
Abstract
The present study was conducted to further examine recent data suggesting that pneumocystosis could be transmitted between patients and healthcare workers in the hospital environment, as has been proven with Pneumocystis-infected SCID mice and immunocompetent Balb/c mice. Using an experimental design (i.e., SCID–Balb/c mouse airborne transmission system), the present work found that healthy host-to-healthy host transmission of Pneumocystis organisms can occur, and that ‘second’ healthy contacts are able to transmit the infectious organisms to immunocompromised hosts. Further tests designed to explore the behavior of Pneumocystis organisms in the lungs of immunocompetent hosts were performed using histological and molecular approaches (e.g. testing the expression of both cyclin-dependent serine-threonine kinase and heat-shock 70 protein in Pneumocystis). The results showed Pneumocystis organisms were able to replicate in the lungs of immunocompetent hosts, which indicates these hosts are a reservoir for Pneumocystis spp.
Similar content being viewed by others


Introduction
Pneumocystis pneumonia (PcP) is a severe opportunistic infection that has a high impact on patients with AIDS and is therefore of growing importance among non-HIV-infected subjects who are submitted to immunosuppressive treatments related to malignancies, connective tissue diseases or organ transplantation [1, 2, 3, 4, 5, 6]. The source of PcP infection remains unknown. It is generally accepted that most PcP cases do not result from reactivation of endogenous latent forms, as was previously thought [7, 8, 9], but rather from de novo airborne infection contracted from unidentified exogenous sources [10, 11]. However, PCR assays to detect Pneumocystis spp. have revealed that hospitalized patients without PcP can be latently infected with Pneumocystis spp. [5, 12, 13, 14, 15, 16, 17, 18, 19]. Therefore, they might be able to transmit the organism to susceptible patients via an airborne route.
The hypothesis has practical importance, especially considering that carriers of Pneumocystis spp. in hospitals are usually more numerous than PcP patients [14]. Furthermore, there have been reports of Pneumocystis spp. being detected by molecular methods in immunocompetent contacts (i.e., mother, nurse and physician) of a hospitalized infant with PcP [20] and in immunocompetent healthcare workers who did and did not have direct contact with immunocompromised patients [21, 22]. Infection with Pneumocystis spp. could thus be transmitted in hospitals through healthcare workers. A more recent report suggested that human-to-human PcP transmission could occur from a mother to her infant on the basis of Pneumocystis jirovecii genotyping at three independent DNA loci [23].
No data are currently available about the role of human carriers in PcP transmission, but recent experimental data we obtained suggests they could represent a risk for immunosuppressed patients [24]. In that study, immunocompetent mice transiently parasitized by Pneumocystis carinii forma specialis muris (Pneumocystis muris) after close contact with infected SCID mice did transmit the infection aerially to uninfected SCID mice [24]. Thus, immunocompetent contacts of PcP patients, such as members of hospital staff who have contracted a subclinical Pneumocystis infection from PcP patients, could be able to transmit the PcP agent via the airborne route to severely immunosuppressed patients in hospitals. This possibility is being explored in a long-term study developed at the Lille-2 University Hospital (Lille, France) within the framework of the European project “Eurocarinii” (“Human Pneumocystis carinii infection in immunocompetent hosts: a public health issue in Europe.” Project QLK2-CT-2000-01369).
An additional aim of the present study was to determine whether Pneumocystis organisms are able to circulate aerially among healthy hosts. These hosts are usually able to radically eliminate the parasites from their lungs, as attested by PCR-positive results turning negative [25]. However, as long as the hosts remain infected, they are able to transmit the infection either to naïve immunocompetent hosts, like infants who will develop a primary infection, or to immunosuppressed hosts, who may then develop clinical PcP, thus amplifying the population of Pneumocystis organisms. In this manner, healthy hosts could behave as a sort of dynamic reservoir of Pneumocystis spp. These aspects were recently explored by Gigliotti et al. [26] using the same experimental design used by Dumoulin et al. [24] (i.e., airborne transmission among co-housed SCID and Balb/c mice). Gigliotti et al. [26] showed clearly that PcP infection can pass through normal hosts; in other words, immunocompetent hosts can transmit the infection to other immunocompetent hosts, and that these ‘second’ contacts are able to pass the infection on to susceptible hosts. In the present report, we describe similar results. However, in our experiments, a co-housing period of just 1 day was found to be enough for Balb/c mice to contract the infection from SCID mice with PcP. This differs from the study of Gigliotti et al. [26] which used an invariable co-housing period of 3 weeks.
Indeed, the main objective of the present work was to explore the behavior of Pneumocystis organisms in the lungs of immunocompetent hosts. Specifically, we sought to determine if the parasites carried by these hosts were able to achieve actual cell division in the host’s pulmonary alveoli or if they were viable latent forms able to pass aerially to other hosts. A strategy based on both histopathology and cell-division-cycle 2 (cdc2) gene-targeted reverse transcriptase polymerase chain reaction (RT-PCR) [27, 28] kinetic study was displayed. The findings are important since the demonstration of actual proliferation of Pneumocystis organisms in the lungs of immunocompetent hosts strengthens the recently formulated hypothesis that these hosts act as a reservoir [22, 26, 29].
