A Systematic Review of the Extra-Hepatic Manifestations of Hepatitis E Virus Infection

 ,
,
Abstract
:1. Introduction
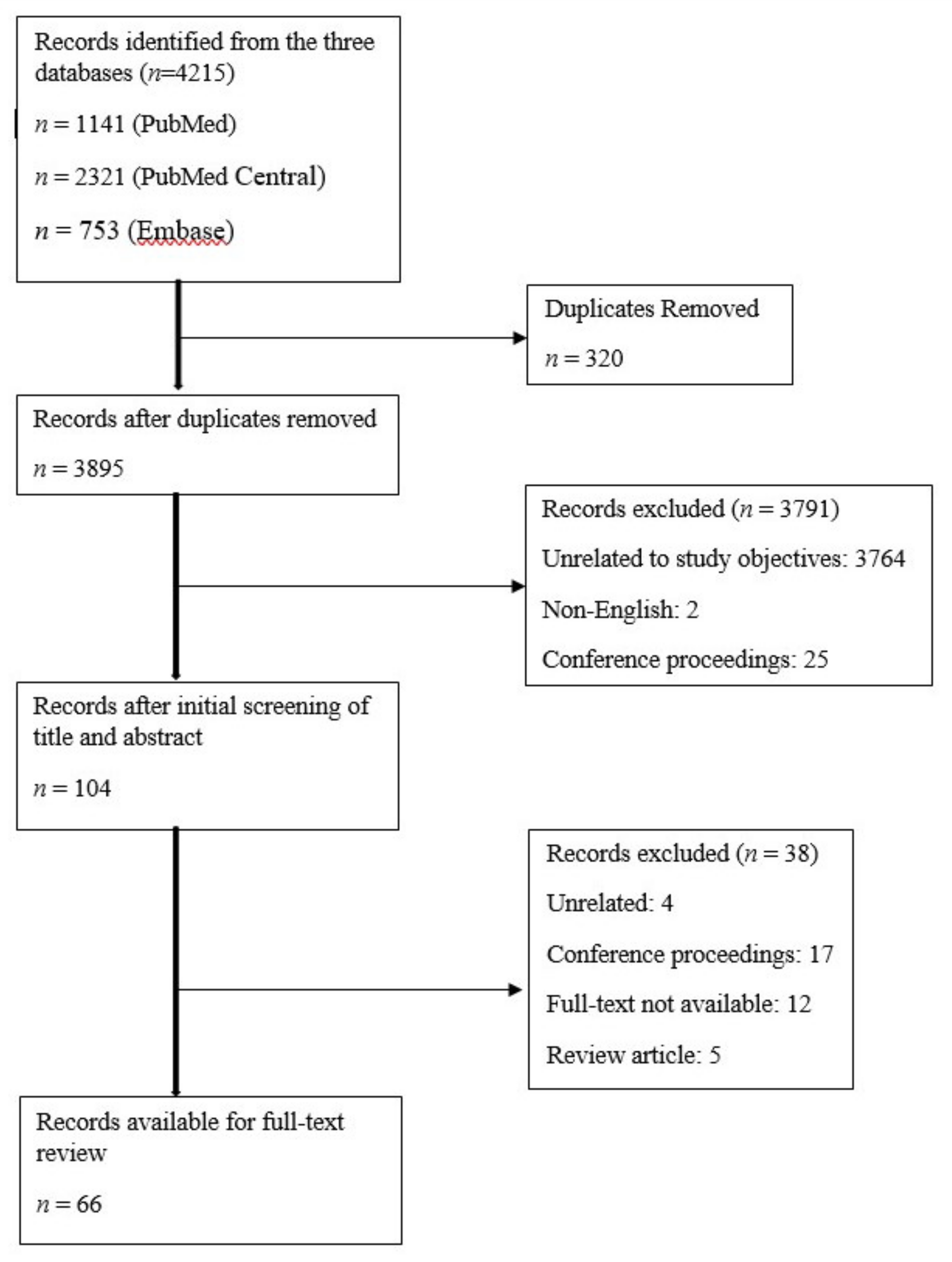
2. Methods
3. Results
3.1. Demographics
3.2. Neurological and Musculoskeletal Manifestations
3.3. Cardiovascular and Hematological Manifestations
3.4. Gastrointestinal/Pancreatico-Biliary and Miscellaneous Manifestations
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Debing, Y.; Moradpour, D.; Neyts, J.; Gouttenoire, J. Update on hepatitis E virology: Implications for clinical practice. J. Hepatol. 2016, 65, 200–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meng, X.-J. Zoonotic and Foodborne Transmission of Hepatitis E Virus. Semin. Liver Dis. 2013, 33, 41–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tengan, F.M.; Figueiredo, G.M.; Nunes, A.K.S.; Manchiero, C.; Dantas, B.P.; Magri, M.C.; Prata, T.V.G.; Nascimento, M.; Mazza, C.C.; Abdala, E.; et al. Seroprevalence of hepatitis E in adults in Brazil: a systematic review and meta-analysis. Infect. Dis. Poverty 2019, 8, 3. [Google Scholar] [CrossRef]
- Rein, D.B.; Stevens, G.A.; Theaker, J.; Wittenborn, J.S.; Wiersma, S.T. The global burden of hepatitis E virus genotypes 1 and 2 in 2005. Hepatol. 2012, 55, 988–997. [Google Scholar] [CrossRef] [PubMed]
- Bazerbachi, F.; Haffar, S. Acute fulminant vs. acute-on-chronic liver failure in hepatitis E: Diagnostic implications. Infect. Dis. 2015, 47, 112. [Google Scholar] [CrossRef] [PubMed]
- Bazerbachi, F.; Haffar, S.; Garg, S.K.; Lake, J.R. Extra-hepatic manifestations associated with hepatitis E virus infection: A comprehensive review of the literature. Gastroenterol. Rep. 2015, 4, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horvatits, T.; Ozga, A.-K.; Westhölter, D.; Hartl, J.; Manthey, C.F.; Lütgehetmann, M.; Rauch, G.; Kriston, L.; Lohse, A.W.; Bendall, R.; et al. Hepatitis E seroprevalence in the Americas: A systematic review and meta-analysis. Liver Int. 2018, 38, 1951–1964. [Google Scholar] [CrossRef]
- Kamar, N.; Izopet, J.; Dalton, H.R. Chronic hepatitis e virus infection and treatment. J. Clin. Exp. Hepatol. 2013, 3, 134–140. [Google Scholar] [CrossRef] [Green Version]
- Avila, J.D.; Lacomis, D.; Lam, E.M. Neuralgic Amyotrophy Associated with Hepatitis E Virus Infection. J. Clin. Neuromuscul. Dis. 2016, 18, 96–100. [Google Scholar] [CrossRef]
- Perrin, H.B.; Cintas, P.; Abravanel, F.; Gerolami, R.; D’Alteroche, L.; Raynal, J.-N.; Alric, L.; Dupuis, E.; Prudhomme, L.; Vaucher, E.; et al. Neurologic Disorders in Immunocompetent Patients with Autochthonous Acute Hepatitis E. Emerg. Infect. Dis. 2015, 21, 1928–1934. [Google Scholar] [CrossRef] [Green Version]
- Dalton, H.R.; Van Eijk, J.J.; Cintas, P.; Madden, R.G.; Jones, C.; Webb, G.W.; Norton, B.; Pique, J.; Lutgens, S.; Devooght-Johnson, N.; et al. Hepatitis E virus infection and acute non-traumatic neurological injury: A prospective multicentre study. J. Hepatol. 2017, 67, 925–932. [Google Scholar] [CrossRef] [PubMed]
