
Abstract
Background
A subgroup analysis of data from a nationwide study (KCSG-ST19-16) was performed to evaluate the efficacy and safety of second-line ramucirumab plus paclitaxel treatment in patients with human epidermal growth factor receptor 2 (HER2)-positive advanced gastric or gastro-esophageal junction (GEJ) adenocarcinoma.
Methods
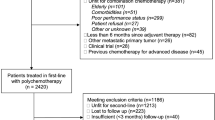
The KCSG-ST19-16 study enrolled a total of 1063 patients from 56 hospitals in South Korea with advanced gastric or GEJ adenocarcinoma, who had received second-line treatment with ramucirumab plus paclitaxel. HER2 status was known for 994 (93.5%) of these patients, who were thus included in the subgroup analysis.
Results
In total, 163 of 994 patients (16.4%), had HER2-positive gastric or GEJ adenocarcinoma. The objective response rate to ramucirumab plus paclitaxel treatment was significantly higher in patients with HER2-positive disease compared to those with HER2-negative disease (23.0% [95% confidence interval (CI), 15.9–30.1] vs. 15.1% [95% CI, 12.3–17.9], p = 0.025). The median progression-free survival was longer in patients with HER2-positive versus HER2-negative disease, but the difference was not statistically significant (4.3 months [95% CI, 3.7–5.3] vs 3.7 months [95% CI, 3.4–4.0], p = 0.054). There was no statistically significant difference in median overall survival (OS) between the groups (9.8 months [95% CI, 8.9–12.3] vs 10.1 months [95% CI, 9.2–10.9], p = 0.564).
Conclusions
In patients with HER2-positive gastric or GEJ adenocarcinoma, the objective response rate to second-line treatment with ramucirumab plus paclitaxel was significantly higher compared to patients with HER2-negative disease. However, an increased response to treatment was not associated with an improvement in OS.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Gastric cancer is the fifth most frequently diagnosed cancer and third leading cause of cancer death worldwide [1]. In South Korea, despite a national screening program, which has contributed to a reduction in mortality, gastric cancer remains the fourth leading cause of cancer death following lung, liver, and colorectal cancer [2].
For advanced inoperable gastric cancer patients, fluoropyrimidine and platinum-containing chemotherapy is used as a first-line treatment. For patients who fail first-line chemotherapy, a combination of ramucirumab (an anti-vascular endothelial growth factor receptor 2 [VEGFR-2] antibody) and paclitaxel has been recommended as a standard second-line treatment, irrespective of human epidermal growth factor receptor 2 (HER2) status, after its efficacy was proven for all-comers without biomarker selection in the RAINBOW trial [3].
HER2 protein overexpression or HER2 gene amplification has been identified in approximately 15–20% of advanced gastric and gastro-esophageal junction (GEJ) cancer patients [4], and based on the ToGA trial [5], trastuzumab in combination with conventional chemotherapy is recommended as a first-line treatment. To date, with the exception of ramucirumab, which is used for all-comers, trastuzumab is the only ‘targeted agent’ approved as a front-line treatment for gastric cancer, and biomarkers that may predict the efficacy of ramucirumab still need to be verified.
Preclinical studies have suggested that ramucirumab, as a second-line treatment, may overcome the trastuzumab resistance observed in HER2-positive gastric cancer patients who fail first-line trastuzumab containing treatment. In vitro data from HER2-positive breast cancer indicate a relationship between HER2 overexpression and activation of the angiogenic pathway in tumor cells [6,7,8] and VEGFR-2 inhibitors, such as ramucirumab, may play a role in overcoming trastuzumab resistance by preventing crosstalk between HER2 signaling and angiogenesis.
According to a subgroup analysis of RAINBOW trial data [9], efficacy outcomes, including overall survival (OS), the objective response rate (ORR) and the disease control rate (DCR), were improved in the patient subgroup that received prior treatment with trastuzumab compared to the overall study population. However, definitive conclusions could not be drawn since only 6% (39 of 665 patients) of the study population had previously received trastuzumab treatment.
