
Abstract
Background
The aim of the present study was to assess the relationship between symptoms of obstructed defecation and findings on magnetic resonance (MR) defecography in males with obstructed defecation syndrome (ODS).
Methods
Thirty-six males with ODS who underwent MR defecography at our institution between March 2013 and February 2016 were asked in a telephone interview about their symptoms and subsequent treatment, either medical or surgical. Patients were divided into 2 groups, one with anismus (Group 1) and one with prolapse without anismus (Group 2). The interaction between ODS type and symptoms with MR findings was assessed by multivariate analysis for categorical data using a hierarchical log-linear model. MR imaging findings included lateral and/or posterior rectocele, rectal prolapse, intussusception, ballooning of levator hiatus with impingement of pelvic organs and dyskinetic puborectalis muscle.
Results
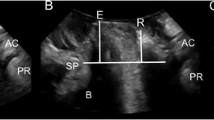
There were 21 males with ODS due to anismus (Group 1) and 15 with ODS due to rectal prolapse/intussusception (Group 2). Mean age of the entire group was 53.6 ± 4.1 years (range 18–77 years). Patients in Group 1 were slightly older than those in Group 2 (age peak, sixth decade in 47.6 vs 20.0%, p < 0.05). Symptoms most frequently associated with Group 1 patients included small volume and hard feces (85.0%, p < 0.01), excessive strain at stool (81.0%, p < 0.05), tenesmus and fecaloma formation (57.1 and 42.9%, p < 0.05); symptoms most frequently associated with Group 2 patients included mucous discharge, rectal bleeding and pain (86.7%, p < 0.05), prolonged toilet time (73.3%, p < 0.05), fragmented evacuation with or without digitation (66.7%, p < 0.005). Voiding outflow obstruction was more frequent in Group 1 (19.0 vs 13.3%; p < 0.05), while non-bacterial prostatitis and sexual dysfunction prevailed in Group 2 (26.7 and 46.7%, p < 0.05). At MR defecography, two major categories of findings were detected: a dyskinetic pattern (Type 1), seen in all Group 1 patients, which was characterized by non-relaxing puborectalis muscle, sand-glass configuration of the anorectum, poor emptying rate, limited pelvic floor descent and final residue ≥ 2/3; and a prolapsing pattern (Type 2), seen in all Group 2 patients, which was characterized by rectal prolapse/intussusception, ballooning of the levator hiatus with impingement of the rectal floor and prostatic base, excessive pelvic floor descent and residue ≤ 1/2. Posterolateral outpouching defined as perineal hernia was present in 28.6% of patients in Group 1 and were absent in Group 2. The average levator plate angle on straining differed significantly in the two patterns (21.3° ± 4.1 in Group 1 vs 65.6° ± 8.1 in Group 2; p < 0.05). Responses to the phone interview were obtained from 31 patients (18 of Group 1 and 13 of Group 2, response rate, 86.1%). Patients of Group 1 were always treated without surgery (i.e., biofeedback, dietary regimen, laxatives and/or enemas) which resulted in symptomatic improvement in 12/18 cases (66.6%). Of the patients in Group 2, 2/13 (15.3) underwent surgical repair, consisting of stapled transanal rectal resection (STARR) which resulted in symptom recurrence after 6 months and laparoscopic ventral rectopexy which resulted in symptom improvement. The other 11 patients of Group 2 were treated without surgery with symptoms improvement in 3 (27.3%).
Conclusions
The appearance of various abnormalities at MR defecography in men with ODS shows 2 distinct patterns which may have potential relevance for treatment planning, whether conservative or surgical.