- Dartevel, A.; Colombe, B.; Bosseray, A.; Larrat, S.; Sarrot-Reynauld, F.; Belbezier, A.; Lagrange, E.; Bouillet, L. Hepatitis E and neuralgic amyotrophy: Five cases and review of literature. J. Clin. Virol. 2015, 69, 156–164. [Google Scholar] [CrossRef] [PubMed]
- Deroux, A.; Brion, J.; Hyerle, L.; Belbézier, A.; Vaillant, M.; Mosnier, E.; Larrat, S.; Morand, P.; Pavese, P. Association between hepatitis E and neurological disorders: Two case studies and literature review. J. Clin. Virol. 2014, 60, 60–62. [Google Scholar] [CrossRef] [PubMed]
- Fong, F.; Illahi, M. Neuralgic amyotrophy associated with hepatitis E virus. Clin. Neurol. Neurosurg. 2009, 111, 193–195. [Google Scholar] [CrossRef] [PubMed]
- Fritz, M.; Berger, B.; Schemmerer, M.; Endres, D.; Wenzel, J.J.; Stich, O.; Panning, M. Pathological Cerebrospinal Fluid Findings in Patients with Neuralgic Amyotrophy and Acute Hepatitis E Virus Infection. J. Infect. Dis. 2018, 217, 1897–1901. [Google Scholar] [CrossRef]
- Jones, K.; Van Eijk, J.; Ripellino, P.; Madden, R.; Herrod, J.; Lissmann, R.; Webb, G.; Abdelrahim, M.; Ashraf, H.; Almasri, O.; et al. Clinical phenotype and outcome of hepatitis E virus associated neuralgic amyotrophy; an international retrospective comparative cohort study. J. Hepatol. 2017, 66, S59. [Google Scholar] [CrossRef]
- Azofra, M.S.; Portales, M.R.; Laureiro, L.T.; García-Samaniego, J.; Sanz, P.M. Hepatitis E virus in neurological disorders: a case of Parsonage-Turner syndrome. Revista Española de Enfermedades Digestivas 2018, 110, 402–403. [Google Scholar]
- Scanvion, Q.; Perez, T.; Cassim, F.; Outteryck, O.; Lanteri, A.; Hatron, P.-Y.; Lambert, M.; Morell-Dubois, S. Neuralgic amyotrophy triggered by hepatitis E virus: a particular phenotype. J. Neurol. 2017, 264, 770–780. [Google Scholar] [CrossRef]
- Silva, M.; Wicki, B.; Tsouni, P.; Cunningham, S.; Doerig, C.; Zanetti, G.; Aubert, V.; Sahli, R.; Moradpour, D.; Kuntzer, T. Hepatitis E virus infection as a direct cause of neuralgic amyotrophy. Muscle Nerve 2016, 54, 325–327. [Google Scholar] [CrossRef]
- Swinnen, B.; Boeynaems, S.; Schrooten, M.; Saegeman, V.; Claeys, K.G.; Van Damme, P. Anterior interosseous mononeuropathy associated with HEV infection. Neurol. Neuroimmunol. Neuroinflamm. 2018, 5, 1–3. [Google Scholar] [CrossRef] [Green Version]
- Theochari, E.; Vincent-Smith, L.; Ellis, C. Neuralgic amyotrophy complicating acute hepatitis E infection: a rare association. BMJ Case Rep. 2015, 2015, 2014–2016. [Google Scholar] [CrossRef]
- Van Eijk, J.J.; Madden, R.G.; Van Der Eijk, A.A.; Hunter, J.G.; Reimerink, J.H.; Bendall, R.P.; Pas, S.D.; Ellis, V.; Van Alfen, N.; Beynon, L.; et al. Neuralgic amyotrophy and hepatitis E virus infection. Neurol. 2014, 82, 498–503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Velay, A.; Kack-Kack, W.; Abravanel, F.; Lhomme, S.; Leyendecker, P.; Kremer, L.; Chamouard, P.; Izopet, J.; Fafi-Kremer, S.; Barth, H. Parsonage-Turner syndrome due to autochthonous acute genotype 3f hepatitis E virus infection in a nonimmunocompromised 55-year-old patient. J. NeuroVirology 2017, 23, 615–620. [Google Scholar] [CrossRef] [PubMed]
