
Abstract
Background
Symptoms related to Coronavirus-19 disease (COVID-19) and quarantine measures have caused pulmonary function abnormality and impaired respiratory mechanics. However, no studies are evaluating pulmonary functions and respiratory muscle strength in female volleyball players according to COVID-19 status in the pandemic.
Aims
This study aims to compare pulmonary functions and respiratory muscle strength in female players with and without COVID-19.
Methods
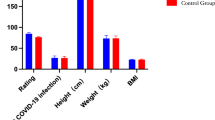
Seventeen players (23.47 ± 5.89 years) who were recovered from COVID-19 and 25 female volleyball players (20.48 ± 5.05 years) who were not infected by SARS-CoV-2 were included in the study. Maximal inspiratory and expiratory pressure, pulmonary functions, body composition, symptom severity, and perceptions of performance were evaluated.
Results
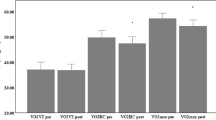
Measured and predicted percent maximal inspiratory pressure and measured maximal expiratory pressure values of COVID-19 players were statistically significantly lower than non-COVID-19 players (p < 0.05). Dynamic lung volumes were similar in groups (p > 0.05).
Conclusions
Inspiratory and expiratory muscle strength in COVID-19 players were more affected compared with non-COVID-19 players. Pulmonary functions were mostly preserved in COVID-19 players. Respiratory muscle weakening can affect the performance of female players. Therefore, respiratory muscle strength training could be suggested in female players with COVID-19 to increase respiratory muscle strength and prevent deterioration in performance.
Trial registration (ClinicalTrials.gov)
Registration ID: NCT04789512.
Similar content being viewed by others
Introduction
In 2019, a new Coronavirus disease (COVID-19), caused by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) or (2019-nCoV), firstly emerged in China and spread quickly around the world. World Health Organization declared COVID-19 as a pandemic on March 2020 [1]. The governments have taken comprehensive isolation and quarantine measures to prevent increasing cases [2]. All sports competitions and training sessions are postponed or canceled. The quarantine measures also affected the athletes, coaches, and sports federations [3]. On the other hand, negative consequences of isolation and quarantine and symptoms related to COVID-19 have affected the physical fitness and performance of athletes [3]. Cytokine storm is associated with abnormalities in inflammatory cytokines; consistently increased systemic inflammation, physiological damage, and high mortality rate have been seen in critical patients with COVID-19 [4]. Although cytokine storm is seen in critical diseases, increased inflammatory cytokines in athletes can affect the performance of the athletes [5]. Furthermore, COVID-19 has been expressed both in acute pulmonary symptoms such as cough and dyspnea and severe pneumonia, and procoagulant condition activated by systemic inflammation resulting in deep vein thrombosis and even pulmonary embolism [6]. Lung infection related to COVID-19 causing impaired pulmonary function progresses in three stages: an early infection stage including viral replication and mild symptoms, a pulmonary stage defined as excitation of adaptive immunity and occurrence of respiratory dysfunction accompanying lung injury and hypoxemia, and finally, hyperinflammation stage associated with severe disease [7]. Although many athletes are predicted to have mild and moderate symptoms related to COVID-19, most athletes have experienced cough and dyspnea during vigorous activity. Normally, respiratory events like allergy, exercise-induced anaphylaxis, bronchoconstriction, pulmonary edema, and respiratory tract infection, pneumothorax, and symptoms such as cough, dyspnea, sputum, and wheeze are fairly common in athletes [8]. COVID-19 can aggravate the aforementioned events and asthma-like symptoms. Therefore, respiratory evaluation is important in athletes to prevent short- and long-term post-COVID pulmonary symptoms and complications [9]. In the literature, not much data is evaluating respiratory functions in volleyball players during the COVID-19 pandemic. The aim of this study is to evaluate and compare pulmonary functions and respiratory muscle strength of female volleyball players who had been diagnosed with and without COVID-19. For this aim, we tested the hypothesis that female COVID-19 players may have worse respiratory functions, muscle strength, and performance situations compared to female players without COVID-19.
