
Abstract
Background
Preoperative nutritional supplementation, management of esophageal leaks, and postoperative anastomotic strictures still remain common problems in the management of esophageal cancer. Jejunal feeding tubes, total parenteral nutrition (TPN) with nasogastric suction, and repeated esophageal dilations remain the most common treatments, respectively. The aim of this study was to evaluate the use of removable silicone stents in (1) the preoperative nutritional optimization during neoadjuvant therapy, (2) the management of perioperative anastomotic leak, and (3) the management of postoperative anastomotic strictures.
Methods
Review of our prospectively maintained esophageal database identified 15 patients who had removable self-expanding silicone stents placed in the management of one of these three management problems from July 2004 to August 2006.
Results
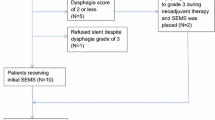
Preoperative therapy: Five patients underwent initial stent placement in preparation for neoadjuvant therapy. Dysphagia relief was seen in 100% of patients, with optimal caloric needs taken within 24 h of placement. All patients tolerated neoadjuvant therapy without delay from dehydration or malnutrition. One stent migration was found at the time of operation, which was removed without sequelae. Perioperative therapy: Five patients developed delayed (>10 days) esophageal leaks that were managed with removable esophageal stent and percutaneous drainage (in three patients). All patients had successful exclusion of the leak on the day of the procedure with resumption of oral intake on the evening of procedure. All five healed leaks without sequelae. Postoperative therapy: Five patients developed postoperative anastomotic strictures that required dilation and placement of removable esophageal stent. The median number of dilations was 1 (range 1–2), with all stents placed for approximate 3 months duration. All patients had immediate dysphagia relief after stent placement.
Conclusion
Removable esophageal stents are novel treatment option to optimize relief of symptoms and return the patients back to a more normal oral intake. Continued evaluation is needed to consider stent use as first-line therapy.


Similar content being viewed by others

References
Baquet CR, Commiskey P, Mack K et al (2005) Esophageal cancer epidemiology in blacks and whites: racial and gender disparities in incidence, mortality, survival rates and histology. J Natl Med Assoc 97:1471–1478
Anderson MR, Jankowski JA (2001) The treatment, management and prevention of oesophageal cancer. Expert Opin Biol Ther 1:1017–1028
Ellul JP, Watkinson A, Khan RJ et al (1995) Self-expanding metal stents for the palliation of dysphagia due to inoperable oesophageal carcinoma. Br J Surg 82:1678–1681
Aiko S, Yoshizumi Y, Sugiura Y et al (2001) Beneficial effects of immediate enteral nutrition after esophageal cancer surgery. Surg Today 31:971–978
Nozoe T, Kimura Y, Ishida M et al (2002) Correlation of pre-operative nutritional condition with post-operative complications in surgical treatment for oesophageal carcinoma. Eur J Surg Oncol 28:396–400
Decker P, Lippler J, Decker D et al (2001) Use of the Polyflex stent in the palliative therapy of esophageal carcinoma: results in 14 cases and review of the literature. Surg Endosc 15:1444–1447
Thompson AM, Rapson T, Gilbert FJ et al (2004) Endoscopic palliative treatment for esophageal and gastric cancer: techniques, complications, and survival in a population-based cohort of 948 patients. Surg Endosc 18:1257–1262
Costamagna G, Shah SK, Tringali A et al (2003) Prospective evaluation of a new self-expanding plastic stent for inoperable esophageal strictures. Surg Endosc 17:891–895
Urschel JD (1995) Esophagogastrostomy anastomotic leaks complicating esophagectomy: a review. Am J Surg 169:634–640
Repici A, Romagnoli R, Reggio D et al (2002) Successful closure of a postsurgical benign esophagomediastinal fistula by temporary placement of a polyester, expandable stent: case report and review. Gastrointest Endosc 56:747–750
Pross M, Manger T, Reinheckel T et al (2000) Endoscopic treatment of clinically symptomatic leaks of thoracic esophageal anastomoses. Gastrointest Endosc 51:73–76
Eleftheriadis E, Kotzampassi K (2005) Temporary stenting of acquired benign tracheoesophageal fistulas in critically ill ventilated patients. Surg Endosc 19:811–815
van Lanschot JJ, van Blankenstein M, Oei HY et al (1999) Randomized comparison of prevertebral and retrosternal gastric tube reconstruction after resection of oesophageal carcinoma. Br J Surg 86:102–108
Walther B, Johansson J, Johnsson F et al (2003) Cervical or thoracic anastomosis after esophageal resection and gastric tube reconstruction: a prospective randomized trial comparing sutured neck anastomosis with stapled intrathoracic anastomosis. Ann Surg 238:803–812
Zieren HU, Muller JM, Pichlmaier H (1993) Prospective randomized study of one- or two-layer anastomosis following oesophageal resection and cervical oesophagogastrostomy. Br J Surg 80:608–611
Urschel JD, Urschel DM, Miller JD et al (2001) A meta-analysis of randomized controlled trials of route of reconstruction after esophagectomy for cancer. Am J Surg 182:470–475
Behzadi A, Nichols FC, Cassivi SD et al (2005) Esophagogastrectomy: the influence of stapled versus hand-sewn anastomosis on outcome. J Gastrointest Surg 9:1031–1040
Repici A, Conio M, De Angelis C et al (2004) Temporary placement of an expandable polyester silicone-covered stent for treatment of refractory benign esophageal strictures. Gastrointest Endosc 60:513–519
Evrard S, Le Moine O, Lazaraki G et al (2004) Self-expanding plastic stents for benign esophageal lesions. Gastrointest Endosc 60:894–900
Mellow MH, Pinkas H (1984) Endoscopic therapy for esophageal carcinoma with Nd:YAG laser: prospective evaluation of efficacy, complications, and survival. Gastrointest Endosc 30:334–339
Sax HC (2005) Immunonutrition and upper gastrointestinal surgery: what really matters. Nutr Clin Pract 20:540–543
Patil PK, Patel SG, Mistry RC et al (1992) Cancer of the esophagus: esophagogastric anastomotic leak–a retrospective study of predisposing factors. J Surg Oncol 49:163–167
Dewar L, Gelfand G, Finley RJ et al (1992) Factors affecting cervical anastomotic leak and stricture formation following esophagogastrectomy and gastric tube interposition. Am J Surg 163:484–489
Langer FB, Wenzl E, Prager G et al (2005) Management of postoperative esophageal leaks with the Polyflex self-expanding covered plastic stent. Ann Thorac Surg 79:398–403
Truong S, Bohm G, Klinge U et al (2004) Results after endoscopic treatment of postoperative upper gastrointestinal fistulas and leaks using combined Vicryl plug and fibrin glue. Surg Endosc 18:1105–1108
Urschel JD, Urschel DM, Miller JD et al (2001) A meta-analysis of randomized controlled trials of route of reconstruction after esophagectomy for cancer. Am J Surg 182:470–475
Johansson J, Zilling T, Von Holstein CS et al (2000) Anastomotic diameters and strictures following esophagectomy and total gastrectomy in 256 patients. World J Surg 24:78–84
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Martin, R., Duvall, R., Ellis, S. et al. The use of self-expanding silicone stents in esophageal cancer care: optimal pre-, peri-, and postoperative care. Surg Endosc 23, 615–621 (2009). https://doi.org/10.1007/s00464-008-9851-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-008-9851-x