
Abstract
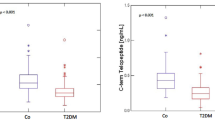
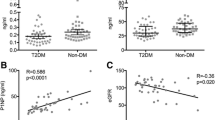
Few reports are available on bone turnover in type 2 diabetes. Impaired bone turnover in type 2 diabetes appears to result from decreased bone formation. Studies also suggest that poor glycaemic control in type 2 diabetes may contribute to osteopaenia. The aim of this study was to investigate biochemical markers of bone turnover in males with poorly controlled type 2 diabetes and look for correlations with glycaemic control and gonadal and hypophyseal hormonal axis. Consecutive male patients with poorly controlled type 2 diabetes and attending the internal medicine department during a period of 6 months were enrolled. The patients were receiving oral hypoglycaemic agents (metformin or sulphonylureas or both). None of the patients had any evidence of macroangiopathy, nephropathy or neuropathy. Only two patients had proliferative retinopathy. Serum osteocalcin, crosslaps (C-telopeptide, CTx), parathyroid hormone (PTH), testosterone, oestrogen, prolactin, follicle-stimulating hormone (FSH) and luteinising hormone (LH) were measured in 35 patients and 35 controls. The mean age of the study population was 53.7 (10.3) years (range: 50.2–57.3) and the mean disease duration was 8.6 (6.0) years (range: 6.5–10.7). No differences between patients and controls were observed in serum calcium, phosphorus, creatinine, albumin, PTH, CTx, oestrogen, testosterone, LH, FSH, prolactin and urinary calcium. Patients had lower serum levels of osteocalcin than controls with a significant statistical difference [15.3 (4.1) vs 18.3 (5.3), p=0.012]. There was a negative significant statistical correlation between CTx levels and HbA1c (r=−0.41, p< 0.05). Our study suggested that bone formation is altered in type 2 diabetes and that bone turnover is affected by glycaemic control status.

Similar content being viewed by others

References
Tohme JF, Seibel MJ, Silberberg SJ, Robins SP, Bilezikian JP (1991) Biochemical markers of bone metabolism. Z Rheumatol 50:135–151
Riis BJ (1993) Biochemical markers of bone turnover II: diagnosis, prophylaxis, and treatment of osteoporosis. Am J Med 95:17–24
Fugimoto D, Moriguchi T, Ishida T et al (1978) The structure of pyridinoline, a collagen crosslink. Biochem Biophys Res Commun 84:52–57
Uebelhart D, Gineyts E, Chapuy MC, Delmas PD (1990) Urinary excretion of pyridinium crosslinks: a new marker of bone resorption in metabolic bone disease. Bone Miner 8:87–96
El Maghraoui A, Borderie D, Edouard R, Roux C, Dougados M (1999) Osteoporosis, body composition and bone turnover in ankylosing spondylitis. J Rheumatol 26:2205–2209
Rico H, Hernandez ER, Cabranes JA, Gomez-Castresana F (1989) Suggestion of a deficient osteoblastic function in diabetes mellitus: the possible cause of osteopenia in diabetics. Calcif Tissue Int 45:71–73
Verhaeghe J, Visser WJ, Einhorn TA, Bouillon R (1990) Osteoporosis and diabetes: lessons from the diabetic BB rat. Horm Res 34:245–248
Montecucco C, Baldi F, Caporali R, Fortina A, Tomassini G, Caprotti M, Fratino P (1990) Serum osteocalcin (bone gla-protein) and bone mineral content in non-insulin dependent diabetes. Diabetes Nutr Metab 4:311–316
Cakatay U, Akcay T, Hacibekiroglu M, Ilkova H, Telci A (1995) Variations in serum osteocalcin levels in diabetic subjects. Med Sci Res 23:489–491
Cakatay U, Telci A, Kayah R, Akcay T, Sivas A, Aral F (1998) Changes in bone turnover on deoxypyridinoline levels in diabetic patients. Diabetes Res Clin Pract 40:75–79
Sayinalp S, Gedik O, Koray Z (1995) Increasing serum osteocalcin after glycemic control in diabetic men. Calcif Tissue Int 57:422–425
Rosato MT, Schneider SH, Shapses SA (1998) Bone turnover and insulin-like growth factor-1 levels increase after improved glycemic control in non insulin-dependent diabetes mellitus. Calcif Tissue Int 63:107–111
Nagasaka S, Murakami T, Uchikawa T, Ishikawa SE, Saito T (1995) Effect of glycemic control on calcium and phosphorus handling and parathyroid hormone in patients with non insulin-dependent diabetes mellitus. Endocr J 42:377–383
Okazaki R, Totsuka Y, Hamano K, Ajima M, Miura M, Hiruta Y et al (1997) Metabolic improvement of poorly controlled non insulin-dependent diabetes mellitus decreases bone turnover. J Clin Endocrinol Metab 82:2915–2920
Bertelloni S (1992) The parathyroid hormone ± 1, 25 ± dihydroxyvitamin D endocrine system and magnesium status in insulin-dependent diabetes mellitus: current concepts. Magnesium Res 5:45–51
Schedl HP, Heath H, Wenger J (1977) Serum calcitonin and parathyroid hormone in experimental diabetes: effects of insulin treatment. Endocrinology 103:1368–1373
Nyomba BL, Verhaeghe J, Thomasset M, Lissens W, Bouillon R (1989) Bone mineral homeostasis in spontaneously diabetic BB rats: abnormal vitamin D metabolism and impaired active intestinal calcium absorption. Endocrinology 124:565–572
Bouillon R, Bex M, Van Herk E et al (1995) Influence of age, sex and insulin on osteoblast function: osteoblast dysfunction in diabetes mellitus. J Clin Endocrinol Metabol 80:1194–1202
Pietschmann P, Schernthaner G, Woloszczuk W (1988) Serum osteocalcin levels in diabetes mellitus: analysis of the type of diabetes and microvascular complication. Diabetologia 31:892–895
Pouillés JM (2001) Os et diabète. Rev Rhum [Ed Fr] 68:718–720
Verhaeghe J, Suiker AMH, Visser WJ, Van Herk E, Van Bree R, Bouillon R (1992) The effects of systemic insulin, insulin like growth factor-1 and growth hormone on bone growth and turnover in spontaneously diabetic BB rats. J Endocrinol 134:485–492
Krakauer JC, McKenna MJ, Buderer NF et al (1995) Bone loss and bone turnover in diabetes. Diabetes 44:775–782
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Achemlal, L., Tellal, S., Rkiouak, F. et al. Bone metabolism in male patients with type 2 diabetes. Clin Rheumatol 24, 493–496 (2005). https://doi.org/10.1007/s10067-004-1070-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-004-1070-9