Materials and Methods
Experimental Design
Two experiments were performed using Balb/c and SCID mice in this study. In both experiments all groups of mice were housed in separate HEPA-filtered air isolators, and drinking water, food and bedding were sterilized.
Experiment 1 was designed to explore the ability of immunocompetent Balb/c mice transiently infected with Pneumocystis muris (carriers) to transmit the infection to other immunocompetent Balb/c mice (contacts). Initially, Pneumocystis muris-free SCID mice (donors) were inoculated intranasally with mouse-derived Pneumocystis. Eight weeks later, Pneumocystis muris-free immunocompetent Balb/c mice were housed in close contact (i.e., in the same cage) with the Pneumocystis muris-infected donor SCID mice for 1 day (Balb/c mice group 1) or 5 days (Balb/c mice group 2) in a proportion of three donor SCID mice to seven contact Balb/c mice.
At the end of the co-housing period the following steps were taken. (i) SCID mice were sacrificed and their lungs were removed for microscopic detection of Pneumocystis muris organisms, PCR detection of Pneumocystis DNA and molecular identification of Pneumocystis muris. (ii) One carrier Balb/c mouse from group 1 and one from group 2 were each co-housed with two new uninfected SCID mice in order to verify that Pneumocystis muris-infected contacts were able to transmit the organism to susceptible hosts. (iii) The six remaining immunocompetent carrier mice from groups 1 and 2 were co-housed respectively with groups 3 and 4, each of which contained six uninfected immunocompetent contact Balb/c mice.
Each of the six mice in groups 1 and 3 were sacrificed sequentially after 1, 4, 6, 8, 12 and 22 days of co-housing. In the same way, mice from groups 2 and 4 were sacrificed sequentially after a co-housing period of 1, 3, 7, 10 and 17 days. The duration of co-housing for individual mice in all groups is presented in Table 1. Additionally, one mouse from group 4 (mouse no. 26, Table 1) was isolated and co-housed with two uninfected SCID mice in order to verify that Pneumocystis muris-infected ‘second’ contacts were able to transmit Pneumocystis infection to susceptible hosts.
Ten Pneumocystis muris-free SCID or Balb/c mice were housed separately, serving as sentinel controls. They were also sacrificed for detection of Pneumocystis muris at the same time as those from groups 1 to 4.
Experiment 2 was designed to explore the ability of Pneumocystis muris organisms transiently carried by Balb/c mice, to develop actively in their lungs. Ten Pneumocystis muris-free SCID mice (donors) were inoculated intranasally with mouse-derived Pneumocystis. Sixty days later, 18 immunocompetent Balb/c mice that were known to be Pneumocystis muris-free were co-housed with the Pneumocystis muris-infected donor SCID mice for 5 days in a proportion of five donor SCID mice to nine contact Balb/c mice in each cage. Then, carrier Balb/c mice were sacrificed and their lungs were removed sequentially at 0, 5, 9, 12, 15, 18, 21, 25, 30 and 35 days after the end of the co-housing period. Microscopic detection of Pneumocystis organisms, histological analysis [30], extraction and amplification of Pneumocystis DNA or RNA, and molecular identification of Pneumocystis muris were performed on the lungs. Serum was sampled from all Balb/c mice used in this experiment for detection of Pneumocystis-specific antibodies (see below).
Source of Mouse-Derived Pneumocystis Organisms
Mouse-derived strains of Pneumocystis muris were obtained from corticosteroid-treated Balb/c/BU mice (Lille Pasteur Institute, France), and parasite extraction was performed as described previously [31]. Parasite isolates were identified as Pneumocystis muris using molecular methods [32]. Fungal samples of mouse origin were stored in liquid nitrogen until use by means of a cryopreservation protocol used successfully for many years in our laboratory [33]. This method has proved to be efficient for obtaining viable, infectious and ultrastructurally well-preserved Pneumocystis parasites [32, 33, 34].
Source of SCID Mice
Pneumocystis muris-free 7-week-old CB17-SCID mice were used. They were obtained from a colony bred in the Pasteur Institute of Lille, France. All mice were administered dexamethasone 2 mg/ml in drinking water from 15 days pre-inoculation until 8 weeks post-inoculation. It was previously shown that even if SCID mice are basically immunosuppressed hosts, by administering dexamethasone higher and more reproducible parasite rates can be achieved [35]. Microscopy and molecular methods confirmed the absence of latent Pneumocystis infection in the lungs of SCID mice sampled prior to parasite inoculation. SCID mice were anesthetized with an intraperitoneally administered drug cocktail (ketamine hydrochloride 150 mg/kg + diazepam 2.5 mg/kg + atropine 0.75 mg/kg) then inoculated intranasally under sterile conditions with 106 Pneumocystis muris organisms per animal suspended in 25 µl of Dulbecco’s modified Eagle’s culture medium [34].
