
Abstract
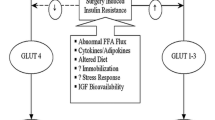
The stress response is viewed as the central physiological upset following major surgery, and reducing its various components is key to the rapid return to normal function. The stress response drives many of the pathophysiological changes in the early postoperative period, such as muscle weakness, insulin resistance and hyperglycemia, organ dysfunction, malaise, and psychological upset. Modification of this stress response is at the heart of ERAS programs and is a multidisciplinary perioperative approach.
In addition, as the role of the anesthesiologist expands to encompass perioperative medicine, there are a number of preoperative and postoperative interventions that can affect the stress response too. This chapter reviews how anesthetic practice can modify the response. Much of it centers around what might just be considered consistent high-quality anesthesia from protocolized pathways. The two major areas viewed as the sole control of the anesthesiologist are fluid administration and analgesia. When undertaken correctly these can revolutionize the patients’ perioperative pathway; but when poorly delivered, the effects can be disastrous and can result in a delayed recovery, with increased length of stay, complications, and cost. Both fluid administration and analgesia require a procedure-specific and patient-specific approach, balancing the anesthesiologist’s choice with potential side effects.
Access this chapter
Tax calculation will be finalised at checkout
Purchases are for personal use only
Similar content being viewed by others


References
Engelman RM, Rousou JA, Flack JE III, et al. Fast-track recovery of the coronary bypass patient. Ann Thorac Surg. 1994;58(6):1742–6.
Kehlet H, Mogensen T. Hospital stay of 2 days after open sigmoidectomy with a multimodal rehabilitation programme. Br J Surg. 1999;86(2):227–30.
Vlug MS, Wind J, Hollmann MW, Ubbink DT, Cense HA, Engel AF, et al. Laparoscopy in combination with fast track multimodal management is the best perioperative strategy in patients undergoing colonic surgery: a randomized clinical trial (LAFA-study). Ann Surg. 2011;254:868–75.
Veenhof AA, Vlug MS, van der Pas MH, Sietses C, van der Peet DL, De Lange-De Klerk ES, Bonjer HJ, et al. Surgical stress response and postoperative immune function after laparoscopy or open surgery with fast track or standard perioperative care: a randomized trial. Ann Surg. 2012;255:216–21.
Desborough JP. The stress response to trauma and surgery. Br J Anaesth. 2000;85:109–17.
Cuthbertson DP. Observations on the disturbance of metabolism produced by injury to the limbs. QJM. 1932;1:233–46.
Hill GL, Douglas RG, Schroeder D. Metabolic basis for the management of patients undergoing major surgery. World J Surg. 1993;17:146–53.
Leliefeld PH, Wessels CM, Leenen LP, Koenderman L, Pillay J. The role of neutrophils in immune dysfunction during severe inflammation. Crit Care. 2016;20:73.
Kehlet H, Mythen M. Why is the surgical high-risk patient still at risk? Br J Anaesth. 2011;106:289–91.
Watt DG, Horgan PG, McMillan DC. Routine clinical markers of the magnitude of the systemic inflammatory response after elective operation: a systematic review. Surgery. 2015;157:362–80.
McDonald RK, Evans FT, Weise VK, et al. Effects of morphine and nalorphine on plasma hydrocortisone levels in man. J Pharmacol Exp Ther. 1959;125:241–7.
Desborough JP, Hall GM. Modification of the hormonal and metabolic response to surgery by narcotics and general anaesthesia. Baillière’s Clin Anaesthesiol. 1989;3:317–34.
Kehlet H, Dahl JB. The value of “multimodal” or “balanced analgesia” in postoperative pain treatment. Anesth Analg. 1993;77:1048–56.
Watanabe K, Kashiwagi K, Kamiyama T, Yamamoto M, Fukunaga M, Inada E, Kamiyama Y. High-dose remifentanil suppresses stress response associated with pneumoperitoneum during laparoscopic colectomy. J Anesth. 2014;28:334–40.
