, French, Spanish or Italian.
Conference abstracts were excluded.
Risk of bias assessment
To assess the risk of bias of included systematic reviews and meta-analyses, the AMSTAR-2 tool was used.17 Each included review or meta-analysis was rated as critically low, low, moderate or high quality. For included RCTs, an abbreviated version of the Cochrane Risk of Bias tool was used,18 assessing four criteria: randomisation procedure, allocation concealment procedure, blinding of participants and blinding of assessors. Each aspect was rated as either low or high/unclear risk of bias. A machine learning algorithm was used to assist the process,19 which identifies passages of text from included manuscripts and assigns grades for each criteria. A reviewer (JMG) checked each of the algorithm’s grades and if there was disagreement, changed the grade. The QUIPS tool was used to assess the quality of observational studies across six domains: study population, attrition, exposure measurement, outcome measurement, confounding and statistical analysis.20
Synthesis of data
Data from articles were extracted into prespecified tables, including study design, demographics, and results of outcomes and follow-up. The data from the individual articles are presented in the form of a narrative summary. Where possible, the mean and SD were extracted. SDs were estimated from 95% CIs or SEs when not reported. Means and SDs were estimated from medians and range/IQR when only these summary statistics were presented using published formulas.21 Furthermore, standardised mean differences (SMD) were calculated for individual studies as this allows results measured on different instruments to be compared and combined (SMDs provided in online supplemental materials). The SMD was estimated as the difference between the scores of the intervention and control group at follow-up divided by the pooled SD. Meta-analysis was used to combine the results of RCTs where possible. An SMD ≥0.2 was considered a small effect, ≥0.5 as a medium-sized effect and ≥0.8 as a large effect.22 Heterogeneity was quantified using the I2 statistic. All statistical analyses were performed using Stata V.14 (StataCorp).