Methods
Study design and participants
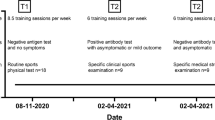
This is a prospective, cross-sectional study. Volleyball players who suffered COVID-19 were named COVID-19 players and non-suffered as non-COVID-19 players. In total, 17 COVID-19 (23.47 ± 5.89 years) and 25 non-COVID-19 (20.48 ± 5.05 years) female volleyball players who came to the clinic for routine control were included in the study. Inclusion criteria include those who had 3 months after the polymerase chain reaction (PCR) test turned negative and were willing to participate in the study. Exclusion criteria include those with a history of chronic lung disease and those who are unwilling to participate in the study. The study was approved (No: 2021–189/16.02.2021) by Gazi University Ethics Committee and conducted following the Declaration of Helsinki. The informed consent form was obtained from all players. All players had a similar training program and were evaluated in the same time frame. The primary outcome was respiratory muscle strength, and secondary outcomes were pulmonary functions and body composition. Pre-pandemic and pandemic training frequency and performance perceptions of athletes, total sleeping time, COVID-19 symptoms and symptom perceptions, smoking exposure, pandemic injury, and whether players were hospitalized or not were recorded.
Pulmonary functions
Pulmonary function test was evaluated using a portable spirometer (MIR Spirodoc, Medical International Research, Rome, Italy) according to the criteria of American Thoracic Society/European Respiratory Society [10]. Forced expiratory volume in the first second (FEV1), forced vital capacity (FVC), forced expiratory volume in the first second/forced vital capacity (FEV1/FVC), peak expiratory flow (PEF), and forced expiratory flow from 25 to 75% (FEF25–75%) were measured and repeated to maximum 8 times until the test was successful. The highest values were selected for analysis and calculated as percentages of predicted values [10, 11]. Percentages of predicted values < 75% for FEV1/FVC and < 80 for other lung volume parameters were indicated as abnormal [12].
Respiratory muscle strength
Inspiratory and expiratory muscle strengths were evaluated using a mouth pressure device (Micro Medical MicroRM, UK) according to the guidelines of American Thoracic Society/European Respiratory Society. The measurements were performed in sitting position. The maximal inspiratory (MIP) and expiratory pressure (MEP) were measured by maximal inspiration at residual volume and maximal expiration from total lung capacity, respectively. [13]. The best MIP and MEP values were selected from three to five trials and expressed as a percentage of the predicted values [14]. Data < 80% of expected values were stated as abnormal [15].
Anthropometric parameters and body composition
Anthropometric parameters including height (m) and body mass (kg) were assessed in volleyball players. Body composition was evaluated using TANITA bioelectrical impedance analysis (BC418-MA, TANITA Corporation, Tokyo, Japan). Fat mass, fat mass percent, fat-free mass, body mass index, and predicted muscle mass were measured and interpreted according to age-gender–adjusted reference values [16].
Perceptions of symptom severity and performance
Perceptions of symptom severity of COVID-19 players and performance of all players were evaluated using the Numeric Rating Scale (NRS). The severity of COVID-19 symptoms is scored 0–10 point. Higher scores indicated higher severity of symptoms. Perceptions of performance of all players were also scored 0–10 points. Higher scores indicated greater performance [17].
Statistical analysis
In this study, a total of 42 participants were included and calculated, based on the pilot results of this study using the maximal inspiratory pressure values for 80% power and α value of 0.05 (G*Power 3.0.10 system, Franz Faul, Universität Kiel, Germany) [18]. The analyses were performed using the Windows-based SPSS 20 statistical analysis program. Shapiro–Wilk test was used to determine whether the data is a normal distribution. To indicate the descriptive analysis of the normal distribution, variables were used to mean the differences, 95% confidence interval (95% CI), means (X), and standard deviation. Descriptive analyses of non-normally distributed variables were indicated median and interquartile range (IQR) values. Categorical variables were stated percentage (%) and frequency (n). Normally distributed variables were compared using the Student t-test, non-normally distributed, and categorical values using Mann–Whitney U and chi-square test. The level of significance was defined as p < 0.05.
Results
Seventeen (17) COVID-19 players and 25 non-COVID-19 players were analyzed in this study. Demographic and clinical characteristics were similar in volleyball players with COVID-19 and non-COVID-19 (Table 1). None of the COVID-19 players had hospitalization due to SARS-CoV-2 infection. Performance perceptions of COVID-19 players tended to decrease, while performance perceptions of non-COVID-19 players tended to increase during pandemic. However, performance perceptions of groups were similar (Table 1; p > 0.05). Time to return to sports after COVID-19 was 14.06 ± 3.37 days in COVID-19 players. Total sleeping times were similar in groups. The mean smoking exposure of non-COVID-19 players was less than 10 pack*years. COVID-19 symptoms severity perceptions of 11 (65%) COVID-19 players were above 5 points in the acute period. The most common COVID-19 symptoms were taste and smell loss (82.4%), fever (52.9%), and myalgia (52.9%). Almost half of the COVID-19 players experienced cough (47.1%) and dyspnea (41.2%) symptoms (Table 2). Measured and predicted percent MIP [(1 − β) = 78%], and measured MEP values of COVID-19 players were statistically significantly lower than non-COVID-19 players (Table 3, p < 0.05). MIP values of 8 (47.1%) players with COVID-19 were below 80% of predicted values. MIP values of all players with non-COVID-19 were higher than 80% of the predicted values. MEP values of 16 (94.1%) players with COVID-19 and 21 (84%) players with non-COVID-19 were lower than 80% of predicted values. However, predicted MEP and dynamic lung volumes including FEV1, FVC, FEV1/FVC, PEF, and FEF25-75% values were similar in groups (Table 3, p > 0.05). One (5.9%), 4 (23.5%), and 1 (5.9%) players suffered from COVID-19 had FVC, FEV1, FEV1/FVC less than 80% of predicted values, respectively.
