
Abstract
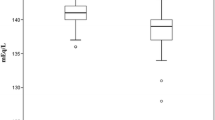
Hypothyroidism is widely accepted as a cause of hyponatremia and hypercreatininemia. However, the prevalence and severity of hy-ponatremia and hypercreatininemia in hypothyroid patients without comorbid conditions have not been well documented. We retrospectively studied serum sodium and creatinine levels in thyroid-ablated patients with differentiated thyroid cancer off (no.=128) and on (no.=60) thyroid hormone therapy. In the hypothyroid state, mean(±SD) TSH, sodium, and creatinine levels were 130.3±104.8 mU/l, 139.3±2.7 mEq/l, and 89.4±20 mmol/l respectively. Twenty-four patients (18.8%) had cre-atinine levels above the age- and sex-adjusted normal range, whereas only five patients (3.9%) had sodium levels below 135 mEq/l. No patient had a sodium level less than 130 mEq/l. Compared to their euthyroid values, mean sodium and creati-nine levels of the hypothyroid patients changed by -1.18 mEq/l (p=0.003) and 17.2 mmol/l (p<0.0001), respectively. There was significant correlation of TSH levels in the hypothyroid state with the changes from the euthyroid state to the hypothyroid state in creatinine levels (r=0.29, p=0.02) but not with the corresponding changes in sodium levels (r=0.06, p=0.6). In thirty-seven patients studied in two hypothyroid episodes, there was a significant correlation between a) TSH levels in hypothyroid state 1 and hypothyroid state 2 (r=0.56, p=0.0003), and b) the change in creatinine levels from the euthyroid state to hypothyroid state 1 and the corresponding change from the euthyroid state to hypothyroid state 2 (r=0.48, p=0.003). There was no significant correlation between the change in sodium levels from the euthyroid state to hypothyroid state 1 and the corresponding change from the euthyroid state to hypothyroid state 2 (r=0.32, p=0.05). We conclude that hyponatremia is very uncommon, whereas mild to moderate elevation in serum creatinine level is not uncommon in patients with short-term uncomplicated hypothyroidism.
Similar content being viewed by others

References
Had C.J. Jr., Bricker N.S. Renal function and I131 clearance in hyperthyroidism and myxedema. J. Clin. Endocrinol. Metab. 14: 1539, 1954.
De Rubertis F.R. Jr, Michelis M.F., Bloom M.E., Miniz D.H., Field J.B., Davis B.B. Impaired water excretion in myxedema. Am. J. Med. 51: 41, 1971.
Robertson G.L., Berl T. Pathophysiology of water metabolism. In: Brenner B.M., Rector F.C. Jr. (Eds.), The Kidney, ed. 4. WB Saunders, Philadelphia 1991, p. 667.
Gabow P.A. Hypo-hypernatremia. In: Cameron S., Davidson A.M., Grunfield J.P., Kerr D., Ritz E. (Eds.), Oxford Textbook of Clinical Nephrology. Oxford University Press, New York, 1992, p. 869.
Bradley S.E., Stephan F., Coelho J.B., Reville P. The thyroid and the kidney. Kidney Int. 6: 346, 1974.
Katz A.I., Emmanuel D.S, Lindheimer M.D. Thyroid hormone and the kidney. Nephron 15: 223, 1975.
Steiger M.J., Watson A.R., Morgan A.G. Hypothyroidism and renal impairment. J. Roy. Soc. Med. 84: 688, 1991.
Hammami M.M., AI-Saihati B., AlAhmari S., AlNuaim A., Khan B.A. Elevated serum creatinine level in thyroid cancer patients undergoing withdrawal of thyroxine therapy for radioiodine scan/treatment. Ann. Saudi Med. 15: 358, 1995.
Skowsky W.R., Kikuchi T.A. The role of vasopressin in the impaired water excretion of myxedema. Am. J. Med. 64: 613, 1978.
Goldberg M., Relvich M. Studies on the mechanism of hyponatremia and impaired water excretion in myxedema. Ann. Intern. Med. 56: 120, 1962.
Surveyor I. Sodium, potassium, and water metabolism in myxedema. Postgrad. Med. J. 45: 659, 1963.
Macaron C., Famuyiwa O. Hyponatremia of hypothyroidism. Appropriate suppression of antidiuretic hormone levels. Arch. Intern. Med. 138: 820, 1978.
Curtis R.H. Case Report: Hyponatremia in primary myxedema. Ann. Intern. Med. 44: 376, 1956.
Woodrow G., Brown J.A.M., Turney J.H. Acute-on-chronic renal failure and hyponatremia associated with severe hypothyroidism. Nephrol. Dial. Transplant. 8: 557, 1993.
Montenegro J., Gonzalez O., Saracho R., Aguirre R., Gonzalez O., Martinez I. Changes in renal function in primary hypothyroidism. Am. Kid. Dis. 27: 195, 1996.
Hammami M.M., AlSaihati B., AlAhmari S. Influence of age and sex in modulating TSH level in primary hypothyroidism. Ann. Saudi Med. 15: 575, 1995.
Ohara H., Kobayashi T., Shiraishi M., Wada T. Thyroid function of the aged as viewed from the pituitary thyroid system. Endocrinol. Jpn. 21: 377, 1974.
Cuttelod S, Lemarchand-Beraud T., Magnenat P., Perret C., Poli S., Vannoti A. Effect of age and role of kidneys and liver on thy-rotropin turnover in man. Metabolism 23: 101, 1974.
Chelimsky G., Davis I.D., Kliegman R.M. Neonatal hyponatremia associated with congenital hypothyroidism. Clin. Pediatr. 3: 177, 1997.
Johnston S., Hoult S., Chan C.A. Falling again. Lancet 349(9044): 26, 1997.
Allon M., Harrow A., Pasque C.B., Rodriguez M. Renal sodium and water handling in hypothyroid patients. The role of renal insufficiency. J. Am. Soc. Nephrol. 1: 205, 1990.
Capasso C., DeSanto N.G., Kinne R. Thyroid hormone and renal transport: Cellular and biochemical aspects. Kidney Int. 32: 443, 1987.
McLaughlin K.J., Mactier R.A. Renal impairment in hypothyroidism (Letter). Nephrol. Dial. Transplant. 9: 1521, 1994.
Vaamonde C.A., Sebastianelli M.J., Vaamonde L.S., Pellegrini E.L., Watts R.S., Klingler E.L. Impaired renal tubular reabsorption in hypothyroid man. J. Lab. Clin. Med. 83: 451, 1975.
Walters A.K. Increased vasopressin secretion in patients with hy-pothyroidism. Acta Endocrinol. (Copenh.). 88: 285, 1978.
Iwasaki Y., Oiso Y., Yamaguchi K., Takatsuki K., Kondo K., Hasegawa H., Tomita A. Osmoregulation of plasma vasopressin in myxedema. J. Clin. Endocrinol. Metab. 70: 534, 1990.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Baajafer, F.S., Hammami, M.M. & Mohamed, G.E.D. Prevalence and severity of hyponatremia and hypercreatininemia in short-term uncomplicated hypothyroidism. J Endocrinol Invest 22, 35–39 (1999). https://doi.org/10.1007/BF03345476
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03345476