
Hyaluronic Acid in Facial Rehabilitation—A Narrative Review

1
Department of Dermatology and Allergology, Städtisches Klinikum Dresden, Academic Teaching Hospital, 01067 Dresden, Germany
2
Faculty of Medicine, Clinic for Dermatology, University Clinical Center, 18104 Nis, Serbia
3
Department of Plastic Surgery, Hospital São Lucas da PUCRS, Porto Alegre 90610-001, Brazil
*
Author to whom correspondence should be addressed.
Cosmetics 2023, 10(2), 61; https://doi.org/10.3390/cosmetics10020061
Submission received: 14 March 2023
/
Revised: 26 March 2023
/
Accepted: 4 April 2023
/
Published: 6 April 2023
(This article belongs to the Special Issue Aesthetic and Cosmetic Dermatology: 2nd Edition)
Abstract
:Background: Hyaluronic acid fillers (HAF) are a versatile tool in esthetic medicine. They also have a potential for medical indications including facial rehabilitation. Materials and methods: We performed a literature search on PUBMED and Google Scholar until December 2022. Clinical trials, clinical studies, review articles, systematic reviews, meta-analyses, case series, and case reports were considered for review. Keywords “facial rehabilitation”, “acne scars”, “traumatic scars”, “oral restoration”, “facial lipoatrophy”, “facial asymmetry”, “periocular correction”, “nasal obstruction”, “ear lobe restoration”, “morphea”, AND “hyaluronic acid filler” were used to select articles. Results: We prepared a narrative review on the use of HAF for correction of facial asymmetry and asymmetric lips, improvement of different types of scars, improvement of the jaw line, improvement of ear lobes, periocular and oral restoration, and the treatment of nasal obstruction and morphea en coub de sabre. The amount of HA used in these indications is often less than 1 mL. The bolus technique, fanning, and dual-plane injections can be utilized for treatment. Duration of clinical effects depends upon the anatomical region and is usually maintained between 2 months and 2 years. Adverse events are often mild and temporary. Vascular occlusion is a severe adverse event, but it has not been reported yet for these medical indications. Repeated injections are recommended to obtain a longer-lasting improvement. In cases of morphea, only stable and non-inflammatory plaques should be treated. The advantage of HAF compared to permanent and semipermanent fillers is the availability of hyaluronidase for rapid removal of filler material and to revise overcorrection. Conclusions: HAF play an auxiliary role in facial rehabilitation. Knowledge of filler qualities, anatomy, and underlying diagnoses is important for their safe application. More prospective controlled trials are necessary to improve evidence.
1. Introduction
Hyaluronic acid (HA) is a high-molecular-weight non-sulphated glycosaminoglycan. HA is an important component of human extracellular matrix. The half-life of natural HA is only 12 h. HA becomes biodegraded by endogenous hyaluronidase. HA fragments are eliminated via lymphatics and hepatic degradation into water and carbon dioxide [1].
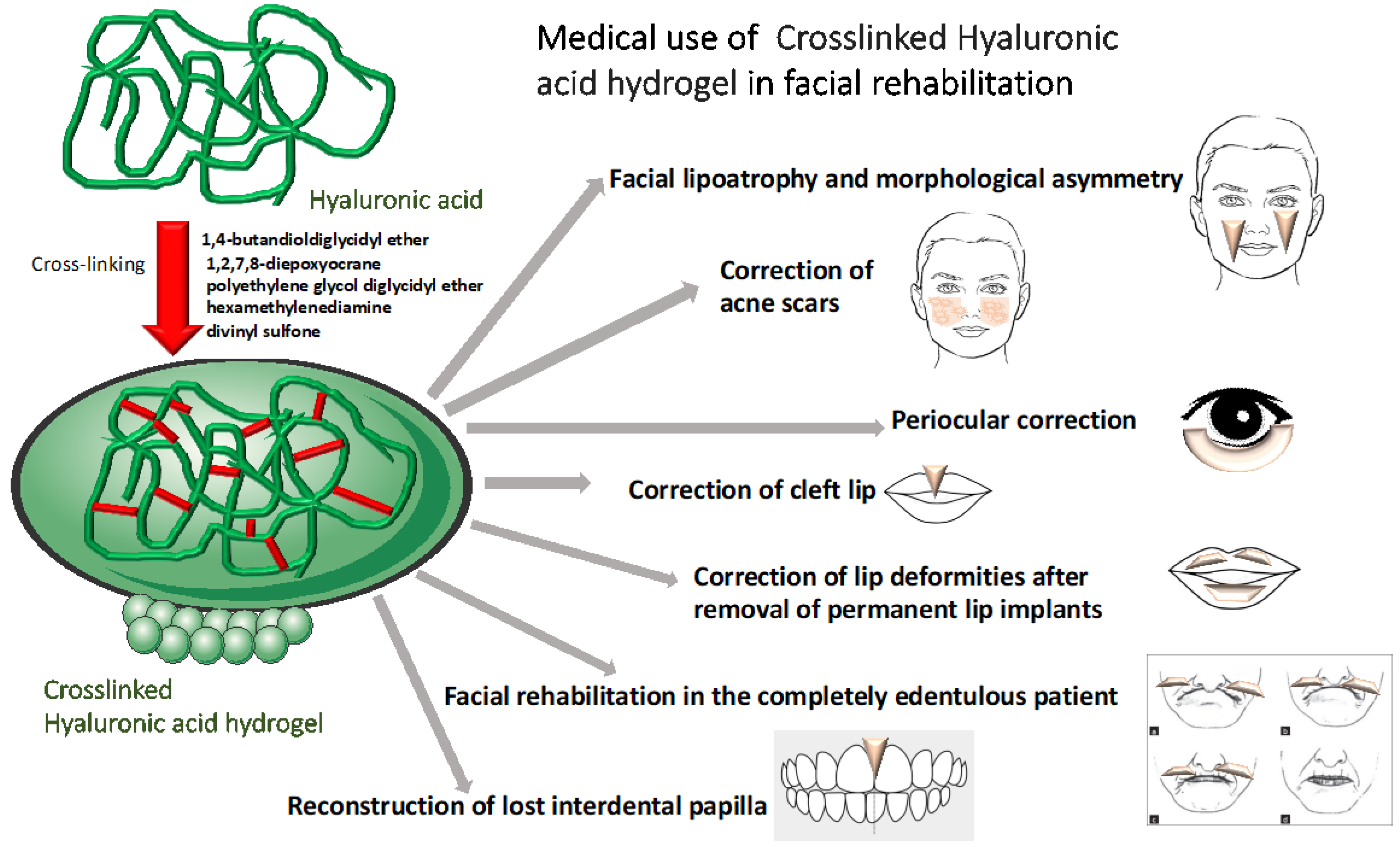
HA has become the dominant filler material in esthetics. It is used for rejuvenation and correction of volume loss during aging. For this purpose, crosslinked HA is preferred, as it offers a greater stability to endogenous hyaluronidase. Various crosslinking agents are employed to prepare HA fillers (HAF) for different indications such as 1,4-butandioldiglycidyl ether, 1,2,7,8-diepoxyocrane, polyethylene glycol diglycidyl ether, hexamethylenediamine, and divinyl sulfone [2].