Similar content being viewed by others


References
Hricak H, Williams RD, Spring DB et al (1983) Anatomy and pathology of the male pelvis by magnetic resonance imaging. Am J Roentgenol 141:1101–1110
Myers RP, Cahill DR, Kay PA et al (2000) Puboperineales: muscular boundaries of the male urogenital hiatus in 3D magnetic resonance imaging. J Urol 164:1412–1415
Brown G, Kirkham A, Williams GT et al (2004) High resolution MRI of the anatomy important in total mesorectal excision of the rectum. Am J Roentgenol 182:431–439
Kiyoshima K, Yokomizo A, Yoshida T et al (2004) Anatomical features of periprostatic tissue and its surroundings: a histological analysis of 79 radical retropubic prostatectomy specimens. Jpn J Clin Oncol 34:463–468
Lienemann A, Anthuber C, Baron A et al (1997) Dynamic MR colpocystorectography assessing pelvic floor descent. Eur Radiol 7:1309–1317
Comiter CV, Vasavada SP, Barbaric ZL et al (1999) Grading pelvic prolapse and pelvic floor relaxation using dynamic magnetic resonance imaging. Urology 54:454–457
Stoker J, Halligan S, Bartram CI (2001) Pelvic floor imaging. Radiology 218:621–641
Fielding JR (2002) Practical MR imaging of female pelvic floor weakness. Radiographics 22:295–304
Cortes E, Reid WMN, Singh K et al (2004) Clinical examination and dynamic magnetic resonance imaging in vaginal vault prolapse. Obstet Gynecol 103:41–46
Dvorkin LS, Hetzer F, Scott SM et al (2004) Open-magnet MR defecography compared with evacuation proctography in the diagnosis and management of patients with rectal intussusception. Colorect Dis 6:45–53
Tomita R, Igarashi S, Fujisaki S et al (2010) Significance of defecography in the diagnosis and evaluation of male patients with defecation disorders. Hepatogastroenterology 57:220–223
Altomare DF, Spazzafumo L, Rinaldi M et al (2008) Set-up and statistical validation of a new scoring system for obstructed defecation syndrome. Colorectal Dis 10:84–88
Piloni V, Tosi P, Vernelli M (2013) MR-defecography in obstructed defecation syndrome (ODS): technique, diagnostic criteria and grading. Tech Coloproctol 17:501–510
Mahieu P, Pringot J, Bodart P (1984) Defecography: II. Contribution to the diagnosis of defecation disorders. Gastrointest Radiol 9:253–261
Kujipers HC, Bleijenberg G (1985) The spastic pelvic floor syndrome: a cause of constipation. Dis Colon Rectum 28:6669–6672
Ekberg O, Mahieu PHG, Bartram CI et al (1990) Defecography: dynamic radiological imaging in proctology. Gastroenterol Int 3:93–99
Piloni V, Amadio L, Marmorale C (1991) Defecography in obstructed defecation. A unifying concept for fecal blockade syndrome. Coloproctology 13:118–122
Wexner SD (1991) Rectal prolapse and intussusception. In: Beck DE, Welling D (eds) Manual of patient care in colorectal surgery. Little Brown, Boston, pp 191–212
Spazzafumo L, Piloni V (1999) Rectal constipation and clinical decision-making: multiple correspondence analysis of defecographic findings. Tech Coloproctol 4:117–121
Fritsch H, Hotzinger H (1995) Tomographical anatomy of the pelvis, visceral pelvic connective tissue, and its compartments. Clin Anat 8:17–24
Skomorowska E, Hegedus V (1987) Sex differences in anorectal angle and perineal descent. Gastrointest Radiol 12:353–355
Cavallo G, Salzano A, Grassi R et al (1991) Rectocele in males: clinical, defecographic, and CT study of singular cases. Dis Colon Rectum 34:964–966
Chen HH, Iroatulam A, Alabaz O et al (2001) Associations of defecography and physiologic findings in male patients with rectocele. Tech Coloproctol 5:157–161
Savoye-Collet C, Savoye G, Koning E et al (2010) Gender influence on defecographic abnormalities in patients with posterior pelvic floor disorders. World J Gastroenterol 16(4):462–466
Andrade LC, Correia H, Semedo LC et al (2015) Conventional videodefecography: pathologic findings according to gender and age. Eur J Radiol 1:1–5
Mikuma N, Namagawa M, Morita K et al (1998) Magnetic resonance imaging of the male pelvic floor. The anatomical configuration and dynamic movement in healthy men. Neurourol Urodyn 17:591–597
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Piloni, V., Bergamasco, M., Melara, G. et al. The clinical value of magnetic resonance defecography in males with obstructed defecation syndrome. Tech Coloproctol 22, 179–190 (2018). https://doi.org/10.1007/s10151-018-1759-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10151-018-1759-4