Bardram L, Funch-Jensen P, Jensen P, Kehlet H, Crawford ME. Recovery after laparoscopic colonic surgery with epidural analgesia, and early oral nutrition and mobilisation. Lancet. 1995;345:763–4.
Kehlet H. The modifying effect of general and regional anesthesia on the endocrine-metabolic response to surgery. Reg Anesth Pain Med. 1982;7(4):S38–48.
Day AR, Smith RV, Scott MJ, Fawcett WJ, Rockall TA. Randomized clinical trial investigating the stress response from two different methods of analgesia after laparoscopic colorectal surgery. Br J Surg. 2015;102:1473–9.
Fawcett WJ, Edwards RE, Quinn AC, MacDonald IA, Hall GM. Thoracic epidural analgesia started after cardiopulmonary bypass: adrenergic, cardiovascular and respiratory sequelae. Anaesthesia. 1997;52:294–9.
Kuo CP, Jao SW, Chen KM, Wong CS, Yeh CC, Sheen MJ, Wu CT. Comparison of the effects of thoracic epidural analgesia and iv infusion with lidocaine on cytokine response, postoperative pain and bowel function in patients undergoing colonic surgery. Br J Anaesth. 2006;97(5):640–6.
Fawcett WJ. Abdominal (upper GI, colorectal and hepatobiliary) surgery. In: Struys M, Hardman J, Hopkins P, editors. The Oxford textbook of anaesthesia. 1st ed: Oxford University Press, Oxford, UK; 2016. p. 1041–56.
Hermanides J, Hollmann MW, Stevens MF, Lirk P. Failed epidural: causes and management. Br J Anaesth. 2012;109:144–54.
Varadhan KK, Lobo DN. A meta-analysis of randomised controlled trials of intravenous fluid therapy in major elective open abdominal surgery: getting the balance right. Proc Nutr Soc. 2010;69(4):488–98.
Gustafsson UO, Hausel J, Thorell A, Ljungqvist O, Soop M, Nygren J. Adherence to the enhanced recovery after surgery protocol and outcomes after colorectal cancer surgery. Arch Surg. 2011;146(5):571–7.
Levy BF, Scott MJP, Fawcett WJ, Fry C, Rockall TA. Randomized clinical trial of epidural, spinal or patient controlled analgesia for patients undergoing laparoscopic colorectal surgery. Br J Surg. 2011;98:1068–78.
Cook TM, Counsell D, Wildsmith JA. Major complications of central neuraxial block: report on the Third National Audit Project of the Royal College of Anaesthetists. Br J Anaesth. 2009;102:179–90.
Maltby JR, Sutherland AD, Sale JP, Shaffer EA. Preoperative oral fluids: is a five-hour fast justified prior to elective surgery? Anesth Analg. 1986;65:1112–6.
Phillips S, Hutchinson S, Davidson T. Preoperative drinking does not affect gastric contents. Br J Anaesth. 1993;70:6–9.
Ljungqvist O, Thorell A, Gutniak M, Häggmark T, Efendic S. Glucose infusion instead of preoperative fasting reduces postoperative insulin resistance. J Am Coll Surg. 1994;178:329–36.
Thorell A, Alston-Smith J, Ljungqvist O. The effect of preoperative carbohydrate loading on hormonal changes, hepatic glycogen, and glucoregulatory enzymes during abdominal surgery. Nutrition. 1996;12:690–5.
Svanfeldt M, Thorell A, Hausel J, Soop M, Nygren J, Ljungqvist O. Effect of ‘preoperative’ oral carbohydrate treatment on insulin action—a randomized cross-over unblended study in healthy subjects. Clin Nutr. 2005;24:815–21.
Fawcett WJ, Ljungvist O. Starvation, carbohydrate loading and outcome after major surgery. Br J Anaesth Educ. 2017;17:312–6.
Awad S, Varadhan KK, Ljungqvist O, Lobo DN. A meta-analysis of randomised controlled trials on preoperative oral carbohydrate treatment in elective surgery. Clin Nutr. 2013;32:34–44.
