
Abstract
Background
Bariatric surgery predisposes patients to cholelithiasis and therefore the need of a subsequent cholecystectomy; however, the incidence of cholecystectomy after bariatric surgery is debated.
Aim and Methods
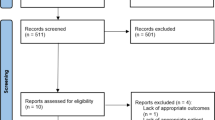
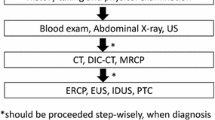
Medical records of 601patients hospitalized for bariatric surgery between January 2010 and July 2018 were reviewed. Our aim was to evaluate the incidence of cholecystectomy following different types of common bariatric procedures. All patients who developed cholelithiasis and a subsequent cholecystectomy were included. Cholelithiasis was diagnosed by clinical criteria and characteristic ultrasound findings.
Results
We retrospectively evaluated 580 patients with an average follow-up of 12 months (range 6–24 months). Twenty-one patients were excluded because of missing data. Mean age was 48 ± 19 years (78% females). Twenty-nine patients (5%) underwent laparoscopic cholecystectomy (LC) before the bariatric surgery, and 58 patients (10%) performed concomitant LC with the bariatric procedure due to symptomatic gallstone disease (including stones, sludge, and polyps). There were 203 laparoscopic sleeve gastrectomy (SG) (35%), 175 laparoscopic gastric band (LAGB) (30%), 55 Roux-en-Y gastric bypass (RYGB) (9.5%), and 147 (25%) mini gastric bypass (MGB) procedures during the study period. At the follow-up period, 36 patients (6.2%) developed symptomatic cholelithiasis, while the most common clinical presentation was biliary colic. There was a significant difference between the type of the bariatric procedure and the incidence of symptomatic cholelithiasis after the operation. The incidence of symptomatic gallstone formation in patients who underwent RYGB was 14.5%. This was significantly higher comparing to 4.4% following SG, 4.1% following LAGB, and 7.5% following MGB (p = 0.04). We did not find any predictive risk factors including smoking; BMI at surgery; change in BMI; comorbidities such as diabetes, hyperlipidemia, hypertension, and COPD for gallstone formation; or a subsequent cholecystectomy. Interestingly we found that previous bariatric surgery was a risk factor for gallstone formation and cholecystectomy, 13/82 patients (15.8%) compared to 23/492 patients (4.6%) among those without previous bariatric operation (p < 0.001)].
Conclusion
Our data demonstrate that patients with previous bariatric surgery or patients planned for RYGB are at high risk to develop postoperative symptomatic gallbladder disease. Concomitant cholecystectomy during the bariatric procedure or alternatively UDCA treatment for at least for 6 months to avoid the high incidence of postoperative symptomatic gallstones should be considered in those asymptomatic patients.
Similar content being viewed by others

References
The National Registry of Bariatric Surgery, The Israel Center for Disease Control, Ministry of Health, State of Israel, 2016.
Coupaye M, Calabrese D, Sami O, et al. Evaluation of incidence of cholelithiasis after bariatric surgery in subjects treated or not treated with ursodeoxycholic acid. Surg Obes Relat Dis. 2017;13(4):681–5. https://doi.org/10.1016/j.soard.2016.11.022.
Guzmán HM, Sepúlveda M, Rosso N, et al. Incidence and risk factors for cholelithiasis after bariatric surgery. Obes Surg. 2019;29(7):2110–4. https://doi.org/10.1007/s11695-019-03760-4.
Altieri MS, Yang J, Nie L, et al. Incidence of cholecystectomy after bariatric surgery. Surg Obes Relat Dis. 2018;14(7):992–6. https://doi.org/10.1016/j.soard.2018.03.028.
Li VK, Pulido N, Fajnwaks P, et al. Predictors of gallstone formation after bariatric surgery: a multivariate analysis of risk factors comparing gastric bypass, gastric banding, and sleeve gastrectomy. Surg Endosc. 2009;23(7):1640–4. https://doi.org/10.1007/s00464-008-0204-6.
Moon RC, Teixeira AF, DuCoin C, et al. Comparison of cholecystectomy cases after Roux-en-Y gastric bypass, sleeve gastrectomy, and gastric banding. Surg Obes Relat Dis. 2014;10(1):64–8. https://doi.org/10.1016/j.soard.2013.04.019.
Melmer A, Sturm W, Kuhnert B, et al. Incidence of gallstone formation and cholecystectomy 10 years after bariatric surgery. Obes Surg. 2015;25(7):1171–6. https://doi.org/10.1007/s11695-014-1529-y.
Yardimci S, Coskun M, Demircioglu S, et al. Is concomitant cholecystectomy necessary for asymptomatic cholelithiasis during laparoscopic sleeve gastrectomy? Obes Surg. 2018;28(2):469–73.3.
Dakour Aridi H, Sultanem S, Abtar H, et al. Management of gallbladder disease after sleeve gastrectomy in a selected Lebanese population. Surg Obes Relat Dis. 2016;12(7):1300–4.
Hasan MY, Lomanto D, Loh LL, et al. Gallstone disease after laparoscopic sleeve gastrectomy in an Asian population-what proportion of gallstones actually becomes symptomatic? Obes Surg. 2017;27(9):2419–23.3–5.
Karadeniz M, Gorgun M, Kara C. The evaluation of gallstone formation in patients undergoing Roux-en-Y gastric bypass due to morbid obesity. Ulus Cerrahi Derg. 2014;30(2):76–9.