Previously, the Korean Cancer Study Group (KCSG) conducted a nationwide, real-world study of a second-line treatment consisting of ramucirumab plus paclitaxel for advanced gastric cancer patients, and established a large-scale cohort. This subgroup analysis aims to determine the efficacy and safety of treatment with ramucirumab plus paclitaxel, according to HER2 status, by analyzing patients whose HER2 status was confirmed.
Methods
Study design
This study performed a subgroup analysis of data from a nationwide, retrospective study conducted in South Korea (KCSG-ST19-16; clinicaltrial.gov identifier: NCT04192734) that evaluated the efficacy and safety of second-line treatment with ramucirumab plus paclitaxel, with the goal of generating real-world evidence of the effects of this treatment in patients with gastric or GEJ adenocarcinoma.
The KCSG-ST19-16 study included South Korean patients with gastric or GEJ adenocarcinoma who received ramucirumab plus paclitaxel between May 1, 2018 and December 31, 2018. Patients aged ≥ 18 years with locally advanced unresectable or initially metastatic or recurrent gastric cancer, who had progressed from first-line fluoropyrimidine plus platinum-containing combination chemotherapy, were included. Patients who started treatment with ramucirumab alone or who had received ramucirumab or paclitaxel before 1 May 2018 were excluded.
The subgroup analysis included patients from the KCSG-ST19-16 study for whom HER2 status was known, as stated above. HER2 positivity was defined as immunohistochemistry (IHC) 3 + or IHC 2 + plus fluorescence in situ hybridization (FISH)/ silver-enhanced in situ hybridization (SISH)-positive.
Study objectives
The study objectives included evaluation of OS, PFS, ORR, DCR and treatment-related adverse events (TRAEs). OS was defined as the time from the start date of ramucirumab plus paclitaxel to the date of death or the last follow-up visit for patients still alive. If it was not known whether a patient had died, observations were censored at the data cut-off date or if available, at the last-known-alive date as captured in the medical records. PFS was defined as the time from the start date of ramucirumab plus paclitaxel to disease progression or death from any cause. Information on tumor response was obtained from medical records or computed tomography (CT) scans, according to the Response Evaluation Criteria in Solid Tumors (RECIST; version 1.1) criteria. Response to treatment was evaluated in patients with measurable disease. The ORR was defined as the proportion of patients who achieved a complete response (CR) or partial response (PR) to treatment. The DCR was defined as the proportion of patients who achieved a CR, PR, or stable disease (SD). Data on TRAEs were collected from the patients’ medical records and laboratory results, and graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events (NCI-CTCAE; version 5.0).
Data collection
The demographic and clinical characteristics analyzed included demographics, tumor stage, histological characteristics, tumor HER2 status, performance status, previous treatment history, subsequent treatments, laboratory results, and death. Descriptive data on ramucirumab plus paclitaxel treatment were also collected and analyzed, including the date of treatment initiation, response to treatment, and treatment end date. Data were collected and managed using an electronic data capture system, which included filters and a query-generating system to guarantee reliability, and to control for missing and inconsistent data and errors. Data were collected up to December 31, 2018.
Statistical analysis
Categorical variables were compared using chi-square or Fisher’s exact tests, as appropriate. OS and PFS curves were estimated using the Kaplan–Meier method and compared using log-rank tests. Univariable and multiple variable analyses were performed to identify the prognostic factors for PFS and OS based on the Cox-proportional hazard model. To minimize selection bias, propensity score matching (PSM) analysis was additionally conducted. The 1:1 nearest neighbor matching was applied, and 1:3 matching between group was achieved. The value of the caliper size was 0.1. Two-sided p values < 0.05 were considered statistically significant. All statistical analyses were performed using R statistical software (version 4.0.3; R Development Core Team Vienna, Austria).
