
Abstract
Background
Radical antegrade modular pancreatosplenectomy (RAMPS) has been propagated as the standard of care for pancreatic cancers involving the body and tail of the pancreas. This procedure has been shown to have promising results in enhancing the microscopically negative tangential resection margins as well as the lymph node yield.
Methods
This is a retrospective analysis of prospectively maintained database on the resections performed for all pancreatic body and tail tumors at Tata Memorial Centre.
Results
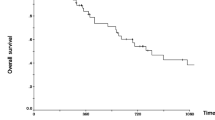
Sixty-five patients underwent RAMPS without any perioperative mortality. The various pathologies comprised of adenocarcinoma (41.5%), neuroendocrine tumors (12.3%), solid pseudopapillary epithelial neoplasm (15.3%), cystic neoplasms (15.2%), etc. The R0 resection rate was 87.7%. Among this cohort, 27 patients had pancreatic adenocarcinoma. The 3-year OS and DFS for distal pancreatic cancers were 56% and 38%, respectively, but 3-year OS and DFS for other distal pancreatic tumors were 97% and 73%, respectively. On multivariate analysis, R0 resection significantly improved disease-free survival (p = 0.023) for pancreatic cancer.
Conclusion
RAMPS procedure aids to achieve high negative tangential margins for all tumors involving the body and tail of the pancreas and not just pancreatic cancer in isolation. Since preoperative histologic diagnosis is not routinely indicated and also a number of other distal pancreatic tumors carry a relatively better prognosis compared with pancreatic cancer, our results provide further evidence that RAMPS should be considered as the procedure of choice for all operable tumors involving body and tail of the pancreas.


Similar content being viewed by others


References
Strasberg SM, Drebin JA, Linehan D (2003) Radical antegrade modular pancreatosplenectomy. Surgery 133:521–527
Mitchem JB, Hamilton N, Gao F, Hawkins WG, Linehan DC, Strasberg SM (2012) Long-term results of resection of adenocarcinoma of the body and tail of the pancreas using radical antegrade modular pancreatosplenectomy procedure. J Am Coll Surg 214:46–52
O’Morchoe CC (1997) Lymphatic system of the pancreas. Microsc Res Tech 37:456–477
Bassi C, Marchegiani G, Dervenis C, Sarr M, Abu Hilal M, Adham M, Allen P, Andersson R, Asbun HJ, Besselink MG, Conlon K, del Chiaro M, Falconi M, Fernandez-Cruz L, Fernandez-del Castillo C, Fingerhut A, Friess H, Gouma DJ, Hackert T, Izbicki J, Lillemoe KD, Neoptolemos JP, Olah A, Schulick R, Shrikhande SV, Takada T, Takaori K, Traverso W, Vollmer CR, Wolfgang CL, Yeo CJ, Salvia R, Buchler M (2017) The 2016 update of the international study group (ISGPS) definition and grading of postoperative pancreatic fistula: 11 years after. Surgery 161:584–591
Clavien PA, Barkun J, de Oliveira ML, Vauthey JN, Dindo D, Schulick RD, de Santibañes E, Pekolj J, Slankamenac K, Bassi C, Graf R, Vonlanthen R, Padbury R, Cameron JL, Makuuchi M (2009) The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg 250:187–196
Barreto SG, Shukla PJ, Shrikhande SV (2010) Tumors of the pancreatic body and tail. World J Oncol 1:52–65
Brennan MF, Moccia RD, Klimstra D (1996) Management of adenocarcinoma of the body and tail of the pancreas. Ann Surg 223:506–511
Sperti C, Pasquali C, Pedrazzoli S (1997) Ductal adenocarcinoma of the body and tail of the pancreas. J Am Coll Surg 185:255–259