- Woolson, K.L.; Forbes, A.; Vine, L.; Beynon, L.; McElhinney, L.; Panayi, V.; Hunter, J.G.; Madden, R.G.; Glasgow, T.; Kotecha, A.; et al. Extra-hepatic manifestations of autochthonous hepatitis E infection. Aliment. Pharmacol. Ther. 2014, 40, 1282–1291. [Google Scholar] [CrossRef] [PubMed]
- Al-Saffar, A.; Al-Fatly, B. Acute Motor Axonal Neuropathy in Association with Hepatitis E. Front. Neurol. 2018, 9, 1–4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bandyopadhyay, D.; Ganesan, V.; Choudhury, C.; Kar, S.S.; Karmakar, P.; Choudhary, V.; Banerjee, P.; Bhar, D.; Hajra, A.; Layek, M.; et al. Two Uncommon Causes of Guillain-Barré Syndrome: Hepatitis E and Japanese Encephalitis. Case Rep. Neurol. Med. 2015, 2015, 1–4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choudhary, M.C.; Bajpai, V.; Anand, L.; Gupta, E. Guillain-Barré syndrome in a patient of acute Hepatitis E virus infection associated with genotype 1: Case report and literature review. Intractable Rare Dis. Res. 2019, 8, 43–47. [Google Scholar]
- Cronin, S.; McNicholas, R.; Kavanagh, E.; Reid, V.; O’Rourke, K. Anti-glycolipid GM2-positive Guillain-Barre syndrome due to hepatitis E infection. Ir. J. Med. Sci. 2011, 180, 255–257. [Google Scholar] [CrossRef]
- Fukae, J.; Tsugawa, J.; Ouma, S.; Umezu, T.; Kusunoki, S.; Tsuboi, Y. Guillain–Barré and Miller Fisher syndromes in patients with anti-hepatitis E virus antibody: a hospital-based survey in Japan. Neurol. Sci. 2016, 37, 1849–1851. [Google Scholar] [CrossRef]
- Higuchi, M.; Fukae, J.; Tsugawa, J.; Ouma, S.; Takahashi, K.; Mishiro, S.; Tsuboi, Y. Dysgeusia in a Patient with Guillain-Barré Syndrome Associated with Acute Hepatitis E: A Case Report and Literature Review. Intern. Med. 2015, 54, 1543–1546. [Google Scholar] [CrossRef] [Green Version]
- Lei, J.; Tian, Y.; Luo, H.; Chen, Z.; Peng, F. Guillain–Barre Syndrome Following Acute Co-Super-Infection of Hepatitis E Virus and Cytomegalovirus in a Chronic Hepatitis B Virus Carrier. J. Med. Virol. 2017, 19, 368–372. [Google Scholar] [CrossRef] [PubMed]
- Loly, J.P.; Rikir, E.; Seivert, M.; Legros, E.; Defrance, P.; Belaiche, J.; Moonen, G.; Delwaide, J. Guillain-Barré syndrome following hepatitis E. World J. Gastroenterol. 2009, 15, 1645–1647. [Google Scholar] [CrossRef]
- Maurissen, I.; Jeurissen, A.; Strauven, T.; Sprengers, D.; De Schepper, B. First case of anti-ganglioside GM1-positive Guillain-Barré syndrome due to hepatitis e virus infection. Infection 2012, 40, 323–326. [Google Scholar] [CrossRef] [PubMed]
- Salim, O.J.; Davidson, A.; Li, K.; Leach, J.P.; Heath, C. Brainstem encephalitis and acute polyneuropathy associated with hepatitis E infection. BMJ Case Rep. 2017, 2017, 2–5. [Google Scholar] [CrossRef] [PubMed]
