
Abstract
Over the past decades, virtual reality (VR) has found its way into biofeedback (BF) therapy programs. Using VR promises to overcome challenges encountered in traditional BF such as low treatment motivation, low attentional focus and the difficulty of transferring learnt abilities to everyday life. Yet, a comprehensive research synthesis is still missing. Hence, this scoping review aims to provide an overview over empirical studies on VR based BF regarding key outcomes, included samples, used soft- and hardware, BF parameters, mode of application and potential limitations. We systematically searched Medline, PsycINFO, Scopus, CINAHL, Google Scholar and Open Grey for empirical research. Eighteen articles met the inclusion criteria. Samples mostly consisted of healthy (44.4%) and/or adult (77.7%) participants. Outcomes were mainly anxiety (44.4%), stress (44.4%) or pain reduction (11.1%), which were reduced by the VR-BF interventions at least as much as by classical BF. Participants in VR-BF interventions showed higher motivation and involvement as well as a better user experience. Heart rate or heart rate variability were the most frequently used BF parameters (50.0%), and most VR-BF interventions (72.2%) employed a natural environment (e.g., island). Currently, there is no clear evidence that VR-BF is more effective than traditional BF. Yet, results indicate that VR-BF may have advantages regarding motivation, user experience, involvement and attentional focus. Further research is needed to assess the specific impact of VR and gamification. Also, testing a broader range of clinical and younger samples would allow more far-reaching conclusions.
Similar content being viewed by others


Introduction
Biofeedback (BF) may be defined as a process which enables individuals to intentionally alter their physiological activity (Schwartz, 2010). Precise instruments measure physiological signals (e.g., heart rate, breathing, muscle tone, or skin temperature) and simultaneously feed this information back to the individual via visual or auditory channels. Ultimately, the individual learns to become independent of the external feedback and progressively experiences control relying solely on internal feedback (Gaume et al., 2016). Areas of application for BF include the improvement of athletic, cognitive, or artistic performance (see Lehrer et al., 2020) and the treatment of a range of health conditions like chronic headache (Nestoriuc et al., 2008), pain (Sielski et al., 2017), high blood pressure (Nakao et al., 2003), or psychiatric disorders (Schoenberg & David, 2014) like anxiety disorders (Tolin et al., 2020) and depression (Walker & Lawson, 2013). Furthermore, BF may be used as a tool for managing stress and anxiety (Goessl et al., 2017).
Although extant data generally supports the use of BF for certain indications, there are several indications which may impact learning and outcome. For instance, it has repeatedly been criticized that visual representations of physiological signals are too abstract, too complex, or not meaningful enough to the user (Blum et al., 2019; Yu et al., 2018). Similarly, the task content has frequently been labelled as “extremely boring” (Gaume et al., 2016, p. 907), and has been found to lack the ability to sufficiently engage the user’s attention (Blum et al., 2019).
According to the psychoengineering model by Gaume et al. (2016) the following five key mechanisms shape BF learning: perceptibility, autonomy, mastery, learnability, and motivation. Particularly with regards to motivation, the authors see considerable need for improvement. It has been shown that extrinsic feedback (e.g., scores, money) facilitates the learning process. Hence, keeping the patient sufficiently motivated and installing adequate reward systems are among the main challenges to training success (see also Schwartz, 1973). In sum, participants must take an active role and continue practicing in order to develop a desired skill (Frank et al., 2010). Apart from motivation, sufficiently engaging and keeping up the users’ attention during the task may be regarded another key factor in the success of BF (Blum et al., 2019). Learning to self-regulate requires the user to keep a sustained attentional focus on the feedback signal. Yet, unappealing task content and distractions from the (laboratory) surroundings, as well as disrupting thoughts may all hinder the user to continuously focus on the task at hand. Another issue lies in the predictive validity of BF tasks (Gaume et al., 2016). The main goal of BF is that users increasingly acquire autonomy in the sense that they learn to rely on their internal feedback. These newly learnt skills then need to generalize from the abstract BF training to the more complex and challenging realm of everyday life. Yet again, abstract stimuli and a rather sterile training environment may make this generalization difficult.
Virtual Reality and Gamification
Embedding BF in a virtual reality (VR) environment may constitute a viable solution to the above-mentioned challenges. Virtual reality is defined as an advanced human–computer interface that simulates a realistic virtual environment (VE) and allows participants to interact with it (Latta & Oberg, 1994). Using interactive elements and multisensory stimulation, VR manages to induce considerable levels of excitement and involvement (Maarsingh et al., 2019).
Additionally, VR facilitates the integration of gamification elements such as progression systems, story lines, or incentives (Deterding et al., 2011). Gamification approaches have experienced a rapid adoption in different scientific disciplines like education, health or work (Hamari et al., 2014). So called serious games combine gamification with educational or therapeutic purposes (Connolly et al., 2012) and have repeatedly been found to be effective in improving motivation (Domínguez et al., 2013; Sailer, 2016). Hence, using gamification mechanics in connection with BF promises to overcome the challenge of low motivational engagement. This may especially be true for children and adolescents. Past findings (see the meta-analysis of Fadhli et al., 2020) indicate that gamification can successfully be used to effectively engage younger generations in learning.
