
Long-Term Health Symptoms and Sequelae Following SARS-CoV-2 Infection: An Evidence Map

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
2.2. Type of Outcome Measures
2.3. Main Outcomes
- Cardiovascular functioning: including symptoms and conditions (i.e., chest pain, arrhythmias, heart failure, ischaemic heart disease, and postural hypotension/tachycardia);
- Fatigue or Exhaustion;
- Pain: localised pain (headache), neuropathic pain, and muscle/joint pain;
- Nervous system functioning: symptoms and conditions (vertigo, dizziness, and paraesthesias/numbness);
- Cognitive functioning: symptoms and conditions, and systematic assessments of cognitive functioning;
- Mental functioning: symptoms and conditions, including but not limited to depression, anxiety, post-traumatic stress disorder, and emotional distress, among others;
- Respiratory functioning: symptoms (e.g., dyspnoea) and conditions, and systematic assessments of respiratory function (i.e., FEV1, FVC);
- Post-exertion symptoms;
- Health-related quality of life: including measurements of physical-mental-social functioning (SF-36 or EuroQOL or other related scales);
- Changes in work/occupation and studies (school attendance);
- Survival related to long-COVID-19 (i.e., not overall survival related to infection, but to the presence of persistent or new long-term symptoms or sequelae);
- Recovery/duration of symptoms;
- Need for rehabilitation/resource use;
- Other complications/sequelae: metabolic, autoimmune, or others.
2.4. Search Methods for Identification of Studies
- The Cochrane COVID-19 Study Register (CCSR) was searched using the Cochrane Register of Studies (https://crsweb.cochrane.org (accessed on 5 November 2021)) which included the following:
- Cochrane Central Register of Controlled Trials (CENTRAL), monthly updates.
- MEDLINE (PubMed), daily updates;
- Embase.com, weekly updates;
- ClinicalTrials.gov (https://www.clinicaltrials.gov, daily updates;
- WHO International Clinical Trials Registry Platform (ICTRP);
- (http://www.who.int/trialsearch, weekly updates;
- medRxiv (https://www.medrxiv.org, weekly updates.
- WHO COVID-19 Global literature on coronavirus disease database (https://search.bvsalud.org/global-literature-on-novel-coronavirus-2019-ncov (accessed on 5 November 2021)).
2.5. Data Collection and Analysis
2.6. Data Extraction
2.7. Data Charting
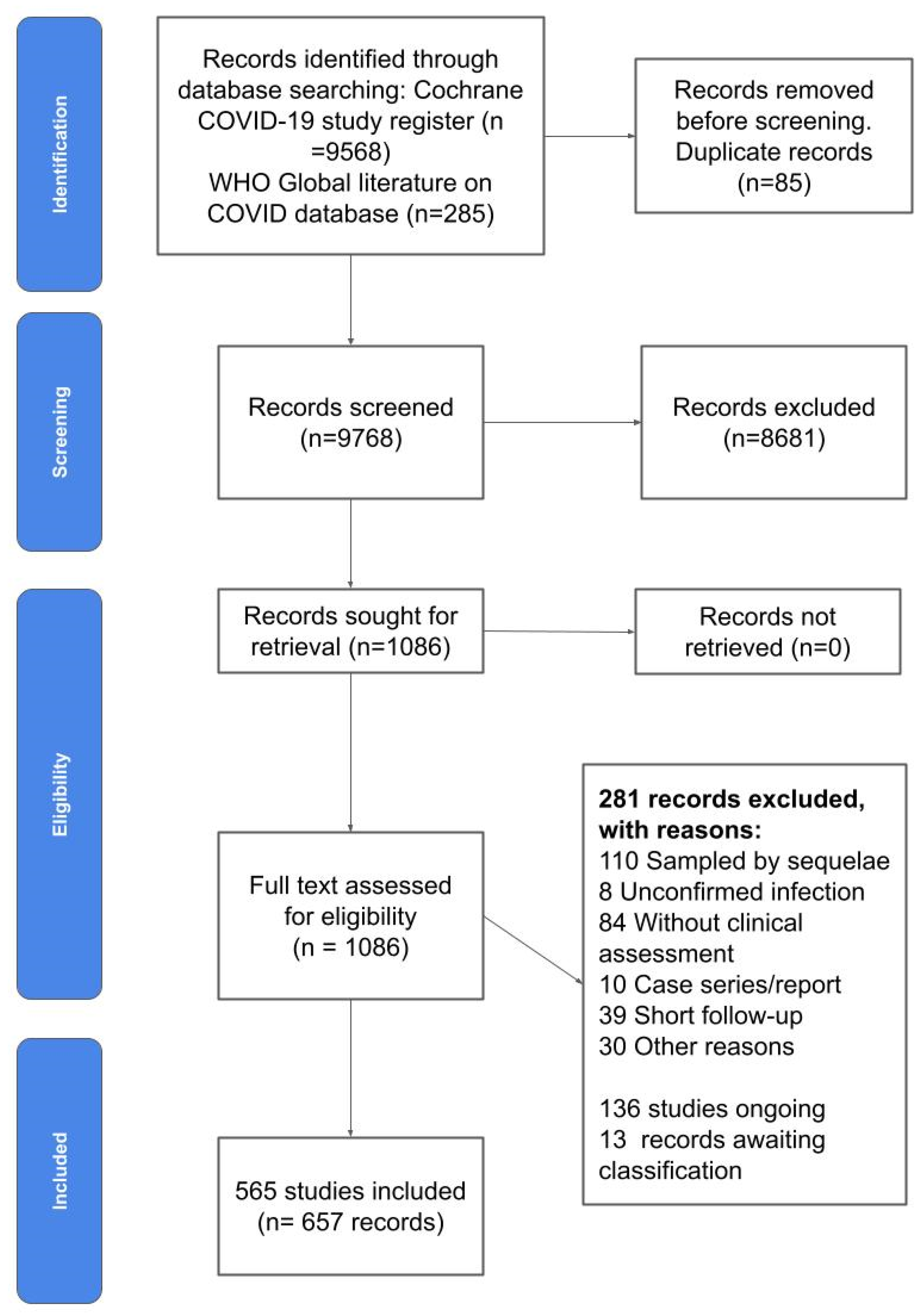
3. Results
4. Discussion
4.1. Main Findings
4.2. Related Research
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- Empirically derived search strategy for the Cochrane COVID-19 Register
- 1.
- (function NEXT (impairment OR abnormalit*)): TI, AB
- 2.
- ((protracted OR residual OR unresolved OR prolonged) ADJ3 symptoms): TI, AB
- 3.
- symptom burden: TI, AB
- 4.
- ((after OR residual) NEXT disease): TI, AB
- 5.
- pulmonary function: TI, AB
- 6.
- “after hospital discharge”: TI, AB
- 7.
- (survivors ADJ2 (COVID OR COVID-19)): TI, AB
- 8.
- symptoms after: TI, AB
- 9.
- sequelae: TI, AB
- 10.
- (post acute NEXT (phase OR COVID OR COVID-19)): TI, AB
- 11.
- long haul*: TI, AB
- 12.
- (long COVID OR long COVID-19): TI, AB
- 13.
- long lasting: TI, AB
- 14.
- function test*: TI, AB
- 15.
- (suffer* ADJ3 symptoms): TI, AB
- 16.
- smell: TI, AB
- 17.
- persist*: TI, AB
- 18.
- (consequences ADJ3 (COVID OR COVID-19)): TI, AB
- 19.
- (discharged ADJ3 patients): TI, AB
- 20.
- (recover* ADJ3 (COVID OR COVID-19)): TI, AB
- 21.