Shrikhande SV, Sivasanker M, Vollmer CM, Friess H, Besselink MG, Fingerhut A, Yeo CJ, Fernandez-delCastillo C, Dervenis C, Halloran C, Gouma DJ, Radenkovic D, Asbun HJ, Neoptolemos JP, Izbicki JR, Lillemoe KD, Conlon KC, Fernandez-Cruz L, Montorsi M, Bockhorn M, Adham M, Charnley R, Carter R, Hackert T, Hartwig W, Miao Y, Sarr M, Bassi C, Büchler MW (2017) Pancreatic anastomosis after pancreatoduodenectomy: a position statement by the International Study Group of Pancreatic Surgery (ISGPS). Surgery 161:1221–1234
Strasberg SM, Fields R (2012) Left-sided pancreatic cancer: distal pancreatectomy and its variants: radical antegrade modular pancreatosplenectomy and distal pancreatectomy with celiac axis resection. Cancer J 18:562–570
Strasberg SM, Linehan DC, Hawkins WG (2007) Radical antegrade modular pancreatosplenectomy procedure for adenocarcinoma of the body and tail of the pancreas: ability to obtain negative tangential margins. J Am Coll Surg 204:244–249
Shimada K, Sakamoto Y, Sano T, Kosuge T (2006) Prognostic factors after distal pancreatectomy with extended lymphadenectomy for invasive pancreatic adenocarcinoma of the body and tail. Surgery 139:288–295
Christein JD, Kendrick ML, Iqbal CW, Nagorney DM, Farnell MB (2005) Distal pancreatectomy for resectable adenocarcinoma of the body and tail of the pancreas. J Gastrointest Surg 9:922–927
Kooby DA, Hawkins WG, Schmidt CM, Weber SM, Bentrem DJ, Gillespie TW et al (2010) A multicenter analysis of distal pancreatectomy for adenocarcinoma: is laparoscopic resection appropriate? J Am Coll Surg 210(779–85):786–787
Kanda M, Fujii T, Sahin TT, Kanzaki A, Nagai S, Yamada S et al (2010) Invasion of the splenic artery is a crucial prognostic factor in carcinoma of the body and tail of the pancreas. Ann Surg 251:483–487
Yamamoto J, Saiura A, Koga R, Seki M, Katori M, Kato Y, Sakamoto Y, Kokudo N, Yamaguchi T (2010) Improved survival of left-sided pancreas cancer after surgery. Jpn J Clin Oncol 40:530–536
Fujita T, Nakagohri T, Gotohda N, Takahashi S, Konishi M, Kojima M, Kinoshita T (2010) Evaluation of the prognostic factors and significance of lymph node status in invasive ductal carcinoma of the body or tail of the pancreas. Pancreas 39:e48–e54
Wu X, Tao R, Lei R, Han B, Cheng D, Shen B, Peng C (2010) Distal pancreatectomy combined with celiac axis resection in treatment of carcinoma of the body/tail of the pancreas: a single-center experience. Ann Surg Oncol 17:1359–1366
Kang CM, Kim DH, Lee WJ (2010) Ten years of experience with resection of left-sided pancreatic ductal adenocarcinoma: evolution and initial experience to a laparoscopic approach. Surg Endosc 24:1533–1541
Rosso E, Langella S, Addeo P, Nobili C, Oussoultzoglou E, Jaeck D, Bachellier P (2013) A safe technique for radical antegrade modular pancreatosplenectomy with venous resection for pancreatic cancer. J Am Coll Surg 217:e35–e39
Kitagawa H, Tajima H, Nakagawara H, Makino I, Miyashita T, Terakawa H, Nakanuma S, Hayashi H, Takamura H, Ohta T (2014) A modification of radical antegrade modular pancreatosplenectomy for adenocarcinoma of the left pancreas: significance of en bloc resection including the anterior renal fascia. World J Surg 38:2448–2454
Trottman P, Swett K, Shen P, Sirintrapun J (2014) Comparison of standard distal pancreatectomy and splenectomy with radical antegrade modular pancreatosplenectomy. Am Surg 80:295–300
Murakawa M, Aoyama T, Asari M, Katayama Y, Yamaoku K, Kanazawa A, Higuchi A, Shiozawa M, Kobayashi S, Ueno M, Morimoto M, Yamamoto N, Yoshikawa T, Rino Y, Masuda M, Morinaga S (2015) The short- and long-term outcomes of radical antegrade modular pancreatosplenectomy for adenocarcinoma of the body and tail of the pancreas. BMC Surg 15:120
