
Abstract
Background
An increasing number of patients have large or complex abdominal wall defects. Component separation technique (CST) is a very effective method for reconstructing complex midline abdominal wall defects in a manner that restores innervated muscle function without excessive tension. Our goal is to show our results by a modified CST for treating large ventral hernias.
Materials and methods
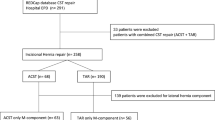
A total of 351 patients with complex ventral hernias have been treated over a 10-year period. Pre- and postoperative CT scans were performed in all patients. All ventral hernias were W3, according to the EHS classification 1. We analyzed demographic variables, co-morbidities, hernia characteristics, operative, and postoperative variables.
Results
One hundred and seventy patients (48.4%) were men; the average age of the study population was 51.6 ± 23.2 years with an average BMI of 32.3 ± 1.3. The hernia was located in the midline in 321 cases (91.5%) versus the flank in 30 (8.5%). In 45 patients, preoperative botulinum toxin (BT) and progressive pneumoperitoneum (PPP) were needed due to giant hernia defects when the VIH/VAC ratio was >20%. Postoperative complications related to the surgical site were seroma (35.1%), hematoma (9.1%), infection (7.2%), and wound necrosis (8.8%). Complications related to the repair were evisceration in 3 patients (1.1%), small bowel fistula in 4 patients (1.5%), 11 cases of mesh infection (2.9%), and abdominal compartment syndrome (ACS) in 2 patients. There were 29 hernia recurrences (8.2%) with a mean follow-up of 31.6 ± 8.1 months.
Conclusion
The modified CST is an effective strategy for managing complex ventral hernias that enables primary fascial closure with low rates of morbidity and hernia recurrence.