- OR/1-20
- Conceptually developed search strategy for the WHO COVID-19 Global literature on coronavirus disease database
References
- Singh, A.; Gupta, V. SARS-CoV-2 therapeutics: How far do we stand from a remedy? Pharmacol. Rep. 2021, 73, 750–768. [Google Scholar] [CrossRef] [PubMed]
- Viswanathan, M.; Kahwati, L.; Jahn, B.; Giger, K.; Dobrescu, A.I.; Hill, C.; Klerings, I.; Meixner, J.; Persad, E.; Teufer, B.; et al. Universal screening for SARS-CoV-2 infection: A rapid review. Cochrane Database Syst. Rev. 2020, 9, CD013718. [Google Scholar] [CrossRef] [PubMed]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef]
- Michelen, M.; Manoharan, L.; Elkheir, N.; Cheng, V.; Dagens, A.; Hastie, C.; O‘Hara, M.; Suett, J.; Dahmash, D.; Bugaeva, P.; et al. Characterising long COVID: A living systematic review. BMJ Glob. Health 2021, 6, e005427. [Google Scholar] [CrossRef] [PubMed]
- Callard, F.; Perego, E. How and why patients made Long COVID. Soc. Sci. Med. 2021, 268, 113426. [Google Scholar] [CrossRef] [PubMed]
- Nabavi, N. Long COVID: How to define it and how to manage it. BMJ 2020, 370, m3489. [Google Scholar] [CrossRef]
- World Health Organization (WHO) Clinical Case Definition Working Group on Post COVID-19 Condition. A Clinical Case Definition of Post COVID-19 Condition by a Delphi Consensus, 6 October 2021. 2021. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-Post_COVID-19_condition-Clinical_case_definition-2021.1 (accessed on 22 October 2021).
- CDC. Post-COVID Conditions. 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/long-term-effects/index.html (accessed on 22 October 2021).
- NICE. Overview|COVID-19 Rapid Guideline: Managing the Long-Term Effects of COVID-19|Guidance|NICE. Available online: https://www.nice.org.uk/guidance/ng188 (accessed on 22 October 2021).
- Koczulla, A.R.; Ankermann, T.; Behrends, U.; Berlit, P.; Böing, S.; Brinkmann, F.; Franke, C.; Glöckl, R.; Gogoll, C.; Hummel, T.; et al. S1-Leitlinie Post-COVID/Long-COVID; Kessel, S.A.M.V., Hartman, T.C.O., Lucassen, P.L.B.J., van Jaarsveld, C.H.M., Eds.; AWMF: Frankfurt am Main, Germany, 2021; Available online: https://www.awmf.org/uploads/tx_szleitlinien/020-027l_S1_Post_COVID_Long_COVID_2021-07.pdf (accessed on 22 October 2021).
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Perelman, C.; Sepulveda, R.; Rebolledo, P.A.; Cuapio, A.; Villapol, S. More than 50 long-term effects of COVID-19: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 16144. [Google Scholar] [CrossRef]
- Himmels, J.P.W.; Qureshi, S.A.; Brurberg, K.G.; Gravningen, K.M. COVID-19: Long Term Effects of COVID-19. [Langvarige effekter av COVID-19 Hurtigoversikt 2021]. 2021. Available online: https://www.fhi.no/globalassets/dokumenterfiler/rapporter/2021/covid-19-long-term-effects-of-covid-19-report-2021.pdf (accessed on 8 August 2022).
