
Abstract
Background
Mesh reinforcement has become the standard of care in the open and laparoscopic repair of inguinal hernia. Chronic pain after inguinal hernia repair is often due to nerve injury by penetrating mesh fixation devices such as staples (ST), tacks, or sutures. In several studies on hernioplasty, atraumatic mesh fixation with fibrin sealant (FS) proved to be efficient in terms of fixation strength and elasticity. Unfortunately, most of these studies did not provide a standardized follow-up and assessment of the development of chronic pain (CP) and the quality of life (QoL). Therefore, a randomized controlled trial comparing CP and QoL after FS fixation of mesh with ST in transabdominal preperitoneal hernioplasty (TAPP) was performed at our department. The primary end point of our study was to assess the patient outcome by using a visual analog scale (VAS) and the short form 36 (SF-36). The evaluation of recurrence rates was the secondary aim.
Methods
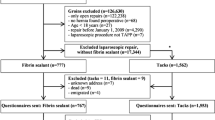
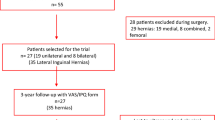
According to the randomization, a macroporous mesh (TiMESH®) was fixed in group A (44 patients with 54 inguinal hernias) with FS (TISSEEL) or in group B (45 patients with 56 inguinal hernias) with ST (EMS® Stapler). The observation period was 1 year with regular clinical check ups and assessment of VAS and SF-36.
Results
Patient characteristics expressed by BMI, ASA scores, and Schumpelick hernia classification were similar in both treatment groups. In each group there was one recurrence within 8 (FS) and 9 months (ST) postsurgery. The mean preoperative pain values scored by VAS were 1.7 (range = 0–7.5) in the FS group and 2.2 (range = 0–6) in the ST group. Postoperative mean VAS scores measured at 1 year postsurgery were 0.4 (range = 0–3) in the FS group and 0.9 (range = 0–7.5) in the ST group. One year postsurgery there was no significant difference between the two groups with respect to the parameter pain in the SF-36 and VAS.
Conclusion
Fibrin sealant fixation leads to a low rate of hernia recurrence and avoids tissue trauma. ST provide similar results in the hand of the expert but bear inherent risks of complications due to tissue perforation.




Similar content being viewed by others

References
Bittner R, Sauerland S, Schmedt CG (2005) Comparison of endoscopic techniques vs Shouldice and other open nonmesh techniques for inguinal hernia repair: a meta-analysis of randomized controlled trials. Surg Endosc 19:605–615
Hindmarsh AC, Cheong E, Lewis MP, Rhodes M (2003) Attendance at a pain clinic with severe chronic pain after open and laparoscopic inguinal hernia repairs. Br J Surg 90:1152–1154
Wijsmuller AR, Lange JF, Kleinrensink GJ, van Geldere D, Simons MP, Huygen FJ, Jeekel J, Lange JF (2007) Nerve-identifying inguinal hernia repair: a surgical anatomical study. World J Surg 31:414–420
Katkhouda N (2004) A new technique for laparoscopic hernia repair using fibrin sealant. Surg Technol Int 12:120–126
Lau H (2005) Fibrin sealant versus mechanical stapling for mesh fixation during endoscopic extraperitoneal inguinal hernioplasty: a randomized prospective trial. Ann Surg 242:670–675
Lovisetto F, Zonta S, Rota E, Mazzilli M, Bardone M, Bottero L, Faillace G, Longoni M (2007) Use of human fibrin glue (Tissucol) versus staples for mesh fixation in laparoscopic transabdominal preperitoneal hernioplasty: a prospective, randomized study. Ann Surg 245:222–231
Petter-Puchner AH, Fortelny R, Mittermayr R, Ohlinger W, Redl H (2005) Fibrin sealing versus stapling of hernia meshes in an onlay model in the rat. Hernia 9:322–329