- Santos, L.; Mesquita, J.; Pereira, N.R.; Lima-Alves, C.; Serrao, R.; Figueiredo, P.; Reis, J.; Simões, J.; Nascimento, M.; Sarmento, A. Acute hepatitis E complicated by Guillain-Barré syndrome in Portugal, December 2012—A case report. Eurosurveillance 2013, 18, 20563. [Google Scholar] [CrossRef] [PubMed]
- Scharn, N.; Ganzenmueller, T.; Wenzel, J.J.; Dengler, R.; Heim, A.; Wegner, F. Guillain-Barré syndrome associated with autochthonous infection by hepatitis E virus subgenotype 3c. Infection 2014, 42, 171–173. [Google Scholar] [CrossRef] [PubMed]
- Stevens, O.; Poesen, K.; Saegeman, V.; Claeys, K.G.; Van Damme, P. Diagnostic Challenges and Clinical Characteristics of Hepatitis E Virus–Associated Guillain-Barré Syndrome. JAMA Neurol. 2017, 74, 26. [Google Scholar] [CrossRef]
- Berg, B.V.D.; Van Der Eijk, A.A.; Pas, S.D.; Hunter, J.; Madden, R.G.; Tio-Gillen, A.P.; Dalton, H.R.; Jacobs, B.C. Guillain-Barre syndrome associated with preceding hepatitis E virus infection. Neurol. 2014, 82, 491–497. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, S.; Wu, J.; Jiang, Y.; Zhang, H.; Li, S.; Liu, H.; Yang, C.; Tang, H.; Guo, N.; et al. Hepatitis E virus infection in acute non-traumatic neuropathy: A large prospective case-control study in China. EBioMedicine 2018, 36, 122–130. [Google Scholar] [CrossRef] [Green Version]
- Zheng, X.; Yu, L.; Xu, Q.; Gu, S.; Tang, L. Guillain-Barre syndrome caused by hepatitis E infection: Case report and literature review. BMC Infect. Dis. 2018, 18, 50. [Google Scholar] [CrossRef]
- Murkey, J.A.; Chew, K.W.; Carlson, M.; Shannon, C.L.; Sirohi, D.; Sample, H.A.; Wilson, M.R.; Vespa, P.; Humphries, R.M.; Miller, S.; et al. Hepatitis E Virus-Associated Meningoencephalitis in a Lung Transplant Recipient Diagnosed by Clinical Metagenomic Sequencing. Open Forum Infect. Dis. 2017, 4, ofx121. [Google Scholar] [CrossRef] [PubMed]
- Belbezier, A.; Deroux, A.; Sarrot-Reynauld, F.; Larrat, S.; Bouillet, L. Myasthenia Gravis Associated with Acute Hepatitis E Infection in Immunocompetent Woman. Emerg. Infect. Dis. 2014, 20, 908–910. [Google Scholar] [CrossRef] [PubMed]
- Belliere, J.; Abravanel, F.; Nogier, M.B.; Martinez, S.; Cintas, P.; Lhomme, S.; Lavayssière, L.; Cointault, O.; Faguer, S.; Izopet, J.; et al. Transfusion-acquired hepatitis E infection misdiagnosed as severe critical illness polyneuromyopathy in a heart transplant patient. Transpl. Infect. Dis. 2017, 19, e12784. [Google Scholar] [CrossRef]
- Despierres, L.-A.; Kaphan, E.; Shahram Attarian, S.C.-B.; Pelletier, J.; Pouget, J.; Motte, A.; Charrel, R.; Gerolami, R.; Colson, P. Neurologic Disorders and Hepatitis E, France, 2010. J. Infect. 2011, 17, 1510–1513. [Google Scholar]
- A De Vries, M.; A Samijn, J.P.; De Man, R.; Boots, J.M.M. Hepatitis E-associated encephalopathy in a renal transplant recipient. BMJ Case Rep. 2014, 2014, 1–4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jha, A.K.; Nijhawan, S.; Nepalia, S.; Suchismita, A. Association of Bell’s Palsy with Hepatitis E Virus Infection: A Rare Entity. J. Clin. Exp. Hepatol. 2012, 2, 88–90. [Google Scholar] [CrossRef] [Green Version]
