
Abstract
Background
Early detection of anastomotic leakage after esophagectomy has the potential to reduce morbidity and mortality. Prompt suspicion of leak may help to exclude patients from fast-track protocols, thereby avoiding early oral feeding and early hospital discharge which could aggravate the prognosis of a clinically occult leak.
Patients and methods
Observational retrospective cohort study. Patients with diagnosis of esophageal cancer who underwent elective minimally invasive esophagectomy were included. The following data were collected: age, gender, BMI, comorbidities, ASA score, tumor histology, TNM staging, use of neo-adjuvant therapy, type of operation, operative time, morbidity, and 90-day mortality. A panel of biomarkers including C-reactive protein (CRP), procalcitonin (PCT), white blood cells (WBC), and percentage of neutrophils (PN) were measured at baseline and on postoperative days 3, 5, and 7.
Results
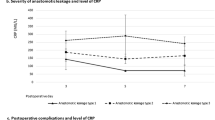
Two hundred forty-three patients operated between 2012 and 2017 were included in the study. Anastomotic leakage occurred in 29 patients. There was a statistical association over time between anastomotic leakage and CRP (p < 0.001), PCT (p < 0.001), WBC (p = 0.019), and PN (p = 0.007). The cut-off value of CRP on POD 5 was 8.3 mg/dL, AUC = 0.818, negative LR = 0.176.
Conclusions
Increased serum CRP, PCT, WBC, and PN after minimally invasive esophagectomy are associated with anastomotic leakage. A CRP value lower than 8.3 mg/dL, combined with reassuring clinical and radiological signs, may be useful to exclude leakage on postoperative day 5.