Results
Patient characteristics
Previous study enrolled 1063 patients with advanced gastric or GEJ adenocarcinoma who had received second-line ramucirumab plus paclitaxel from 56 hospitals in South Korea. HER2 status was known for 994 of these patients, who were thus included in the subgroup analysis. Among the 994 patients, 163 (16.4%) had HER2-positive advanced gastric or GEJ adenocarcinoma; the patients’ baseline characteristics are presented in Table 1. Patients with HER2-positive disease were more likely to be male than those with HER2-negative disease (81.0% vs. 66.8%, p < 0.001), and patients with HER2-positive disease were also more likely to have GEJ adenocarcinoma as the primary tumor site (8.5% vs. 3.6%, p = 0.007) and a well-to-moderately differentiated histology (56.4% vs. 31.8%, p = < 0.001). Compared to patients with HER2-positive disease, those with HER2-negative disease had a lower disease burden (number of metastatic site ≥ 3, 25.5% vs. 16.6%, p = 0.007) and were also more likely to have peritoneal metastasis (42.9% vs. 55.4%, p = 0.004) and ascites (12.3% vs. 20.9%, p = 0.011). Time from start of the first-line chemotherapy to second-line ramucirumab plus paclitaxel was longer in patients with HER2-positive disease who received HER2 targeted treatment for the first-line treatment (≥ 6 months, 61% vs. 52.2%, p = 0.042). After disease progression to ramucirumab plus paclitaxel, 46% of patients (75 of 163) with HER2-positive disease and 47.1% (390 of 828) with HER2-negative disease received subsequent chemotherapy (p = 0.799). The proportion of patients who received anti-programmed cell death-1 (PD-1) antibody salvage treatment was slightly higher in the HER2-negative than -positive disease group, although the difference was not statistically significant (14.1% [23 of 163] vs. 17.5% [145 of 828], p = 0.361).
Efficacy and safety
Among patients (n = 755) who had measurable disease at the time of treatment, the ORR (23.0% [95% confidence interval (CI), 15.9–30.1] vs. 15.1% [95% CI, 12.3–17.9], p = 0.025) to ramucirumab plus paclitaxel treatment was significantly higher in those with HER2-positive compared to HER2-negative disease. The DCR was not significantly different between the groups (64.4% [95% CI, 56.3–72.5] vs. 56.6% [95% CI, 52.7–60.5], p = 0.093) (Table 2). Among all patients, including those with measurable and non-measurable disease, the ORR was significantly higher in patients with HER2-positive disease (23.3% [95% CI, 17.2–30.7] vs. 13.8% [95% CI, 11.6–16.4], p = 0.002) as was the DCR (65.6% [95% CI, 57.8–72.8] vs. 56.5% [95% CI, 53.1–59.9], p = 0.031) (Supplementary Table 1).
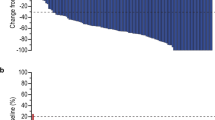
Based on a median follow-up of 7.0 months (range 0–17.2 months), the median PFS was numerically longer in patients with HER2-positive disease than in those without but, it was not statistically significant (4.3 months [95% CI, 3.7–5.3] vs. 3.7 months [95% CI, 3.4–4.0], p = 0.054) (Fig. 1A). There was no statistical significance in the median OS between the HER2-positive and -negative groups (9.8 months [95% CI, 8.9–12.3] vs. 10.1 months [95% CI, 9.2–10.9], p = 0.564) (Fig. 1B).

Kaplan–Meier estimates of progression-free survival A and overall survival B according to HER2 status
Of the 163 patients with HER2-positive disease, 37 (22.7%) did not receive a trastuzumab-containing regimen as the first-line treatment; most of these patients received fluoropyrimidine and platinum doublet chemotherapy (34 of 37, 91.8%) without trastuzumab. Efficacy analysis of patients with HER2-positive disease showed that the response to ramucirumab plus paclitaxel treatment and survival outcomes were not significantly different according to prior trastuzumab exposure (Supplementary Table 2 and Supplementary Fig. 1).
The incidences of adverse events are listed in Table 3. In patients with HER2-positive disease, the rates of grade ≥ 3 stomatitis (3.7% vs. 0.2%, p < 0.001) and all grades of hypertension (6.1% vs. 1.4%, p = 0.001) were higher than in patients with HER2-negative disease.