HAF present as hydrogels in either phosphate-buffered or physiological solutions. They are versatile tools in esthetic medicine. HAF can be classified into “monophasic” and “biphasic”, depending on production modalities. It is important to understand biophysical and rheological qualities of HAF to choose a product for a certain indication (Table 1) [3]. After injection into human tissue, water diffuses into the gel, which consists of confined and bulk water with different water dynamics [4]. Distribution of HAF in human tissue depends upon filler qualities, injection technique, and anatomical region. It was demonstrated that manual remodeling of HAF after injection did not translate into significant changes in the filler pool size [5]. More fluid and less cohesive HAF spread more into superficial layers, whereas those with a stronger elastic modulus G’ tend to stay deeper [6]. HAF reduce lipolysis and ensure lipid accumulation of human pre-adipocytes, suggesting that interactions of HAF with skin-associated adipose tissue is responsible for volumizing effects [7,8].
For application of HAF, sharp needles or blunt cannulas are used. Slow, low-pressure injection is recommended. For safe application of HAF, it is indispensable to know the anatomy of the region. Vasculature and nerves are the most critical structures [9]. Adverse events associated with HAF are often mild and temporary in the hands of the experienced physician, but catastrophic events have occasionally been observed due to vascular compromise. This includes loss of vision, cerebral embolism, and skin necrosis [10,11,12]. In contrast to the common assumption, cannulas are not safer [13]. A negative aspiration before HAF injection is often recommended, but some authors suggest that it is not reliable and therefore dispensable [14].
In addition to the beneficial effects in esthetic medicine, HAF may also be used for medical purposes. In this review, we will focus on HAF in facial rehabilitation (Figure 1).
2. Material and Methods
The literature was searched through PubMed and Google Scholar to retrieve relevant published articles on the use of HAF in facial rehabilitation. Clinical trials, clinical studies, review articles, systematic reviews, meta-analyses, case series, and case reports were considered for review. Keywords “facial rehabilitation”, “acne scars”, “traumatic scars”, “oral restoration”, “facial lipoatrophy”, “facial asymmetry”, “periocular correction”, “nasal obstruction”, “ear lobe restoration”, “morphea”, AND “hyaluronic acid filler” were used to search the articles. Articles published until 2022 along with reference lists of relevant articles were included for review. During the literature search, 203 articles were screened, of which 56 were included in this review after detailed analysis. Purely esthetic articles, duplicate articles, and articles missing details of treatment and adverse events were excluded.
3. Medical Use in Facial Rehabilitation
3.1. Facial Lipoatrophy and Morphological Asymmetry
Facial nerve palsy is a common disease with an estimated prevalence of up to 40 per 100,000 inhabitants without a gender preference [15]. Idiopathic (Bell’s) palsy, viral infections including herpes simplex, herpes zoster or SARS-CoV-2, tumors, and trauma are possible causes [16]. It leads to an asymmetric appearance of the face, soft tissue atrophy, contracture, and hyper- and synkinesis. The severity of facial palsy is classified according to the House–Brackmann grading system in six categories from zero (normal facial function) to six (no movement at all) [15].
HIV-associated facial lipoatrophy of the malar and temporal regions is a possible adverse event of anti-retroviral therapy. It is more common with the use of specific thymidine analog nucleoside reverse transcriptase inhibitors. The prevalence is between 10% and 80%. The exact pathogenesis is unknown [17,18]. Only lipoatrophy can be targeted by HAF.
Other causes of facial asymmetry include muscular hypotrophy, autoimmune connective tissue disease, or trauma. Facial asymmetry can cause psychological distress and can impair self-esteem.
There are several case reports on correction of facial asymmetry or lipoatrophy by HAF (Table 2) [19,20]. In two prospective open trials, correction of facial lipoatrophy and morphological asymmetry with HAF resulted in a success rate of 100% at week four [21,22].
The effects were documented using the nasolabial fold severity rating scale and the global esthetic improvement scale.
3.2. Correction of Depressed Post-Traumatic Scars
Correction of post-traumatic scars is possible with HAF. HAF are a versatile tool, especially for depressed facial scars (Figure 2) [23,24,25,26]. The filler is placed under the depressed area. In a prospective trial, 41 patients with a median age of 34 years were treated twice with HAF for depressed scars. Injections were done two weeks apart. There was a follow-up of 90 days after the second treatment. During the study period, the median observer total score decreased by 77.5%, and the median patient total score decreased by 73.7%. Younger patients benefitted more [27].
3.3. Correction of Acne Scars
Acne, a common inflammatory disease of adolescents and young adults, can results in scarring. The Quantitative Global Scarring Grading System for Post-acne Scarring differentiates four grades: I with macular flat marks of different color; II with mild atrophic or hypertrophic scars; III with moderate atrophic or hypertrophic scars; and IV with severe atrophic or hypertrophic scars [28].
There are different types of acne scars. Atrophic scars include deep and narrow icepick scars, larger rolling scars, and depressed boxcar scars. Other types are hypertrophic scars and acne keloids. HAF are only useful in treating atrophic variants of acne scars [29].
HAF are usually used as an adjunct to laser treatment (Table 3) [30,31,32,33,34,35,36]. In an open trial of patients (n = 12) with moderate to severe acne scarring, microinjections of low-viscosity 20 mg/mL HAF were performed into discrete depressed acne scars on the face. All these patients had previously completed a series of fractional laser resurfacing. An immediate visual improvement was observed in all lesions. Transient pinpoint bleeding at the injection site was observed as a temporary mild adverse event [31]. Pain during injection was scored mild to moderate [30].
Fifteen patients were included in a split-face, blind, randomized, placebo-controlled clinical trial. HAF (1 mL) was compared to 1 mL of physiological saline to treat atrophic rolling scars. One touch-up treatment was allowed. Patient satisfaction was 93% in favor of HAF. Scores from the Quantitative Global Scarring Grading System for Post-acne Scarring after 90 days were -6.6 (HAF) and -1.7 (saline), respectively [36].
Most studies used scoring systems to document the clinical effects.
4. Periocular Correction
The inability to completely close the eyelids is known as lagophthalmos. It is caused either by paralysis, lid retraction, or exophthalmos. Injection of 0.1 to 1.2 mL HAF in the pretarsal or pre-elevator of the upper eyelid can improve lagophthalmos by 4.6 to 4.8 mm. Duration of the effect is about four months. The major side effects are ecchymosis, blepharoptosis, and contour irregularities [37,38]. Upper eyelid margin irregularities have been corrected by injection of small amounts of HAF (0.1 to 0.4 mL) with at least 8 months duration [39].
Orbital volume deficiency can lead to enophthalmos. Orbital volume enhancement was performed with a standard transcutaneous inferotemporal peribulbar-type approach. Two milliliters of either Restylane Sub-Q (Q-Med, Uppsala, Sweden) or Juvederm Voluma (Allergan, Dublin, Ireland) led to a 2 mm improvement for about 6 months. Vasovagal reaction is a possible complication [40,41,42].
A similar technique may be used for anophthalmic sockets or sockets of phtisis eyes after severe trauma [40].
5. Correction of Cleft Lip
Nasoalveolar molding, surgical lip repair techniques, and use of recombinant human bone morphogenetic protein-2 for alveolar bone grafting show promising results in the repair of lip and palate clefts [43].
