
Abstract
Purpose
Propofol and ketamine have become progressively popular in electroconvulsive therapy (ECT) anesthesia, although propofol shortened seizure duration and ketamine might cause cardiotoxicity, psychotic episodes, and delayed recovery. Ketofol is a combination of ketamine and propofol, and the current study was designed to evaluate the effect of ketamine, propofol, and ketofol on hemodynamic profile, duration of seizure activity, and recovery times in patients undergoing ECT.
Methods
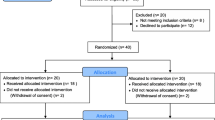
Ninety patients (44 women, mean age 27.8 ± 7.2 years) in one ECT session were enrolled and randomized to the propofol, ketamine, or ketofol group. Hemodynamic profile duration of seizure activity and recovery times were recorded.
Results
Motor seizure duration in the propofol group was significantly decreased compared to other groups (p < 0.001), whereas spontaneous breathing time in the ketamine group statistically increased compared to the propofol group (p = 0.001), and also eye-opening time (p < 0.001) and obeying-command time (p < 0.001) was significantly increased in the ketamine group compared to other groups. Heart rate (HR) at induction (ketamine 91.2 ± 13.6 vs. propofol 77 ± 13.4 and ketofol 79.9 ± 15.6; p < 0.013; p < 0.08, respectively) was statistically significantly increased in the ketamine group compared to other groups, and HR at the third minute (ketamine 92 ± 12.9 vs. propofol 79.4 ± 9.3 and ketofol 81.5 ± 14.2; p < 0.012, p < 0.048) was also statistically significantly increased in ketamine group compared to other groups.
Conclusion
The ketofol 1:1 mixture is associated with longer mean seizure time than propofol, and shorter mean recovery times than ketamine, with better hemodynamic stability, without any important side effects in ECT anesthesia.


Similar content being viewed by others


References
Ding Z, White PF. Anesthesia for electroconvulsive therapy. Anesth Analg. 2002;94:1351–64.
Mizrak A, Koruk S, Ganidagli S, Bulut M, Oner U. Premedication with dexmedetomidine and midazolam attenuates agitation after electroconvulsive therapy. J Anesth. 2009;23:6–10.
Bowley CJ, Walker HAC. Anaesthesia for ECT. In: Scott AIF, editor. The ECT handbook. 2nd ed. London: Royal College of Psychiatrists; 2005. p. 124–35.
Hooten WM, Rasmussen KG Jr. Effects of general anesthetic agents in adults receiving electroconvulsive therapy: a systematic review. J ECT. 2008;24:208–23.
Patel AS, Gorst-Unsworth C, Venn RM, Kelley K, Jacob Y. Anesthesia and electroconvulsive therapy: a retrospective study comparing etomidate and propofol. J ECT. 2006;22:179–83.
Mitchell P, Torda T, Hickie I, Burke C. Propofol as an anaesthetic agent for ECT: effect on outcome and length of course. Aust N Z J Psychiatry. 1991;25:255–61.
Rosa MA, Rosa MO, Marcolin MA, Fregni F. Cardiovascular effects of anesthesia in ECT: a randomized, double-blind comparison of etomidate, propofol, and thiopental. J ECT. 2007;23:6–8.
Okamoto N, Nakai T, Sakamoto K, Nagafusa Y, Higuchi T, Nishikawa T. Rapid antidepressant effect of ketamine anesthesia during electroconvulsive therapy of treatment-resistant depression: comparing ketamine and propofol anesthesia. J ECT. 2010;26:223–7.
Rasmussen KG, Jarvis MR, Zorumski CF. Ketamine anesthesia in electroconvulsive therapy. Convuls Ther. 1996;12:217–23.
Green SM, Andolfatto G, Krauss B. Ketofol for procedural sedation? Pro and con. Ann Emerg Med. 2011;57:444–8.
Petrides G, Fink M. The “half-age” stimulation strategy for ECT dosing. Convuls Ther. 1996;12:138–46.
Willman EV, Andolfatto G. A prospective evaluation of ‘‘Ketofol’’ (ketamine/propofol combination) for procedural sedation and analgesia in the emergency department. Ann Emerg Med. 2007;49:23–30.
Botero CA, Smith CE, Holbrook C, Chavez AM, Snow NJ, Hagen JF, Pinchak AC. Total intravenous anesthesia with a propofol–ketamine combination during coronary artery surgery. J Cardiothorac Vasc Anesth. 2000;14:409–15.