- Yazaki, Y.; Sugawara, K.; Honda, M.; Ohnishi, H.; Nagashima, S.; Takahashi, M.; Okamoto, H. Characteristics of 20 Patients with Autochthonous Acute Hepatitis E in Hokkaido, Japan: First Report of Bilateral Facial Palsy Following the Infection with Genotype 4 Hepatitis E Virus. Tohoku J. Exp. Med. 2015, 236, 263–271. [Google Scholar] [CrossRef] [Green Version]
- Pasha, S.A.; Pasha, S.A.; Suhasini, T.; Rao, D.A. Hepatitis E Virus-Associated Acute Encephalitic Parkinsonism. J. Assoc. Physicians India 2018, 66, 87–88. [Google Scholar]
- Sarkar, P.; Morgan, C.; Ijaz, S. Transverse myelitis caused by hepatitis E: previously undescribed in adults. BMJ Case Rep. 2015, 2015, 2014–2016. [Google Scholar] [CrossRef] [Green Version]
- Bennett, S.; Li, K.; Gunson, R.N. Hepatitis E virus infection presenting with paraesthesia. Scott. Med J. 2015, 60, e27–e29. [Google Scholar] [CrossRef]
- Mengel, A.M.; Stenzel, W.; Meisel, A.; Büning, C. Hepatitis E-induced severe myositis. Muscle Nerve 2016, 53, 317–320. [Google Scholar] [CrossRef]
- Kamar, N.; Izopet, J.; Cintas, P.; Garrouste, C.; Uro-Coste, E.; Cointault, O.; Rostaing, L. Hepatitis e virus-induced neurological symptoms in a kidney-transplant patient with chronic hepatitis: Case report. Am. J. Transpl. 2010, 10, 1321–1324. [Google Scholar] [CrossRef] [PubMed]
- Blayney, L.; Morrish, P. Acute hepatitis E infection as a cause of unexplained neurological symptoms. BMJ Case Rep. 2018, 2018, 9–11. [Google Scholar] [CrossRef] [PubMed]
- Alpers, E.C.; Smith, K.D. Cryoglobulinemia and renal disease. Curr. Opin. Nephrol. Hypertens. 2008, 17, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Marion, O.; Abravanel, F.; Del Bello, A.; Esposito, L.; Lhomme, S.; Puissant-Lubrano, B.; Alric, L.; Faguer, S.; Izopet, J.; Kamar, N. Hepatitis E virus-associated cryoglobulinemia in solid-organ-transplant recipients. Liver Int. 2018, 38, 2178–2189. [Google Scholar] [CrossRef]
- Premkumar, M.; Rangegowda, D.; Vashishtha, C.; Bhatia, V.; Khumuckham, J.S.; Kumar, B. Acute Viral Hepatitis E Is Associated with the Development of Myocarditis. Case Rep. Hepatol. 2015, 2015, 1–6. [Google Scholar] [CrossRef]
- Dougherty, T.; Bashir, S.; Adam, M.K.J.; Borum, M. Acute Myopericarditis due to Hepatitis E Virus Infection: The First Reported Case in the Western Hemisphere. J. Gastrointest. Dig. Syst. 2016, 6, 5–6. [Google Scholar] [CrossRef]
- Aiqin, Z.; Dongming, X.; Kejun, T.; Yun, Z. Long Qt Syndrome and Torsades De Points in a Patient with Acute Hepatitis E Virus Infection: An Unusual Case. Hear. 2012, 98, E222–E223. [Google Scholar] [CrossRef] [Green Version]
- Kishore, J.; Sen, M. Parvovirus B19-induced Thrombocytopenia and Anemia in a Child with Fatal Fulminant Hepatic Failure Coinfected with Hepatitis A and E Viruses. J. Trop. Pediatr. 2009, 55, 335–337. [Google Scholar] [CrossRef] [Green Version]