Grades of Recommendations, Assessment, Development and Evaluation (GRADE) defines high-quality evidence as evidence where further research is very unlikely to change our confidence in the estimate of effect.23 Therefore, evidence was rated as high quality if supported by meta-analyses of ≥5 RCTs at low-moderate risk of bias reporting consistent results without important limitations.24 GRADE defines moderate quality evidence as evidence where further research is likely to have an important impact on the confidence of the estimate of effect, or may change the estimate.23 Evidence was rated as moderate if supported by meta-analyses of ≥3 RCTs or supported by a single RCT with a sample size ≥100 and at low-moderate risk of bias or multiple large observational studies. GRADE defines low quality evidence as evidence where further research is very likely to have an important influence on our confidence in the estimates, or likely to change the estimate.23 Evidence was rated as low if supported by multiple RCTs of small sample size or high risk of bias or by single observational studies only. GRADE defines very low quality of evidence as evidence where the estimate of the effect is very uncertain.23 Evidence was rated as very low if supported by single small RCTs, or non-randomised trials or single arm intervention studies. Evidence could be downgraded in the event of other potential biases (such as study limitations, inconsistency of results, imprecision, publication bias24 or conflicts of interest).
Results
Search strategy and study characteristics
The search strategy to identify published systematic reviews identified 1507 abstracts, of which 16 were duplicates and were removed by reference managing software. After title and abstract screening, 1366 abstracts were excluded and the full manuscripts of the remaining 125 were screened. Seventy-nine of these assessed exercise and 10 assessed weight (figure 1).

Flow chart of search strategy to identify published systematic reviews and meta-analyses. *EMBASE search excluded journals included in MEDLINE.
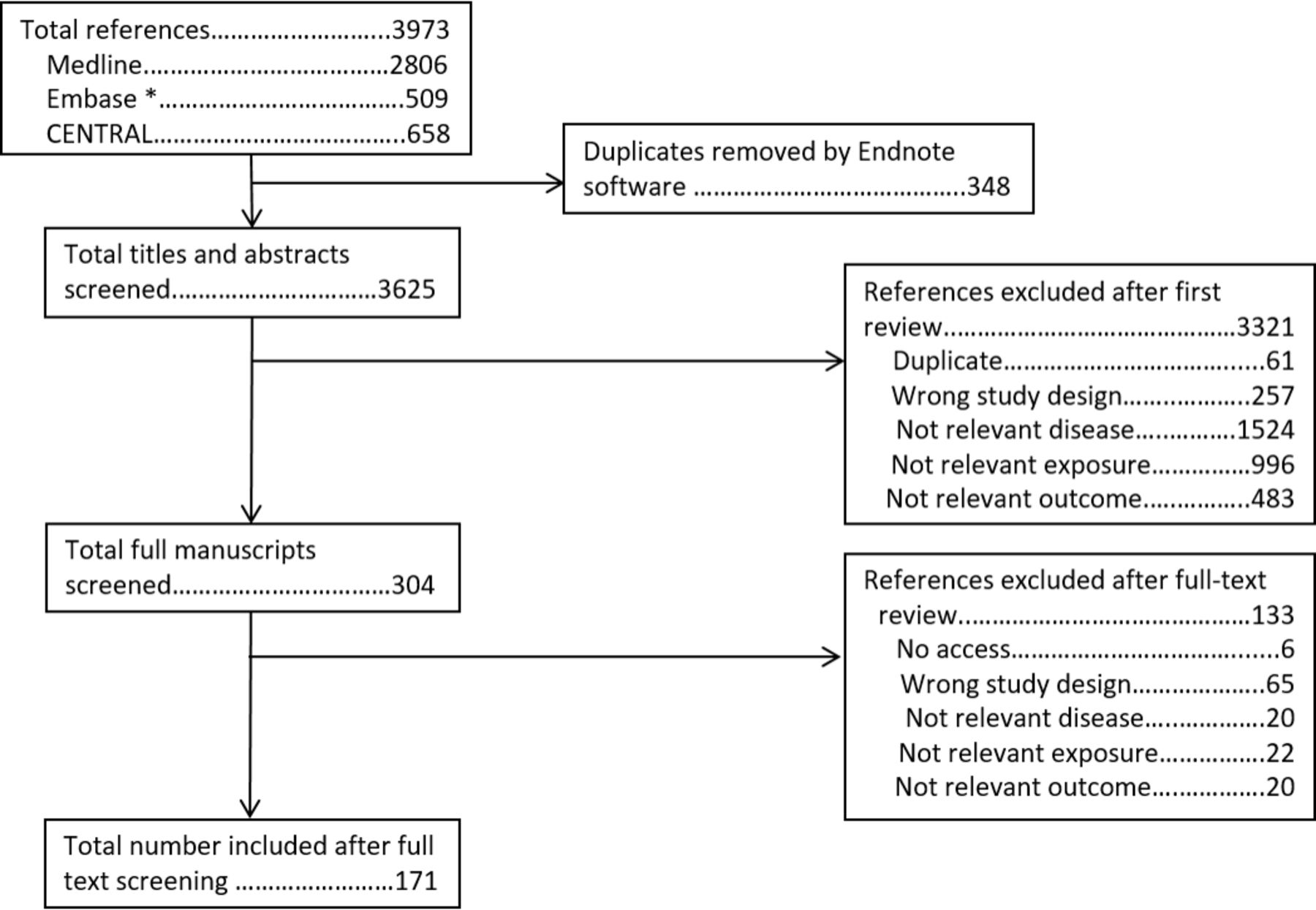
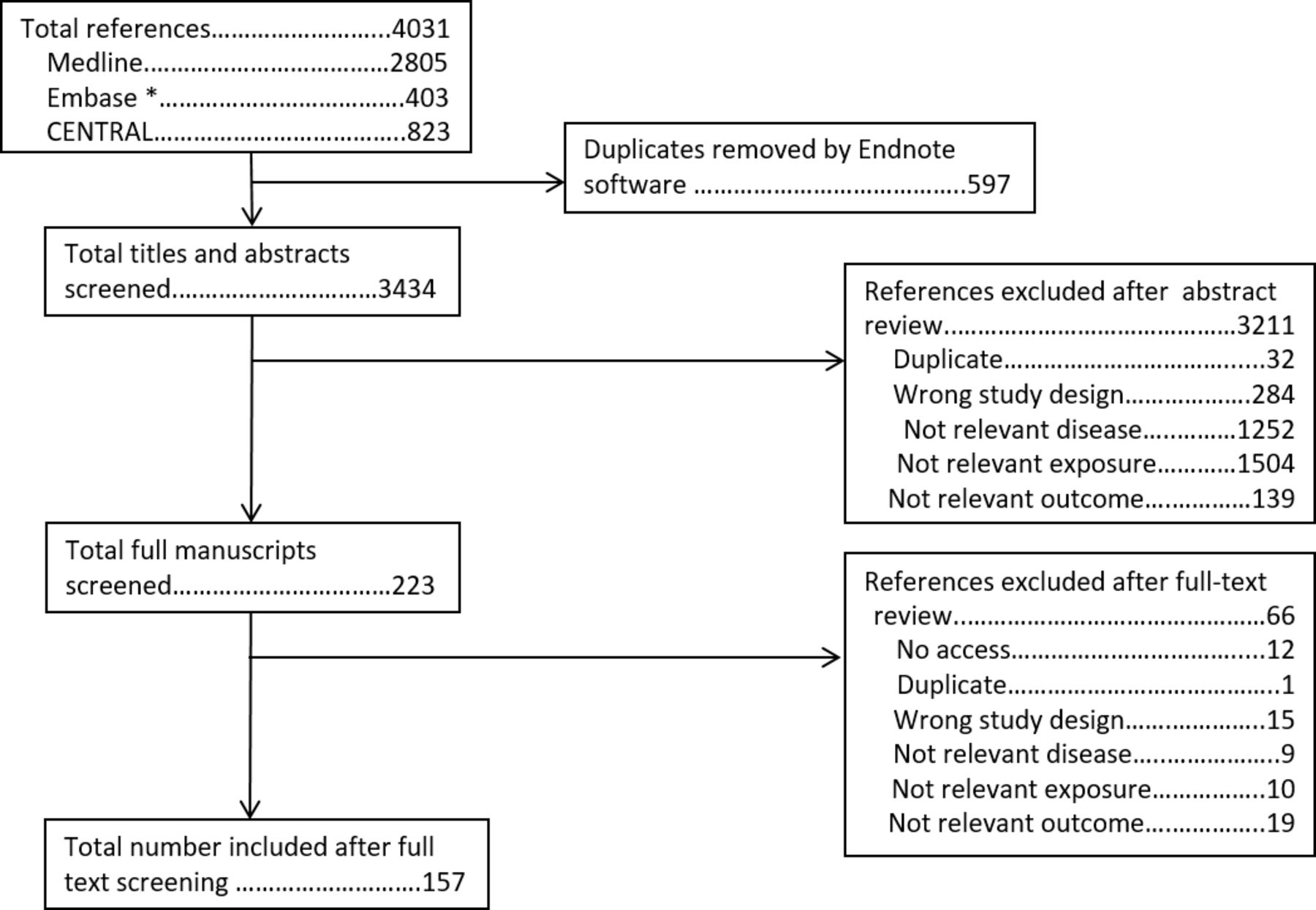
The search strategy to identify original articles assessing exercise in RMDs identified 4031 abstracts. After removal of 597 duplicates, 3434 titles and abstracts were screened. Of these 223 full manuscripts were screened, of which 157 are included in this review (figure 2). The search strategy to identify original articles assessing weight identified 3973 abstracts. Once duplicates were removed, 3625 abstracts were screened, followed by screening of 304 full manuscripts. In total, 171 studies on weight were included (figure 3). Results are summarised in tables 1 and 2, with additional information on demographics, specific interventions and control groups (typically usual care or wait-list control), and results of meta-analyses provided in online supplemental material.