Prognostic factors
Univariable and multivariable analyses were performed to identify potential prognostic factors for PFS and OS (Table 4). The multivariable analysis included all pre-specified factors of interest. In all patients, eight factors were independently associated with a poor prognosis in the multivariable analysis: Eastern Cooperative Oncology Group (ECOG) performance status ≥ 2 (hazard ratio [HR] for PFS, 1.42 [95% CI 1.11–1.81], p = 0.005; HR for OS, 1.84 [95% CI 1.37–2.46], p < 0.001), weight loss in the previous 3 months ≥ 10% of body weight (HR for PFS, 1.4 [95% CI 1.10–1.79], p = 0.007; HR for OS, 1.67 [95% CI 1.25–2.24], p = 0.001), GEJ as the primary tumor (HR for PFS, 1.54 [95% CI 1.09–2.17], p = 0.014; HR for OS, 1.78 [95% CI 1.18–2.68], p = 0.006), poor or unknown histology grade (HR for OS, 1.29 [95% CI 1.05–1.60], p = 0.018), ≥ 3 metastatic sites (HR for PFS, 1.38 [95% CI 1.14–1.67], p = 0.001; HR for OS, 1.58 [95% CI 1.25–2.00], p < 0.001), presence of ascites (HR for PFS, 1.24 [95% CI 1.02–1.51], p = 0.03; HR for OS, 1.45 [95% CI 1.14–1.84], p = 0.003), no prior gastrectomy (HR for PFS, 1.56 [95% CI 1.34–1.82], p < 0.001; HR for OS, 1.56 [95% CI 1.27–1.91], p < 0.001), and time from first-line treatment to second-line treatment < 6 months (HR for PFS, 1.47 [95% CI 1.26–1.71], p < 0.001; HR for OS, 1.65 [95% CI 1.36–2.00], p < 0.001). HER2 status was not identified as a significant prognostic factor for PFS or OS based on the multivariable analysis, after adjustment for other variables (HR for PFS, 1.11 [95% CI 0.91–1.37], p = 0.311; HR for OS, 0.97 [95% CI 0.75–1.26], p = 0.820).
PSM was used to compare PFS and OS between the two groups; after propensity score matching, 146 patients in HER-2 positive group and 375 patients in HER-2 negative group were matched. The differences in baseline characteristics between the two groups were all eliminated after adjusting with PSM (Supplementary Table 3). In the matched group comparison, similar to the result of multivariable analysis, HER2 status was not a significant prognostic factor for PFS (HR, 1.14 [95% CI 0.92–1.41], p = 0.221) and OS (HR, 0.95 [95% CI 0.72–1.24], p = 0.692).
In patients with HER2-positive disease, four factors were independently associated with a poor prognosis (Supplementary Table 4): GEJ as the primary tumor (HR for PFS, 2.36 [95% CI 1.21–4.58], p = 0.011; HR for OS, 2.52 [95% CI 1.17–5.43], p = 0.019), presence of ascites (HR for PFS, 2.24 [95% CI 1.19–4.22], p = 0.013; HR for OS, 2.82 [95% CI 1.33–5.99], p = 0.007), no prior gastrectomy (HR for PFS, 1.96 [95% CI 1.29–2.97], p = 0.002), and time from first-line treatment to second-line treatment < 6 months (HR for PFS, 3.21 [95% CI 2.11–4.88], p < 0.001; HR for OS, 3.25 [95% CI 1.85–5.70], p < 0.001).
Discussion
This is the subgroup analysis of data from previous nationwide, retrospective study of ramucirumab plus paclitaxel in patients with gastric or GEJ adenocarcinoma, and to the best of our knowledge, this is the largest study comparing the efficacy and safety of second-line ramucirumab plus paclitaxel according to HER2 status in gastric cancer patients.