Source of Balb/c Mice
Immunocompetent Balb/c mice from a selected, known Pneumocystis muris-free colony (Charles River, France) were used as Pneumocystis contacts. By administering dexamethasone (2 mg/ml in drinking water) to 10 mice in the colony and sacrificing them 63 days later for Pneumocystis DNA or microscopic parasite detection, we were able to confirm the absence of latent Pneumocystis infection.
PCR Detection of Pneumocystis DNA
DNA was extracted using the QIAmp DNA mini-kit (QIAGEN, Courtaboeuf, France) processed according to the manufacturer’s recommendations for tissue protocol. PCR detection of Pneumocystis DNA was performed, based on the method of Wakefield et al. [36], at the large subunit of the mitochondrial ribosomal RNA gene using primers pAZ102-H and pAZ102-E. Nested-PCR with the internal primers pAZ102-X and pAZ102-Y was used when the amount of Pneumocystis muris in the sample was low and insufficient to produce a visible band on the ethidium bromide-stained gel after a single round of amplification [37]. The reaction mixtures were prepared in 1×PCR buffer (75 mM Tris HCl, pH 8.8—20 mM [NH4]2SO4—0.01% Tween 20) and contained, per 50 µl reaction, 3 mM of MgCl2, 0.5 µM of both primers (Eurogentec, Seraing, Belgium), 400 µM of each dNTP, 1 U of Goldstar DNA polymerase (Eurogentec) and 20 µl of the purified DNA in the first round of amplification. In the second round, 2 µl of the first PCR product was used, and the PCR conditions were the same as those of the first round. DNA amplification was carried out using a PTC 200 thermocycler (MJ Research, Foster City, CA, USA). The conditions for amplification were 40 cycles of denaturation at 94°C for 1.5 min, annealing at 55°C for 1.5 min and extension at 72°C for 2 min. PCR product was analyzed by electrophoresis in a 2% agarose gel and was visualized after ethidium-bromide staining. Negative controls with no added DNA were included in the DNA extraction procedure and in the amplification run.
Hybridization Method
When analysis of PCR products by direct sequencing was not possible (i.e., no amplification product was visualized on agarose gels), hybridization of PCR products with an oligonucleotide probe specific to Pneumocystis muris (IPL-M) was used as described previously [32].
RNA Extraction
In order to preserve RNA, the lung samples of both Balb/c and SCID mice used in experiment 2 were put into RNA later solution (QIAGEN) immediately after sacrifice. RNA extraction was performed using the RNAeasy Protect midi kit (QIAGEN). Briefly, lung tissues were lysed in adequate buffer and homogenized using the PT3100 system (Kinematica Polytron, Brinkmann, USA). Extraction was then performed according to the manufacturer’s instructions.
RT-PCR on cdc2 Gene
In this study, the primers used for RT-PCR were based on those previously described for the rat-derived-Pneumocystis cdc2 gene [28] and were as follows: CDC2-A (5’-ATG-GAG-CAA-TAT-CAG-AGG-TTA-GAG-3’) and CDC2-B (5’-CTA-TAG-CAC-CAC-ATT-AGA-TCT-ATT-3’). Procedures were based on single-tube RT-PCR using the Titan One Tube RT-PCR System (Roche Diagnostics, Meyran, France). Each 50 µl of reaction mixture contained 5 µl RNA, 0.5 µM of each primer, 0.2 mM of each dNTP, 4 mM of MgCl2, 5 mM of DTT, 5 to 10 U of RNase inhibitor, 5×RT-PCR buffer pH 7.5, and 1 µl of enzyme mix (AMV and Expand High Fidelity PCR-system; Roche Diagnostics).
Reaction mixtures were incubated at 50°C for 45 min and 94°C for 4 min then subjected to amplification for 30 cycles of denaturation at 94°C for 1 min, annealing at 56°C for 1 min and extension at 72°C for 1 min, followed by incubation at 72°C for 10 min. The RT-PCR products were analyzed by electrophoresis in a 1.5% agarose gel and were visualized after ethidium-bromide staining. Negative control reactions included one with RNA from a Pneumocystis muris-free mouse lung, one with a sample that had not undergone reverse transcription, and one from which the nucleic acid template was omitted in order to confirm that the PCR products were not due to contamination. Sensitivity of the cdc2 RT-PCR was evaluated on total RNA samples prepared from log-unit dilutions of Pneumocystis organisms extracted from Pneumocystis muris-infected SCID mice.
RT-PCR on Pneumocystis SA1 Gene
Specific primers of the mRNA PcSA1 gene, member of the Pneumocystis carinii heat shock protein 70 multigene family [38, 39], were used in a RT-PCR to assess organism viability. The Titan One Tube RT-PCR System (Roche Diagnostics) was again used. The reaction mixtures were identical to those described above for cdc2, and the primers or RT-PCR conditions were the same as those used by Maher et al. [38] with some modifications. Briefly, samples were incubated at 50°C for 45 min, followed by 40 cycles at 94°C for 1 min, 50°C for 1 min and 72°C for 1 min, and a final 7-min extension at 72°C. RT-PCR products were electrophoresed on 1.5% agarose gels and revealed with ethidium bromide. The negative controls were the same as those used for cdc2 RT-PCR.