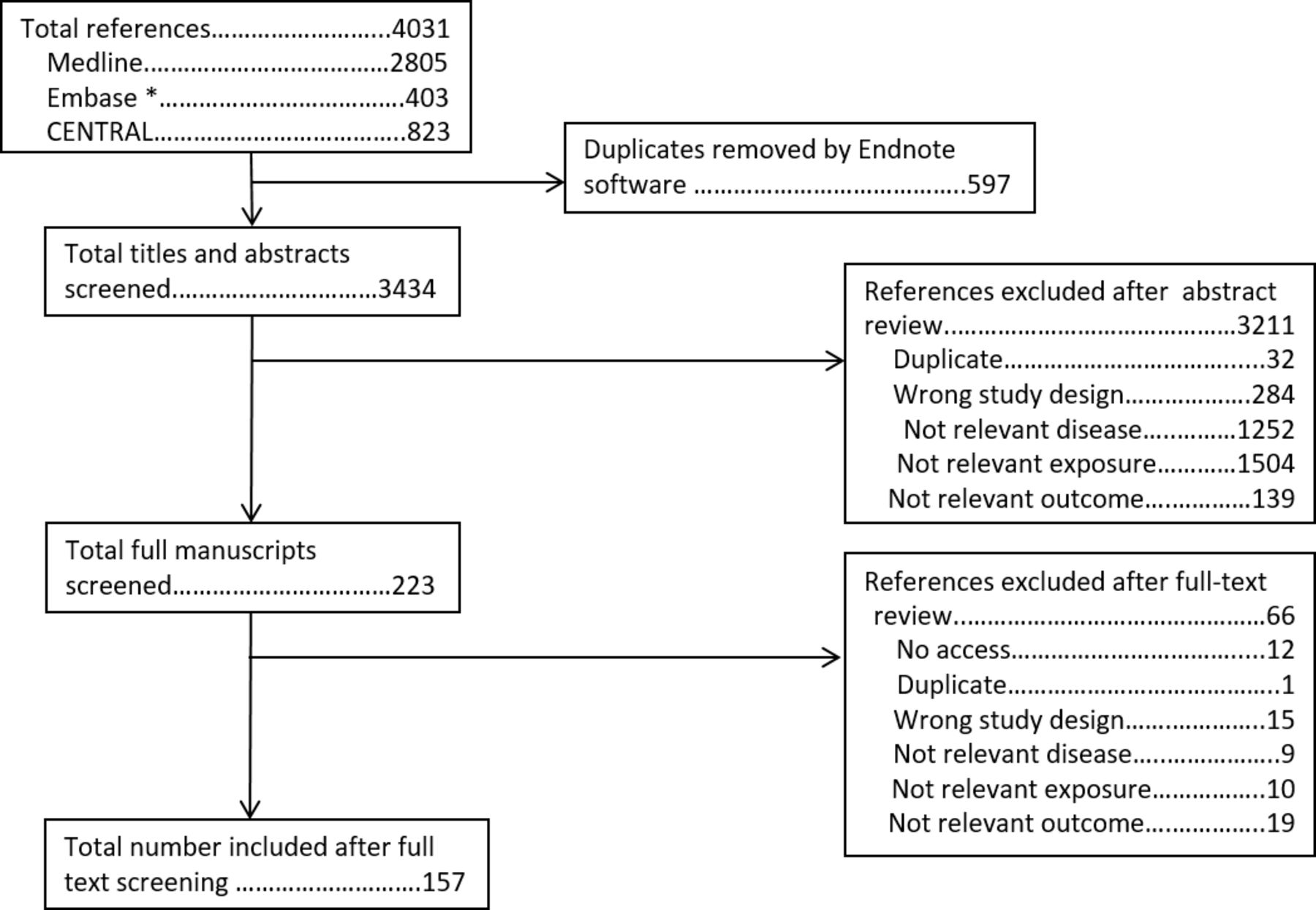
PRISMA flow chart for review of individual studies of exercise. *EMBASE search excluded journals included in MEDLINE. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
{kind=link}
{kind=link}
{kind=link}
PRISMA flow chart for review of individual studies of weight. *EMBASE search excluded journals included in MEDLINE. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Summary table of results regarding exercise
Summary table of results from observational studies within the weight systematic review
Exercise
Osteoarthritis
Aerobic exercise
Four meta-analyses of RCTs,25–28 four systematic reviews of RCTs29–32 and three systematic reviews of observational studies33–35 assessed aerobic exercise for OA. Aerobic exercise improved pain25–27 30–33 and function25 29–32 34 with small-medium effect sizes (pain SMD ranges −0.24 (95% CI −0.50 to 0.02)30 to -0.61 (95% CI −0.75 to –0.48)25; function −0.30 (95% CI −1.53 to 0.92)28 to −0.58 (95% CI −0.75 to –0.40)25) as well as one study reporting an association with health-related QoL (HR-QoL).31 Another review reported no association with radiographic damage35 (online supplemental tables 6 and 7).