Fortelny RH, Schwab R, Glaser KS, Puchner KU, May C, Konig F, Redl H, Petter-Puchner AH (2008) The assessment of quality of life in a trial on lightweight mesh fixation with fibrin sealant in transabdominal preperitoneal hernia repair. Hernia 12:499–505
Olmi S, Erba L, Bertolini A, Scaini A, Croce E (2006) Fibrin glue for mesh fixation in laparoscopic transabdominal preperitoneal (TAPP) hernia repair: indications, technique, and outcomes. Surg Endosc 20:1846–1850
Schwab R, Schumacher O, Junge K, Binnebosel M, Klinge U, Schumpelick V (2007) Fibrin sealant for mesh fixation in Lichtenstein repair: biomechanical analysis of different techniques. Hernia 11:139–145
Schwab R, Schumacher O, Junge K, Binnebosel M, Klinge U, Becker HP, Schumpelick V (2008) Biomechanical analyses of mesh fixation in TAPP and TEP hernia repair. Surg Endosc 22:731–738
Novik B, Hagedorn S, Mork UB, Dahlin K, Skullman S, Dalenback J (2006) Fibrin glue for securing the mesh in laparoscopic totally extraperitoneal inguinal hernia repair: a study with a 40-month prospective follow-up period. Surg Endosc 20:462–467
ten Hallers EJ, Jansen JA, Marres HA, Rakhorst G, Verkerke GJ (2007) Histological assessment of titanium and polypropylene fiber mesh implantation with and without fibrin tissue glue. J Biomed Mater Res A 80:372–380
Fortelny RH, Petter-Puchner AH, Khakpour Z, May C, Mika K, Glaser KS, Redl H (2010) Spray application of fibrin sealant with an angled spray tip device in laparoscopic inguinal hernia repair. Eur Surg 42:171–176
Fortelny RH, Petter-Puchner AH, Ferguson J, Gruber-Blum S, Brand J, Mika K, Redl H (2011) A comparative biomechanical evaluation of hernia mesh fixation by fibrin sealant. J Surg Res. doi:10.1016/j.jss.2010.06.001
Neumayer L, Giobbie-Hurder A, Jonasson O, Fitzgibbons R Jr, Dunlop D, Gibbs J, Reda D, Henderson W (2004) Open mesh versus laparoscopic mesh repair of inguinal hernia. N Engl J Med 350:1819–1827
Bittner R, Schmedt CG, Schwarz J, Kraft K, Leibl BJ (2002) Laparoscopic transperitoneal procedure for routine repair of groin hernia. Br J Surg 89:1062–1066
Schumpelick V, Treutner K-H, Arlt G (1994) Classification of inguinal hernias. Chirurg 65:877–879
Owens WD, Felts JA, Spitznagel EL Jr (1978) ASA physical status classifications: a study of consistency of ratings. Anesthesiology 49:239–243
Smith AI, Royston CM, Sedman PC (1999) Stapled and nonstapled laparoscopic transabdominal preperitoneal (TAPP) inguinal hernia repair. A prospective randomized trial. Surg Endosc 13:804–806
Bittner R, Gmähle E, Gmähle B, Schwarz J, Aasvang E, Kehlet H (2010) Lightweight mesh and noninvasive fixation: an effective concept for prevention of chronic pain with laparoscopic hernia repair (TAPP). Surg Endosc 24:2958–2964
Disclosure
Prof. Redl works as senior consultant for Baxter Biosciences. Drs. Fortelny, Petter-Puchner, May, Jaksch, and Benesch, Mr. Kkakpour, and Prof. Glaser have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Additional information
R. H. Fortelny and A. H. Petter-Puchner contributed equally to this work.
Rights and permissions
About this article
Cite this article
Fortelny, R.H., Petter-Puchner, A.H., May, C. et al. The impact of atraumatic fibrin sealant vs. staple mesh fixation in TAPP hernia repair on chronic pain and quality of life: results of a randomized controlled study. Surg Endosc 26, 249–254 (2012). https://doi.org/10.1007/s00464-011-1862-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-011-1862-3