Cloning, DNA Sequencing and DNA Sequence Analysis
Amplified PCR and RT-PCR products were purified by filtration using microcon 50 (Amicon, Beverly, MA, USA). Amplified RT-PCR products were cloned into the pCR2.1 vector using the TOPO TA Cloning kit (Invitrogen, Paris, France). Recombinant plasmids were sequenced in both directions using a model ABI 377 automated sequencer with the Big Dye Terminator Cycle Sequencing kit (Perkin Elmer-Applied Biosystems, Foster City, CA, USA), according to the manufacturer’s instructions. The NCBI BLAST program (www.ncbi.nlm.nih.gov/BLAST/) was used to search for sequence identity in the sequence databases.
Histological Study
Lung samples were fixed in a 10% buffered formalin solution, embedded in paraffin, sectioned (4–5 µm) and stained with hematoxylin-eosin-saffron, Masson trichromic, reticulin and orcein [30, 40]. For the detection of Pneumocystis cystic forms, Grocott’s modified methenamine silver stain was used [40].
Detection of Pneumocystis-Specific Antibodies
A Western blot assay was used to detect Pneumocystis antibody in Balb/c mouse serum diluted 1/50 [8]. The antigens used were cryopreserved Pneumocystis carinii organisms from Wistar rats with steroid-induced pneumocystosis [35]. Anti-Pneumocystis antibodies were detected using a goat anti-mouse immunoglobulin-alkaline phosphatase-labeled antibody (Southern Biotechnology, Birmingham, Ala., USA). Sera from Balb/c mice before co-housing with infected mice were used as negative controls. A monoclonal antibody specific for Pneumocystis muris (Dako, Glostrup, Denmark) was used as positive control.
Results
Pneumocystis Infection in Donor Mice
All SCID mice infected with Pneumocystis muris developed PcP with total parasite rates ranging from 5 to 20×106 organisms per animal.
Pneumocystis Carriage in Balb/c Mice after Co-Housing with Donor SCID Mice
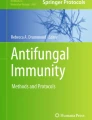
Results of PCR and microscopic examination performed on lung samples from immunocompetent Balb/c contact mice in experiment 1 are shown in Table 1. All lung samples from Balb/c mice co-housed with infected donor SCID mice for 1 or 5 days yielded positive first- or second-round PCR results (groups 1 and 2, Table 1). No mouse from group 1 (1 day of co-housing with SCID mice) showed parasites during the microscopic examination; however, rare Pneumocystis cystic forms were observed in the lung imprint of one mouse (no. 13, Table 1) from group 2 (5 days of co-housing with SCID mice) (Fig. 1).

Pneumocystis cystic forms observed in dried lung imprints of mouse no. 13 (Table 1), which was co-housed for 5 days with Pneumocystis muris-infected SCID mice (donors) and sacrificed 28 days after the end of the co-housing period. Toluidin blue stain. Direct magnification: ×1000
In experiment 2, all lung samples from the 18 contact Balb/c mice, collected from the end of the 5-day-co-housing period with the donor SCID mice through the end of the experiment (40 days), showed positive first-round PCR results at a large subunit of the mitochondrial ribosomal RNA locus (Table 2).
Pneumocystis Transmission Among Immunocompetent Hosts (Table 1)
Three of the 12 Balb/c mice in groups 3 and 4 showed positive PCR results: one mouse in group 3 (no. 20) after a 22-day-period of co-housing with mice in group 1, and two mice in group 4 (no. 25 and 26) after a 17-day co-housing period with mice in group 2. Rare cystic forms were microscopically observed in the lung imprint of mouse no. 26 (group 4).
Viability and Multiplication of Pneumocystis Organisms in Immunocompetent Carriers
All Balb/c mice in experiment 2 showed positive PcSA1 RT-PCR results, indicating that Pneumocystis organisms carried by these immunocompetent hosts were viable (Table 2). Moreover, three Balb/c mice sacrificed at 0, 5 or 21 days after the 5-day co-housing period with donor SCID mice, were found to express the cdc2 gene, suggesting that parasites were able to achieve cell division in the host lungs (Table 2).
Pneumocystis muris Large Subunit of the Mitochondrial Ribosomal RNA Gene, Heat Shock Protein 70 and cdc2 Gene Amplified Sequences
Using the Pneumocystis-specific oligonucleotide primers pAZ102-E and pAZ102-H at the large subunit of the mitochondrial ribosomal RNA locus, the sequence of amplified products identified Pneumocystis muris in positive lung samples from both the SCID and Balb/c mice from both experiments. For experiment 2, RT-PCR amplified products from PcSa1 (GenBank accession number AY382182) and cdc2 (GenBank accession number AY382183) genes were cloned, sequenced and compared with those from other fungi, humans or other Pneumocystis spp. using the NCBI Blast program. Analysis of the results obtained at the two loci showed the highest homology with rat-derived Pneumocystis. Actually, for the two amplified sequences (cdc2 and PcSa1 gene fragments) an identity of 89% was found between mouse-derived Pneumocystis and rat-derived Pneumocystis. These results allow the conclusion that sequences amplified from SCID or Balb/c mice following RT-PCR of cdc2 or PcSA1 are new Pneumocystis muris cDNA sequences.