Aquatic exercise
Five meta-analyses of RCTs28 36–39 and three systematic reviews of RCTs7 32 40 studied aquatic exercise for OA. Small effects on pain7 28 32 36 37 39 (SMDs ranging −0.26 (95% CI −0.41 to –0.11)39 to −1.16 (95% CI -3.03 to 0.71)38) function7 32 37–39 (SMDs ranging −0.22 (95% CI −0.38 to –0.07)39 to −0.55 (95% CI −0.94 to –0.16)38) and HR-QoL37–39 (SMDs ranging −0.21 (95% CI −0.59 to 0.18)38 to −0.25 (95% CI −0.49 to –0.01)37)were reported (online supplemental tables 8 and 9).
Guidelines / recommendations
Two systematic reviews41 42 summarised recent guidelines and evidence for OA and exercise, both concluding that exercise is strongly recommended for OA. A third paper43 contained a literature review supporting EULAR recommendations for the non-pharmacological management of OA, also recommending that patients with OA have regular, individualised exercise regimens (online supplemental tables 10 and 11).
High vs low intensity exercise
One Cochrane review44 reported that high intensity exercise was more beneficial than low intensity exercise for pain (meta-MD in the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain scale −0.84 (95% CI −1.63 to –0.04)) and function (meta-MD WOMAC function −2.65 (95% CI −5.29 to –0.01)) in OA. A systematic review45 identified one prospective study46 that reported no exercise or low intensity exercise was associated with deterioration in physical function (online supplemental tables 12 and 13).
Home exercise
One meta-analysis47 reported that home exercise interventions were superior to no exercise in terms of pain (SMD −0.46 (95% CI −0.68 to –0.24)) and function (SMD −0.35 (95% CI −0.56 to –0.15)) in OA, but home exercise programmes were inferior to supervised exercise (online supplemental tables 14 and 15).
Land-based exercise
Several articles assessed the efficacy of any type of land-based exercise (as opposed to aquatic) for OA: five meta-analyses of RCTs,36 48–51 one systematic review of meta-analyses, reviews and RCTs7 and one systematic review of RCTs.40 The meta-analyses all reported small effects in favour of land based exercise in terms of pain (SMDs ranging from −0.24 (95% CI −0.42 to –0.06)48 to −0.49 (95% CI −0.59 to –0.39)51) and function (SMDs ranging from −0.34 (95% CI −0.50 to –0.18)48 to -0.52 (95% CI −0.64 to –0.39)51), with the systematic reviews in agreement. One meta-analysis also reported an improvement in HR-QoL following exercise (SMD 0.28 (95% CI 0.15 to 0.40))51 (online supplemental tables 16 and 17).
Multidisciplinary interventions
One meta-analysis52 and one systematic review53 reported multimodal interventions were superior to exercise only for pain, function and HR-QoL (online supplemental tables 18 and 19).
Muscle strengthening exercise
Nine meta-analyses of RCTs,25–28 54–58 four systematic reviews of RCTs,29 59 60 and one review of meta-analyses, reviews and RCTs7 assessed muscle strengthening exercise for OA. Small26 55 56 58 to medium25 27 28 sized effects on pain7 59 60 (SMDs ranging from −0.23 (95% CI −0.42 to –0.04)55 to −1.19 (95% CI −1.67 to –0.70)57), as well as small28 56 to medium25 57 58 effects on function were reported7 59 60 (SMDs ranging from −0.10 (95% CI −0.33 to 0.13)55 to −0.60 (95% CI −0.83 to –0.37)25). One meta-analysis reported no effect of muscle strengthening exercise on HR-QoL for hand OA,56 whereas a systematic review reported improvements in HR-QoL in knee OA59 (online supplemental tables 20 and 21).
Physical exercise therapy
In total, five meta-analyses of RCTs,61–65 two systematic reviews of RCTs,60 66 and one systematic review of reviews and RCTs67 assessed exercise therapy for OA. Small effects for pain60 62–64 66 (SMDs ranging from −0.20 (95% CI −0.28 to –0.11)62 to -0.71 (95% CI −1.60 to 0.19)64) and function were reported60 62 63 65 66 (SMDs ranging from −0.07 (95% CI −0.28, 0.15)64 to −0.33 (95% CI −0.50 to –0.15)63), and no effect on anxiety (SMD −0.11 (95% CI −0.26 to 0.05)) and depression (SMD −0.16 (95% CI −0.29 to –0.02)).62 One meta-analysis reported a medium-sized effect on HR-QoL in knee OA (SMD 0.70 (95% CI 0.20 to 1.20)),61 but another reported no effect in hip OA (SMD −0.06 (95% CI −0.27 to 0.16))63 (online supplemental tables 22 and 23).