HAF can be used as secondary treatment to improve projection and volume of the affected area in a profile view and to correct asymmetries [44,45]. This leads to an improvement in self-esteem, but it does not seem to affect lip strength, articulation, or orofacial myofunctional behavior [46]. The volume effect lasts for about 4 months.
6. Correction of Lip Deformities after Removal of Permanent Lip Implants
Permanent soft tissue implants can result in severe adverse events, even after many years. Complete removal often needs surgery with or without intralesional laser application [47]. After surgical removal, lip competence can be impaired.
7. Facial Rehabilitation in the Completely Edentulous Patient
Edentulism is related to the aging process and presents the endpoint of dental disease. The world-wide prevalence for 2010 was estimated to be 2.3% [49]. The etiology is complex and depends on genetics, lifestyle, and comorbidities. Edentulism leads to significant alveolar bone resorption of up to 25% within its first year. In addition to this, the jawbone height becomes reduced, changing the profile of the face. The chin gets projected forward, and the lips appear thinner and crushed. Another consequence of edentulism is an ongoing atrophy of the orbicularis oculi muscle, leading the invagination of the red lips and accentuation of fine lines, the labiomental fold, and the labiomental crease [50,51].
In the concept of complex rehabilitation (bone, teeth, and gingiva), HAF may play an auxiliary role.
HAF can be used to improve nasolabial folds, labial commissures, lip contour, and philtrum. This contributes to improved self-esteem and self-rated health [52]. Documentation of clinical effects is done by clinical investigation, subjective data from the patients, and standardized photography.
8. Reconstruction of Lost Interdental Papilla
Gingiva and dental papilla play an important role in protecting and maintaining periodontal structure and health. They are also involved in phonetics. Loss of dental papilla is multifactorial. Known factors include colonization with Porphyromonas gingivalis, herpes, periodontitis, senescence, and oral exposure to metals and metalloids [53,54].
9. Reshaping Lower Jaw and Restoration after Delayed Diagnosis of Malar Arch Fracture
In a retrospective trial, 36 female patients (mean age 45.7 years) were treated by subcutaneous HAF injections to restore the jawline during aging. Four different HAF brand were employed with different G’ modules. Bolus injections with 0.1 to 0.5 mL were used on the symphysis, parasymphysis, and gonial angle. Injection was completed by retrograde release of 0.5 to 1.1 mL HAF along the mandibular ramus, the mandibular body, and the cutaneous part of the lower lip. After 21 days, all patients reported a rate of satisfaction of at least 80 on a VAS scale of 0 to 100. Side effects were temporary and mild [60].
A 26-year-old male patient with a complete fracture of the zygomatic arch after a soccer match presented 9 months after the trauma with facial asymmetry. There was no functional impairment in mouth opening, but there was edema. For this patient, both a surgical and a non-surgical approach were proposed. The patient decided to have the non-surgical treatment. High-viscose HAF was injected supra-periosteally. A second HAF was injected subcutaneously to restore the malar projection. The result was stable for 8 months. A touch-up was suggested after 12 months [61].
In cases of early diagnosed malar arch fracture, the surgical approach remains the gold standard.
10. Ear Lobe Restoration
The outer ears contribute to facial appearance and symmetry. Asymmetry of ears is seen after trauma, tumor surgery, or by adornment of jewelry and piercings. The latter can cause stretching and sagging of ear lobes. Genetics as well as intrinsic and extrinsic aging also contribute. Earlobe ptosis can be classified according to Mowlavi et al. (2005) into three degrees of severity [62].
Nonsurgical earlobe correction is limited to class I and II, i.e., ptosis ≤ 10 mm.
Injection of HAF into these earlobes results in an immediate improvement of ptosis, a better fullness of the soft tissue, and improved esthetics. The procedure is well tolerated [63,64,65]. In a retrospective trial including 26 adult women, 8% were very satisfied and 92% were satisfied with the results. The effect lasted on average 9 months, but in some patients, it lasted even 12 months [64]. Another trial on 12 women with Movlawi grade I and II reported effects lasting even 14 months (Table 5) [66]. Clinical effects were documented by subjective criteria and semi-quantitative scorings.
There was one animal study on rabbit ears that demonstrated improved cartilage re-shaping 8 weeks after injection of HAF [67].
11. Nasal Obstruction
Nasal valve irregularities can result in nasal obstruction. HAF injection into the internal valve from the anterior part results in nasal widening. This technique, also known as “liquid spreader grafts”, reduced mean nasal resistance from 3.4 ± 5.6 sPa/mL to 0.4 ± 0.3 sPa/mL one month after HAF injection in 16 adult patients. The reported data suggest a repeated injection after 12 months [68]. Measurement of nasal resistance by rhinomanometry is an objective tool.
12. Facial Morphea
Morphea or localized scleroderma can cause depressed fibrotic lesions by ongoing inflammation. Active plaques are characterized by a lilac ring. Morphea en coup de sabre is a stigmatizing linear type of localized scleroderma of the face.
The intralesional injection of fillers in lesions of morphea and other autoimmune connective tissue disorders is controversial. According to a recent review, most published data are available for HAF as filler material. It was concluded that HAF injection seems to be a safe adjunctive procedure for morphea [69].
The use of soft tissue fillers is not recommended in active lesions, since the volumizing effect of non-permanent fillers is very limited and relapses are common. In stable lesions without obvious clinical signs of inflammation, however, injection of HAF may result in prolonged efficacy. Table 6 summarizes trials and outcomes for patients with morphea en coup de sabre [70,71,72,73,74,75,76]. The volumizing effect was calculated by clinical criteria only.
13. Limitations
HAF are non-permanent fillers. The effects on hydration, tissue stimulation, and volumizing also remain temporary. Therefore, repeated application is recommended to maintain the effect. Areas of danger for filler injections need to be avoided. One example is the forehead, where acute and delayed vascular compromise can lead to disastrous consequences such as skin necrosis, blindness, or even stroke [77].
Filler injection requires a detailed knowledge of filler properties, anatomy, and management of adverse events. Hyaluronidase is the major tool in management of minor (granuloma) and severe side effects (vascular compromise) and should be available on site [78]. Based on clinical data, 10 to 20 U of hyaluronidase are sufficient to dissolute 0.2 mL of HAF in most cases [79,80].
In recent years during the COVID-19 pandemic, adverse reactions to HAF (particularly acute inflammatory reactions) have been reported due to SARS-CoV-2 infection [81]. Although exact mechanisms have not been elucidated, three possible hypotheses are discussed: (a) an intensified hygiene regimen during the COVID-19 pandemic and the use of protective face masks changed the cutaneous microbiome, (b) increased stress levels with higher endogenous cortisol, and (c) induction of delayed immune response by viral infection. Both (a) and (b) result in activation of a Th2 response. COVID-19 vaccination may also increase the risk of unwanted side effects with HAF [82]. Although most adverse filler reactions have been documented after mRNA vaccines, they may occur with other vaccine types as well. For mRNA vaccines, hypersensitivity to polyethylene glycol or interaction with the spike protein of SARS-CoV-19 have been discussed [83].