Furthermore, the use of immersive VR technology such as head-mounted-displays (HMDs), which cover the users’ full field of view (Slater & Wilbur, 1997), may promote sustained attention. Prior research has suggested that particularly immersive and interactive VEs which depict a nature environment like a beach, or a mountain scenery are effective in terms of stress reduction and relaxation (e.g., Annerstedt et al., 2013; Liszio et al., 2018). Virtual nature environments may be particularly suitable for BF applications as they can “replenish attentional resources in a comforting and relaxing way and provide plenty of opportunities for immersive and meaningful feedback elements” (Blum et al., 2019, p. 3). In their complexity and interactivity, VEs may furthermore improve the generalization of learnt skills to real-world settings. Generally, VEs are regarded as more ecologically valid than abstract tasks presented via 2D-screens (see Kothgassner & Felnhofer, 2020). Even when depicting phantasy worlds (e.g., underwater surroundings), VEs provide complex, contextually rich scenarios whose sensory vividness approximates that of everyday environments; also, the dynamic engagement of the sensorimotor system provokes more naturalistic behavioral and physiological responses than abstract stimuli (Bohil et al., 2011). According to this, the generalization to everyday life is expected to be easier with VR-BF than with traditional BF (Pallavicini et al., 2009).
In light of these advantages, it is not surprising that VR has found its way into the field of BF. However, VR based BF protocol are still rather new, and although the body of literature continues to grow, there is, to date, no research synthesis on VR-BF. Hence, we set out to conduct a scoping review to map out this emerging field with regards to the extent, range, and nature of existing literature to guide the planning and commissioning of future studies. In particular, we were interested in identifying key characteristics of existing studies such as included samples, design, types of physiological signals used, task content, type of VR equipment (hard- and software), mode of application (e.g., free body movements), and key outcomes (e.g., health, usability, motivation), as well as potential limitations (e.g., cybersickness).
Methods
Since this research is rather young and heterogeneous, we chose the method of a scoping review to stake out the field (Arksey & O'Malley, 2005). Scoping reviews aim to provide an orientation over an ambiguous and heterogeneous field of research which is conceptually and methodologically too broad for a systematic review; another goal of scoping reviews is to create a knowledge synthesis of the main concepts and theories of a given field and map out open research questions (Tricco et al., 2018). Their objectives typically encompass summarizing research findings and identifying research gaps to derive recommendations for future studies (Peters et al., 2015). In our approach, we adhered to the methods proposed by Arksey and O'Malley (2005), and Levac et al. (2010); also, we closely followed the PRISMA-ScR Guidelines formulated by Tricco et al. (2018).
Inclusion and Exclusion Criteria
We included studies in English and German from the beginning of database records until June 2021. Studies were eligible for inclusion if they evaluated a VR-BF treatment in at least one experimental group. We therefore limited our search to empirical research and excluded theoretical research like conceptual works. Furthermore, we excluded research that was solely qualitative, and reported no quantitative analyses. We searched peer reviewed and grey literature, and no limit was imposed on age groups. Our search exclusively focused on BF methods using peripheral psychophysiological parameters (i.e., heart rate (HR), heart rate variability (HRV), electrodermal activity (EDA), and breathing). Neurofeedback as well as proprioceptive and motor feedback interventions were excluded from the current scoping review for the sake of more stringency in content. In accordance with the VR definition of Riva (2003), we focused on studies utilizing immersive HMDs instead of flat screen or room-based systems.
Search Strategy
We searched the databases Medline, PsycINFO (OVID), Scopus, CINAHL, Google Scholar and Open Grey for fitting literature. Additionally, Google Scholar alerts were enabled to ensure inclusion of articles in press. Search terms were selected to target papers addressing the intersection between BF (biofeedback, biofeedback training) and VR (virtual reality, vr, virtual environment, computer simulation). A detailed list of search strings is available as a supplement (Appendix Table A).
Study Selection and Data Extraction
We de-duplicated the retrieved records using Zotero v5.0.87. We then individually reviewed the titles and abstracts and removed those which did not fit the inclusion criteria. One author (R.L.) independently reviewed all remaining full texts to establish eligibility. Whenever he was unsure, consensus with the second author (A.F.) was sought. The reference lists of chosen full texts were searched manually to find studies which had not been identified in the database research. To ‘chart’ the data, we built a form that we tested on articles we had retrieved in an earlier prescreening. Charting is a technique “for synthesizing and interpreting qualitative data by sifting, categorizing, and sorting material according to key issues and themes” (Arksey & O’Malley, 2005, p. 15). Following this technique, we charted key information and quantitative data in the full texts. We used Microsoft Excel to design a data charting form based on the variables relevant with regards to the scope of the review.