Tai chi
Four meta-analyses of RCTs26 68–70 and one systematic review of RCTs71 assessed tai chi for OA. Medium-sized effects were reported in terms of pain26 68–70 (SMDs ranged from −0.45 (95% CI −0.70 to –0.20)70 to −0.77 (95% CI −1.13 to –0.41)68) and function68–70 (SMDs ranged from −0.61 (95% CI −0.85 to –0.37)70 to −0.75 (95% CI −0.98 to –0.52)68), and small effects on stiffness68 70 and HR-QoL68 69 (online supplemental tables 24 and 25).
Yoga
One meta-analysis of RCTs,72 two systematic reviews of RCTs71 73 and one systematic review of RCTs and single arm interventions,74 assessed yoga in OA. Three systematic reviews reported benefits of yoga on pain and function.71 73 74 The meta-analysis reported a large effect of yoga on function (SMD −1.83 (95% CI −2.09 to –1.57)).72 One systematic review reported inconsistent findings in terms of the effect of yoga on HR-QoL74 (online supplemental tables 26 and 27).
OA summary
The majority of systematic reviews and meta-analyses reported medium-sized effects of physical activity on pain and function in OA, including both aerobic and muscle strengthening physical activity. The quality of the evidence was generally moderate to high (table 1). While the majority of studies on OA included people with knee or hip OA, several studies included people with hand OA.42 52 55 56 64 73
Rheumatoid arthritis
Aerobic exercise
One meta-analysis,75 three systematic reviews76–78 (which highlighted a 2010 meta-analysis,79) eight RCTs,80–87 four non-randomised studies,88–91 one case–control study92 and two prospective cohort studies93 94 assessing aerobic exercise in RA were included. Aerobic exercise improved pain76 77 79 80 82 84 87 (meta-analysis79: SMD 0.31 (95% CI 0.06 to 0.55)); and function76 79 80 84 (meta-analysis79: SMD 0.24 (95% CI 0.10 to 0.38)) in RA with small effect sizes, although some studies reported statistically non-significant results. One meta-analysis and four included RCTs reported no effect of aerobic exercise on disease activity79 80 82 83 85 (meta-analysis79: SMD 0.08 (95% CI −0.08 to 0.25)), while another reported a weak correlation.78 Furthermore, studies reported a small effect on HR-QoL.79 81 82 84 Small effects were also reported on fatigue (meta-analysis75: SMD −0.31 (95% CI –0.55 to –0.06)), anxiety, depression and self-efficacy75 81 82 85 (online supplemental tables 28–31).
Aerobic + muscle strengthening exercise
Twenty-one reports of RCTs,95–115 one non-randomised trial,116 and seven single arm studies117–123 reported on interventions containing both aerobic and muscle strengthening elements in RA. Small effects were reported for pain96 99 101 106 110–112 and function,95–100 102 106 108–111 115 with wide heterogeneity between studies potentially due to differences in the interventions and follow-up lengths. No effect was observed for disease activity102 106 108 110 and depression.97 101 Two RCTs reported a small effect on HR-QoL, which was not statistically significant.98 102 One recent RCT reported a medium-sized effect on fatigue,96 with two older RCTs reporting no effect101 115 (online supplemental tables 32 and 33).
Aquatic exercise
Two systematic reviews,77 124 four RCTs87 125–127 and one non-randomised trial89 studied aquatic exercises for RA. Small-medium effects on pain87 124 126 and function77 124–127 were reported (online supplemental tables 34–36).
High vs low intensity
Three RCTs128–130 and one long-term extension131 were included, with none reporting significant differences between high and low intensity exercise on pain or function (online supplemental tables 37 and 38).
Home exercise
Two systematic reviews,77 132 and five RCTs101 133–136 studied home exercise programmes. The reviews concluded that home exercise was beneficial for reducing pain and function.77 132 In studies comparing home-based unsupervised physical activity to supervised physical activity, inconsistent results were reported in terms of pain101 134 135 and function134–136 potentially due to differences in the interventions between studies (online supplemental tables 39–41).
Muscle strengthening exercise
One meta-analysis of hand muscle strengthening exercises,137 three systematic reviews (one including a 2012 meta-analysis138)77 139 140 17 reports of RCTs and long-term extensions,128 131 141–155 1 non-randomised trial156 and 1 single-arm study157 assessed muscle strengthening exercise in RA. Small effects from muscle strengthening exercise were reported on pain77 137 138 140 141 143 144 153 (meta-analysis138: MD pain Visual Analogue Scale −4.13 (95% CI −10.97 to 2.71)). Inconsistent results were reported in terms of function, with several studies reporting improvements in function77 137 138 143 148 149 151 (meta-analysis138: MD Health Assessment Questionnaire −0.22 (95% CI −0.35 to –0.10)), whereas other RCTs reported no benefit,128 144 147 152 153 potentially due to differences in the comparison group where some were given low-intensity exercise or exercise advice. No effect was reported on disease activity128 140 143 145 147 and HR-QoL142 144 145 147 (online supplemental tables 42–44).