Pneumocystis muris in the Lungs of Immunocompetent Hosts
Grocott’s modified methenamine silver stain revealed rare clustered cystic forms, closely associated with lung tissue, lining the alveolar walls of Balb/c mice sacrificed 21, 25, 30 or 35 days after the end of the 5-day co-housing period with donor SCID mice (Table 2, Fig. 2). Associated pulmonary changes were mild and parasite groups were apparently not associated with inflammatory changes. No fibrosis was observed. However, moderate mononuclear infiltrates were noted around bronchial or vascular sections. Vascular congestion and a few alveolar hemorrhagic infiltrates, surely related with post-mortem changes, were also recorded.

Pneumocystis carinii f. sp. muris in the lungs of healthy Balb/c mice. Clustered Pneumocystis cysts (arrows) attached to the alveolar epithelium (a) or placed depth in the alveolar tissue (c). This mouse contracted the Pneumocystis infection by co-housing for 5 days with SCID mice with pneumocystosis (donors). After the co-housing period the mouse was isolated from donors and sacrificed 35 days later. Direct magnification: ×160 (a) and ×200 (c). In micrographs b and d, parasitic clusters (arrows) are clearly visible closely attached to the alveolar epithelium of a healthy Balb/c mouse. It had been co-housed for 5 days with Pneumocystis-infected donor SCID mice, and then isolated from them for 21 days. Grocott’s methenamine silver stain. Direct magnification: ×1000 (b and d)
Pneumocystis-Specific Immunoglobulin in the Sera of Immunocompetent Carriers
Pneumocystis antibody was detected in the sera of the Balb/c mice as early as 17 days after the start of the 5-day co-housing period with donor mice and henceforth (Table 2).
Sentinel Mice
Ten sentinel mice (4 SCID mice and 6 Balb/c mice) sacrificed during the experiment were found to be negative by both microscopy and nested-PCR assay.
Transmission of Pneumocystis muris to SCID Mice Through Immunocompetent Balb/c Mice
Pneumocystis muris DNA was detected by PCR in all of the SCID mice (6/6) co-housed for 45 days with either the contact mice of groups 1 and 2 (no. 7 and 14, Table 1) or with one contact mouse of group 4 (no. 26, Table 1). Parasites were observed on the lung imprint of all SCID mice.
Discussion
The understanding of Pneumocystis infection mechanisms is a crucial epidemiological challenge, since the source and reservoir of the infection in humans have not yet been established. The infection can be transmitted aerially [24, 41, 42], and cross-infection experiments have shown that a Pneumocystis sp. from a given mammal cannot infect other host species [32, 34, 43, 44]. Pneumocystis jirovecii could behave in a similar manner, and humans could therefore constitute the reservoir for this species. Pneumocystis DNA has been detected consistently in hospitalized patients without PcP and in immunocompetent hospital staff members who either had or did not have contact with immunocompromised patients [20, 21, 22].
The detection of Pneumocystis carriers among immunocompetent healthcare workers led us to wonder about their role as a possible source of infection for either susceptible inpatients or other healthcare workers. Thus, a recent study was conducted by our team that demonstrated that Pneumocystis muris can be transmitted from SCID mice with PcP to immunocompetent mice, which were then able to transmit the pathogen to susceptible hosts [24]. Only 1 day of contact was enough to transmit the infection [24, 42]. In the present study the period examined was 1 or 5 days, which seems more representative of clinical situations in a nosocomial context than the 3-week co-housing period used by Gigliotti et al. [26] in a recent study.
Regarding the transmission of Pneumocystis organisms among immunocompetent hosts, the present study confirmed that immunocompetent mice transiently parasitized by Pneumocystis spp. were able to transmit the organism to other immunocompetent Pneumocystis-free mice. However, healthy host-to-healthy host transmission was not detected in all cases (3 of 12 healthy mice) and a minimal co-housing period of 17 days was required for transmission in our conditions (Table 1). In addition, we demonstrated that these ‘second’ healthy contacts were able to transmit the infection to susceptible hosts, a result that is consistent with the recent observations of Gigliotti et al. [26]. Indeed, the results of the present work suggest that even a weak parasite load is enough to transmit the infection from healthy hosts to susceptible hosts, as in the case of mouse no. 26, which contracted the infection from a healthy carrier (Table 1).
On the whole, our results show the potential importance of immunocompetent carriers in the circulation of Pneumocystis spp. in host populations. A further aim of our study was to explore the potential role of immunocompetent hosts as a reservoir for Pneumocystis organisms. Gigliotti et al. [26] showed that the infection passes through normal Balb/c mice and, from this fact, they concluded that active replication takes place in immunocompetent hosts. However, transmission may also occur by airborne transfer of latent forms of Pneumocystis spp. without increasing their population. This is a key point because only the demonstration of actual parasite replication in the lungs of immunocompetent hosts allows them to be considered reservoirs for Pneumocystis spp. For this reason, we attempted to demonstrate actual cell division of Pneumocystis in the lungs of healthy hosts.