- Martimbianco, A.L.C.; Pacheco, R.L.; Bagattini, M.; Riera, R. Frequency, signs and symptoms, and criteria adopted for long COVID-19: A systematic review. Int. J. Clin. Pract. 2021, 75, e14357. [Google Scholar] [CrossRef]
- Groff, D.; Sun, A.; Ssentongo, A.E.; Ba, D.M.; Parsons, N.; Poudel, G.R.; Lekoubou, A.; Oh, J.S.; Ericson, J.E.; Ssentongo, P.; et al. Short-term and Long-term Rates of Postacute Sequelae of SARS-CoV-2 Infection: A Systematic Review. JAMA Netw. Open 2021, 4, e2128568. [Google Scholar] [CrossRef]
- Kessel, S.A.M.v.; Hartman, T.C.O.; Lucassen, P.L.B.J.; van Jaarsveld, C.H.M. Post-acute and long-COVID-19 symptoms in patients with mild diseases: A systematic review. Fam. Pract. 2021, 39, 159–167. [Google Scholar] [CrossRef]
- Iwu, C.J.; Iwu, C.D.; Wiysonge, C.S. The occurrence of long COVID: A rapid review. Pan Afr. Med. J. 2021, 38, 65. [Google Scholar] [CrossRef] [PubMed]
- Akbarialiabad, H.; Taghrir, M.H.; Abdollahi, A.; Ghahramani, N.; Kumar, M.; Paydar, S.; Razani, B.; Mwangi, J.; Asadi-Pooya, A.A.; Malekmakan, L.; et al. Long COVID, a comprehensive systematic scoping review. Infection 2021, 49, 1163–1186. [Google Scholar] [CrossRef] [PubMed]
- Sinclair, D.; E Adams, C. Treatment resistant schizophrenia: A comprehensive survey of randomised controlled trials. BMC Psychiatry 2014, 14, 253. [Google Scholar] [CrossRef] [PubMed]
- Franco, J.V.A.; Oltra, G.; Metzendorf, M.-I.; Garegnani, L.I.; Ducks, D.; Heldt, K.; Mumm, R.; Barnes, B.; Scheidt-Nave, C. LongCOV_521; RKI: Berlin, Germany, 2021. [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Munblit, D.; Nicholson, T.; Akrami, A.; Apfelbacher, C.; Chen, J.; De Groote, W.; Diaz, J.; Gorst, S.L.; Harman, N.; Kokorina, A.; et al. Core Outcome Set for Research and Clinical Practice in Post COVID-19 Condition (Long COVID): An International Delphi Consensus Study ‘PC-COS’. 2022. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=4017375 (accessed on 8 August 2022). [CrossRef]
- Long COVID Deutschland. Available online: https://longcoviddeutschland.org/ (accessed on 22 October 2021).
- Metzendorf, M.-I.; Featherstone, R.M. Evaluation of the comprehensiveness, accuracy and currency of the Cochrane COVID-19 Study Register for supporting rapid evidence synthesis production. Res. Synth. Methods 2021, 12, 607–617. [Google Scholar] [CrossRef]
- Hausner, E.; Waffenschmidt, S.; Kaiser, T.; Simon, M. Routine development of objectively derived search strategies. Syst. Rev. 2012, 1, 19. [Google Scholar] [CrossRef]
- Hausner, E.; Guddat, C.; Hermanns, T.; Lampert, U.; Waffenschmidt, S. Development of search strategies for systematic reviews: Validation showed the noninferiority of the objective approach. J. Clin. Epidemiol. 2015, 68, 191–199. [Google Scholar] [CrossRef]
- Adam, G.P.; Paynter, R. Development of literature search strategies for evidence syntheses: Pros and cons of incorporating text mining tools and objective approaches. BMJ Evid. Based Med. 2022. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (Updated February 2021); Cochrane: London, UK, 2021; Available online: https://www.training.cochrane.org/handbook (accessed on 8 August 2022).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 88, 105906. [Google Scholar] [CrossRef]
- Thomas, J.; Graziosi, S.; Brunton, J.; Ghouze, Z.; O’Driscoll, P.; Bond, M.; Koryakina, A. EPPI-Reviewer: Advanced Software for Systematic Reviews, Maps and Evidence Synthesis; EPPI-Centre, UCL Social Research Institute; University College London: London, UK, 2022. [Google Scholar]
- EPPI-Mapper; Digital Solution Foundry and EPPI-Centre: London, UK, 2022.