Smith MD, McCall J, Plank L, Herbison GP, Soop M, Nygren J. Preoperative carbohydrate treatment for enhancing recovery after elective surgery. Cochrane Libr. 2014;8:CD009161.
Amer MA, Smith MD, Herbison GP, Plank LD, McCall JL. Network meta-analysis of the effect of preoperative carbohydrate loading on recovery after elective surgery. Br J Surg. 2017;104:187–97.
Strøm C, Rasmussen LS, Sieber FE. Should general anaesthesia be avoided in the elderly? Anaesthesia. 2014;69:35–44.
Hunter JM. Reversal of residual neuromuscular block: complications associated with perioperative management of muscle relaxation. Br J Anaesth. 2017;119:i53–62.
Noblett SE, Snowden CP, Shenton BK, Horgan AF. Randomized clinical trial assessing the effect of Doppler-optimized fluid management on outcome after elective colorectal resection. Br J Surg. 2006;93:1069–76.
Lilot M, Ehrenfeld JM, Lee C, Harrington B, Cannesson M, Rinehart J. Variability in practice and factors predictive of total crystalloid administration during abdominal surgery: a retrospective two-center analysis. Br J Anaesth. 2015;114:767–76.
Minto G, Mythen MG. Perioperative fluid management: science, art or random chaos? Br J Anaesth. 2015;114:717–21.
Kunst G, Ostermann M. Intraoperative permissive oliguria – how much is too much? Br J Anaesth. 2017;119(6):1075–7.
Rollins KE, Lobo DN. Intraoperative goal-directed fluid therapy in elective major abdominal surgery: a meta-analysis of randomized controlled trials. Ann Surg. 2016;263:465–76.
Levy BF, Fawcett WJ, Scott MJP, Rockall TA. Intra-operative oxygen delivery in infusion volume optimized patients undergoing laparoscopic colorectal surgery within an enhanced recovery programme: effect of different analgesic modalities. Color Dis. 2012;14:887–92.
Cata JP, Guerra CE, Chang GJ, Gottumukkala V, Joshi GP. Non-steroidal anti-inflammatory drugs in the oncological surgical population: beneficial or harmful? A systematic review of the literature. Br J Anaesth. 2017;119:750–64.
Doleman B, Leonardi-Bee J, Heinink TP, Bhattacharjee D, Lund J, Williams JP. Pre-emptive and preventive NSAIDs for postoperative pain in adults undergoing all types of surgery. Cochrane Database Syst Rev. 2018;(3). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6517298/.
Wu Q, Purusram G, Wang H, Yuan R, Xie W, Gui P, Dong N, Yao S. The efficacy of parecoxib on systemic inflammatory response associated with cardiopulmonary bypass during cardiac surgery. Br J Clin Pharmacol. 2013;75:769–78.
Huang Z, Jiang H, Zhao H, Liu Z, Dong Z, Zhu B. Efficacy of parecoxib on the level of IL-6, CRP, and postoperative pain relief after percutaneous nephrolithotomy. Int J Clin Exp Med. 2016;9:19454–60.
Schmidt SC, Hamann S, Langrehr JM, Höflich C, Mittler J, Jacob D, Neuhaus P. Preoperative high-dose steroid administration attenuates the surgical stress response following liver resection: results of a prospective randomized study. J Hepato-Biliary-Pancreat Surg. 2007;14:484–92.
Srinivasa S, Kahokehr AA, Yu TC, Hill AG. Preoperative glucocorticoid use in major abdominal surgery: systematic review and meta-analysis of randomized trials. Ann Surg. 2011;254:183–91.
Hall GM, Peerbhoy D, Shenkin A, Parker CJ, Salmon P. Relationship of the functional recovery after hip arthroplasty to the neuroendocrine and inflammatory responses. Br J Anaesth. 2001;87(4):537–42.