The ORR of patients with HER2-positive disease was significantly higher compared to patients with HER2-negative disease. However, a higher response to treatment did not lead to improvement in the PFS or OS. While the median PFS was numerically longer in patients with HER2-positive disease than in those without but, was not statistically significant. Although treatment duration (time from first-line treatment to second-line treatment) of fist-line treatment and the ORR to second-line treatment were significantly better in patients with HER2-positive disease, several predominant poor prognostic factors (GEJ adenocarcinoma, high disease burden) in HER2-positive gastric cancer patients may have influenced the survival outcomes.
With regard to treatment safety, the overall frequency of adverse events in this study was significantly lower than in the RAINBOW study; however, the adverse events were likely underestimated in this study since the data collection relied solely on electrical chart review. Stomatitis (≥ grade 3) and hypertension (all grades) were frequently reported in patients with HER2-positive disease, but the caution is needed in interpretation given the small number of adverse events reported.
In addition to our study, a few other recent retrospective studies [10, 11] examined the role of ramucirumab in patients with HER2-positive gastric cancer, and reported that ramucirumab containing treatments showed better efficacy outcomes in patients with HER2-positive disease; however, interpretation of the results of these studies is also limited due to the small number of patients enrolled.
After the approval of trastuzumab, a concerted effort was made to discover novel HER2-directed therapy for patients with HER2-positive gastric cancer. Based on the success in HER2-positive breast cancer, other HER2-targeting drugs, trastuzumab emtansine and lapatinib, were investigated in patients with HER2-positive gastric or GEJ cancer, but failed to demonstrate survival benefits in phase III trials [12, 13]. Continuing trastuzumab treatment beyond first-line treatment was also proposed, but this strategy also failed to improve survival outcomes in a recent randomized phase II study [14]. Despite these failures, several recent attempts to treat patients with HER2-positive gastric cancer have shown promising results. Trastuzumab deruxtecan, an HER2-targeting antibody–drug conjugate, significantly improved the treatment response and OS in a phase 2 trial of treatment-refractory HER2-positive gastric cancer [15] and a randomized phase 3 trial comparing trastuzumab deruxtecan to paclitaxel plus ramucirumab as a second-line treatment is ongoing [16]. In the 2021 American Society of Clinical Oncology annual meeting, the combination of a standard HER2-directed treatment and immune check-point inhibitor was reported to show promising results. Although this was a preliminary report of an ongoing phase 3 trial [17], pembrolizumab in combination with standard trastuzumab plus chemotherapy was associated with a substantial, statistically significant increase in ORR.
While further improvement in treatment outcomes is expected given recent study results, the development of a treatment strategy for HER2-positive gastric cancer appears to be more complex compared to breast cancer, for which treatments have been rapidly developed. Several factors, including tumor heterogeneity [18], loss of HER2 positivity after initial trastuzumab chemotherapy [19, 20], and an acquired resistance mechanism interacted by multiple signaling pathways [21], underlie the difficulty of developing an HER2-targeted treatment for gastric cancer.
The RTK-RAS-PI3K signaling pathway is the most well-known co-mutated pathway associated with HER2 overexpression [21]. As identified in breast cancer cell lines, complex interaction between downstream activation of angiogenic pathway and HER2 overexpression has been assumed as one of the structural mechanisms of trastuzumab resistance [6,7,8]. Considering the potential relationship between HER2 overexpression and angiogenesis in gastric cancer, a combination of anti-HER2 and anti-angiogenic agents could be one of strategies to improve survival outcomes in patients with HER2-positive gastric cancer. To test this hypothesis, a prospective phase Ib/II trial evaluating the combination of ramucirumab, trastuzumab and paclitaxel as a second-line treatment for HER2-positive gastric cancer is being conducted [22].
Combining our results with background rationales, it would be meaningful to reconsider the role of anti-VEGF antibody in HER2-positive gastric or GEJ cancer, which may contribute to broadening the therapeutic landscape for HER2-positive gastric or GEJ adenocarcinoma. The sequencing of biologic agents, toxicity concern of concomitant treatment, and appropriate patient selection should be addressed for future clinical studies.