Results
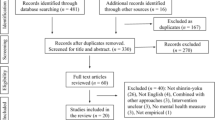
Our initial search yielded 1028 articles. After removing duplicates and papers not fitting the inclusion criteria, n = 18 studies with 865 subjects (54.54% female; of those studies which reported gender) were included in this review (Table 1). For the detailed selection process, see Fig. 1. Most studies (n = 13) were published between 2016 and 2021. Studies originated from different countries, yet most studies could be related to either Germany (n = 5), the Netherlands (n = 5) or Italy (n = 4). Studies either reported randomized controlled trials (RCTs, n = 9) or a pre-post-design (n = 9). For the studies’ place of origin, objectives, design, used methods, measures and outcomes see Table 1.

PRISMA flowchart of screening, exclusion, and inclusion criteria
Participants’ Characteristics
Overall, n = 14 studies used adult samples (> 18 years), only n = 2 studies were conducted among underage participants, and two (Hendriks & Rombout, 2018; Tu et al., 2020) did not report age. The mean age across all studies was M = 31.23 years, with the youngest sample being M = 10.1 years (Van Rooij et al., 2016) and the oldest sample being M = 68.0 years old (Prabhu et al., 2019). Most participants were healthy (n = 9 studies), followed by persons with general anxiety disorder (GAD) in n = 3 studies.
VR technology and Implementation of Feedback
Most studies (n = 14) used virtual nature environments such as islands (n = 8), forests (n = 3), underwater worlds (n = 2), or a hilly landscape (n = 1). Also, the majority (n = 12) employed modern 100-to-110-degree diagonal field-of-view (FoV) HMD solutions, including the Oculus Rift or HTC Vive, while n = 4 studies used older HMDs like the VUZIX iWear, which are only capable of delivering a 30-to-40-degree FoV. One study reported the use of the smartphone-based HMD setup Google Daydream View (90 degree) and one used the Deepstream stereoscopic viewer (85 degree), a VR solution mounted on a mechanic arm instead of the participant’s head in order to free it from additional weight. Most studies (n = 15) were either single task exercises or a sequence of narratively unconnected tasks (e.g., calming down to lighten up a fire). Only n = 3 studies used a narrative logically connecting different exercises with each other, and only one embedded them into a larger storyline. All applications presented their feedback primarily visually; participants had to alter their physiological state in order to affect campfires, lamps, waterfalls or waves (n = 5), to change the weather (n = 6), or the color palette of the environment (n = 4), or to eliminate obstacles in the way (n = 2). Some used correctly performed BF as vehicle of movement through the VR (n = 3), and some presented just an animation like a flattening curve, a scale changing circle or a lung (n = 3). Only n = 2 studies also reported using audio output, and only one of them additionally changed the soundscape based on the physiological state. Eight studies used HR (n = 4) or HRV (n = 3) as the main BF parameter, followed by breathing (n = 5), and electrodermal activity (n = 2).
Primary and Secondary Outcomes
A considerable number of studies (n = 8) targeted anxiety or GAD as primary outcomes. The authors consistently reported a significant anxiety-reducing effect of VR-BF compared to baseline. Stress reduction was evaluated in n = 6 studies; of those, five reported a significant effect compared to base level, and one found no treatment-specific differences in subjective stress or physiological arousal compared to controls (BF on a computer screen, and VR without BF). Furthermore, n = 3 reported a decrease in pain when compared to baseline or to treatment as usual (TAU) without VR or BF. Other findings regarding primary outcomes were a significantly improved quality of life (n = 1) and coping skills (n = 1), a non-significant reduction in disruptive classroom behavior (n = 1), and no changes in self-reported and physiological arousal compared to placebo (n = 1), as well as in positive/negative affect compared to baseline (n = 1).
Regarding secondary outcomes, n = 13 studies focused on user experience or involvement. Findings showed a higher sense of presence (n = 1), a significantly better training experience such as relaxed and stable respiration and sustained attention (n = 2), and higher motivation to use VR-BF (n = 1) in the experimental groups than in classical BF settings carried out on a desktop PC. Furthermore, an increased attentional focus on the present moment and less incidents of mind wandering (n = 1), and higher levels of flow (n = 1) were found when compared to traditional BF. Studies also reported high levels of personal gratification (n = 1), and high involvement in the application (n = 1). VR-BF was also rated as more sympathetic and helpful than a classical BF condition (n = 1). Detrimental outcomes were rarely reported. Only one study assessed simulator sickness and another one signs of nausea while performing the VR intervention: Rockstroh et al. (2021) reported low values for simulation sickness (M = 1.40, SD = 0.40, Likert scale from 1 to 5), Van Rooij et al. (2016) reported that 86% of participants did not show any signs of nausea, yet the authors do not discuss the remaining 14% that did. Prabhu et al. (2019) reported excluding a priori participants with simulation sickness, and four studies reported excluding patients with neurological diseases, migraine, headache, or vestibular abnormalities (Gaggioli et al., 2014; Gorini et al., 2010; Pallavicini et al., 2009; Repetto et al., 2011). Other detrimental outcomes did not find mention in any of the studies.
