
Abstract
Background
Optimal resource utilization in high-cost environments like operating theatres is fundamental in today’s cost constrained health care systems. Interruptions of the surgical workflow, i.e. microcomplications (MC), lead to prolonged procedure times and higher costs and can be indicative of surgical mistakes. Reducing MC can improve operating room efficiency and prevent intraoperative complications. We, therefore, aimed to evaluate the impact of a high-resolution standardized laparoscopic cholecystectomy protocol (HRSL) on operative time and intraoperative interruptions in a teaching hospital.
Methods
HRSL consisted of a detailed stepwise protocol for the procedure, supported by a teaching video, both to be reviewed as mandatory preparation by each team member before surgery. Audio–video records of laparoscopic cholecystectomies were reviewed regarding type, frequency and duration of MC before and after implementation of HRSL.
Results
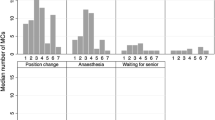
Thirty-nine (20 control and 19 HRSL) audio–video records of laparoscopic cholecystectomies with a total duration of 51.36 h (28.92 pre 22.44 post) were reviewed. The majority of operations (86%) were performed by teams who had completed less than 10 procedures together previously. Communication-related interruptions and instrument changes accounted for the majority of MC. Median frequency and duration of MC were 95 events/h and 15.6 min/h, respectively, of surgery pre-intervention. With HRSL this was reduced to 76 events/h and 10.6 min/h of operating. In multivariable analysis, HRSL was an independent predictor for shorter delay and lower frequency of MC [percentage decrease 27% (95% CI 18–35%), resp. 30% (95% CI 19–40%)]. Procedure-related risk factors for the longer delay due to MC in multivariable analysis were less experience of the surgeon and intraoperative adhesiolysis.
Conclusions
HRSL is effective in reducing delays due to MC in a teaching institution with limited team experience. These findings should be tested in larger potentially cluster-randomized controlled trials.
The trial has been registered with clinicaltrials.gov: NCT03329859.

Similar content being viewed by others


References
Weiser T, Haynes A, Molina G, Lipsitz S, Esquivel M, Uribe-Leitz T, Fu R, Azad T, Chao T, Berry W, Gawande A (2015) Estimate of the global volume of surgery in 2012: an assessment supporting improved health outcomes. Lancet 385(Suppl 2):S11
Gonzalez AA, Dimick JB, Birkmeyer JD, Ghaferi AA (2014) Understanding the volume-outcome effect in cardiovascular surgery: the role of failure to rescue. JAMA Surg 149:119–123
Arriaga AF, Lancaster RT, Berry WR, Regenbogen SE, Lipsitz SR, Kaafarani HM, Elbardissi AW, Desai P, Ferzoco SJ, Bleday R, Breen E, Kastrinakis WV, Rubin MS, Gawande AA (2009) The better colectomy project: association of evidence-based best-practice adherence rates to outcomes in colorectal surgery. Ann Surg 250:507–513
Haugen AS, Softeland E, Almeland SK, Sevdalis N, Vonen B, Eide GE, Nortvedt MW, Harthug S (2015) Effect of the World Health Organization checklist on patient outcomes: a stepped wedge cluster randomized controlled trial. Ann Surg 261:821–828
Haynes A, Weiser T, Berry W, Lipsitz S, Breizat A, Dellinger E, Herbosa T, Joseph S, Kibatala P, Lapitan M, Merry A, Moorthy K, Reznick R, Taylor B, Gawande A (2009) A surgical safety checklist to reduce morbidity and mortality in a global population. N Engl J Med 360:491–499
Nicolay C, Purkayastha S, Greenhalgh A, Benn J, Chaturvedi S, Phillips N, Darzi A (2012) Systematic review of the application of quality improvement methodologies from the manufacturing industry to surgical healthcare. Br J Surg 99:324–335