In this part of our study, we detected Pneumocystis cdc2 mRNA in the lungs of immunocompetent Balb/c mice that had contracted a transient Pneumocystis infection by a natural airborne route from Pneumocystis muris-infected SCID mice. The cdc2 gene encodes a cyclin-dependent serine-threonine kinase whose activity is essential for cell division [45, 46, 47]. The presence of this gene has been detected previously in the genome of Pneumocystis carinii by Thomas et al. [28] and in the genome of Pneumocystis jirovecii by Kaiser et al. [48, 49], who revealed in vitro that the expression of this gene is correlated with the growth rate of the organism [48]. We successfully detected the mouse-derived Pneumocystis cdc2 gene in Balb/c mice sacrificed 5, 10 and 26 days after the start of the 5-day co-housing period, suggesting that active replication of Pneumocystis organisms occurred in these immunocompetent hosts.
The RNA preservation or extraction methods we used were validated by the fact that PcSA1 mRNA was detected in all of the lung samples of Balb/c contact mice. RT-PCR amplification of the mRNA of a member of the heat shock protein 70 family, which is usually employed to assess viability, has been reported previously for rat and human-derived Pneumocystis spp. [38, 39]. The method was successfully applied in our study enabling us to amplify for the first time the homologous mouse-derived Pneumocystis heat shock protein 70 mRNA fragment.
The histological finding of parasites in Balb/c mice sacrificed 26 to 40 days after the 5-day co-housing period provides a morphological basis for the observations resulting from the molecular approach and strengthen their significance. The presence of clustered parasites (Fig. 2) closely attached to the alveolar cells suggests that they actively replicate in this location. Further evidence of the close interaction between Pneumocystis muris and the immunocompetent host was provided by the detection of antibodies to Pneumocystis in the sera of the Balb/c contact mice, suggesting that seroconversion took place. The first detectable serum antibody response, revealed by using an anti-mouse immunoglobulin-alkaline phosphatase-labeled antibody, was observed as early as 17 days after the start of the co-housing period (Table 2). This result is consistent with a recent report describing the detection of Pneumocystis muris-specific immunoglobulin G in the sera of immunocompetent mice after about 4 weeks of co-housing with SCID mice [50].
In conclusion, our study has demonstrated that healthy hosts transiently parasitized by Pneumocystis organisms could serve as a reservoir for Pneumocystis spp. Extrapolation of these results to the natural history of human PcP leads us to hypothesize that PcP patients, immunodeficient carriers (or colonized patients) and transiently parasitized immunocompetent individuals can all play a role as both a source of infection and a reservoir of Pneumocystis jirovecii. These new data suggest that infection with Pneumocystis spp. can be transmitted in a nosocomial pattern. Prevention strategies targeting Pneumocystis carriers should therefore be defined in order to prevent the circulation of Pneumocystis spp. in the hospital environment.
References
Arend SM, Kroon FP, van’t Wout JW (1995) Pneumocystis carinii pneumonia in patients without AIDS, 1980 through 1993. An analysis of 78 cases. Arch Intern Med 155:2436–2441
Cardenal R, Medrano FJ, Varela JM, Ordonez A, Regordan C, Rincon M, Martinez A, Calderon EJ (2001) Pneumocystis carinii pneumonia in heart transplant recipients. Eur J Cardiothorac Surg 20:799–802
de Hoon JN, Peetermans WE, Bobbaers HJ (1997) Pneumocystis carinii pneumonia. Review of 32 cases in immunocompromised hosts. Acta Clin Belg 52:19–26
Pagano L, Fianchi L, Mele L, Girmenia C, Offidani M, Ricci P, Mitra ME, Picardi M, Caramatti C, Piccaluga P, Nosari A, Buelli M, Allione B, Cortelezzi A, Fabbiano F, Milone G, Invernizzi R, Martino B, Masini L, Todeschini G, Cappucci MA, Russo D, Corvatta L, Martino P, Del Favero A (2002) Pneumocystis carinii pneumonia in patients with malignant haematological diseases: 10 years’ experience of infection in GIMEMA centres. Br J Haematol 117:379–386
Sepkowitz KA, Brown AE, Armstrong D (1995) Pneumocystis carinii pneumonia without acquired immunodeficiency syndrome. More patients, same risk. Arch Intern Med 155:1125–1128