Pineda O, Maydon HG, Amado M, et al. A prospective study of the conservative management of asymptomatic preoperative and postoperative gallbladder disease in bariatric surgery. Obes Surg. 2017;27(1):148–53. 6–9
Nougou A, Suter M. Almost routine prophylactic cholecystectomy during laparoscopic gastric bypass is safe. Obes Surg. 2008;18(5):535–9.
Amstutz S, Michel JM, Kopp S, et al. Potential benefits of prophylactic cholecystectomy in patients undergoing bariatric bypass surgery. Obes Surg. 2015;25(11):2054–60.
Weiss AC, Inui T, Parina R, et al. Concomitant cholecystectomy should be routinely performed with laparoscopic Roux-en-Y gastric bypass. Surg Endosc. 2015;29(11):3106–11.
Chen JH, Tsai MS, Chen CY, et al. Bariatric surgery did not increase the risk of gallstone disease in obese patients: a comprehensive cohort study. Obes Surg. 2019;29(2):464–73. https://doi.org/10.1007/s11695-018-3532-1.
Magouliotis DE, Tasiopoulou VS, Svokos AA, et al. Ursodeoxycholic acid in the prevention of gallstone formation after bariatric surgery: an updated systematic review and meta-analysis. Obes Surg. 2017;27(11):3021–30. https://doi.org/10.1007/s11695-017-2924-y.
Della Penna A, Lange J, Hilbert J, et al. Ursodeoxycholic acid for 6 months after bariatric surgery is impacting gallstone associated morbidity in patients with preoperative asymptomatic gallstones. Acta Cir Bras. 2019;34(1):e20190010000009. https://doi.org/10.1590/s0102-865020190010000009.
Machado FHF, Castro Filho HF, Babadopulos RFAL, et al. Ursodeoxycholic acid in the prevention of gallstones in patients subjected to Roux-en-Y gastric bypass1. Obes Surg. 2019;29(4):1216–21. https://doi.org/10.1007/s11695-018-03651-0.
Attili AF, Carulli N, Roda E, et al. Epidemiology of gallstone disease in Italy: prevalence data of the multicenter Italian study on cholelithiasis (M.I.COL.). Am J Epidemiol. 1995;141(2):158–65.
LJ Jr W, Wright JK, Debelak JP, et al. Prevention of gallstone formation in morbidly obese patients undergoing rapid weight loss: results of randomized controlled pilot study. J Surg Res. 2002;102(1):50–6.
Coupaye M, Castel B, Sami O, et al. Comparison of the incidence of cholelithiasis after sleeve gastrectomy and Roux-en-Y gastric bypass in obese patients: a prospective study. Surg Obes Relat Dis. 2015;11(4):779–84. https://doi.org/10.1016/j.soard.2014.10.015.
D’Hondt M, Sergeant G, Deylgat B, et al. Prophylactic cholecystectomy, a mandatory step in morbidly obese patients undergoing laparoscopic Roux-en-Y gastric bypass? J Gastrointest Surg. 2011;15:1532–6.
Ettleson MD, Lager CJ, Kraftson AT, et al. Roux-en-Y gastric bypass versus sleeve gastrectomy: risks and benefits. Minerva Chir. 2017;72(6):505–19. https://doi.org/10.23736/S0026-4733.17.07441-7.
Lee JH, Nguyen QN, Le QA. Comparative effectiveness of 3 bariatric surgery procedures: Roux-en-Y gastric bypass, laparoscopic adjustable gastric band, and sleeve gastrectomy. Surg Obes Relat Dis. 2016;12(5):997–1002. https://doi.org/10.1016/j.soard.2016.01.020.
Bettencourt-Silva R, Neves JS, Pedro J, et al. Freitas P; AMTCO group, Carvalho D. Comparative effectiveness of different bariatric procedures in super morbid obesity. Obes Surg. 2019;29(1):281–91. https://doi.org/10.1007/s11695-018-3519-y.
Manatsathit W, Leelasinjaroen P, Al-Hamid H, et al. The incidence of cholelithiasis after sleeve gastrectomy and its association with weight loss: a two-centre retrospective cohort study. Int J Surg. 2016;30:13–8. https://doi.org/10.1016/j.ijsu.2016.03.060.
Aridi HD, Sultanem S, Abtar H, et al. Management of gallbladder disease after sleeve gastrectomy in a selected Lebanese population. Surg Obes Relat Dis. 2016;12:1300–4.
Tustumi F, Bernardo WM, Santo MA, et al. Cholecystectomy in patients submitted to bariatric procedure: a systematic review and meta-analysis. Obes Surg. 2018;28(10):3312–20. https://doi.org/10.1007/s11695-018-3443-1.
Warschkow R, Tarantino I, Ukegjini K, et al. Concomitant cholecystectomy during laparoscopic Roux-en-Y gastric bypass in obese patients is not justified: a meta-analysis. Obes Surg. 2013;23(3):397–407. https://doi.org/10.1007/s11695-012-0852-4.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Sneineh, M.A., Harel, L., Elnasasra, A. et al. Increased Incidence of Symptomatic Cholelithiasis After Bariatric Roux-En-Y Gastric Bypass and Previous Bariatric Surgery: a Single Center Experience. OBES SURG 30, 846–850 (2020). https://doi.org/10.1007/s11695-019-04366-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-019-04366-6