There have been various attempts to establish a consensus on HAF safety and prevention of adverse events [84,85,86]. Heydenrych et al. (2021) developed a 10-point algorithm to increase patient safety with HAF injection. The included (1) patient’s medical history, (2) assessment (ethnicity, gender, and beauty), (3) consent, (4) product reversibility, (5) product characteristics (i.e., HA concentration, crosslinking, and G’), (6) product layering, (7) photo-documentation, (8) procedural planning and aseptic technique, (9) anatomy of injections, and (10) technical knowledge [87].
Within these limitations, HAF can be used safely for various medical indications such as facial rehabilitation. Prospective, controlled trials are sparse but necessary to gain better evidence for the proposed techniques and indications.
14. Conclusions
In the concept of facial rehabilitation, different and often complex approaches are necessary to obtain satisfying results. Surgical and non-surgical methods have been developed to tailor the treatment to the individual patient’s needs.
HAF can be considered as an auxiliary procedure in combination with cold steel or laser surgery. Despite the wide accessibility of HAF and the minimal invasive approach to apply, there are several limitations. HAF need to be applied repeatedly to maintain the clinical effects. Application needs experience and management of possible adverse events. Costs for the treatment have to be covered by the patients.
Nevertheless, HAF injections have been documented for a wide range of possible indications in facial rehabilitation. In the hands of experienced physicians, they can help to improve function, appearance, and self-esteem of patients.
Further studies are necessary since the level of evidence is rather low.
Author Contributions
A.G. and U.W. have done the conceptualization and data collection. U.W. wrote the first draft. A.G., H.K. and U.W. were involved in review and editing. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The review was conducted according to the professional regulations of the Saxonian Physicians Chamber. Such type of study does not require ethical approval.
Informed Consent Statement
All patients gave their written informed consent for publication of their photographs.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Wollina, U.; Goldman, A. Hyaluronic acid dermal fillers: Safety and efficacy for the treatment of wrinkles, aging skin, body sculpturing and medical conditions. Clin. Med. Rev. Ther. 2011, 3, 107–121. [Google Scholar] [CrossRef] [Green Version]
- Zerbinati, N.; D’Este, E.; Farina, A.; Rauso, R.; Cherubino, M.; Calligaro, A. Morphological evidences following pegylated filler treatment in human skin. J. Biol. Regul. Homeost. Agents 2017, 31 (2 Suppl. 2), 79–85. [Google Scholar] [PubMed]
- Fundarò, S.P.; Salti, G.; Malgapo, D.M.H.; Innocenti, S. The rheology and physicochemical characteristics of hyaluronic acid fillers: Their clinical implications. Int. J. Mol. Sci. 2022, 23, 10518. [Google Scholar] [CrossRef] [PubMed]
- Kruk, D.; Rochowski, P.; Masiewicz, E.; Wilczynski, S.; Wojciechowski, M.; Broche, L.M.; Lurie, D.J. Mechanism of water dynamics in hyaluronic dermal fillers revealed by nuclear magnetic resonance relaxometry. Chemphyschem 2019, 20, 2816–2822. [Google Scholar] [CrossRef] [PubMed]
- Vandeputte, J.; Leemans, G.; Dhaene, K.; Forsyth, R.; Vanslembrouck, J.; Hatem, F.; Micheels, P. Spreading pattern and tissue response to hyaluronic acid gel injections in the subcutis: Ultrasound videos, ultrasound measurements, and histology. Aesthetic Surg. J. 2021, 41, 224–241. [Google Scholar] [CrossRef] [Green Version]
- Rosamilia, G.; Hamade, H.; Freytag, D.L.; Frank, K.; Green, J.B.; Devineni, A.; Gavril, D.L.; Hernandez, C.A.; Pavicic, T.; Cotofana, S. Soft tissue distribution pattern of facial soft tissue fillers with different viscoelastic properties. J. Cosmet. Dermatol. 2020, 19, 312–320. [Google Scholar] [CrossRef]
- Nadra, K.; André, M.; Marchaud, E.; Kestemont, P.; Braccini, F.; Cartier, H.; Kéophiphath, M.; Fanian, F. A hyaluronic acid-based filler reduces lipolysis in human mature adipocytes and maintains adherence and lipid accumulation of long-term differentiated human preadipocytes. J. Cosmet. Dermatol. 2021, 20, 1474–1482. [Google Scholar] [CrossRef]
- Wollina, U. Midfacial rejuvenation by hyaluronic acid fillers and subcutaneous adipose tissue—A new concept. Med. Hypotheses 2015, 84, 327–330. [Google Scholar] [CrossRef]
- Wollina, U.; Goldman, A. Facial vascular danger zones for filler injections. Dermatol. Ther. 2020, 33, e14285. [Google Scholar] [CrossRef]
- Walker, L.; Convery, C.; Davies, E.; Murray, G.; Croasdell, B. Consensus opinion for the management of soft tissue filler induced vision loss. J. Clin. Aesthetic Dermatol. 2021, 14, E84–E94. [Google Scholar]
- Wang, H.C.; Yu, N.; Wang, X.; Dong, R.; Long, X.; Feng, X.; Li, J.; Wu, W.T.L. Cerebral Embolism as a Result of Facial Filler Injections: A Literature Review. Aesthetic Surg. J. 2022, 42, NP162–NP175. [Google Scholar] [CrossRef]
- Soares, D.J. Bridging a century-old problem: The pathophysiology and molecular mechanisms of HA filler-induced vascular occlusion (FIVO)-implications for therapeutic interventions. Molecules 2022, 27, 5398. [Google Scholar] [CrossRef]
- Wang, H.C.; Yu, N.; Wang, X. False sense of safety: Blunt cannulas cause the majority of severe vascular complications in hyaluronic acid injection. Plast. Reconstr. Surg. 2021, 147, 694e–695e. [Google Scholar] [CrossRef]
- Goodman, G.J.; Magnusson, M.R.; Callan, P.; Roberts, S.; Hart, S.; Lin, F.; Rahman, E.; McDonald, C.B.; Liew, S.; Porter, C.; et al. Aspiration before tissue filler-an exercise in futility and unsafe practice. Aesthetic Surg. J. 2022, 42, 89–101. [Google Scholar] [CrossRef]
- Singh, A.; Deshmukh, P. Bell’s palsy: A review. Cureus 2022, 14, e30186. [Google Scholar] [CrossRef]