Tai chi
One systematic review (which identified a 2004 review158)77 one RCT,159 one non-randomised trial160 and two single-arm studies161 162 assessed tai chi for RA. The reviews and RCT reported no benefit in terms of pain,159 function,77 158 159 disease activity77 158 or depression159 (online supplemental tables 45–47).
Yoga
One meta-analysis,72 one systematic review,73 three RCTs163–165 and two non-randomised trials166 167 studied yoga for RA. The meta-analysis reported a large effect of yoga on pain (but included some patients with OA)72 as did one RCT,165 whereas two other RCTs reported no effect, and the systematic review graded the evidence as very low.73 163 164 The meta-analysis (only including studies of RA)72 and one RCT reported medium-sized effects on function,163 whereas another RCT reported no effect.164 No effect on disease activity was reported by two RCTs.163 164 Studies were generally small therefore potentially some findings are due to chance (online supplemental tables 48–50).
RA summary
There was moderate-high quality evidence of a small effect of physical activity on pain and function in RA. Physical activity did not affect disease activity (table 1).
Systemic lupus erythematosus
Aerobic exercise
Two meta-analyses,168 169 three systematic reviews,170–172 four RCTs173–176 and three non-randomised trials177–179 assessed aerobic exercise in SLE. One RCT reported lower pain,173 whereas another did not174 although both studies had low sample sizes. No effect of disease activity was reported.168 173 174 A medium-sized effect on fatigue was also reported (MD −0.61 [95% CI −1.19 to –0.02]168; MD −0.52 [95% CI −0.92 to –0.13]169)168 169 171 172 175 176 (online supplemental tables 51–53).
Aerobic & muscle strengthening exercise
One meta-analysis,168 one systematic review171 and three RCTs173 180 181 compared aerobic and muscle strengthening exercise, whereas one RCT182 and one non-randomised trial183 assessed interventions combining both aerobic and muscle strengthening exercises. Aerobic exercise was reported to lead to less fatigue compared with muscle strengthening in two studies,168 171 but two other RCTs reported no difference,180 181 although again sample sizes were small. No difference was reported in terms of disease activity168 173 181 or depression168 173 180 (online supplemental tables 54–56).
Muscle strengthening exercise
One RCT compared muscle strengthening exercise to control in SLE,173 reporting no effect on disease activity, pain and fatigue, but a medium-sized effect on depression in favour of muscle strengthening exercise (online supplemental tables 57 and 58).
SLE summary
There is moderate quality evidence of a medium-sized effect of aerobic exercise on fatigue in SLE. There is low-quality evidence that physical activity does not affect disease activity in SLE (table 1).
Axial spondyloarthritis
Aerobic exercise
Two systematic reviews,184 185 four RCTs,186–189 one single arm study190 and three prospective cohort studies191–193 assessed aerobic exercise in axSpA. One RCT investigating exercising with the aid of a video game console reported a medium-sized effect on pain, function and disease activity,186 whereas other studies of traditional exercise interventions reported no effect184 187–189 (online supplemental tables 59–62).
Aerobic + muscle strengthening exercise
Six meta-analyses,194–199 3 systematic reviews,184 185 200 10 RCTs,201–210 3 non-randomised trials,211–213 5 single arm studies214–218 and 1 prospective cohort study219 assessed aerobic + muscle strengthening exercise in axSpA. Small effects were reported for pain,185 196 197 204 209 210 but with some inconsistency200 207 208 (SMDs ranging from −0.22 (95% CI −0.49 to 0.06)197 to −0.42 (95% CI −0.74 to –0.09),196 whereas consistent medium-sized improvements in function184 194–199 201 203 205 207 210 (SMDs ranging from −0.44 (95% CI −0.79 to –0.09)199 to −0.72 (−1.03 to –0.40),194 and disease activity184 194–199 201 205 206 (SMDs ranging from −0.47 (95% CI −0.84 to –0.09)196 to -0.90 (−1.52 to –0.27)194 were reported. Medium-sized effects on fatigue201 202 and spinal mobility195 198 199 205 were also reported (online supplemental tables 63–66).
Aquatic exercise
Three systematic reviews184 200 220 and two RCTs221 222 assessing aquatic exercise for axSpA were included. Small, inconsistent effects were reported in terms of pain,184 220–222 function184 200 220–222 and disease activity184 220–222 and no effect on spinal mobility184 221 222 (online supplemental tables 67–69).
Home-based exercise
One meta-analysis,197 one systematic review,185 eight RCTs,186 189 203 207 210 223–225 five non-randomised trials212 226–229 and one single arm study217 assessed home-based exercise. Compared with control, home exercise had a medium-sized effect on pain,186 197 210 224 function,186 189 197 210 223–225 disease activity186 197 223 224 and HR-QoL.186 224 However, several studies found that group-based exercise was more effective than home-based exercise in terms of function203 207 and disease activity203 (online supplemental tables 70–72).
Muscle strengthening exercise
Eight RCTs (and two long-term follow-ups),223 225 230–237 three non-randomised trials226–228 and three single arm studies238–240 assessed muscle strengthening exercise. Medium-sized effects of muscle strengthening exercise were reported in terms of pain,225 231–233 235 function223 225 230 232–235 and disease activity223 230 232–235 (online supplemental tables 73 and 74).