Varthalitis I, Aoun M, Daneau D, Meunier F (1993) Pneumocystis carinii pneumonia in patients with cancer. An increasing incidence. Cancer 71:481–485
Pifer LL, Hughes WT, Stagno S, Woods D (1978) Pneumocystis carinii infection: evidence for high prevalence in normal and immunosuppressed children. Pediatrics 61:35–41
Peglow SL, Smulian AG, Linke MJ, Pogue CL, Nurre S, Crisler J, Phair J, Gold JW, Armstrong D, Walzer PD (1990) Serologic responses to Pneumocystis carinii antigens in health and disease. J Infect Dis 161:296–306
Latouche S, Rabodonirina M, Mazars E (1998) Pneumocystis: the ‘carrier state’: epidemiology and transmission of human pneumocystosis. FEMS Immunol Med Microbiol 22:81–86
Peters SE, Wakefield AE, Sinclair K, Millard PR, Hopkin JM (1992) A search for Pneumocystis carinii in post-mortem lungs by DNA amplification. J Pathol 166:195–198
Keely SP, Baughman RP, Smulian AG, Dohn MN, Stringer JR (1996) Source of Pneumocystis carinii in recurrent episodes of pneumonia in AIDS patients. AIDS 10:881–888
Calderon EJ, Regordan C, Medrano FJ, Ollero M, Varela JM (1996) Pneumocystis carinii infection in patients with chronic bronchial disease. Lancet 347:977
Mazars E, Herbecq S, Szypura AS, Fruit J, Camus D, Dei-Cas E (1996) Pneumocystis carinii detection in 158 HIV-seronegative patients. J Eukaryot Microbiol 43 (Suppl):28
Nevez G, Jounieaux V, Linas MD, Guyot K, Leophonte P, Massip P, Schmit JL, Seguela JP, Camus D, Dei-Cas E, Raccurt C, Mazars E (1997) High frequency of Pneumocystis carinii sp.f. hominis colonization in HIV-negative patients. J Eukaryot Microbiol 44 (Suppl):36
Nevez G, Raccurt C, Jounieaux V, Dei-Cas E, Mazars E (1999) Pneumocystosis versus pulmonary Pneumocystis carinii colonization in HIV-negative and HIV-positive patients. AIDS 13:535–536
Nevez G, Raccurt C, Vincent P, Jounieaux V, Dei-Cas E (1999) Pulmonary colonization with Pneumocystis carinii in human immunodeficiency virus-negative patients: assessing risk with blood CD4+ T cell counts. Clin Infect Dis 29:1331–1332
Nevez G, Totet A, Raccurt C (2001) Typing of Pneumocystis carinii f.sp. hominis in patients with or without pneumocystosis. J Eukaryot Microbiol 47 (Suppl):124–125
Probst M, Ries H, Schmidt-Wieland T, Serr A (2000) Detection of Pneumocystis carinii DNA in patients with chronic lung diseases. Eur J Clin Microbiol Infect Dis 19:644–645
Wakefield AE, Lindley AR, Ambrose HE, Denis CM, Miller RF (2003) Limited asymptomatic carriage of Pneumocystis jiroveci in human immunodeficiency virus-infected patients. J Infect Dis 187:901–908
Vargas SL, Ponce CA, Gigliotti F, Ulloa AV, Prieto S, Munoz MP, Hughes WT (2000) Transmission of Pneumocystis carinii DNA from a patient with P. carinii pneumonia to immunocompetent contact health care workers. J Clin Microbiol 38:1536–1538
Miller RF, Ambrose HE, Wakefield AE (2001) Pneumocystis carinii f. sp. hominis DNA in immunocompetent health care workers in contact with patients with P. carinii pneumonia. J Clin Microbiol 39:3877–3882
Durand-Joly I, Soula F, Chabé M, Dalle JH, Lafitte JJ, Sénechal M, Pinon A, Camus D, Dei-Cas E (2003) Long-Term Colonization with Pneumocystis jirovecii in hospital staffs: a challenge to prevent nosocomial pneumocystosis. J Eukaryot Microbiol (in press)
Miller RF, Ambrose HE, Novelli V, Wakefield AE (2002) Probable mother-to-infant transmission of Pneumocystis carinii f.sp. hominis infection. J Clin Microbiol 40:1555–1557
Dumoulin A, Mazars E, Seguy N, Gargallo-Viola D, Vargas S, Cailliez JC, Aliouat EM, Wakefield AE, Dei-Cas E (2000) Transmission of Pneumocystis carinii disease from immunocompetent contacts of infected hosts to susceptible hosts. Eur J Clin Microbiol Infect Dis 19:671–678
Sepkowitz K, Schluger N, Godwin T, Armstrong D, Cerami A, Bucala R (1993) DNA amplification in experimental pneumocystosis: characterization of serum Pneumocystis carinii DNA and potential P. carinii carrier states. J Infect Dis 168:421–426
Gigliotti F, Harmsen AG, Wright TW (2003) Characterization of transmission of Pneumocystis carinii f.sp. muris through immunocompetent BALB/c mice. Infect Immun 71:3852–3856
Limper AH, Thomas CF Jr, Mubarak KK, Gustafson MP, Kottom TJ, Leof EB (1997) Characterization of the Pneumocystis carinii cyclin-dependent kinase life cycle regulatory system. J Eukaryot Microbiol 44 (Suppl):32
Thomas CF, Anders RA, Gustafson MP, Leof EB, Limper AH (1998) Pneumocystis carinii contains a functional cell-division-cycle Cdc2 homologue. Am J Respir Cell Mol Biol 18:297–306