Similar content being viewed by others

References
Schmidt HM, Gisbertz SS, Moons J, Rouvelas I, Kauppi J, Brown A, Asti E, Luyer M, Lagarde SM, Berlth F, Philippron A, Bruns C, Hölscher A, Schneider PM, Raptis DA, Henegouwen MIB, Nafteux P, Nilsson M, Räsanen J, Palazzo F, Rosato E, Mercer S, Bonavina L, Nieuwenhuijzen G, Wijnhoven BPL, Schröder W, Pattyn P, Grimminger PP, Gutschow CA (2017) Defining benchmarks for transthoracic esophagectomy. A multicenter analysis of total minimally invasive esophagectomy in low risk patients. Ann Surg 266(5):814–821. https://doi.org/10.1097/SLA.0000000000002445
Low DE, Alderson D, Cecconello I, Chang A, Darling GE, Benoit D’Journo X et al (2015) International consensus on standardization of data collection for complications associated with esophagectomy. Ann Surg 262:286–294
Kassis ES, Kosinski AS, Jr RP, Koppes KE, Donahue JM, Daniel VC (2013) Predictors of anastomotic leak after esophagectomy: an analysis of the society of thoracic surgeons general thoracic database. Ann Thorac Surg 96:1919–1926
Bonavina L, Scolari F, Aiolfi A, Bonitta G, Sironi A, Saino G, Asti E (2016) Early outcome of thoracoscopic and hybrid esophagectomy: propensity-matched comparative analysis. Surgery 159:1073–1081
Biere SS, van Berge Henegouwen MI, Bonavina L, Rosman C, Roig Garcia J, Gisbertz SS, van der Peet DL, Cuesta MA (2017) Predictive factors for post-operative respiratory infections after esophagectomy for esophageal cancer: outcome of randomized trial. J Thorac Dis 9:S861–S867
Straatman J, Harmsen AM, Cuesta MA, Berkhof J, Jansma EP, Van der Peet DL (2015) Predictive value of C-reactive protein for major complications after major abdominal surgery: a systematic review and pooled-analysis. PLoS One 10:e0132995
Adamina M, Steffen T, Tarantino I, Beutner U, Schmied BM, Warschkow R (2015) Meta-analysis of the predictive value of C-reactive protein for infectious complications in abdominal surgery. Br J Surg 102:590–598
Hoeboer SH, Groeneveld AB, Engels N, Van Genderen M, Wijnhoven BPL, Van Bommel J (2015) Rising C-reactive protein and procalcitonin levels precede early complications after esophagectomy. J Gastrointest Surg 19:613–624
Miki Y, Toyokawa T, Kubo N, Tamura T, Sakurai K, Tanaka H, Muguruma K, Yashiro M, Hirakawa K, Ohira M (2017) C-reactive protein indicates early stage of postoperative infectious complications in patients following minimally invasive esophagectomy. World J Surg 41:796–803
Park JK, Kim JJ, Moon SW (2017) C-reactive protein for the early prediction of anastomotic leak after esophagectomy in both neo-adjuvant and non-neoadjuvant therapy case: a propensity score matching analysis. J Thorac Dis 9(10):3963–3702
Findlay JM, Tilson RC, Harikrishnan A, Sgromo B, Marshall REK, Maynard ND, Gillies RS, Middleton MR (2015) Attempted validation of the Nun score and inflammatory markers as predictors of esophageal anastomotic leak and major complications. Dis Esophagus 28:626–633
Bonavina L, Asti E, Sironi A, Bernardi D, Aiolfi A (2017) Hybrid and total minimally invasive esophagectomy: how I do it. J Thorac Dis 9:S761–S772
Dindo D, Demartines N, Clavien PA (2004) Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240:205–213
Fitzmaurice GM, Laird NM, Ware JH (2011) Applied longitudinal analysis. Wiley, Hoboken
Youden WJ (1950) Index for rating diagnostic tests. Cancer 3:32–35
Agresti A, Coull BA (1998) Approximate is better than “exact” for interval estimation of binomial proportions. Am Stat 52:119–126
Simel DL, Samsa GP, Matchar DB (1991) Likelihood ratios with confidence: sample size estimation for diagnostic test studies. J Clin Epidemiol 44:763–770
Šimundić AM (2009) Measures of diagnostic accuracy: basic definitions. EJIFCC 19:203–211
Sloane P, Slatt L, Ebell NH, Smith MA, Power DV, Viera AJ (2012) Essentials of family medicine, 6th edn. Walters Kluwer. Health, Philadelphia
R Core Team Development (2008) R: a language and environment for statistical computing. R Foundation for Statistical Computing, Vienna
Singh PP, Zeng IS, Srinivasa S, Lemanu DP, Connolly AB, Hill AG (2014) Systematic review and meta-analysis of use of serum C-reactive protein levels to predict anastomotic leak after colorectal surgery. Br J Surg 101:339–346
Motoyama S, Miura M, Hinai Y, Maruyama K, Usami S, Nakatsu T, Saito H, Minamiya Y, Suzuki T, Ogawa JI (2009) C-reactive protein 1059G>C genetic polymorphism influences serum C-reactive protein levels after esophagectomy in patients with thoracic esophageal cancer. J Am Coll Surg 209:477–483
Frees EW (2006) Longitudinal and panel data: analysis and applications in the social sciences. J Am Stat Assoc 101(March):402–402. https://doi.org/10.2307/30047489
Acknowledgements
This work was supported by AIRES (Associazione Italiana Ricerca Esofago).
Author information
Authors and Affiliations
Contributions
Authorship EA, GB, MM, ST, PM, AS, EC, and LB participated in the acquisition, analysis, or interpretation of data for the work and drafting or revising it critically for important intellectual content; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity in any part of the work are appropriately investigated and resolved.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with 1964 Helsinki declaration and its later amendments.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Electronic supplementary material
ESM 1
(DOCX 19 kb)
Rights and permissions
About this article

Cite this article
Asti, E., Bonitta, G., Melloni, M. et al. Utility of C-reactive protein as predictive biomarker of anastomotic leak after minimally invasive esophagectomy. Langenbecks Arch Surg 403, 235–244 (2018). https://doi.org/10.1007/s00423-018-1663-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00423-018-1663-4