AxSpA summary
There is high-quality evidence of a medium-sized effect of aerobic + muscle strengthening exercise in axSpA. Muscle strengthening exercise results in larger and more consistent effects on pain, function and disease activity compared with aerobic exercise (table 1).
Psoriatic arthritis
Muscle strengthening exercise
One RCT241 and one single arm study242 assessed muscle strengthening exercise in PsA. The RCT reported better function and disease activity at 12 weeks compared with the control arm241 (online supplemental tables 75 and 76).
PsA Summary
There is little evidence of the effect of physical activity in PsA.
Systemic sclerosis
Aerobic exercise
One single arm study243 reported improvements in function between baseline and 4 months after the intervention (online supplemental tables 77 and 78).
Aerobic + muscle strengthening exercise
One systematic review,244 two RCTs245 246 and one single arm study247 assessed aerobic plus muscle strengthening interventions for SSc, reporting a small effect on function245 246 but no effect on pain246 (online supplemental tables 79–81).
Aquatic exercise
One RCT,248 which only reported data on the intervention group, showed improvements in function from baseline to 18 weeks follow-up (online supplemental tables 82 and 83).
Muscle strengthening exercise
One RCT,249 one non-randomised trial250 and three single arm studies251–253 assessed muscle strengthening exercise in SSc. The RCT reported a medium-sized effect on function249 and the non-randomised study reported better outcomes in terms of pain and function in the exercise arm250 (online supplemental tables 84 and 85).
SSc summary
There is very-low-quality evidence of a medium effect of physical activity on function in SSc (table 1).
Gout
Aerobic exercise
One case–control study254 reported that performing regular exercise ≥150 min per week was associated with reduced odds of tophus in gout (online supplemental tables 86 and 87).
Yoga
One RCT compared yoga to blood-letting in gout,255 reporting benefits of yoga in terms of pain and serum uric acid (online supplemental tables 88 and 89).
Gout summary
There is little research on the effect of physical activity in gout.
Body weight and weight reduction
Osteoarthritis
Two meta-analyses,26 33 5 systematic reviews,32 34 35 43 45 21 reports describing RCTs and long-term follow-up studies,256–276 2 non-randomised trials277 278 and 6 single-arm intervention studies assessing weight-loss interventions,279–284 as well as 44 observational studies285–328 assessing the association between body weight and outcomes in OA were identified. From studies assessing weight-loss interventions, small effects on pain,26 32 43 265–267 270 275 function,259 265–268 270 272 273 stiffness256 266 273 and walking tests,260 265 272 276 but no effect on HR-QoL260 269 or patient global assessment260 269 were reported. In observational studies, higher body weight was associated with higher pain33 291 292 299 300 302 307 but not with worse function45 287 297 303 319 or radiographic progression35 294 301 306 (online supplemental tables 90–115).
Rheumatoid arthritis
Three meta-analyses329–331 and 61 observational studies92 332–391 assessed the relationship between body weight and outcomes in RA. Higher weight was associated with worse pain,329 354 361 362 380 function,329 336 344 362 disease activity,329 330 336 338 339 342 344 347 357 361–363 366 384 389 and fatigue,351 as well as more comorbidities.331 355 360 365 374 390 Higher baseline weight was associated with lower risk of death.335 367 378 379 However, high rates of weight loss were associated with increased mortality risk.335 340 356 381 Higher weight was associated with lower radiographic progression337 341 346 347 368 371 375 376 (online supplemental tables 116–132).
Systemic lupus erythematosus
Eight prospective studies were identified assessing the relationship between body weight and outcomes in SLE.392–399 Higher weight was associated with worse function,394 comorbidity,396 398 399 employment status394 and mental health,392 but no associations between weight and disease activity395 or fatigue395 were reported (online supplemental tables 133–139).
Axial spondyloarthritis
Thirteen observational studies were identified assessing the relationship between body weight and outcomes in axSpA.192 359 400–410 Higher weight was associated with worse pain,410 disease activity,405 410 fatigue,405 radiographic progression,401 403 comorbidity359 404 and lower odds of meeting response criteria.405 409 One unadjusted analysis reported people with higher weight were more likely to discontinue anti-tumour necrosis factor treatment,406 but another study adjusting for confounders reported no association405 (online supplemental tables 140–149).
Psoriatic arthritis
One meta-analysis,330 one RCT,411 one single-arm study412 and seven observational studies413–419 were identified assessing the relationship between weight and outcomes in PsA. Higher weight was associated with worse pain,415 function,415 disease activity,330 414–417 joint counts,415 enthesitis occurrence413 and psoriasis score.415 Interventional studies reported improvements in pain,411 412 function,411 412 patient global assessment,411 412 and reductions in disease activity411 412 and C-reactive protein411 412 following weight loss (online supplemental tables 150–170).
Systemic sclerosis
Two observational studies reported that higher weight was associated with a lower risk of mortality in SSc420 421 (online supplemental tables 171 and 172).
Gout
One systematic review,422 one single-arm study423 and five observational studies424–428 were identified assessing the relationship between weight and outcomes in gout. One observational study reported no association between weight and function.428 Weight loss was associated with improvements in serum uric acid level,422 423 425 and less frequent gout attacks.422–425 Higher weight was associated with renal failure in one study426 but not another428 (online supplemental tables 173–180).