Lunn TH, Andersen LØ, Kristensen BB, Husted H, Gaarn-Larsen L, Bandholm T, Ladelund S, Kehlet H. Effect of high-dose preoperative methylprednisolone on recovery after total hip arthroplasty: a randomized, double-blind, placebo-controlled trial. Br J Anaesth. 2012;110(1):66–73.
Lunn TH, Kristensen BB, Andersen LØ, Husted H, Otte KS, Gaarn-Larsen L, Kehlet H. Effect of high-dose preoperative methylprednisolone on pain and recovery after total knee arthroplasty: a randomized, placebo-controlled trial. Br J Anaesth. 2010;106(2):230–8.
Cassuto J, Sinclair R, Bonderovic M. Anti-inflammatory properties of local anesthetics and their present and potential clinical implications. Acta Anaesthesiol Scand. 2006;50:265–82.
Dunn LK, Durieux ME. Perioperative use of intravenous lidocaine. Anesthesiology. 2017;126:729–37.
Hollmann MW, McIntire WE, Garrison JC, Durieux ME. Inhibition of mammalian Gq protein function by local anesthetics. Anesthesiology. 2002;97:1451–7.
Weibel S, Jokinen J, Pace NL, Schnabel A, Hollmann MW, Hahnenkamp K, Eberhart LH, Poepping DM, Afshari A, Kranke P. Efficacy and safety of intravenous lidocaine for postoperative analgesia and recovery after surgery: a systematic review with trial sequential analysis. Br J Anaesth. 2016;116(6):770–83.
Weibel S, Jelting Y, Pace NL, Helf A, Eberhart LH, Hahnenkamp K, Hollmann MW, Poepping DM, Schnabel A, Kranke P. Continuous intravenous perioperative lidocaine infusion for postoperative pain and recovery in adults. Cochrane Database Syst Rev. 2018;6:CD009642.
Levy BF, Scott MJ, Fawcett WJ, Rockall TA. 23-hour stay laparoscopic colectomy. Dis Colon Rectum. 2009;52:1239–43.
Richardson J, Sabanathan S, Jones J, Shah RD, Cheema S, Mearns AJ. A prospective, randomized comparison of preoperative and continuous balanced epidural or paravertebral bupivacaine on post-thoracotomy pain, pulmonary function and stress responses. Br J Anaesth. 1999;83(3):387–92.
O’Riain SC, Buggy DJ, Kerin MJ, Watson RW, Moriarty DC. Inhibition of the stress response to breast cancer surgery by regional anesthesia and analgesia does not affect vascular endothelial growth factor and prostaglandin E2. Anesth Analg. 2005;100(1):244–9.
Abu Elyazed MM, Mostafa SF, Abdullah MA, Eid GM. The effect of ultrasound-guided transversus abdominis plane (TAP) block on postoperative analgesia and neuroendocrine stress response in pediatric patients undergoing elective open inguinal hernia repair. Pediatr Anesth. 2016;26(12):1165–71.
Purdy M, Kokki M, Anttila M, Aspinen S, Juvonen P, Korhonen R, Selander T, Kokki H, Eskelinen M. Does the rectus sheath block analgesia reduce the inflammatory response biomarkers’ IL-1ra, IL-6, IL-8, IL-10 and IL-1β concentrations following surgery? A randomized clinical trial of patients with cancer and benign disease. Anticancer Res. 2016;36:3005–11.
Levy N, Mills P, Mythen M. Is the pursuit of DREAM ing (drinking, eating and mobilising) the ultimate goal of anaesthesia? Anaesthesia. 2016;71:1008–12.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Fawcett, W.J. (2020). Anesthetic Management and the Role of the Anesthesiologist in Reducing Surgical Stress and Improving Recovery. In: Ljungqvist, O., Francis, N., Urman, R. (eds) Enhanced Recovery After Surgery. Springer, Cham. https://doi.org/10.1007/978-3-030-33443-7_14
Download citation
DOI: https://doi.org/10.1007/978-3-030-33443-7_14
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-33442-0
Online ISBN: 978-3-030-33443-7
eBook Packages: MedicineMedicine (R0)