Similar content being viewed by others


References
den Hartog D, Dur AHM, Tuinebreijer WE, Kreis RW (2008) Open surgical procedures for incisional hernias. Cochrane Database Syst Rev (3), Article no CD006438. doi:10.1002/14651858.CD006438.pub2
Heller Lior, Colton McNichols H, Oscar Ramirez M (2012) Component Separations. Semin Plast Surg 26(1):25–28
Carbonell Tatay F, Bonafé Diana S, García Pastor P, Gómez i Gavara C, Baquero Valdelomar R (2009) Nuevo método de operar en la eventración compleja: separación anatómica de componentes con prótesis y nuevas inserciones musculares. Cir Esp (Ed impr) 86(2):87–93
Saulis AS, Dumanian GA (2002) Periumbilical rectus abdominis perforator preservation significantly reduces superficial wound complication in “separation of parts” hernia repairs. Plast Reconstr Surg 109(7):2275–2280 (discussion 2281–2282)
Sukkar SM, Dumanian GA, Szcerba SM, Tellez MG (2001) Challenging abdominal Wall defects. Am J Surg 181(2):115–121
Maas SM, van Engeland M, Leeksma NG, Bleichrodt RP (1999) A modification of the “components separation” technique for closure of abdominal Wall defects in the presence of an enterostomy. J Am Coll Surg 189(1):138–140
Lowe JB, Garza JR, Bowman JL, Rohrich RJ, Strodel WE (2000) Endoscopically assisted “components separation” for closure abdominal Wall defects. PlastReconstrSurg 105(2):731–738 (quiz 739)
Maas SM, deVries RS, vanGoor H, de Jong D, Bleichrodt R (2002) Endoscopically assisted “component separations technique” for the repair of complicated ventral hernias. J. Am Coll Surg 194(3):269–275 (discussion 275)
Fabian TC, Croce MA, Pritchard FE et al (1994) Planned ventral hernia. Staged management for acute abdominal Wall defects. Ann Surg 219(6):643–650 (discussion 651-653)
Ramirez OM, Ruas E, Dellon AL (1990) “Components separation” method for closure of abdominal-wall defects: an anatomic and clinical study. PlastReconstrSurg 86(3):519–526
Tanaka EY, Yoo JH, Rodrigues AJ Jr, Ultiyama EM, Birolini D, Rasslan S (2010) Computerized tomography scan method for calculating the hernia sac and abdominal cavity volume in complexlarge incisional hernia with loss of domain. Hernia 14:63–69
Sabbagh C, Dumont F, Robert B, Badaoui R, Verhaeghe P, Regimbeau JM (2011) Peritoneal volumen is predictive of tensión-free fascia closure of large incisional hernias with loss of domain: a prospective study. Hernia 15(5):559–565
Bueno-Lledó J, Torregrosa A, Ballester N et al (2017) Preoperative progressive pneumoperitoneum and botulinum toxin type A in patients with large incisional hernia. Hernia 21:233–243. doi:10.1007/s10029-017-1582-2
DiBello JN Jr (1996) Moore jrJH. Sliding myofascial flap of the rectus abdominus muscles for the closure of recurrent ventral hernias. Plast Reconstr Surg 98:464–469
Yegiyants S, Tam M, Lee DJ et al (2012) Outcome of components separation for contaminated complex abdominal wall defects. Hernia 16:41–45
Slater NJ, van der Kolk M, Hendricks T et al (2013) Biologic grafts for ventral hernia repair: a systematic review. Am J Surg 205:220–230
deVries Reilingh TS, van Goor H, Rosman C et al (2003) Components separation technique” for the repair of large abdominal Wall hernias. J Am Coll Surg 196:32–37
Slater NJ, van Goor H, Bleichrodt RP (2015) Large and complex ventral hernia repair using “components separation technique” without mesh results in a high recurrence rate. Am J Surg 209:170–179
de Vries Reilingh TS, van Goor H, Charbon JA, Rosman C, Hesselink EJ, van der Wilt GJ, Bleichrodt RP (2007) Repair of giant midline abdominal wall hernias: "components separation technique" versus prosthetic repair: interim analysis of a randomized controlled trial. World J Surg 31(4):756–763
Rosen MJ, Krpata DM, Ermlich B et al (2013) A 5-year clinical experience with single-staged repairs of infected and contaminated abdominal Wall defects utilizing biologic mesh. Ann Surg 257:991–996
Morris LM, LeBlanc KA (2013) Components separation technique utilizing an intraperitoneal biologic and an onlay lightweight polypropilene mesh: “a sándwich technique”. Hernia 17(1):45–51. doi:10.1007/s10029-012-0949-7
Agnew SP, Small W Jr, Wang E, Smith LJ, Hadad I, Dumanian GA (2010) Prospective measurements of intraabdominal volume and pulmonary function after repair of massive ventral hernias with the components separation technique. Ann Surg 251(5):981–988
Castellanos-Escrich G, Piñero-Madrona A (2012) Síndrome compartimental abdominal. In: Carbonell-Tatay F, Moreno-Egea A (eds) Eventraciones. Otras hernias de pared y cavidad abdominal. Ed. Vimar, Picanya
Goñi Moreno I (1946) Eventraciones crónicas y hernias voluminosas. Preparación para neumoperitoneo progresivo. Procedimiento original. Soc Argent Cir 30:1041–1053
Goñi Moreno I (1947) Chronic eventrations and large hernias. Preoperative treatment by progressive pneumoperitoneum. Original procedure. Surg 22:945–953
Goñi Moreno I (1940) Eventración crónica gigante preparada con neumoperitoneo y operada. Informe preliminar. In: Buenos Aires: XXII Congreso Argentino de Cirugía
Ibarra-Hurtado TR, Nuño-Guzmán CM, Echegaray-Herrera JE, Robles-Vélez E, González-Jaime JJ (2009) Use of botulinum toxin type A before abdominal wall hernia reconstruction. World J Surg 33:2553–2556
Novitsky YW, Elliott HL, Orenstein SB, Rosen MJ (2012) Tranversus abdominis muscle release: a novel approach to posterior component separation during complex abdominal wall reconstruction. Am J Surg 204:709–716
Krpata DM, Blatnik JA, Novitsky YW, Rosen MJ (2012) Posterior and anterior components separations: a comparative analysis. Am J Surg 203:318–322
Carbonell AM, Cobb WS, Chen SM (2008) Posterior components separation during retromuscular hernia repair. Hernia 12:359–362
Rosen MJ, Fatima J, Sarr MG (2010) Repair of abdominal wall hernias with restoration of abdominal wall function. J Gastrointest Surg 14:175–185
Pauli EM, Wang J, Petro CC, Juza RM, Novitsky YJ, Rosen MJ (2015) Posterior component separation with transversus abdominis release successfully addresses recurrent ventral hernias following anterior component separation. Hernia 19:285–291
Petro CC, Raigani S, Fayezizadeh M, Rowbottom JR, Klick JC, Prabhu AS, Novisky YW, Rosen MJ (2015) Permissible intra-abdominal hypertension following complex abdominal wall reconstruction. Plast Reconstr Surg 136(4):868–881
Carbonell F, Bonafé S (2012) Separación anatómica de componentes (SAC) con prótesis y nuevas inserciones musculares. In: Carbonell F, Moreno A Técnica de Carbonell-Bonafé. Eventraciones y otras hernias de pared y cavidad abdominal. AEC, Madrid
Acknowledgements
Thanks to Fernando Carbonell who created the Abdominal Wall Unit in our hospital and shared his advices and love for surgery. The authors also thanks Hobart W. Harris for his editorial input; he should be one more of the authors.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors declare that they have no conflicts of interests.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and /or national research commitee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Human and animal rights
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
For this type of study formal consent is not required.
Rights and permissions
About this article

Cite this article
Torregrosa-Gallud, A., Sancho Muriel, J., Bueno-Lledó, J. et al. Modified components separation technique: experience treating large, complex ventral hernias at a University Hospital. Hernia 21, 601–608 (2017). https://doi.org/10.1007/s10029-017-1619-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10029-017-1619-6