Discussion
This scoping review aimed to establish the state of research regarding a novel form of BF, i.e., the integration of VR in traditional BF protocols. The main objective was to provide an overview over study design, samples, used soft- and hardware, and outcomes.
Overall, 18 studies were included in the current scoping review, most of which were published in the last five years. This rise in interest may be explained by the acceleration in the development of VR technology which followed the launch of the affordable Oculus Rift HMD in 2013. The rapid growth of the VR market since then (Chang & Chen, 2017) has resulted in a broader variety not only of providers but also of cheaper VR soft- and hardware (Hodgson et al., 2015). Big game engine companies like Epic Games or Unity Technologies have expanded their gaming engines with tools to design environments directly for VR, thus making it easier to program inexpensive, high-quality VR applications. Accordingly, most studies included in this review applied of high-end, usable, and comfortable to wear HMDs like Oculus Rift or HTC Vive that provide a 100-to-110-degree diagonal FoV immersion instead of more conservative alternatives like the VUZIX Eyewear (30-to-40-degree) or the DeepStream stereoscopic viewer (85 degree).
Most studies originated from one of three countries: Italy, Germany, or The Netherlands. While research from Italy, namely the EU-funded INTREPID (Gorini et al., 2010; Pallavicini et al., 2009; Repetto et al., 2011) and INTERSTRESS (Gagglioni et al., 2014) projects performed ground work in the field, new research mostly emerges out of one research group located in Freiburg, Germany (Blum et al., 2019; Rockstroh et al., 2019, 2020, 2021) and several research groups in The Netherlands (Bossenbroek et al., 2020; Hendriks & Rombout, 2018; Maarsingh et al., 2019; Van Rooij et al., 2016).
The studies included in this review primarily targeted anxiety, stress, and pain as their main outcomes. Results indicate that VR-BF successfully reduces anxiety, stress and pain compared to baseline. When compared to classical BF, VR-BF was equally effective in reducing stress (Blum et al., 2019; Rockstroh et al., 2019, 2020) and anxiety (Gagglioni et al., 2014; Gorini et al., 2010; Repetto et al., 2011). With regards to pain reduction, VR-BF seems to be even more effective than traditional BF (Tong et al., 2015), yet, with just thirteen participants in total, the generalizability of this study’s finding is limited. Moreover, one study (Tinga et al., 2019) found a higher reduction in arousal in a control group using only VR (a moving cloud automatically simulating breath) and no BF compared to a VR-BF group (moving cloud controlled by participant’s respiration), raising the additional question of the necessity of BF in relaxation interventions.
While at this point there is no unambiguous evidence that VR-BF is more effective than classical BF, the current review indicates that VR based BF protocols have advantages over traditional ones when it comes to motivation, user experience and involvement. Results show a better training experience, a high motivation to use VR-BF, as well as strong involvement, better focused and sustained attention, and high levels of flow. Similarly, in the reviewed studies, personal gratification was elevated, and the technology was found to be sympathetic and helpful. In light of these encouraging findings, one may cautiously conclude that combining VR with BF may support particularly those factors which – according to the psychoengineering model (Gaume et al., 2016) – are key to feedback learning and thus, to the success of BF.
However, the role of gamification in increasing motivation remains unclear. Most studies in this review used single task exercises and only two studies applied an elaborate gamification approach: Houzangbe et al. (2020) placed the participants in a sequence of adjoining futuristic laboratory rooms, with the subsequent rooms opening up after room-specific BF exercises had been solved (e.g., regulating their HR to shoot a weapon). Similarly, in “Stressjam”, the exercises were embedded in a cohesive story line in which the participants had to prevent an island from being destroyed by a volcano (Maarsingh et al., 2019). Both studies, however, lacked a control group and tested their prototype in no more than three sessions, precluding generalizations and conclusions with regards to long-term treatment effects.
Overall, not only gamification elements, but also the VE itself may influence motivation. The interactive nature of fully immersive VEs has been found to be particularly engaging and add to a rewarding user experience (Tcha-Tokey et al., 2018). Above all, however, the advantage of using VR in combination with BF seems to lie in the positive impact it has on attention: The increase in focused and sustained attention, and the decrease in mind-wandering incidents, as well as experiences of flow (Csikszentmihalyi & Csikzentmihaly, 1990) may all be attributable to the immersiveness of the technology which shields from distractions (Slater & Wilbur, 1997). Furthermore, according to the Attention Restoration Theory (Kaplan, 1995), nature environments – such as those which were used in most studies – facilitate replenishing attentional resources. Despite these positive results, some authors (Yu et al., 2018) argue that interactive immersive VEs coupled with BF displays may require even more (attentional) effort to engage in the feedback learning process. Hence, the exact relationship between VR-BF and cognitive remains to be established.