The major limitation of this study is that this study was conducted retrospectively. With this limitation, the prognostic factors were unbalanced between the groups, and there is no obvious explanation for the fact that an increased ORR in patients with HER2-positive disease did not lead to improvements in PFS or OS. Receiving subsequent chemotherapy after progression to ramucirumab plus paclitaxel was associated with 50% reduction in the risk of death (HR for OS, 0.5 [95% CI 0.40–0.62], p < 0.001) in our study. However, the proportion of patients receiving treatment beyond second-line chemotherapy was similar in both groups, and it is not clear whether subsequent chemotherapy affects OS.
Conclusion
In conclusion, although limited by the retrospective nature of the study, subgroup analysis of data from KCSG-ST19-16 study showed that second-line treatment with ramucirumab plus paclitaxel is associated with a better treatment response in HER2-positive gastric or GEJ cancer patients. More robust studies are required to validate the potential role of ramucirumab in overcoming trastuzumab resistance.
References
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–424.
Hong S, Won YJ, Park YR, Jung KW, Kong HJ, Lee ES. Cancer statistics in Korea: incidence, mortality, survival, and prevalence in 2017. Cancer Res Treat. 2020;52:335–50.
Wilke H, Muro K, Van Cutsem E, Oh SC, Bodoky G, Shimada Y, et al. Ramucirumab plus paclitaxel versus placebo plus paclitaxel in patients with previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (RAINBOW): a double-blind, randomised phase 3 trial. Lancet Oncol. 2014;15:1224–35.
Van Cutsem E, Bang YJ, Feng-Yi F, Xu JM, Lee KW, Jiao SC, et al. HER2 screening data from ToGA: targeting HER2 in gastric and gastroesophageal junction cancer. Gastric Cancer. 2015;18:476–84.
Bang YJ, Van Cutsem E, Feyereislova A, Chung HC, Shen L, Sawaki A, et al. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): a phase 3, open-label, randomised controlled trial. Lancet. 2010;376:687–97.
Alameddine RS, Otrock ZK, Awada A, Shamseddine A. Crosstalk between HER2 signaling and angiogenesis in breast cancer: molecular basis, clinical applications and challenges. Curr Opin Oncol. 2013;25:313–24.
Klos KS, Wyszomierski SL, Sun M, Tan M, Zhou X, Li P, et al. ErbB2 increases vascular endothelial growth factor protein synthesis via activation of mammalian target of rapamycin/p70S6K leading to increased angiogenesis and spontaneous metastasis of human breast cancer cells. Cancer Res. 2006;66:2028–37.
Xiong S, Grijalva R, Zhang L, Nguyen NT, Pisters PW, Pollock RE, et al. Up-regulation of vascular endothelial growth factor in breast cancer cells by the heregulin-beta1-activated p38 signaling pathway enhances endothelial cell migration. Cancer Res. 2001;61:1727–32.
De Vita F, Borg C, Farina G, Geva R, Carton I, Cuku H, et al. Ramucirumab and paclitaxel in patients with gastric cancer and prior trastuzumab: subgroup analysis from RAINBOW study. Future Oncol. 2019;15:2723–31.
Tehfe M, Tabchi S, Laterza MM, Vita FD. Ramucirumab in HER-2-positive gastroesophageal adenocarcinoma: an argument for overcoming trastuzumab resistance. Future Oncol. 2018;14:223–8.
Sanchís AC, Gallego J, Hernandez R, Arrazubi V, Custodio A, Cano JM, et al. Second-line treatment in advanced gastric cancer: Data from the Spanish AGAMENON registry. PLoS ONE. 2020;15: e0235848.
Satoh T, Xu R-H, Chung HC, Sun GP, Doi T, Xu JM, et al. Lapatinib plus paclitaxel versus paclitaxel alone in the second-line treatment of HER2-amplified advanced gastric cancer in Asian populations: TyTAN–a randomized, phase III study. J Clin Oncol. 2014;32:2039–49.
Thuss-Patience PC, Shah MA, Ohtsu A, Van Cutsem E, Ajani JA, Castro H, et al. Trastuzumab emtansine versus taxane use for previously treated HER2-positive locally advanced or metastatic gastric or gastro-oesophageal junction adenocarcinoma (GATSBY): an international randomised, open-label, adaptive, phase 2/3 study. Lancet Oncol. 2017;18:640–53.