Tosun Z, Esmaoglu A, Coruh A. Propofol–ketamine vs. propofol–fentanyl combinations for deep sedation and analgesia in pediatric patients undergoing burn dressing changes. Pediatr Anesth. 2008;18:43–7.
Erden IA, Pamuk AG, Akinci SB, Koseoglu A, Aypar U. Comparison of propofol–fentanyl with propofol–fentanyl–ketamine combination in pediatric patients undergoing interventional radiology procedures. Pediatr Anesth. 2009;19:500–6.
Frizelle HP, Duranteau J, Samii K. A comparison of propofol with a propofol–ketamine combination for sedation during spinal anesthesia. Anesth Analg. 1997;84:1318–22.
Akin A, Guler G, Esmaoglu A, Bedirli N, Boyaci A. A comparison of fentanyl–propofol with a ketamine–propofol combination for sedation during endometrial biopsy. J Clin Anesth. 2005;17:187–90.
Frey K, Sukhani R, Pawlowski J, Pappas AL, Mikat-Stevens M, Slogoff S. Propofol versus propofol ketamine for retrobulbar nerve block: comparison of sedation quality, intraocular pressure changes, and recovery profiles. Anesth Analg. 1999;89:317–21.
Aouad MT, Moussa AR, Dagher CM, Muwakkit SA, Jabbour-Khoury SI, Zbeidy RA, Abboud MR, Kanazi GE. Addition of ketamine to propofol for initiation of procedural anesthesia in children reduces propofol consumption and preserves hemodynamic stability. Acta Anaesthesiol Scand. 2008;52:561–5.
Weatherall A, Venclovas R. Experince with a propofol–ketamine mixture for sedation during pediatric orthopedic surgery. Pediatr Anesth. 2010;20:1009–16.
Donnelly RF, Willman E, Andolfatto G. Stability of ketamine–propofol mixtures for procedural sedation and analgesia in the emergency department. Can J Hosp Pharm. 2008;61:426–30.
Strayer RJ, Nelson LS. Adverse events associated with ketamine for procedural sedation in adults. Am J Emerg Med. 2008;26:985–1028.
Shah A, Mosdossy G, McLeod S, Lehnhardt K, Peddle M, Rieder M. A blinded, randomized controlled trial to evaluate ketamine/propofol versus ketamine alone for procedural sedation in children. Ann Emerg Med. 2011;57:425–33.
Green S. Research advances in procedural sedation and analgesia. Ann Emerg Med. 2007;49:31–6.
Berman RM, Cappiello A, Anand A, Oren DA, Heninger GR, Charney DS, Krystal JH. Antidepressant effects of ketamine in depressed patients. Biol Psychiatry. 2000;47:351–4.
Zarate CA Jr, Singh JB, Carlson PJ, Brutsche NE, Ameli R, Luckenbaugh DA, Charney DS, Manji HK. A randomized trial of an N-methyl-d-aspartate antagonist in treatment-resistant major depression. Arch Gen Psychiatry. 2006;63:856–64.
Kranaster L, Kammerer-Ciernioch J, Hoyer C, Sartorius A. Clinically favourable effects of ketamine as an anaesthetic for electroconvulsive therapy: a retrospective study. Eur Arch Psychiatry Clin Neurosci. 2011;261:575–82.
Ostroff R, Gonzales M, Sanacora G. Antidepressant effect of ketamine during ECT. Am J Psychiatry. 2005;162:1385–6.
Goforth HW, Holsinger T. Rapid relief of severe major depressive disorder by use of preoperative ketamine and electroconvulsive therapy. J ECT. 2007;23:23–5.
McDaniel WW, Sahota AK, Vyas BV, Laguerta N, Hategan L, Oswald J. Ketamine appears associated with better word recall than etomidate after a course of 6 electroconvulsive therapies. J ECT. 2006;22:103–6.
Adell A, Jiménez-Sánchez L, López-Gil X, Romón T. Is the acute NMDA receptor hypofunction a valid model of schizophrenia? Schizophr Bull. 2012;38:9–14.
Malhotra AK, Pinals DA, Adler CM, Elman I, Clifton A, Pickar D, Breier A. Ketamine-induced exacerbation of psychotic symptoms and cognitive impairment in neuroleptic-free schizophrenics. Neuropsychopharmacology. 1997;17:141–50.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Yalcin, S., Aydoğan, H., Selek, S. et al. Ketofol in electroconvulsive therapy anesthesia: two stones for one bird. J Anesth 26, 562–567 (2012). https://doi.org/10.1007/s00540-012-1378-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00540-012-1378-6