Overall, the positive effects of VR do not seem to translate into an advantage of VR-BF over classical BF in terms of effectiveness. One answer may be that the motivational aspects only come into play after several sessions. At the beginning, classical BF as well as VR-BF may both profit of the novelty effect, but over time the abstract, “boring” (Gaume et al., 2016) traditional BF tasks may make it difficult keep up attention and motivation. This assumption is supported by the fact that those studies which compared VR-BF with a classical intervention over several sessions also found a higher decrease in HR and EDA (Pallavicini et al., 2009; Repetto et al., 2011) and stress (Tu et al., 2020) and a higher increase in coping skills (Gagglioni et al., 2014) in the VR-BF condition. Similarly, trials with more than three sessions were accompanied by a more positive training experience (Tu et al., 2020), high involvement (Maarsingh et al., 2019) and a higher feeling of flow and sympathy (Kojic et al., 2019). However, nine studies in this review performed BF only once. Hence, the impact of repeated VR based BF training on long-term motivation and ultimately on treatment outcomes remains to be evaluated.
The majority of participants in this review were adults. This is noteworthy, since children and adolescents may particularly benefit from innovative BF protocols which use gamification and VR to increase involvement and motivation (see Fadhli et al., 2020). While adults may succeed with a goal orientation (e.g., pain relief), children are even more dependent on an intervention which facilitates intrinsic motivation (Kanfer, 1990). Generally, the use of VR in underage samples particularly for therapeutic interventions is still in its infancy (Kothgassner & Felnhofer, 2021). Thus, future research is encouraged to increasingly consider children and adolescents as possible target groups for VR-BF.
Apart from minors, clinical samples are also worth investigating. It was surprising to find that most studies (n = 9) in this review focused exclusively on healthy participants. Only GAD (Gorini et al., 2010; Pallavicini et al., 2009; Repetto et al., 2011) and chronic pain (Prabhu et al., 2019; Tong et al., 2015) patients were treated in more than one study. Rather innovative indications such as with ADHD or ASD patients (Bossenbroek et al., 2020) show promising improvements with VR-BF. However, VR-BF interventions in these samples primarily focused on stress regulation and relaxation rather than on alleviating symptoms specific to ADHD and ASD such as attention deficits, impulsivity and hyperactivity, or social deficits and restrictive behaviors. This is in line with the assumption, that BF training may be more useful as an adjuvant therapy rather than a first line treatment for some disorders.
Limitations
The present review has several limitations which are common for scoping reviews. First, we did not perform a quantitative data synthesis, as our research question was broad in scope and the quality of most included papers was rather low, with only nine papers reporting RCTs. Hence, future systematic reviews and meta-analyses should pursue a much narrower research question than the one posed for this review. Also, we could not derive any conclusions regarding possible contraindications to VR-BF. Even though VR constitutes a promising technology, it may, in some cases, induce cybersickness (i.e., nausea, headache, tiredness or discomfort, (Mehrfard et al., 2019). Hence, patients with epilepsy, monocular vision, or vestibular impairments are not suitable for inclusion in VR based treatments. All studies stated that they had excluded participants with the above-mentioned impairments, but no study raised additional impairments or reported on incidents of cybersickness. Similarly, none of the studies discussed the issue of body position and movements during training: Since VR is mostly used in a standing position, this could cause artifacts in physiological signals. Overall, a more thorough documentation in future research is necessary.
Conclusion
Recent years have brought forward research on VR-BF interventions aimed at treating anxiety, stress, and chronic pain. HMDs have superseded alternate, less functional VE solutions such as smartphones or heavy, unwieldy apparatuses like the stereoscopic viewers. Despite these developments, the field may still be regarded as new. Further RCTs with representative samples and higher training frequency are necessary to establish whether VR-BF is superior to classical BF.
Also, further research is needed to assess the specific impact of VR and gamification on motivation, attention, and user experience. This would help establish if the use of BF protocols based on gaming mechanisms constitute an advantage over more traditional protocols, particularly in those target groups that are considered hard to motivate such as children and adolescents (see Fadhli et al., 2020). Finally, ecologically valid VEs promise to facilitate the transfer learnt skills to real-world settings (Kothgassner & Felnhofer, 2020). None of the studies included in this review assessed whether the newly acquired abilities were transferred to everyday life. Focusing on this aspect would help future research determine whether the use of VR has added benefit compared to traditional BF protocols or whether it is better suited as a complementary therapy.
Data Availability
The authors confirm that the data supporting the findings of this study are available within the article and its supplementary materials.
Code Availability
Not applicable.