Discussion
This study firstly provides information about the respiratory muscle strength and pulmonary functions in volleyball players who suffered from COVID-19 compared with non-COVID-19 players. The most striking findings of our study are that inspiratory and expiratory muscle strength is impaired in volleyball players with COVID-19 compared with non-COVID-19 players although pulmonary functions are in normal ranges except for PEF values of players with COVID-19.
Lungs are the most affected organ by COVID-19, and as a result, many pathologies such as diffuse alveolar epithelium destruction, capillary damage, hyaline membrane formation, alveolar septal fibrous proliferation, and pulmonary consolidation occur [12]. These impairments cause worsening respiratory muscle strength and lung functions [15]. Although it is stated that COVID-19 have not caused serious symptoms in young athletes, the long-term effects on respiratory parameters are unclear in these populations [5]. The mean MIP and MEP values of volleyball players with COVID-19 in our study were lower than normal healthy females predicted values [14]. Furthermore, although none of the players had ongoing post-COVID symptoms such as dyspnea and cough, and they were evaluated in the chronic period after COVID-19 infection, inspiratory (47.1%) and expiratory (94.1%) muscle-weakening were considerably higher in COVID-19 players compared with non-COVID-19 players (0–84%). Unfortunately, there is no other study that can compare the respiratory muscle strength value of female volleyball players suffered from COVID-19 in the pandemic period. Though it is not possible to completely compare our results and the data of Ohya et al.’s study [19] conducted in the pre-pandemic period, the mean MIP values (103.9 ± 24.6 cmH2O) of elite female athletes who played in different sports branches were higher compared to the results of volleyball players in our study carried out in the pandemic period. In addition, they found that MIP value is higher in sports branches that cause more inspiratory muscle fatigue [19]. Respiratory muscle strength is correlated to many factors such as inspiratory muscle fatigue [19], skeletal muscle mass index, and peripheral muscle strength [20]. In our study, weakened respiratory muscle strength in COVID-19 players can be associated with COVID-19 infection, lung, and diaphragmatic pathologies triggered by COVID-19 along with the factors mentioned above. Respiratory muscle-weakening negatively affects the performance in athletes [21], while inspiratory muscle training advances performance in athletes [22]. In addition, inspiratory muscle training increases peak inspiratory pressures and ventilatory capacity [23] and reduces dyspnea [24]. Therefore, inspiratory muscle training can be effective to increase respiratory muscle strength and develop the performance of volleyball players with COVID-19.
The COVID-19 infection could aggravate asthma-like symptoms and airway dysfunctions in players with COVID-19. Some cases have had COVID-19-related pneumonia, chest restriction, increased dyspnea, fatigue, and decreased performance. Therefore, the evaluation of pulmonary functions is important in players who suffered from COVID-19 [9]. Although respiratory muscle strength was impaired, pulmonary functions were preserved in our volleyball players who suffered from COVID-19. The long-term effects of COVID-19 are uncertain [9]; respiratory muscle strength may have been more affected in the early period. There is a need for longitudinal studies evaluating pulmonary functions of athletes in the long term. Busse et al. emphasized that patients may have normal pulmonary function tests even though they have symptoms; therefore, additional diagnostic test is required [25]. Evaluation of diffusion capacity and static lung volumes may be more notable in individuals with COVID-19 [12]. PEF values of players with COVID-19 were minimally below the predicted values. Four players with COVID-19 had obstructive and one had restrictive pulmonary function abnormalities in the current study. In one study evaluating the pulmonary functions of athletes with COVID-19 by Gervasi et al., akin to our study, they found that dynamic lung volume is similar to both COVID-19 and non-COVID-19 players [26]. However, they have shown that it is a significant reduction after the COVID-19 outbreak when compared to the before pandemic era. The types of sport, age, race, and gender can affect respiratory parameters [19, 27]. Pulmonary function results of Gervasi et al. who conducted the study in male soccer players were higher than the results of female volleyball players in our study. The difference of results may be linked to the inclusion of athletes in different sport types, races, and gender in studies. PEF values are related to the strength of expiratory muscles [28]. Reduced PEF values may be associated with impaired expiratory muscle strength in our study. The cause of these decreases in female athletes exposed to COVID-19 needs to be investigated.