- Saarwaani, V.; Prabhu, M.; Weena, S.; Saraschandra, V. Multiorgan Dysfunction from Hepatitis E infection. Crit. Care Med. 2017, 46, 240. [Google Scholar]
- Karki, P.; Malik, S.; Mallick, B.; Sharma, V.; Rana, S.S. Massive Hemolysis Causing Renal Failure in Acute Hepatitis E Infection. JCTH 2016, 4, 345–347. [Google Scholar] [PubMed] [Green Version]
- Deniel, C.; Coton, T.; Brardjanian, S.; Guisset, M.; Nicand, E.; Simon, F. Acute pancreatitis: A rare complication of acute hepatitis E. J. Clin. Virol. 2011, 51, 202–204. [Google Scholar] [CrossRef] [PubMed]
- Mithun, R.; Kumar, K.; Ghoshal , U.C.; Saraswat, V.A.; Aggarwal, R.; Mohindra, S. Acute hepatitis E-associated acute pancreatitis a single center experience and literature review. Pancreas 2015, 44, 1320–1322. [Google Scholar]
- Peter, J.; Stallmach, A.; Tannapfel, A.; Bruns, T. Acute-on-Chronic Liver Failure with Complicating Pancreatitis After Autochthonous Hepatitis E Infection. Zahedan J. Res. Med Sci. 2017, 17, 1–4. [Google Scholar] [CrossRef]
- Sinha, S.; Jha, R.; Lakhtakia, S.; Narayan, G. Acute pancreatitis following kidney transplantation—Role of viral infections. Clin. Transplant. 2003, 17, 32–36. [Google Scholar] [CrossRef]
- Somani, S.K.; Ghosh, A.; Awasthi, G. Severe acute pancreatitis with pseudocyst bleeding due to hepatitis e virus infection. Clin. J. Gastroenterol. 2009, 2, 39–42. [Google Scholar] [CrossRef]
- Thakur, A.; Basu, P.P. Acute Non-Fulminant Viral Hepatitis E Presenting with Acute Pancreatitis—An Unusual Presentation. MJMS 2017, 24, 102–105. [Google Scholar] [CrossRef]
- Fujioka, K.; Nishimura, T.; Seki, M.; Kinoshita, M.; Mishima, N.; Irimajiri, S.; Yamato, M. Genotype 1 hepatitis E virus infection with acute acalculous cholecystitis as an extrahepatic symptom: a case report. Trop. Med. Heal. 2016, 44, 18. [Google Scholar] [CrossRef] [Green Version]
- Dumoulin, F.L.; Liese, H. Acute hepatitis E virus infection and autoimmune thyroiditis: yet another trigger? BMJ Case Rep. 2012, 2012, 2011–2012. [Google Scholar] [CrossRef] [Green Version]
- Mallet, V.; Bruneau, J.; Zuber, J.; Alanio, C.; Leclerc-Mercier, S.; Roque-Afonso, A.M.; Kraft, A.R.M.; Couronné, L.; Roulot, D.; Wedemeyer, H.; et al. Hepatitis E virus-induced primary cutaneous CD30(+) T cell lymphoproliferative disorder. J. Hepatol. 2017, 67, 1–26. [Google Scholar] [CrossRef]
- Hillebrandt, K.H.; Arsenic, R.; Hofmann, J.; Eurich, D.; Gül, S.; Strücker, B.; Sauer, I.M.; Pratschke, J.; Stockmann, M.; Raschzok, N. Acute Graft Dysfunction 17 Years After Liver Transplant: A Challenging Clinical and Histologic Manifestation of Hepatitis E. Exp. Clin. Transplant. 2018, 16, 348–351. [Google Scholar] [PubMed]
- Del Bello, A.; Guilbeau-Frugier, C.; Josse, A.-G.; Rostaing, L.; Izopet, J.; Kamar, N. Successful treatment of hepatitis E virus-associated cryoglobulinemic membranoproliferative glomerulonephritis with ribavirin. Transpl. Infect. Dis. 2015, 17, 279–283. [Google Scholar] [CrossRef] [PubMed]