- Chen, C.; Haupert, S.R.; Zimmermann, L.; Shi, X.; Fritsche, L.G.; Mukherjee, B. Global Prevalence of Post COVID-19 Condition or Long COVID: A Meta-Analysis and Systematic Review. J. Infect. Dis. 2022. [Google Scholar] [CrossRef]
- Nittas, V.; Gao, M.; West, E.A.; Ballouz, T.; Menges, D.; Hanson, S.W.; Puhan, M.A. Long COVID Through a Public Health Lens: An Umbrella Review. Public Health Rev. 2022, 43, 1604501. [Google Scholar] [CrossRef] [PubMed]
- Borel, M.; Xie, L.; Kapera, O.; Mihalcea, A.; Kahn, J.; Messiah, S.E. Long-term physical, mental and social health effects of COVID-19 in the pediatric population: A scoping review. World J. Pediatr. 2022, 18, 149–159. [Google Scholar] [CrossRef] [PubMed]
- Ansems, K.; Grundeis, F.; Dahms, K.; Mikolajewska, A.; Thieme, V.; Piechotta, V.; Metzendorf, M.-I.; Stegemann, M.; Benstoem, C.; Fichtner, F. Remdesivir for the treatment of COVID-19. Cochrane Database Syst. Rev. 2021, 8, CD014962. [Google Scholar] [CrossRef]
- Popp, M.; Stegemann, M.; Riemer, M.; Metzendorf, M.-I.; Romero, C.S.; Mikolajewska, A.; Kranke, P.; Meybohm, P.; Skoetz, N.; Weibel, S. Antibiotics for the treatment of COVID-19. Cochrane Database Syst. Rev. 2021, 10, CD015025. [Google Scholar] [CrossRef] [PubMed]
- Mikolajewska, A.; Fischer, A.-L.; Piechotta, V.; Mueller, A.; Metzendorf, M.-I.; Becker, M.; Dorando, E.; Pacheco, R.L.; Martimbianco, A.L.C.; Riera, R.; et al. Colchicine for the treatment of COVID-19. Cochrane Database Syst. Rev. 2021, 10, CD015045. [Google Scholar] [CrossRef]
- Wagner, C.; Griesel, M.; Mikolajewska, A.; Mueller, A.; Nothacker, M.; Kley, K.; Metzendorf, M.-I.; Fischer, A.-L.; Kopp, M.; Stegemann, M.; et al. Systemic corticosteroids for the treatment of COVID-19. Cochrane Database Syst. Rev. 2021, 8, CD014963. [Google Scholar] [CrossRef]
- Mathes, T.; Klaßen, P.; Pieper, D. Frequency of data extraction errors and methods to increase data extraction quality: A methodological review. BMC Med. Res. Methodol. 2017, 17, 152. [Google Scholar] [CrossRef]
- Taylor, K.S.; Mahtani, K.R.; Aronson, J.K. Summarising good practice guidelines for data extraction for systematic reviews and meta-analysis. BMJ Evid. Based Med. 2021, 26, 88–90. [Google Scholar] [CrossRef]
- Munblit, D.; Nicholson, T.R.; Needham, D.M.; Seylanova, N.; Parr, C.; Chen, J.; Kokorina, A.; Sigfrid, L.; Buonsenso, D.; Bhatnagar, S.; et al. Studying the post-COVID-19 condition: Research challenges, strategies, and importance of Core Outcome Set development. BMC Med. 2022, 20, 50. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Organisation | Definition (Elements) |
|---|---|
| WHO [7] | Post-COVID-19 conditions
|
| CDC [8] USA |
|
| NICE [9] UK |
|
| AWMF [10] Germany |
|
| Characteristics | Proportion |
|---|---|
| Publication type | |
| Preprint | 39/565 (6.90%) |
| Journal article | 421/565 (74.51%) |
| Abstract | 66/565 (11.68%) |
| Research letter/brief report | 39/565 (6.90%) |
| Language | |
| English | 555/565 (98.23%) |
| Other | 10/565 (1.77%) |
| Study design | |
| Cross-sectional | 142/565 (25.12%) |
| Longitudinal | 422/565 (74.69%) |
| With a control group | 83/565 (15%) |
| Follow-up ≥ 12 weeks | 377/565 (66.73%) |
| Median sample size (interquartile range) | 134 participants (73 to 397) |