Dei-Cas E (2000) Pneumocystis infections: the iceberg? Med Mycol 38 (Suppl 1):23–32
Dei-Cas E, Fleurisse L, Aliouat EM, Bahon-Le Capon J, Cailliez JC, Creusy C (1998) Morphological and ultrastructural methods for Pneumocystis. FEMS Immunol Med Microbiol 22:185–189
Aliouat A, Dei-Cas E, Ouaissi MA, Palluault F, Soulez B, Camus D (1993) In vitro attachment of Pneumocystis carinii from mouse and rat origin. Biol Cell 77:209–217
Durand-Joly I, Aliouat EM, Recourt C, Guyot K, Francois N, Wauquier M, Camus D, Dei-Cas E (2002) Pneumocystis carinii f.sp. hominis is not infectious for SCID mice. J Clin Microbiol 40:1862–1865
Anonymous (1996) In vitro systems in Pneumocystis research: the members of the European concerted action on Pneumocystis. Parasitol Today 12:245–249
Aliouat EM, Mazars E, Dei-Cas E, Cesbron JY, Camus D (1993) Intranasal inoculation of mouse, rat or rabbit-derived Pneumocystis in SCID mice. J Protozool Res 3:94–98
Dei-Cas E, Brun-Pascaud M, Bille-Hansen V, Allaert A, Aliouat EM (1998) Animal models of pneumocystosis. FEMS Immunol Med Microbiol 22:163–168
Wakefield AE, Pixley FJ, Banerji S, Sinclair K, Miller RF, Moxon ER, Hopkin JM (1990) Detection of Pneumocystis carinii with DNA amplification. Lancet 336:451–453
Wakefield AE (1996) DNA sequences identical to Pneumocystis carinii f. sp. carinii and Pneumocystis carinii f. sp. hominis in samples of air spora. J Clin Microbiol 34:1754–1759
Maher N, Vermund S, Lasbury M, Lee C, Bartlett M, Unnasch TR (2000) Development and evaluation of a molecular viability assay for Pneumocystis carinii. J Clin Microbiol 38:1947–1952
Maher NH, Vermund SH, Welsh DA, Dillon HK, Awooda A, Unnasch TR (2001) Development and characterization of a molecular viability assay for Pneumocystis carinii f sp hominis. J Infect Dis 183:1825–1827
Creusy C, Bahon-Le Capon J, Fleurisse L, Mullet C, Dridba M, Cailliez JC, Camus D, Dei-Cas E (1996) Pneumocystis carinii pneumonia in four mammal species: histopathology and ultrastructure. J Eukaryot Microbiol 43 (Suppl 1):47–48
Hughes WT (1982) Natural mode of acquisition for de novo infection with Pneumocystis carinii. J Infect Dis 145:842–848
Soulez B, Palluault F, Cesbron JY, Dei-Cas E, Capron A, Camus D (1991) Introduction of Pneumocystis carinii in a colony of SCID mice. J Protozool 38 (Suppl):123-125
Gigliotti F, Harmsen AG, Haidaris CG, Haidaris PJ (1993) Pneumocystis carinii is not universally transmissible between mammalian species. Infect Immun 61:2886–2890
Aliouat EM, Mazars E, Dei-Cas E, Delcourt P, Billaut P, Camus D (1994) Pneumocystis cross infection experiments using SCID mice and nude rats as recipient host, showed strong host-species specificity. J Eukaryot Microbiol 41 (Suppl):71
Nurse P (1990) Universal control mechanism regulating onset of M-phase. Nature 344:503–508
Nurse P, Thuriaux P (1980) Regulatory genes controlling mitosis in the fission yeast Schizosaccharomyces pombe. Genetics 96:627–637
Iino Y, Hiramine Y, Yamamoto M (1995) The role of cdc2 and other genes in meiosis in Schizosaccharomyces pombe. Genetics 140:1235–1245
Kaiser K, Rabodonirina M, Mayencon M, Picot S (1999) Cdc2 gene of Pneumocystis carinii hominis and its expression during culture. J Eukaryot Microbiol 46 (Suppl):130
Kaiser K, Rabodonirina M, Picot S (2001) Real time quantitative PCR and RT–PCR for analysis of Pneumocystis carinii hominis. J Microbiol Methods 45:113–118
An CL, Gigliotti F, Harmsen AG (2003) Exposure of immunocompetent adult mice to Pneumocystis carinii f. sp. muris by cohousing: growth of P. carinii f. sp. muris and host immune response. Infect Immun 71:2065–2070
Acknowledgments
This work was developed within the framework of research programs supported by the European network “Eurocarinii” (QLK2-CT-2000–01369), ANRS (“Agence Nationale de Recherche sur le SIDA”, contract No98016) and the French Ministry of Education, Research and Technology (“Programme de Recherche Fondamentale en Microbiologie et Maladies Infectieuses et Parasitaires”). I. D.-J. was supported in part by ANRS. We would like to thank C. Recourt for technical assistance.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Chabé, M., Dei-Cas, E., Creusy, C. et al. Immunocompetent Hosts as a Reservoir of Pneumocystis Organisms: Histological and RT-PCR Data Demonstrate Active Replication. Eur J Clin Microbiol Infect Dis 23, 89–97 (2004). https://doi.org/10.1007/s10096-003-1092-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10096-003-1092-2