References
Annerstedt, M., Jönsson, P., Wallergård, M., Johansson, G., Karlson, B., Grahn, P., Hansen, Å. M., & Währborg, P. (2013). Inducing physiological stress recovery with sounds of nature in a virtual reality forest — Results from a pilot study. Physiology and Behavior, 118, 240–250. https://doi.org/10.1016/j.physbeh.2013.05.023
Arksey, H., & O’Malley, L. (2005). Scoping studies: Towards a methodological framework. International Journal of Social Research Methodology, 8(1), 19–32. https://doi.org/10.1080/1364557032000119616
Blum, J., Rockstroh, C., & Göritz, A. S. (2019). Heart rate variability biofeedback based on slow-paced breathing with immersive virtual reality nature scenery. Frontiers in Psychology, 10(2172), 2172. https://doi.org/10.3389/fpsyg.2019.02172
Bohil, C. J., Alicea, B., & Biocca, F. A. (2011). Virtual reality in neuroscience research and therapy. Nature Reviews Neuroscience, 12(12), 752–762. https://doi.org/10.1038/nrn3122
Bossenbroek, R., Wols, A., Weerdmeester, J., Lichtwarck-Aschoff, A., Granic, I., & van Rooij, M. (2020). Efficacy of a virtual reality biofeedback game (DEEP) to reduce anxiety and disruptive classroom behavior: single-case study. JMIR Ment Health, 7(3), e16066. https://doi.org/10.2196/16066
Chang, S., & Chen, W. (2017). Does visualize industries matter? A Technology Foresight of Global Virtual Reality and Augmented Reality Industry. International Conference on Applied System Innovation (ICASI). https://doi.org/10.1109/ICASI.2017.7988432
Connolly, T. M., Boyle, E. A., Macarthur, E., Hainey, T., & Boyle, J. M. (2012). A systematic literature review of empirical evidence on computer games and serious games. Computers & Education, 59(2), 661–686. https://doi.org/10.1016/j.compedu.2012.03.004
Csikszentmihalyi, M., & Csikzentmihaly, M. (1990). Flow: The psychology of optimal experience. Harper & Row New York.
Deterding, S., Dixon, D., Khaled, R., & Nacke, L. (2011) From game design elements to gamefulness: defining gamification. Proceedings of the 15th international academic MindTrek conference Envisioning future media environments, Doi: https://doi.org/10.1145/2181037.2181040
Domínguez, A., Saenz-de-Navarrete, J., & de-Marcos, L., Fernández-Sanz, L., Pagés, C., & Martínez-Herráiz, J.-J. (2013). Gamifying learning experiences Practical implications and outcomes. Computers & Education, 63, 380–392. https://doi.org/10.1016/j.compedu.2012.12.020
Fadhli, M., Brick, B., Setyosari, P., Ulfa, S., & Kuswandi, D. (2020). A meta-analysis of selected studies on the effectiveness of gamification method for children. International Journal of Instruction, 13(1), 845–854. https://doi.org/10.29333/iji.2020.13154a
Frank, D. L., Khorshid, L., Kiffer, J. F., Moravec, C. S., & McKee, M. G. (2010). Biofeedback in medicine: Who, when, why and how? Mental Health in Family Medicine, 7(2), 85.
Gaggioli, A., Pallavicini, F., Morganti, L., Serino, S., Scaratti, C., Briguglio, M., Crifaci, G., Vetrano, N., Giulintano, A., Bernava, G., Tartarisco, G., Pioggia, G., Raspelli, S., Cipresso, P., Vigna, C., Grassi, A., Baruffi, M., Wiederhold, B., & Riva, G. (2014). Experiential virtual scenarios with real-time monitoring (Interreality) for the management of psychological stress: a block randomized controlled trial. Journal of Medical Internet Research, 16(7), e167. https://doi.org/10.2196/jmir.3235
Gaume, A., Vialatte, A., Mora-Sánchez, A., Ramdani, C., & Vialatte, F. B. (2016). A psychoengineering paradigm for the neurocognitive mechanisms of biofeedback and neurofeedback. Neuroscience and Biobehavioral Reviews, 68, 891–910. https://doi.org/10.1016/j.neubiorev.2016.06.012
Goessl, V. C., Curtiss, J. E., & Hofmann, S. G. (2017). The effect of heart rate variability biofeedback training on stress and anxiety: A meta-analysis. Psychological Medicine, 47(15), 2578–2586. https://doi.org/10.1017/S0033291717001003
Gorini, A., Pallavicini, F., Algeri, D., Repetto, C., Gaggioli, A., & Riva, G. (2010). Virtual reality in the treatment of generalized anxiety disorders. Studies in Health Technology and Informatics, 154, 39–43. https://doi.org/10.3233/978-1-60750-561-7-39
Hamari, J., Koivisto, J., & Sarsa, H. (2014). Does gamification work? A literature review of empirical studies on gamification: 47th Hawaii international conference on system sciences. https://doi.org/10.1109/HICSS.2014.377
Hendriks, M., & Rombout, L. (2018). Towards attention-based design of mental health interventions in virtual reality. 10th Cracow Cognitive Science Conference-Technology CEUR.