- Turki, A.; Abbas, K.S.; Makram, A.M.; Elfert, M.; Elmarabea, M.; El-Shahat, N.A.; Abdalshafy, H.; Sampong, A.; Chintalapati, S.; Huy, N.T. Epidemiology, clinical features, and treatment modalities of facial nerve palsy in COVID-19 patients: A systematic review. Acta Neurol. Belg. 2022, 122, 1419–1432. [Google Scholar] [CrossRef]
- Carey, D.; Liew, S.; Emery, S. Restorative interventions for HIV facial lipoatrophy. AIDS Rev. 2008, 10, 116–124. [Google Scholar]
- Guzman, N.; Vijayan, V. HIV-Associated Lipodystrophy; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Pavicic, T.; Ruzicka, T.; Korting, H.C.; Gauglitz, G. Monophasic, cohesive-polydensified-matrix crosslinking-technology-based hyaluronic acid filler for the treatment of facial lipoatrophy in HIV-infected patients. J. Drugs Dermatol. 2010, 9, 690–695. [Google Scholar]
- Wollina, U.; Goldman, A. Botulinum toxin A and/or soft tissue fillers for facial rehabilitation. Wien. Med. Wochenschr. 2017, 167, 92–95. [Google Scholar] [CrossRef]
- Kopera, D.; Ivezic-Schoenfeld, Z.; Federspiel, I.G.; Grablowitz, D.; Gehl, B.; Prinz, M. Treatment of facial lipoatrophy, morphological asymmetry, or debilitating scars with the hyaluronic acid dermal filler Princess® FILLER. Clin. Cosmet. Investig. Dermatol. 2018, 11, 621–628. [Google Scholar] [CrossRef] [Green Version]
- Grablowitz, D.; Ivezic-Schoenfeld, Z.; Federspiel, I.G.; Gehl, B.; Kopera, D.; Prinz, M. Long-term effectiveness of a hyaluronic acid soft tissue filler in patients with facial lipoatrophy, morphological asymmetry, or debilitating scars. J. Cosmet. Dermatol. 2020, 19, 2536–2541. [Google Scholar] [CrossRef] [PubMed]
- Hussain, S.N.; Goodman, G.J.; Rahman, E. Treatment of a traumatic atrophic depressed scar with hyaluronic acid fillers: A case report. Clin. Cosmet. Investig. Dermatol. 2017, 10, 285–287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mashiko, T.; Mori, H.; Kato, H.; Doi, K.; Kuno, S.; Kinoshita, K.; Kunimatsu, A.; Ohtomo, K.; Yoshimura, K. Semipermanent volumization by an absorbable filler: Onlay injection technique to the bone. Plast. Reconstr. Surg. Glob. Open 2013, 1, e4–e14. [Google Scholar] [CrossRef] [PubMed]
- Richards, K.N.; Rashid, R.M. Twenty-four-month persistence of hyaluronic acid filler for an atrophic scar. J. Cosmet. Dermatol. 2011, 10, 311–312. [Google Scholar] [CrossRef] [PubMed]
- Kasper, D.A.; Cohen, J.L.; Saxena, A.; Morganroth, G.S. Fillers for postsurgical depressed scars after skin cancer reconstruction. J. Drugs Dermatol. 2008, 7, 486–487. [Google Scholar]
- Riccio, M.; Marchesini, A.; Senesi, L.; Skrami, E.; Gesuita, R.; De Francesco, F. Managing pathologic scars by injecting auto-cross-linked hyaluronic acid: A preliminary prospective clinical study. Aesthetic Plast. Surg. 2019, 43, 480–489. [Google Scholar] [CrossRef]
- Goodman, G.J.; Baron, J.A. Postacne scarring--a quantitative global scarring grading system. J. Cosmet. Dermatol. 2006, 5, 48–52. [Google Scholar] [CrossRef]
- Wollina, U.; Goldman, A. Fillers for the improvement in acne scars. Clin. Cosmet. Investig. Dermatol. 2015, 8, 493–499. [Google Scholar] [CrossRef] [Green Version]
- Hasson, A.; Romero, W.A. Treatment of facial atrophic scars with Esthélis, a hyaluronic acid filler with polydense cohesive matrix (CPM). J. Drugs Dermatol. 2010, 9, 1507–1509. [Google Scholar]
- Halachmi, S.; Ben Amitai, D.; Lapidoth, M. Treatment of acne scars with hyaluronic acid: An improved approach. J. Drugs Dermatol. 2013, 12, e121–e123. [Google Scholar]
- Goodman, G.J.; Van Den Broek, A. The modified tower vertical filler technique for the treatment of post-acne scarring. Australas. J. Dermatol. 2016, 57, 19–23. [Google Scholar] [CrossRef]
- Dierickx, C.; Larsson, M.K.; Blomster, S. Effectiveness and safety of acne scar treatment with nonanimal stabilized hyaluronic acid gel. Dermatol. Surg. 2018, 44 (Suppl. 1), S10–S18. [Google Scholar] [CrossRef]
- Artzi, O.; Cohen, S.; Koren, A.; Niv, R.; Friedman, O. Dual-plane hyaluronic acid treatment for atrophic acne scars. J. Cosmet. Dermatol. 2020, 19, 69–74. [Google Scholar] [CrossRef]
- Siperstein, R.; Nestor, E.; Meran, S.; Grunebaum, L. A split-face, blind, randomized placebo-controlled clinical trial investigating the efficacy and safety of hyaluronic acid filler for the correction of atrophic facial scars. J. Cosmet. Dermatol. 2022, 21, 3768–3778. [Google Scholar] [CrossRef]
- Akerman, L.; Mimouni, D.; Nosrati, A.; Hilewitz, D.; Solomon-Cohen, E. A combination of non-ablative laser and hyaluronic acid injectable for postacne scars: A novel treatment protocol. J. Clin. Aesthetic Dermatol. 2022, 15, 53–56. [Google Scholar]
- Taban, M.; Mancini, R.; Nakra, T.; Velez, F.G.; Ela-Dalman, N.; Tsirbas, A.; Douglas, R.S.; Goldberg, R.A. Nonsurgical management of congenital eyelid malpositions using hyaluronic acid gel. Ophthalmic Plast. Reconstr. Surg. 2009, 25, 259–263. [Google Scholar] [CrossRef] [Green Version]
- Martín-Oviedo, C.; García, I.; Lowy, A.; Scola, E.; Aristegui, M.; Scola, B. Hyaluronic acid gel weight: A nonsurgical option for the management of paralytic lagophthalmos. Laryngoscope 2013, 123, E91–E96. [Google Scholar] [CrossRef]
- Mancini, R.; Khadavi, N.M.; Goldberg, R.A. Nonsurgical management of upper eyelid margin asymmetry using hyaluronic acid gel filler. Ophthalmic Plast. Reconstr. Surg. 2011, 27, 1–3. [Google Scholar] [CrossRef]
- Malhotra, R. Deep orbital Sub-Q restylane (nonanimal stabilized hyaluronic acid) for orbital volume enhancement in sighted and anophthalmic orbits. Arch. Ophthalmol. 2007, 125, 1623–1629. [Google Scholar] [CrossRef] [Green Version]
- Tay, E.; Olver, J. Intraorbital hyaluronic acid for enophthalmos. Ophthalmology 2008, 115, 1101–1101.e2. [Google Scholar] [CrossRef]
- Zamani, M.; Thyagarajan, S.; Olver, J.M. Adjunctive use of hyaluronic acid gel (Restylane Sub-Q) in anophthalmic volume deficient sockets and phthisical eyes. Ophthalmic Plast. Reconstr. Surg. 2010, 26, 250–253. [Google Scholar] [CrossRef] [PubMed]