Grossman JG, Fields RC, Hawkins WG, Strasberg SM (2016) Single institution results of radical antegrade modular pancreatosplenectomy for adenocarcinoma of the body and tail of pancreas in 78 patients. J Hepatobiliary Pancreat Sci 23:432–441
Hartwig W, Schneider L, Diener MK, Bergmann F, Büchler MW, Werner J (2009) Preoperative tissue diagnosis for tumours of the pancreas. Br J Surg 96:5–20
Cooper M, Newman NA, Ibrahim AM, Lam E, Herman JM, Singh VK et al (2013) Unnecessary tests and procedures in patients presenting with solid tumors of the pancreas. J Gastrointest Surg 17:1218–1223
Abe T, Ohuchida K, Miyasaka Y, Ohtsuka T, Oda Y, Nakamura M (2016) Comparison of surgical outcomes between radical antegrade modular pancreatosplenectomy (RAMPS) and standard retrograde pancreatosplenectomy (SPRS) for left-sided pancreatic cancer. World J Surg 40:2267–2275
Sierzega M, Bobrzyński Ł, Matyja A, Kulig J (2016) Factors predicting adequate lymph node yield in patients undergoing pancreatoduodenectomy for malignancy. World J Surg Oncol 14(1):248
Neoptolemos JP, Palmer DH, Ghaneh P, Psarelli EE, Valle JW, Halloran CM, Faluyi O, O'Reilly DA, Cunningham D, Wadsley J, Darby S, Meyer T, Gillmore R, Anthoney A, Lind P, Glimelius B, Falk S, Izbicki JR, Middleton GW, Cummins S, Ross PJ, Wasan H, McDonald A, Crosby T, Ma YT, Patel K, Sherriff D, Soomal R, Borg D, Sothi S, Hammel P, Hackert T, Jackson R, Büchler MW (2017) Comparison of adjuvant gemcitabine and capecitabine with gemcitabine monotherapy in patients with resected pancreatic cancer (ESPAC-4): a multicentre, open-label, randomised, phase 3 trial. Lancet 389(10073):1011–1024
Fernández-Cruz L, Poves I, Pelegrina A, Burdío F, Sánchez-Cabus S, Grande L (2016) Laparoscopic distal pancreatectomy for pancreatic tumors: does size matter? Dig Surg 33:290–298
Lee SH, Kang CM, Hwang HK, Choi SH, Lee WJ, Chi HS (2014) Minimally invasive RAMPS in well-selected left-sided pancreatic cancer within Yonsei criteria: long-term (>median 3 years) oncologic outcomes. Surg Endosc 28:2848–2855
Acknowledgements
The authors would like to thank the Department of Gastrointestinal Surgery and Surgical Oncology, Tata Memorial Hospital, Mumbai, India.
Author information
Authors and Affiliations
Contributions
Study concept and design: MS, MG, and SVS. Acquisition of data: MS, AD, MB, and VC. Analysis and interpretation of data: MS, VC, and SVS. Drafting of the manuscript: MS and SVS. Critical revision of the manuscript for important intellectual content: VC and SVS.
Corresponding author
Ethics declarations
Conflicts of interest
The authors declare that they have no conflict of interest.
Ethical approval
The data of the present study were collected in the course of common clinical practice and accordingly, the signed informed consent was obtained from each patient for any clinical procedure as well as for clinical data procurement. The study protocol was in accordance with ethical standards of the institutional research committee and the 1964 Helsinki Declaration and its later amendments. Since this was a retrospective study, formal consent for this study is not required and no approval of the institutional research committee was needed.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Sivasanker, M., Desouza, A., Bhandare, M. et al. Radical antegrade modular pancreatosplenectomy for all pancreatic body and tail tumors: rationale and results. Langenbecks Arch Surg 404, 183–190 (2019). https://doi.org/10.1007/s00423-019-01763-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00423-019-01763-4