Hodgson, E., Bachmann, E. R., Vincent, D., Zmuda, M., Waller, D., & Calusdian, J. (2015). WeaVR: A self-contained and wearable immersive virtual environment simulation system. Behavior Research Methods, 47(1), 296–307. https://doi.org/10.3758/s13428-014-0463-1
Houzangbe, S., Christmann, O., Gorisse, G., & Richir, S. (2020). Effects of voluntary heart rate control on user engagement and agency in a virtual reality game. Virtual Reality, 24(4), 665–681. https://doi.org/10.1007/s10055-020-00429-7
Kanfer, R. (1990). Motivation and individual differences in learning: An integration of developmental, differential and cognitive perspectives. Learning and Individual Differences, 2(2), 221–239. https://doi.org/10.1016/1041-6080(90)90023-A
Kaplan, S. (1995). The restorative benefits of nature: Toward an integrative framework. Journal of Environmental Psychology, 15(3), 169–182. https://doi.org/10.1016/0272-4944(95)90001-2
Kojic, T., Nugyen, L. T., & Voigt-Antons, J.-N. (2019). Impact of constant visual biofeedback on user experience in virtual reality. Exergames. https://doi.org/10.1109/ism46123.2019.00068
Kothgassner, O. D., & Felnhofer, A. (2020). Does virtual reality help to cut the Gordian knot between ecological validity and experimental control? Annals of the International Communication Association, 44(3), 210–218. https://doi.org/10.1080/23808985.2020.1792790
Kothgassner, O. D., & Felnhofer, A. (2021). Lack of research on efficacy of virtual reality exposure therapy (VRET) for anxiety disorders in children and adolescents. Neuropsychiatrie, 35(2), 68–75. https://doi.org/10.1007/s40211-020-00349-7
Latta, J. N., & Oberg, D. J. (1994). A conceptual virtual reality model. IEEE Computer Graphics and Applications, 14(1), 23–29. https://doi.org/10.1109/38.250915
Lehrer, P., Kaur, K., Sharma, A., Shah, K., Huseby, R., Bhavsar, J., & Zhang, Y. (2020). Heart rate variability biofeedback improves emotional and physical health and performance: a systematic review and meta analysis. Applied Psychophysiology and Biofeedback, 45(3), 109–129. https://doi.org/10.1007/s10484-020-09466-z
Levac, D., Colquhoun, H., & O’Brien, K. K. (2010). Scoping studies: Advancing the methodology. Implementation Science, 5(1), 69. https://doi.org/10.1186/1748-5908-5-69
Liszio, S., Graf, L., & Masuch, M. (2018). The relaxing effect of virtual nature: Immersive technology provides relief in acute stress situations. Annual Review of Cybertherapy and Telemedicine, 16, 87–93.
Maarsingh, B. M., Bos, J., Van Tuijn, C. F. J., & Renard, S. B. (2019). Changing stress mindset through stressjam: a virtual reality game using biofeedback. Games Health J, 8(5), 326–331. https://doi.org/10.1089/g4h.2018.0145
Mehrfard, A., Fotouhi, J., Taylor, G., Forster, T., Navab, N., & Fuerst, B. (2019). A Comparative Analysis of Virtual Reality Head-Mounted Display Systems arXiv: 1912.02913
Nakao, M., Yano, E., Nomura, S., & Kuboki, T. (2003). Blood pressure-lowering effects of biofeedback treatment in hypertension: A meta-analysis of randomized controlled trials. Hypertension Research, 26(1), 37–46. https://doi.org/10.1291/hypres.26.37
Nestoriuc, Y., Rief, W., & Martin, A. (2008). Meta-analysis of biofeedback for tension-type headache: Efficacy, specificity, and treatment moderators. Journal of Consulting and Clinical Psychology, 76(3), 379–396. https://doi.org/10.1037/0022-006X.76.3.379
Pallavicini, F., Algeri, D., Repetto, C., Gorini, A., & Riva, G. (2009). Biofeedback, virtual reality and mobile phones in the treatment of generalized anxiety disorder (GAD): A phase-2 controlled clinical trial. Journal of Cyber Therapy and Rehabilitation, 2(4), 315–327.
Peters, M. D., Godfrey, C. M., Khalil, H., McInerney, P., Parker, D., & Soares, C. B. (2015). Guidance for conducting systematic scoping reviews. JBI Evidence Implementation, 13(3), 141–146. https://doi.org/10.1097/XEB.0000000000000050
Prabhu, V. G., Linder, C., Stanley, L. M., & Morgan, R. (2019). An Affective computing in virtual reality environments for managing surgical pain and anxiety. IEEE International Conference on Artificial Intelligence and Virtual Reality (AIVR). https://doi.org/10.1109/AIVR46125.2019.00049
Repetto, C., Gaggioli, A., Pallavicini, F., Cipresso, P., Raspelli, S., & Riva, G. (2011). Virtual reality and mobile phones in the treatment of generalized anxiety disorders: A phase-2 clinical trial. Pers Ubiquitous Comput, 17(2), 253–260. https://doi.org/10.1007/s00779-011-0467-0
Riva, G. (2003). Virtual environments in clinical psychology. Psychotherapy Theory, Research, Practice, Training, 40(1), 68. https://doi.org/10.1037/0033-3204.40.1-2.33
Rockstroh, C., Blum, J., & Göritz, A. S. (2019). Virtual reality in the application of heart rate variability biofeedback. International Journal of Human-Computer Studies, 130, 209–220. https://doi.org/10.1016/j.ijhcs.2019.06.011
Rockstroh, C., Blum, J., & Göritz, A. S. (2020). Combining VR and Biofeedback. Journal of Media Psychology, 32(4), 176–186. https://doi.org/10.1027/1864-1105/a000270
Rockstroh, C., Blum, J., & Göritz, A. S. (2021). A mobile VR-based respiratory biofeedback game to foster diaphragmatic breathing. Virtual Reality, 25(2), 539–552. https://doi.org/10.1007/s10055-020-00471-5
Sailer, M. (2016). Die Wirkung von Gamification auf Motivation und Leistung. Springer.