- Wadde, K.; Chowdhar, A.; Venkatakrishnan, L.; Ghodake, M.; Sachdev, S.S.; Chhapane, A. Protocols in the management of cleft lip and palate: A systematic review: Running Title: Management of Cleft Lip and Palate. J. Stomatol. Oral Maxillofac. Surg. 2022, 142, 101338. [Google Scholar] [CrossRef]
- Schweiger, E.S.; Riddle, C.C.; Tonkovic-Capin, V.; Aires, D.J. Successful treatment with injected hyaluronic acid in a patient with lip asymmetry after surgical correction of cleft lip. Dermatol. Surg. 2008, 34, 717–719. [Google Scholar] [CrossRef]
- Manzoni, A.P.D.; Venier, N.A.B. Hyaluronic acid filler correction of scars and asymmetries secondary to cleft lip repair. Dermatol. Surg. 2022, 48, 1264–1266. [Google Scholar] [CrossRef] [PubMed]
- Alighieri, C.; Bettens, K.; Roche, N.; Bruneel, L.; Van Lierde, K. Lipofilling in patients with a cleft lip (and palate)—A pilot study assessing functional outcomes and patients’ satisfaction with appearance. Int. J. Pediatr. Otorhinolaryngol. 2020, 128, 109692. [Google Scholar] [CrossRef]
- Goldman, A.; Wollina, U. Polymethylmethacrylate-induced nodules of the lips: Clinical presentation and management by intralesional neodymium:YAG laser therapy. Dermatol. Ther. 2019, 32, e12755. [Google Scholar] [CrossRef] [Green Version]
- Rauso, R.; Federico, F.; Zerbinati, N.; De Cicco, D.; Nicoletti, G.F.; Tartaro, G. Hyaluronic acid injections to correct lips deformity following surgical removal of permanent implant. J. Craniofac. Surg. 2020, 31, e604–e606. [Google Scholar] [CrossRef]
- Vos, T.; Flaxman, A.D.; Naghavi, M.; Lozano, R.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; Aboyans, V.; et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2163–2196. [Google Scholar] [CrossRef]
- Wollina, U. Perioral rejuvenation: Restoration of attractiveness in aging females by minimally invasive procedures. Clin. Interv. Aging 2013, 8, 1149–1155. [Google Scholar] [CrossRef] [Green Version]
- Steenen, S.A.; Bauland, C.G.; van der Lei, B.; Su, N.; van Engelen, M.D.G.; Anandbahadoer-Sitaldin, R.D.; Koeiman, W.; Jawidan, T.; Hamraz, Y.; Lange, J. Head-to-head comparison of 4 hyaluronic acid dermal fillers for lip augmentation: A multicenter randomized, quadruple-blind, controlled clinical trial. J. Am. Acad. Dermatol. 2022, 88, 932–935. [Google Scholar] [CrossRef]
- Aubry, S.; Collart-Dutilleul, P.Y.; Renaud, M.; Batifol, D.; Montal, S.; Pourreyron, L.; Carayon, D. Benefit of hyaluronic acid to treat facial aging in completely edentulous patients. J. Clin. Med. 2022, 11, 5874. [Google Scholar] [CrossRef]
- Villalobos, V.; Garrido, M.; Reyes, A.; Fernández, C.; Diaz, C.; Torres, V.A.; González, P.A.; Cáceres, M. Aging envisage imbalance of the periodontium: A keystone in oral disease and systemic health. Front. Immunol. 2022, 13, 1044334. [Google Scholar] [CrossRef]
- Tian, W.; Gao, P.; Zong, D.P.; Liu, J.J.; Zhang, M.Y.; Wang, C.C.; Wang, Z.X.; Wang, J.M.; Niu, Y.Y.; Xiang, P. The oral bioaccessibility and gingival cytotoxicity of metal(loid)s in wild vegetables from mining areas: Implication for human oral health. Front. Nutr. 2022, 9, 1042300. [Google Scholar] [CrossRef]
- Awartani, F.A.; Tatakis, D.N. Interdental papilla loss: Treatment by hyaluronic acid gel injection: A case series. Clin. Oral Investig. 2016, 20, 1775–1780. [Google Scholar] [CrossRef]
- Alhabashneh, R.; Alomari, S.; Khaleel, B.; Qinawi, H.; Alzaubi, M. Interdental papilla reconstruction using injectable hyaluronic acid: A 6 month prospective longitudinal clinical study. J. Esthet. Restor. Dent. 2021, 33, 531–537. [Google Scholar] [CrossRef]
- Lee, W.P.; Kim, H.J.; Yu, S.J.; Kim, B.O. Six month clinical evaluation of interdental papilla reconstruction with injectable hyaluronic acid gel using an image analysis system. J. Esthet. Restor. Dent. 2016, 28, 221–230. [Google Scholar] [CrossRef]
- Patil, S.C.; Dhalkari, C.D.; Indurkar, M.S. Hyaluronic acid: Ray of hope for esthetically challenging black triangles: A case series. Contemp. Clin. Dent. 2020, 11, 280–284. [Google Scholar] [CrossRef]
- Castro-Calderón, A.; Roccuzzo, A.; Ferrillo, M.; Gada, S.; González-Serrano, J.; Fonseca, M.; Molinero-Mourelle, P. Hyaluronic acid injection to restore the lost interproximal papilla: A systematic review. Acta Odontol. Scand. 2022, 80, 295–307. [Google Scholar] [CrossRef]
- Rauso, R.; Rugge, L.; Chirico, F.; Nicoletti, G.F.; Fragola, R.; Bove, P.; Zerbinati, N.; Giudice, G.L. Nonsurgical reshaping of the lower jaw with hyaluronic acid fillers: A retrospective case series. Dermatol. Pract. Concept. 2022, 12, e2022095. [Google Scholar] [CrossRef]
- Rauso, R.; Lo Giudice, G.; Zerbinati, N.; Tartaro, G. Hyaluronic acid injections as nonsurgical alternative in case of delayed diagnosis of malar arch fracture: Case report and literature review. Case Rep. Surg. 2019, 2019, 1360741. [Google Scholar] [CrossRef]
- Mowlavi, A.; Meldrum, D.G.; Kalkanis, J.; Wilhelmi, B.J.; Russell, R.C.; Zook, E.G. Surgical design and algorithm for correction of earlobe ptosis and pseudoptosis deformity. Plast. Reconstr. Surg. 2005, 115, 290–295. [Google Scholar] [CrossRef] [PubMed]
- Qian, W.; Zhang, Y.K.; Cao, Q.; Hou, Y.; Lv, W.; Fan, J.F. Clinical application of earlobe augmentation with hyaluronic acid filler in the Chinese population. Aesthetic Plast. Surg. 2017, 41, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Wollina, U. Filler-rejuvenation of the earlobes. J. Appl. Cosmetol. 2019, 37, 12–16. [Google Scholar]
- Arora, G.; Arora, S. Rejuvenating earlobe esthetics with dermal fillers. J. Cosmet. Dermatol. 2022, 21, 2788–2792. [Google Scholar] [CrossRef]
- Di Gregorio, C.; D’Arpa, S. Nonsurgical treatment of earlobe aging in Mowlavi stages I and II earlobe ptosis with Hyaluronic acid fillers. J. Cosmet. Dermatol. 2019, 18, 508–510. [Google Scholar] [CrossRef]
- Gümüş, N.; Acaban, M.B.; Demirbağ, H.O. Hyaluronic acid dermal filler promotes cartilage reshaping in rabbit ears. Aesthetic Plast. Surg. 2022, 46, 1932–1941. [Google Scholar] [CrossRef]