| Median follow up (interquartile range) | 13 weeks (9 to 24) |
| Setting | |
| Country | |
| High income | 410/565 (72.57%) |
| Upper middle income | 96/565 (17.17%) |
| Lower middle income | 50/565 (8.85%) |
| Low income | 0/565 (0%) |
| Recruitment | |
| Community/contact tracing | 120/565 (21.24%) |
| Outpatient | 194/565 (34.34%) |
| Hospital | 327/565 (57.88%) |
| ICU | 192/565 (33.98%) |
| Population | |
| Children | 55/565 (9.73%) |
| Aged 0–5 | 26/565 (4.60%) |
| Aged 6–11 | 36/565 (6.37%) |
| Aged 11–18 | 50/565 (8.85%) |
| Adults | 528/565 (93.45%) |
| Only elderly adults | 7/565 (1%) |
| Subpopulation | |
| Healthcare workers | 22/565 (3.89%) |
| Pregnant persons | 1/565 (0.18%) |
| Socially vulnerable | 15/565 (2.65%) |
| Chronic conditions | 116/565 (20.53%) |
| Vaccinated | 4/565 (0.71%) |
| Severity | |
| Asymptomatic | 111/565 (19.65%) |
| Mild | 306/565 (54.16%) |
| Moderate | 346/565 (61.24%) |
| Severe | 353/565 (62.48%) |
| Critical | 311/565 (55.04%) |
| Prognostic factors | |
| Symptoms/onset | 182/565 (32.21%) |
| Severity/infection | 244/565 (43.19%) |
| Vaccination status | 3/565 (0.53%) |
| Age | 243/565 (43.01%) |
| Gender/sex | 238/565 (42.12%) |
| Race/ethnicity | 48/565 (8.50%) |
| Socio-economic status | 43/565 (7.61%) |
| Comorbidities | 200/565 (35.40%) |
| Non-Communicable Diseases | 131/565 (23.19%) |
| Immunosuppression | 24/565 (4.25%) |
| Outcomes | |
| Cardiovascular functioning | 227/565 (40.18%) |
| Fatigue or Exhaustion | 307/565 (54.34%) |
| Pain | 281/565 (49.73%) |
| Nervous system functioning | 324/565 (57.35%) |
| Cognitive functioning | 146/565 (25.84%) |
| Mental functioning | 241/565 (42.65%) |
| Respiratory functioning | 401/565 (70.97%) |
| Post-exertion symptoms | 156/565 (27.61%) |
| Health-related Quality of Life | 92/565 (16.28%) |
| Changes in work/occupation and study | 57/565 (10.09%) |
| Survival related to long-COVID-19 | 25/565 (4.42%) |
| Recovery/duration of symptoms | 135/565 (23.89%) |
| Need for rehabilitation/resource use | 101/565 (17.88%) |
| Other complications/sequelae | 271/565 (47.96%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Franco, J.V.A.; Garegnani, L.I.; Oltra, G.V.; Metzendorf, M.-I.; Trivisonno, L.F.; Sgarbossa, N.; Ducks, D.; Heldt, K.; Mumm, R.; Barnes, B.; et al. Long-Term Health Symptoms and Sequelae Following SARS-CoV-2 Infection: An Evidence Map. Int. J. Environ. Res. Public Health 2022, 19, 9915. https://doi.org/10.3390/ijerph19169915
Franco JVA, Garegnani LI, Oltra GV, Metzendorf M-I, Trivisonno LF, Sgarbossa N, Ducks D, Heldt K, Mumm R, Barnes B, et al. Long-Term Health Symptoms and Sequelae Following SARS-CoV-2 Infection: An Evidence Map. International Journal of Environmental Research and Public Health. 2022; 19(16):9915. https://doi.org/10.3390/ijerph19169915
Chicago/Turabian StyleFranco, Juan Victor Ariel, Luis Ignacio Garegnani, Gisela Viviana Oltra, Maria-Inti Metzendorf, Leonel Fabrizio Trivisonno, Nadia Sgarbossa, Denise Ducks, Katharina Heldt, Rebekka Mumm, Benjamin Barnes, and et al. 2022. "Long-Term Health Symptoms and Sequelae Following SARS-CoV-2 Infection: An Evidence Map" International Journal of Environmental Research and Public Health 19, no. 16: 9915. https://doi.org/10.3390/ijerph19169915