Schoenberg, P. L., & David, A. S. (2014). Biofeedback for psychiatric disorders: A systematic review. Applied Psychophysiology and Biofeedback, 39(2), 109–135. https://doi.org/10.1007/s10484-014-9246-9
Schwartz, G. E. (1973). Biofeedback as therapy: Some theoretical and practical issues. American Psychologist, 28(8), 666–673. https://doi.org/10.1037/h0035759
Schwartz, M. S. (2010). A new improved universally accepted official definition of biofeedback: Where Did It Come From? Why? Who Did It? Who Is It for? What’s Next? Biofeedback, 38(3), 88–90. https://doi.org/10.5298/1081-5937-38.3.88
Sielski, R., Rief, W., & Glombiewski, J. A. (2017). Efficacy of biofeedback in chronic back pain: A meta-analysis. International Journal of Behavioral Medicine, 24(1), 25–41. https://doi.org/10.1007/s12529-016-9572-9
Slater, M., & Wilbur, S. (1997). A framework for immersive virtual environments (FIVE) Speculations on the role of presence in virtual environments. Presence Teleoperators & Virtual Environments, 6(6), 603–616. https://doi.org/10.1162/pres.1997.6.6.603
Tcha-Tokey, K., Christmann, O., Loup-Escande, E., Loup, G., & Richir, S. (2018). Towards a model of user experience in immersive virtual environments. Advances in Human-Computer Interaction. https://doi.org/10.1155/2018/7827286
Tinga, A. M., Nyklíček, I., Jansen, M. P., de Back, T. T., & Louwerse, M. M. (2019). Respiratory biofeedback does not facilitate lowering arousal in meditation through virtual reality. Applied Psychophysiology and Biofeedback, 44(1), 51–59. https://doi.org/10.1007/s10484-018-9421-5
Tolin, D. F., Davies, C. D., Moskow, D. M., & Hofmann, S. G. (2020). Biofeedback and neurofeedback for anxiety disorders: A quantitative and qualitative systematic review. Anxiety Disorders. https://doi.org/10.1007/978-981-32-9705-0_16
Tong, X., Gromala, D., Choo, A., Amin, A., & Shaw, C. (2015). The Virtual meditative walk: an immersive virtual environment for pain self-modulation through mindfulness-based stress reduction meditation. In Virtual, Augmented and Mixed Reality Springer. https://doi.org/10.1007/978-3-319-21067-4_40
Tricco, A. C., Lillie, E., Zarin, W., O’Brien, K. K., Colquhoun, H., Levac, D., Moher, D., Peters, M. D. J., Horsley, T., Weeks, L., Hempel, S., Akl, E. A., Chang, C., McGowan, J., Stewart, L., Hartling, L., Aldcroft, A., & Wilson, M. G. (2018). PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Annals of Internal Medicine, 169(7), 467–473. https://doi.org/10.7326/M18-0850
Tu, L., Hao, T., Bi, C., & Xing, G. (2020). BreathCoach: A smart in-home breathing training system with bio-feedback via VR game. Smart Health, 16, 100090. https://doi.org/10.1016/j.smhl.2019.100090
Van Rooij, M., Lobel, A., Harris, O., Smit, N., & Granic, I. (2016). DEEP: A biofeedback virtual reality game for children at-risk for anxiety. Proceedings of the CHI Conference Extended Abstracts on Human Factors in Computing Systems. https://doi.org/10.1145/2851581.2892452
Walker, J. E., & Lawson, R. (2013). FP02 beta training for drug-resistant depression - A new protocol that usually reduces depression and keeps it reduced. Journal of Neurotherapy, 17(3), 198–200. https://doi.org/10.1080/10874208.2013.785784
Yu, B., Funk, M., Hu, J., Wang, Q., & Feijs, L. (2018). Biofeedback for everyday stress management: A systematic review. Frontiers in ICT, 5, 23. https://doi.org/10.3389/fict.2018.00023
Funding
Open access funding provided by Medical University of Vienna. No funds, grants or other support was received for conducting this research.
Author information
Authors and Affiliations
Contributions
A.F. devised the idea for the study and developed a procedure plan as well as the inclusion/ exclusion criteria. R.L. collected the data and performed the analysis under supervision of A.F. Both R.L. and A.F. discussed the results. R.L. wrote the first draft of the manuscript and both authors commented on previous versions of the manuscript. Both authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical Approval
Not applicable.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lüddecke, R., Felnhofer, A. Virtual Reality Biofeedback in Health: A Scoping Review. Appl Psychophysiol Biofeedback 47, 1–15 (2022). https://doi.org/10.1007/s10484-021-09529-9
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10484-021-09529-9