- Guinault, D.; Ribes, D.; Delas, A.; Milongo, D.; Abravanel, F.; Puissant-Lubrano, B.; Izopet, J.; Kamar, N. Hepatitis E Virus–Induced Cryoglobulinemic Glomerulonephritis in a Nonimmunocompromised Person. Am. J. Kidney Dis. 2016, 67, 660–663. [Google Scholar] [CrossRef]
- Kumar, K.; Kumar, H.K.; Manjunath, V.; Umesh, L.; Kj, K.; Hc, K.K.; Vg, M.; L, U. Pleural effusion: A rare complication of co-infection of hepatitis A and hepatitis E. Ann. Trop. Med. Public Heal. 2012, 5, 532. [Google Scholar] [CrossRef]
- Kamar, N.; Abravanel, F.; Lhomme, S.; Rostaing, L.; Izopet, J. Hepatitis E virus: Chronic infection, extra-hepatic manifestations, and treatment. Clin. Res. Hepatol Gastroenterol 2014, 39, 1–8. [Google Scholar] [CrossRef] [PubMed]
- McLean, B.N.; Gulliver, J.; Dalton, H.R. Hepatitis E virus and neurological disorders. Pr. Neurol. 2017, 17, 282–288. [Google Scholar] [CrossRef]
- Dalton, H.R.; Kamar, N.; Van Eijk, J.J.J.; Mclean, B.N.; Cintas, P.; Bendall, R.P.; Jacobs, B.C. Hepatitis E virus and neurological injury. Nat. Rev. Neurol. 2016, 12, 77–85. [Google Scholar] [CrossRef]
- Brown, L.M.; Gridley, G.; Check, D.; Landgren, O. Risk of multiple myeloma and monoclonal gammopathy of undetermined significance among white and black male United States veterans with prior autoimmune, infectious, inflammatory, and allergic disorders. Blood 2008, 111, 3388–3394. [Google Scholar] [CrossRef] [Green Version]
- Maso, L.D.; Franceschi, S. Hepatitis C Virus and Risk of Lymphoma and Other Lymphoid Neoplasms: A Meta-analysis of Epidemiologic Studies. Cancer Epidemiol. Biomark. Prev. 2006, 15, 2078–2085. [Google Scholar] [CrossRef] [Green Version]
- Shenoy, R.; Nair, S.; Kamath, N. Thrombocytopenia in hepatitis A--An atypical presentation. J. Trop. Pediatr. 2004, 50, 241–244. [Google Scholar] [CrossRef] [Green Version]
- Ji, S.B.; Lee, S.S.; Jung, H.C.; Kim, H.J.; Kim, H.J.; Kim, T.H.; Jung, W.T.; Lee, O.J.; Song, D.H. A Korean patient with Guillain-Barré syndrome following acute hepatitis E whose cholestasis resolved with steroid therapy. Clin. Mol. Hepatol. 2016, 22, 396–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| S. No | Disorder | First Author (Year, Study Design) | Number of Patients |
|---|---|---|---|
| 1 | Guillain–Barré syndrome | Al-Saffar (2018, CR) [25], Bandyopadhyay (2015, CR) [26], Blasco-Perin * (2015, RS) [10], Choudhary (2019, CR) [27], Cronin (2011, CR) [28], Fukae * (2016, CC) [29], Higuchi (2015, CR) [30], Ji (2016, CR) [54], Lei (2017, CR) [31], Loly (2009, CR) [32], Maurissen (2012, CR) [33], Salim (2017, CR) [34], Santos (2012, CR) [35], Scharn (2014, CR) [36], Stevens (2015, RS) [37], Van Den Berg (2014, CC) [38], Wang (2018, CC) [39], Woolson (2014, RS) [24], Zheng (2018, CR) [40]. | 36 |