Weiser T, Haynes A, Dziekan G, Berry W, Lipsitz S, Gawande A (2010) Effect of a 19-item surgical safety checklist during urgent operations in a global patient population. Ann Surg 251:976–980
Balayla J, Bergman S, Ghitulescu G, Feldman LS, Fraser SA (2012) Knowing the operative game plan: a novel tool for the assessment of surgical procedural knowledge. Can J Surg 55:S158–162
Madani A, Watanabe Y, Feldman LS, Vassiliou MC, Barkun JS, Fried GM, Aggarwal R (2015) Expert intraoperative judgment and decision-making: defining the cognitive competencies for safe laparoscopic cholecystectomy. J Am Coll Surg 221:931–940, e938
Watanabe Y, Bilgic E, Lebedeva E, McKendy KM, Feldman LS, Fried GM, Vassiliou MC (2016) A systematic review of performance assessment tools for laparoscopic cholecystectomy. Surg Endosc 30:832–844
Mechera R, Dell-Kuster S, von Strauss Und Torney M, Langer I, Furrer M, Bucher HC, Rosenthal R (2017) Tutorial assistance for board certification in surgery: frequency, associated time and cost. World J Surg 41:1950–1960
von Strauss Und Torney M, Dell-Kuster S, Mechera R, Rosenthal R, Langer I (2012) The cost of surgical training: analysis of operative time for laparoscopic cholecystectomy. Surg Endosc 26:2579–2586
Brennan TA, Gawande A, Thomas E, Studdert D (2005) Accidental deaths, saved lives, and improved quality. N Engl J Med 353:1405–1409
Cendan J, Good M (2006) Interdisciplinary work flow assessment and redesign decreases operating room turnover time and allows for additional caseload. Arch Surg 141:65–69 (discussion 70)
Hanss R, Buttgereit B, Tonner P, Bein B, Schleppers A, Steinfath M, Scholz J, Bauer M (2005) Overlapping induction of anesthesia: an analysis of benefits and costs. Anesthesiology 103:391–400
Sokolovic E, Biro P, Wyss P, Werthemann C, Haller U, Spahn D, Szucs T (2002) Impact of the reduction of anaesthesia turnover time on operating room efficiency. Eur J Anaesthesiol 19:560–563
Lingard L, Espin S, Whyte S, Regehr G, Baker G, Reznick R, Bohnen J, Orser B, Doran D, Grober E (2004) Communication failures in the operating room: an observational classification of recurrent types and effects. Qual Saf Health Care 13:330–334
Ahmed K, Aydin A, Dasgupta P, Khan MS, McCabe JE (2015) A novel cadaveric simulation program in urology. J Surg Educ 72:556–565
Arora S, Aggarwal R, Sevdalis N, Moran A, Sirimanna P, Kneebone R, Darzi A (2010) Development and validation of mental practice as a training strategy for laparoscopic surgery. Surg Endosc 24:179–187
Grantcharov T, Kristiansen V, Bendix J, Bardram L, Rosenberg J, Funch-Jensen P (2004) Randomized clinical trial of virtual reality simulation for laparoscopic skills training. Br J Surg 91:146–150
Immenroth M, Burger T, Brenner J, Nagelschmidt M, Eberspacher H, Troidl H (2007) Mental training in surgical education: a randomized controlled trial. Ann Surg 245:385–391
Vine SJ, Masters RS, McGrath JS, Bright E, Wilson MR (2012) Cheating experience: guiding novices to adopt the gaze strategies of experts expedites the learning of technical laparoscopic skills. Surgery 152:32–40
Wilson M, Vine S, Bright E, Masters R, Defriend D, McGrath J (2011) Gaze training enhances laparoscopic technical skill acquisition and multi-tasking performance: a randomized, controlled study. Surg Endosc 25:3731–3739
Strauss G, Schmitz P (2016) Standardization and modeling of surgical processes. Chirurg 87:1008–1014
Healey T, Peterson T, Healey J, El-Othmani M, Saleh K (2015) Improving operating room efficiency, part 2: intraoperative and postoperative strategies. JBJS Rev. https://doi.org/10.2106/JBJS.RVW.N.00110