Makiyama A, Sukawa Y, Kashiwada T, Kawada J, Hosokawa A, Horie Y, et al. Randomized, phase II study of trastuzumab beyond progression in patients with HER2-positive advanced gastric or gastroesophageal junction cancer: WJOG7112G (T-ACT Study). J Clin Oncol. 2020;38:1919–27.
Shitara K, Bang YJ, Iwasa S, Sugimoto N, Ryu MH, Sakai D, et al. Trastuzumab deruxtecan in previously treated HER2-positive gastric cancer. N Engl J Med. 2020;382:2419–30.
Daiichi Sankyo, Inc. A phase 3, multicenter, 2-arm randomized, open-label study of trastuzumab deruxtecan in subjects with HER2-positive metastatic and/or unresectable gastric or gastro-esophageal junction (GEJ) adenocarcinoma subjects who have progressed on or after a trastuzumab-containing regimen (DESTINY-Gastric04). Available from: http://www.clinicaltrials.gov/ct2/show/NCT04704934
Merck Sharp & Dohme Corp. A phase III, randomized, double-blind trial comparing trastuzumab plus chemotherapy and pembrolizumab with trastuzumab plus chemotherapy and placebo as first-line treatment in participants with HER2 positive advanced gastric or gastroesophageal junction adenocarcinoma (KEYNOTE 811). Available from: http://www.clinicaltrials.gov/ct2/show/NCT03615326
Hofmann M, Stoss O, Shi D, Büttner R, van de Vijver M, Kim W, et al. Assessment of a HER2 scoring system for gastric cancer: results from a validation study. Histopathology. 2008;52:797–805.
Seo S, Ryu MH, Park YS, Ahn JY, Park Y, Park SR, et al. Loss of HER2 positivity after anti-HER2 chemotherapy in HER2-positive gastric cancer patients: results of the GASTric cancer HER2 reassessment study 3 (GASTHER3). Gastric Cancer. 2019;22:527–35.
Saeki H, Oki E, Kashiwada T, Arigami T, Makiyama A, Iwatsuki M, et al. Re-evaluation of HER2 status in patients with HER2-positive advanced or recurrent gastric cancer refractory to trastuzumab (KSCC1604). Eur J Cancer. 2018;105:41–9.
Janjigian YY, Sanchez-Vega F, Jonsson P, Chatila WK, Hechtman JF, Ku GY, et al. Genetic predictors of response to systemic therapy in esophagogastric cancer. Cancer Discov. 2018;8:49–58.
Yonsei University. An open-label, multicenter phase Ib/II study of ramucirumab in combination with trastuzumab and weekly paclitaxel in patients with HER2-positive recurrent/metastatic gastric cancer. Available from: http://www.clinicaltrials.gov/ct2/show/NCT04888663
Acknowledgements
This work was supported by the Health Insurance Review & Assessment Service (HIRA) and Korean Cancer Study Group (KCSG). We would like to thank all of the investigators and support staff who generously participated in this study.
Funding
This work was funded by the HIRA.
Author information
Authors and Affiliations
Contributions
Conceptualization: DYZ, SYR, HSH, MR, KL, DO. Data collection & curation: SYR, HSH, MR, SHP, JGK, WKB, KL, DO, DYZ. Formal analysis: HJ, YJS, HA. Methodology: DYZ, JB, DSK. Writing (original draft): BJK. Writing (review and editing): all authors.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest to disclose.
Ethical approval
This study was approved by the review boards of each participating institution. This study was a non-interventional retrospective study; therefore, written informed consent of patients was not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Kim, B.J., Jee, HJ., Rha, S.Y. et al. Ramucirumab plus paclitaxel as a second-line treatment in HER2-positive gastric cancer: subgroup analysis of a nationwide, real-world study in Korea (KCSG-ST19-16). Gastric Cancer 25, 609–618 (2022). https://doi.org/10.1007/s10120-021-01276-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10120-021-01276-4