Many factors affect performance and respiratory functions in athletes. One of these is body composition and anthropometric variables [29]. In our study, although internal and external factors affecting performance such as training programs, demographic characteristics, body compositions, total sleeping times, and injury frequencies were similar in both groups, the mean perception of the performance of volleyball players suffered from COVID-19 was decreased after COVID-19 infection. The effect of COVID-19 infection on performance and respiratory parameters should be investigated in more detail.
Limitations
Unfortunately, a limitation is the lack of longitudinal data in participants. Pre-COVID-19 data of the players were not available. Therefore, only post-COVID-19 results are given in this study. The other limitation of this study is the inability to objectively evaluate performance of players.
Conclusion
Although players with COVID-19 did not have severe symptoms and were not hospitalized, their respiratory muscle strengths were more affected compared with non-COVID-19 players after 3 months of the infection. Though pulmonary functions were mostly preserved, pulmonary evaluation may be beneficial for players before returning to sports after COVID-19 infection. Respiratory muscle strength training could be suggested to players with a history of COVID-19 to increase respiratory muscle strength and prevent a decrease in performance.
Data availability
The data that support the findings of this study are available on request from the corresponding author.
References
Yuen K-S, Ye Z-W, Fung S-Y et al (2020) SARS-CoV-2 and COVID-19: the most important research questions. Cell Biosci 10:1–5. https://doi.org/10.1186/s13578-020-00404-4
Parmet WE, Sinha MS (2020) Covid-19—the law and limits of quarantine. N Engl J Med 382:e28. https://doi.org/10.1056/NEJMp2004211
Jukic I, Calleja-González J, Cos F et al (2020) Strategies and solutions for team sports athletes in isolation due to COVID-19. Sports 8:56. https://doi.org/10.3390/sports8040056
Mehta P, McAuley DF, Brown M et al (2020) COVID-19: consider cytokine storm syndromes and immunosuppression. Lancet 395:1033–1034. https://doi.org/10.1016/S0140-6736(20)30628-0
Mulcahey MK, Gianakos AL, Mercurio A et al (2021) Sports medicine considerations during the COVID-19 pandemic. Am J Sports Med 49:512–521. https://doi.org/10.1177/0363546520975186
Xiong T-Y, Redwood S, Prendergast B et al (2020) Coronaviruses and the cardiovascular system: acute and long-term implications. Eur Heart J 41:1798–1800. https://doi.org/10.1093/eurheartj/ehaa231
Romagnoli S, Peris A, De Gaudio AR et al (2020) SARS-CoV-2 and COVID-19: from the bench to the bedside. Physiol Rev 100:1455–1466. https://doi.org/10.1152/physrev.00020.2020
Hull JH, Ansley L, Robson-Ansley P et al (2012) Managing respiratory problems in athletes. Clin Med 12:351. https://doi.org/10.7861/clinmedicine.12-4-351
Wilson MG, Hull JH, Rogers J et al (2020) Cardiorespiratory considerations for return-to-play in elite athletes after COVID-19 infection: a practical guide for sport and exercise medicine physicians. Br J Sports Med 54:1157–1161. https://doi.org/10.1136/bjsports-2020-102710
Miller MR, Crapo R, Hankinson J et al (2005) General considerations for lung function testing. Eur Respir J 26:153–161. https://doi.org/10.1183/09031936.05.00034505
Hankinson JL, Odencrantz JR, Fedan KB (1999) Spirometric reference values from a sample of the general US population. Am J Respir Crit Care Med 159:179–187. https://doi.org/10.1164/ajrccm.159.1.9712108
Mo X, Jian W, Su Z et al (2020) Abnormal pulmonary function in COVID-19 patients at time of hospital discharge. Eur Respir J 55:2001217. https://doi.org/10.1183/13993003.01217-2020
European Respiratory Society and American Thoracic Society (2002) ATS/ERS Statement on respiratory muscle testing. Am J Respir Crit Care Med 166:518–624. https://doi.org/10.1164/rccm.166.4.518
Black LF, Hyatt RE (1969) Maximal respiratory pressures: normal values and relationship to age and sex. Am Rev Respir Dis 99:696–702. https://doi.org/10.1164/arrd.1969.99.5.696