- Radulesco, T.; Winter, C.; Kestemont, P.; Braccini, F.; Castillo, L.; Michel, J. Liquid spreader grafts: Internal nasal valve opening with hyaluronic acid. Aesthetic Plast. Surg. 2022, 46, 2912–2916. [Google Scholar] [CrossRef]
- Gonzalez, C.D.; Pamatmat, J.J.; Goff, H.W. Safety and efficacy of dermal fillers in patients with connective tissue disease: A review. Dermatol. Surg. 2021, 47, 360–364. [Google Scholar] [CrossRef]
- Lane, T.K.; Cheung, J.; Schaffer, J.V. Parry-Romberg syndrome with coexistent morphea. Dermatol. Online J. 2008, 14, 21. [Google Scholar] [CrossRef]
- Choksi, A.N.; Orringer, J.S. Linear morphea-induced atrophy treated with hyaluronic acid filler injections. Dermatol. Surg. 2011, 37, 880–883. [Google Scholar] [CrossRef] [Green Version]
- Thareja, S.K.; Sadhwani, D.; Alan Fenske, N. En coup de sabre morphea treated with hyaluronic acid filler. Report of a case and review of the literature. Int. J. Dermatol. 2015, 54, 823–836. [Google Scholar] [CrossRef]
- Sivek, R.; Emer, J. Use of a blunt-tipped microcannula for soft tissue filler injection in the treatment of linear scleroderma (en coup de sabre). Dermatol. Surg. 2014, 40, 1439–1441. [Google Scholar] [CrossRef]
- Sharquie, K.E.; Al-Jaralla, F.; Sharquie, I.K. Intralesional injection of hyaluronic acid as a long lasting therapy of morphea sclerosis. Am. J. Dermatol. Venereol. 2019, 8, 45–48. [Google Scholar] [CrossRef]
- Owczarczyk-Saczonek, A.; Kasprowicz-Furmańczyk, M.; Kruszewska, A.; Krajewska-Włodarczyk, M.; Bechtold, A.; Klimek, P.; Placek, W. The correction of facial morphea lesions by hyaluronic acid: A case series and literature review. Dermatol. Ther. 2020, 10, 1423–1434. [Google Scholar] [CrossRef]
- Sharad, J. Hyaluronic acid filler injection for localized scleroderma—Case report and review of literature on filler injections for localized scleroderma. Clin. Cosmet. Investig. Dermatol. 2022, 15, 1627–1637. [Google Scholar] [CrossRef]
- Moore, R.M.; Mueller, M.A.; Hu, A.C.; Evans, G.R.D. Asymptomatic Stroke After Hyaluronic Acid Filler Injection: Case Report and Literature Review. Aesthetic Surg. J. 2021, 41, NP602–NP608. [Google Scholar] [CrossRef] [PubMed]
- Rzany, B.; Becker-Wegerich, P.; Bachmann, F.; Erdmann, R.; Wollina, U. Hyaluronidase in the correction of hyaluronic acid-based fillers: A review and a recommendation for use. J. Cosmet. Dermatol. 2009, 8, 317–323. [Google Scholar] [CrossRef] [Green Version]
- Zhang-Nunes, S.; Ryu, C.; Cahill, K.; Straka, D.; Nabavi, C.; Czyz, C.; Foster, J. Prospective in vivo evaluation of three different hyaluronic acid gels to varying doses of hyaluronidase with long-term follow-up. J. Plast. Reconstr. Aesthetic Surg. 2021, 74, 874–880. [Google Scholar] [CrossRef]
- Vartanian, A.J.; Frankel, A.S.; Rubin, M.G. Injected hyaluronidase reduces restylane-mediated cutaneous augmentation. Arch. Facial Plast. Surg. 2005, 7, 231–237. [Google Scholar] [CrossRef] [Green Version]
- Kato, K.; Inoue, E.; Tanaka, S.; Kawamoto, H. Increase in the incidence of acute inflammatory reactions to injectable fillers during COVID-19 era. J. Cosmet. Dermatol. 2022, 21, 1816–1821. [Google Scholar] [CrossRef] [PubMed]
- McMahon, D.E.; Amerson, E.; Rosenbach, M.; Lipoff, J.B.; Moustafa, D.; Tyagi, A.; Desai, S.R.; French, L.E.; Lim, H.W.; Thiers, B.H.; et al. Cutaneous reactions reported after Moderna and Pfizer COVID-19 vaccination: A registry-based study of 414 cases. J. Am. Acad. Dermatol. 2021, 85, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Aryanian, Z.; Balighi, K.; Emadi, S.N.; Razavi, Z.; Hatami, P.; Afshar, Z.M. COVID-19 vaccines and filler reactions: Should it be considered as a concern? J. Cosmet. Dermatol. 2022, 21, 6564–6567. [Google Scholar] [CrossRef]
- Signorini, M.; Liew, S.; Sundaram, H.; De Boulle, K.L.; Goodman, G.J.; Monheit, G.; Wu, Y.; Trindade de Almeida, A.R.; Swift, A.; Vieira Braz, A.; et al. Global Aesthetics Consensus: Avoidance and management of complications from hyaluronic acid fillers-evidence- and opinion-based review and consensus recommendations. Plast. Reconstr. Surg. 2016, 137, 961e–971e. [Google Scholar] [CrossRef]
- Philipp-Dormston, W.G.; Bergfeld, D.; Sommer, B.M.; Sattler, G.; Cotofana, S.; Snozzi, P.; Wollina, U.; Hoffmann, K.P.J.; Salavastru, C.; Fritz, K. Consensus statement on prevention and management of adverse effects following rejuvenation procedures with hyaluronic acid-based fillers. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 1088–1095. [Google Scholar] [CrossRef]
- Galadari, H.; Krompouzos, G.; Kassir, M.; Gupta, M.; Wollina, U.; Katsambas, A.; Lotti, T.; Jafferany, M.; Navarini, A.A.; Vasconcelos Berg, R.; et al. Complication of soft tissue fillers: Prevention and management review. J. Drugs Dermatol. 2020, 19, 829–832. [Google Scholar] [CrossRef]
- Heydenrych, I.; De Boulle, K.; Kapoor, K.M.; Bertossi, D. The 10-Point Plan 2021: Updated concepts for improved procedural safety during facial filler treatments. Clin. Cosmet. Investig. Dermatol. 2021, 14, 779–814. [Google Scholar] [CrossRef]
Figure 1.
Possible indications of HAF for facial rehabilitation.

Figure 2.
53-year-old patient with a traumatic scar on the glabella. (a) Before and (b) after fractional CO2 laser and superficial injection of HAF.
Figure 2.
53-year-old patient with a traumatic scar on the glabella. (a) Before and (b) after fractional CO2 laser and superficial injection of HAF.

Figure 3.
PMMA intralesional laser removal (a) and after HAF injection in the central portion of lower lip to correct irregularity (b).
Figure 3.
PMMA intralesional laser removal (a) and after HAF injection in the central portion of lower lip to correct irregularity (b).

Figure 4.
Asymmetric upper and lower lips after gnathosurgery with a flattened philtrum (a). Correction by injection of HAF in the upper lip (vermillion, philtrum, and cutaneous mucosa line) (b).
Figure 4.