Discussion
These three systematic reviews summarise the current evidence regarding the effects of physical activity and body weight on disease outcomes of people with seven RMDs. The data from over 400 published reviews and original articles suggests there are benefits of exercising for a range of outcomes important to people with RMDs, and also indicate an association between heavier body weight and worse outcomes, although differences were noted across RMDs. There was moderate-to-high-quality evidence that exercise interventions resulted in less pain and better function in RMDs, and exercise was also associated with reductions in disease activity in axSpA. The size of the effect of exercise varied between RMDs. For instance, there were medium-sized effects demonstrated in people with axSpA and only small effects in those with RA. There was moderate-quality evidence that heavier body weight was associated with poorer outcomes, including pain, function and disease activity, with relatively consistent results across the seven RMDs. However, the amount of available evidence varied considerably between RMDs, with the majority of studies focusing on OA, RA, axSpA and to a lesser extent SLE, with only a few studies available focusing on PsA, SSc and gout.
The majority of studies of exercise across the RMDs focused on aerobic and muscle strengthening exercise. Both appeared to improve outcomes in the seven RMDs included in this review, and when combined they seemed to produce stronger effects, although relatively few studies compared aerobic plus muscle strengthening exercise to either form of exercise individually.173 A few studies indicated that supervised exercise was marginally more effective than unsupervised home-based exercise,47 134 203 although this should not deter individuals who do not wish to attend exercise classes from performing home-based exercise. Overall, the current evidence base indicates that exercising results in better outcomes in people with RMDs, when compared with groups assigned to control groups with no exercise intervention. People with RMDs should be encouraged by their health professionals to start exercising if they currently perform no exercise, or maintain their exercise if they already perform a sufficient amount of exercise. Health professionals should also recognise that there are potentially large barriers to initiating and continuing to exercise for people with RMDs, including time, resources and lack of motivation, as well as disease specific barriers.429–431
Heavier body weight was consistently associated with poorer outcomes, including pain, function, disease activity, fatigue and comorbidities. The included studies evaluating weight-loss interventions typically reported improved outcomes in the weight-loss groups compared with controls.260 265 411 Additionally, multiple observational studies have reported an association between heavier baseline weight and worse disease outcomes. While these observational studies typically have longer follow-up compared with RCTs, causality between heavier body weight and worse outcomes is difficult to establish, given the complex interrelated associations between heavy weight and other potential sociodemographic and biological factors that could be influencing outcomes.432 433 Furthermore, the majority of research focused on OA and RA, with few research studies published on the other RMDs. Despite this, given the deleterious effect of heavier weight on other outcomes (eg, cardiovascular disease13 and type 2 diabetes14) and the association between weight and poor outcomes in RMDs, people with RMDs should be encouraged to attain and maintain a healthy weight (what consists a healthy weight will be person-specific and should be decided in consultation between the person with an RMD and their health professional).
This review has several limitations. While the large scope and high number of studies included means that a large proportion of the literature has been surveyed, due to the breadth of the research questions, some studies may have been missed. However, the extensive search strategies which were implemented in several databases should mean that these missing studies comprise a low proportion of the total evidence base. Due to the large number of studies, data extraction and risk of bias assessment were not performed in duplicate. Furthermore, due to the nature of the method of identifying studies, some selection bias could be influencing the results, particularly in the body weight systematic review. Many studies will assess multiple factors influencing progression of outcomes, and will often only report the significant associations in their abstracts. As our search strategy identified studies reporting that they studied the association between weight and outcomes in their abstracts, this potentially means we missed studies that assessed the association, found no relationship, and therefore did not report they had assessed weight in their abstract. The majority of studies on exercise were RCTs, with strict inclusion criteria, meaning the samples in these studies were often highly selected, thus reducing generalisability. The majority of studies on weight were longitudinal observational studies. While these studies typically had longer follow-up periods than the few interventional studies included, there is the possibility of differential attrition leading to biased results. For instance, those with higher weight may be more likely to have worse outcomes, which could lead them to leave the study before these outcomes are assessed. Lastly, as the evidence within this review was used to formulate the taskforce’s recommendations, an update was not deemed appropriate. However, this means that some relevant papers have been published in the interim between implementing the search strategy and publishing this paper which are not included.434 435
In conclusion, these reviews inform the 2021 EULAR recommendations which advise people with RMDs to perform sufficient amounts of exercise, given the beneficial effects of exercise on numerous outcomes. Furthermore, the 2021 EULAR recommendations also advise people with RMDs to maintain a healthy weight, given the association between heavier weight and poor outcomes, as detailed in this review.
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
References
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @james_gwinnutt
Contributors Study concept and design: JMG, MW, JR-C, GC, FG and SMMV; Acquisition of data: JMG, MW, JR-C, GC and SMMV; Analysis and interpretation of data: JMG, MW, JR-C, ABa, HB-F, ABo, GC, SdS, AdT, TED, RHM, PP, LS-F, TAS, KW-B, JW, MZ-S, FG and SMMV; Review of manuscript: JMG, MW, JR-C, ABa, HB-F, ABo, GC, SdS, AdT, TED, RHM, PP, LS-F, TAS, KW-B, JW, MZ-S, FG and SMMV; Guarantor: SMMV.
Funding This work was funded by the European League Against Rheumatism. SMMV and JMG are supported by Versus Arthritis (grant number 21755) and the NIHR Manchester Biomedical Research Centre. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.