Huang Y, Tan C, Wu J et al (2020) Impact of coronavirus disease 2019 on pulmonary function in early convalescence phase. Respir Res 21:1–10. https://doi.org/10.1186/s12931-020-01429-6
Gallagher D, Heymsfield SB, Heo M et al (2000) Healthy percentage body fat ranges: an approach for developing guidelines based on body mass index. The Am J Clin Nutr 72:694–701. https://doi.org/10.1093/ajcn/72.3.694
Farrar JT, Young JP Jr, LaMoreaux L et al (2001) Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain 94:149–158. https://doi.org/10.1016/S0304-3959(01)00349-9
Faul F, Erdfelder E, Lang A-G et al (2007) G* Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods 39:175–191. https://doi.org/10.3758/bf03193146
Ohya T, Hagiwara M, Chino K et al (2017) Maximal inspiratory mouth pressure in Japanese elite female athletes. Respir Physiol Neurobiol 238:55–58. https://doi.org/10.1016/j.resp.2017.01.005
Sawaya Y, Ishizaka M, Kubo A et al (2018) Correlation between skeletal muscle mass index and parameters of respiratory function and muscle strength in young healthy adults according to gender. J Phys Ther Sci 30:1424–1427. https://doi.org/10.1589/jpts.30.1424
Jurić I, Labor S, Plavec D et al (2019) Inspiratory muscle strength affects anaerobic endurance in professional athletes. Arh Hig Rada Toksikol 70:42–48. https://doi.org/10.2478/aiht-2019-70-3182
Silva RLC, Hall E, Maior AS (2019) Inspiratory muscle training improves performance of a repeated sprints ability test in professional soccer players. J Bodyw Move Ther 23:452–455. https://doi.org/10.1016/j.jbmt.2019.01.016
Sheel AW (2002) Respiratory muscle training in healthy individuals. Sports Med 32:567–581. https://doi.org/10.2165/00007256-200232090-00003
Ramsook AH, Molgat-Seon Y, Schaeffer MR et al (2017) Effects of inspiratory muscle training on respiratory muscle electromyography and dyspnea during exercise in healthy men. J Appl Physiol 122:1267–1275. https://doi.org/10.1152/japplphysiol.00046.2017
Busse WW (2012) What is the best pulmonary diagnostic approach for wheezing patients with normal spirometry? Respir Care 57:39–49. https://doi.org/10.4187/respcare.01449
Gervasi SF, Pengue L, Damato L et al (2021) Is extensive cardiopulmonary screening useful in athletes with previous asymptomatic or mild SARS-CoV-2 infection? Br J Sports Med 55:54–61. https://doi.org/10.1136/bjsports-2020-102789
Mazic S, Lazovic B, Djelic M et al (2015) Respiratory parameters in elite athletes–does sport have an influence? Rev Port Pneumol 21:192–197. https://doi.org/10.1016/j.rppnen.2014.12.003
Miller MR, Hankinson J, Brusasco V et al (2005) Standardisation of spirometry. Eur Respir J 26:319–338. https://doi.org/10.1183/09031936.05.00034805
Leone M, Lariviere G, Comtois AS (2002) Discriminant analysis of anthropometric and biomotor variables among elite adolescent female athletes in four sports. J Sports Sci 20:443–449. https://doi.org/10.1080/02640410252925116
Acknowledgements
The authors would like to thank Gazi University Academic Writing Research and Application Centre for English editing their contribution and support.
Funding
This study is supported by the Gazi University Scientific Research Projects Coordination Unit under grant number: 2021-7080.
Author information
Authors and Affiliations
Contributions
Z.C: conceptualization, methodology, data curation, writing-original draft preparation, visualization, investigation; N.A.G: conceptualization, methodology, visualization, investigation, supervision, reviewing and editing; N. Ka. and N. Ko.: visualization, investigation, supervision, reviewing and editing.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration. A cross-sectional study was approved (No: 2021–189/16.02.2021) by Gazi University Ethics Committee and performed following the Declaration of Helsinki. A clinical trial number was obtained (NCT04789512). All participants approved the informed consent form before the study. Data collection was applied after the informed consent form was signed.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Çelik, Z., Güzel, N.A., Kafa, N. et al. Respiratory muscle strength in volleyball players suffered from COVID-19. Ir J Med Sci 191, 1959–1965 (2022). https://doi.org/10.1007/s11845-021-02849-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11845-021-02849-z