Asymmetric upper and lower lips after gnathosurgery with a flattened philtrum (a). Correction by injection of HAF in the upper lip (vermillion, philtrum, and cutaneous mucosa line) (b).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Basic biophysical and rheological qualities of HAF [3].
Table 1.
Basic biophysical and rheological qualities of HAF [3].
| HA concentration | The total concentration per mL depends on crosslinked (non-soluble) and extractable (soluble) HA in each HAF |
| Crosslinking | Depends on crosslinking agent, ratio of crosslinking agent to the HA concentration, and the ratio of crosslinked agent to the total amount of the crosslinking agent |
| Hydration | The capacity of HAF to swell when in contact to phosphate-buffered NaCl |
| Elastic module (G’) | Describes the shape memory of an HAF gel under pressure |
| Viscous modulus (G’’) | Describes the behavior of HAF under shear forces (friction) |
| Complex modulus (G*) | Describes the resistance of HAF to deformation under shear forces |
| Cohesivity | A measure of internal adhesion strength |
| Tangential delta (tan δ) | The ratio of viscous to elastic quality |
Table 2.
Use of HAF in facial asymmetry (n—patient number).
| Author(s) | n | Indication(s) | HAF (HA Concentration) | Outcome |
|---|---|---|---|---|
| Pavicic et al. (2010) [19] | 2 | HIV-associated facial lipoatrophy (FAL) | Belotero balance (22.5 mg/mL) | Improvement during 24 months |
| Wollina and Goldman (2017) [20] | 2 | 1× Bell’s palsy, 1× after orthognathic surgery | Belotero balance (22.5 mg/mL) | Improvement for 6–9 months for palsy in combination with repeated treatments of botulinum toxin type A |
| Kopera et al. (2018) [21] | 53 | FAL, morphological asymmetry (MA), debilitating scars (DS) | Princess (23 mg/mL) | Success rate 100% (FLA and MA), touch-up after 2 weeks, for DS 94% follow-up 24 weeks |
| Grablowitz et al. (2020) [22] | 60 | FLA, MA, and DS | Princess (23 mg/mL) | Success rate 98% at 4 weeks, 80% at week 24, and 61% at week 36 |
Table 3.
HAF to correct acne scars.
| Author (s) | n | Treatment | Outcome |
|---|---|---|---|
| Hasson and Romero (2010) [30] | 12 | Linear threading, serial puncture, or a combination of both | Improvement moderate (27%), good (57%), and excellent (17%) |
| Halachmi et al. (2013) [31] | 12 | Low-viscosity HAF after laser treatment and discrete depressed scars | Immediate visual improvement |
| Goodman and Van den Broek (2016) [32] | 5 | Modified tower-technique, two injections, 3-month follow-up | Static objective grading scale improvement from 3.2 to 2.6 |
| Dierickx et al. (2018) [33] | 12 | Low-viscosity HAF three times, 4 weeks apart, follow-up to 36 weeks | Scar severity, self-esteem, and self-confidence improved |
| Artzi et al. 2020 [34] | 12 | Dual-plane technique, two times, 4 weeks apart | 4 weeks apart improved by 2.5 |
| Siperstein et al. (2022) [35] | 15 | Split-face study, 1mL HAF vs. 1 mL saline, one touch-up, follow-up 90 days | Quantitative global scarring grading system: –6.6 (HAF), −1.7 (saline) |
| Akerman et al. (2022) [36] | 12 | Four sessions non-ablative laser, immediate after session one and three injection of high-viscose HAF | Mild to moderate improvement in all patients and overall scar appearance improved by 1.88 |
Table 4.
Use of HAF to restore interdental papilla (BTA, black triangle area; BTH, black triangle height; BTW, black triangle width).
Table 4.
Use of HAF to restore interdental papilla (BTA, black triangle area; BTH, black triangle height; BTW, black triangle width).
| Author (s) | n | Injections Schedule | Outcome (6 Months) |
|---|---|---|---|
| Awartani and Tatakis (2016) [55] | 9 | 0.2 mL day 0 and day 21 | Lost interdental papilla area reduced from 1.2 to 0.7 |
| Lee et al. (2016) [56] | 10 | Five injections in 3 weeks | 29 of 43 sites complete restoration and 14 of 43 sites improved |
| Patil et al. (2020) [57] | 5 | <0.2 mL repeated 2–3 times | BTA decrease 0.25 mm2, BTH decrease 0.85 mm2, and BTW decrease 0.34 mm2 |
| Alhabashneh et al. (2021) [58] | 12 | 0.2 mL day 0 and day 21 | BTH reduction 29% |
Table 5.
Effect of HAF on earlobe ptosis Mowlavi grade I and II [60].
Table 5.
Effect of HAF on earlobe ptosis Mowlavi grade I and II [60].
| Author (s) | n | Treatment | Duration of Effects |
|---|---|---|---|
| Qian et al. (2017) [63] | 19 | One injection, HAF 0.3–0.5 mL | 6–9 Months |
| Wollina (2019) [64] | 26 | One injection, HAF ≤ 0.5 mL | 9–12 months |
| Di Gregorio and D’Arpa (2019) [66] | 16 | One injection, five patients with a touch-up after 5–6 months | 14 months |
Table 6.
HAF for correction of facial morphea (morphea en coup de sabre).
| Author (s) | n | Treatment | Outcome (Duration of Volumizing Effect) |
|---|---|---|---|
| Lane et al. (2008) [70] | 1 | HAF | 2 months |
| Choksi and Orringer (2011) [71] | 1 | Restylane Perlane 1 mL (20 mg HAF/mL), repeated after 5 months | 5 months |
| Mashiko et al. (2013) [24] | 1 | Restylane SubQ 1 mL (20 mg/mL) followed by Macrolane (20 mg/mL) | 12 months |
| Thareja et al. (2013) [72] | 1 | HAF, repeated after 6 months | 6 months |
| Sivek and Emer (2014) [73] | 1 | Juvederm Ultra Plus 0.8 mL (24 mg/mL) | >9 months |
| Sharquie et al. (2019) [74] | 16 | HAF, 1-2 times, 4 weeks apart | 2–24 months (stable disease, n = 6) and ≤2 months (unstable disease, n = 10) |
| Owczarczyk-Saczonek et al. (2020) [75] | 2 | HAF 0.5 mL once or twice, one week apart | Up to 1.5 years |
| Sharad (2022) [76] | 1 | Restylane Lyft 1.0 mL (20 mg/mL) plus Restylane 0.5 mL (20 mg/mL) 4 weeks later | 12 months |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Wollina, U.; Kocic, H.; Goldman, A. Hyaluronic Acid in Facial Rehabilitation—A Narrative Review. Cosmetics 2023, 10, 61. https://doi.org/10.3390/cosmetics10020061
AMA Style
Wollina U, Kocic H, Goldman A. Hyaluronic Acid in Facial Rehabilitation—A Narrative Review. Cosmetics. 2023; 10(2):61. https://doi.org/10.3390/cosmetics10020061
Chicago/Turabian StyleWollina, Uwe, Hristina Kocic, and Alberto Goldman. 2023. "Hyaluronic Acid in Facial Rehabilitation—A Narrative Review" Cosmetics 10, no. 2: 61. https://doi.org/10.3390/cosmetics10020061
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.