von Strauss Und Torney M, Dell-Kuster S, Hoffmann H, von Holzen U, Oertli D, Rosenthal R (2016) Microcomplications in laparoscopic cholecystectomy: impact on duration of surgery and costs. Surg Endosc 30:2512–2522
Strasberg SM, Hertl M, Soper NJ (1995) An analysis of the problem of biliary injury during laparoscopic cholecystectomy. J Am Coll Surg 180:101–125
Zeger S, Liang K (1988) Models for longitudinal data: a generalized estimating equation approach. Biometrics 44:1049–1060
Swiss DRG AG (2014) Swiss DRG Grouper. Bern [13.11.2017]. Available from https://grouper.swissdrg.org/swissdrg/single?locale=de
Fong A, Smith M, Langerman A (2016) Efficiency improvement in the operating room. J Surg Res 204:371–383
Attarian DE, Wahl JE, Wellman SS, Bolognesi MP (2013) Developing a high-efficiency operating room for total joint arthroplasty in an academic setting. Clin Orthop Relat Res 471:1832–1836
Krasner H, Connelly NR, Flack J, Weintraub A (1999) A multidisciplinary process to improve the efficiency of cardiac operating rooms. J Cardiothorac Vasc Anesth 13:661–665
Chalian AA, Kagan SH, Goldberg AN, Gottschalk A, Dakunchak A, Weinstein GS, Weber RS (2002) Design and impact of intraoperative pathways for head and neck resection and reconstruction. Arch Otolaryngol Head Neck Surg 128:892–896
Iannettoni MD, Lynch WR, Parekh KR, McLaughlin KA (2011) Kaizen method for esophagectomy patients: improved quality control, outcomes, and decreased costs. Ann Thorac Surg 91:1011–1017 (discussion 1017–1018)
Mason SE, Nicolay CR, Darzi A (2015) The use of Lean and Six Sigma methodologies in surgery: a systematic review. Surgeon 13:91–100
Iwashita Y, Hibi T, Ohyama T, Honda G, Yoshida M, Miura F, Takada T, Han HS, Hwang TL, Shinya S, Suzuki K, Umezawa A, Yoon YS, Choi IS, Huang WS, Chen KH, Watanabe M, Abe Y, Misawa T, Nagakawa Y, Yoon DS, Jang JY, Yu HC, Ahn KS, Kim SC, Song IS, Kim JH, Yun SS, Choi SH, Jan YY, Shan YS, Ker CG, Chan DC, Wu CC, Lee KT, Toyota N, Higuchi R, Nakamura Y, Mizuguchi Y, Takeda Y, Ito M, Norimizu S, Yamada S, Matsumura N, Shindoh J, Sunagawa H, Gocho T, Hasegawa H, Rikiyama T, Sata N, Kano N, Kitano S, Tokumura H, Yamashita Y, Watanabe G, Nakagawa K, Kimura T, Yamakawa T, Wakabayashi G, Mori R, Endo I, Miyazaki M, Yamamoto M (2017) An opportunity in difficulty: Japan-Korea-Taiwan expert Delphi consensus on surgical difficulty during laparoscopic cholecystectomy. J Hepatobiliary Pancreat Sci 24:191–198
Acknowledgements
The authors want to thank Charles Rudin for his technical support and advice in audio–video recording and preparing the audio–video records for analysis and Alistair Geraghty for his careful and critical review of the manuscript as native speaker.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Rachel Rosenthal is an employee of F. Hoffmann-La Roche Ltd. since 01 May 2014. The present study has no connection to her employment by the company. Rachel Rosenthal continues to be affiliated with the University of Basel. Marco von Strauss und Torney, Sohelia Aghlmandi, Jasmin Zeindler, Debora Senn, Christian Nebiker, Christoph Kettelhack, Raoul Droeser, Savas Soysal, Henry Hoffmann and Robert Mechera have no conflict of interest or financial ties to disclose.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplemental digital content (SDC 5) (MP4 26955 KB)
Rights and permissions
About this article

Cite this article
von Strauss und Torney, M., Aghlmandi, S., Zeindler, J. et al. High-resolution standardization reduces delay due to workflow disruptions in laparoscopic cholecystectomy. Surg Endosc 32, 4763–4771 (2018). https://doi.org/10.1007/s00464-018-6224-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-018-6224-y