| 2 | Neuralgic amyotrophy (Parsonage Turner syndrome/Brachial neuritis) | Avila (2016, CR) [9], Blasco-Perin (2015, RS) [10], Dalton (2017, CSS) [11]. Dartevel (2015, CS) [12], Deroux (2014, CS) [13], Fong (2009, CR) [14], Frtiz (2018, CC) [15], Jones (2017, RS) [16], Sanchez-Azofra (2018, CR) [17], Scanvion (2017, CR) [18], Silva (2016, CR) [19], Swinnen # (2018, CR) [20], Theochari (2015, CR) [21], Van Eijk (2014, Cohort) [22], Velay (2017, CR) [23], Woolson (2014, RS) [24]. | 102 |
| 3 | Myasthenia gravis | Belbeizer (2014, CR) [42] | 1 |
| 4 | Polyneuromyopathy | Belliere (2017, CR), [43] Woolson (2014, RS) [24] | 2 |
| 5 | Mononeuritis multiplex | Blasco-Perin (2015, RS) [10] | 6 |
| 6 | Meningo-radiculitis | Blasco-Perin (2015, RS), [10] Despierres (2011, CS) [44] | 5 |
| 7 | Non-specific symptoms | Blayney (2018, CR), [53] Kamar (2010, CR) [52] | 2 |
| 8 | Cerebral ischemia | Dalton (2017, CSS), [11] Wang (2018, CC) [39] | 5 |
| 9 | Epilepsy | Dalton (2017, CSS) [11] | 2 |
| 10 | Encephalitis | Dalton (2017, CSS) [11], Deroux (2014, CS) [13], Murkey (2017, CR) [41], Wang (2018, CC) [39] | 5 |
| 11 | Facial nerve palsy | Dalton (2017, CSS) [11], Jha (2012, CR) [46], Yazaki (2015, CS) [47] | 3 |
| 12 | Encephalopathy | De Vries (2014, CR) [45] | 1 |
| 13 | Encephalitic Parkinsonism | Pasha (2018, CR) [48] | 1 |
| 14 | Transverse myelitis | Sarkar (2015, CR) [49] | 1 |
| 15 | Peripheral neuropathy | Bennet (2015, CR) [50], Wang (2018, CC) [39], Woolson (2014, RS) [24] | 3 |
| 16 | Vestibular neuritis | Woolson (2014, RS) [24] | 1 |
| 17 | Small fiber neuropathy | Woolson (2014, RS) [24] | 1 |
| 18 | Myositis | Mengel (2016, CR) [51] | 1 |
| S. No | Disorder | First Author (Year, Study Design) | Number of Patients |
|---|---|---|---|
| 1 | Cardiac Arrhythmia | Woolson (2014, RS) [24] | 1 |
| 2 | Long QT Syndrome and Torsade’s de pointes | Aiqin (2012, CR) [58] | 1 |
| 3 | Myocarditis | Dougherty (2016, CR) [57], Premkumar (2015, CR) [56] | 2 |
| 4 | Anemia | Kishore (2009, CR) [59] | 1 |
| 5 | Thrombocytopenia | Kishore (2009, CR) [58], Woolson (2014, RS) [24] | 13 |
| 6 | Lymphocytosis | Woolson (2014, RS) [24] | 14 |
| 7 | Lymphopenia | Woolson (2014, RS) [24] | 8 |
| 8 | Leukocytosis | Saarwaani (2017, CR) [60] | 1 |
| 9 | Massive hemolysis | Karki (2016, CR) [61] | 1 |
| 10 | Monoclonal gammopathy | Woolson (2014, RS) [24] | 17 |
| 11 | Cryoglobulinemia | Marion (2018, CC) [55] | 51 |
| 12 | Metabolic acidosis | Saarwaani (2017, CR) [60] | 1 |
| 13 | Malignancies (Acute myeloid leukemia, plasmacytoma) | Woolson (2014, RS) [24] | 2 |
| S. No | Disorder | System | First Author (Year, Study Design) | No. of Patients |
|---|---|---|---|---|
| 1 | Autoimmune Thyroiditis | Endocrine | Dumoulin (2012, CR) [69] | 1 |
| 2 | Cutaneous T-Cell lymphoproliferative disorder | Dermatology | Mallet (2017, CR) [70] | 1 |
| 3 | Pancreatitis | Gastro-intestinal | Deniel (2011, CR) [62], Mithun (2015, RS) [63], Peter (2017, CR) [64], Saarwaani (2017, CR) [60], Sinha (2003, CS) [65], Somani (2009, CR) [66], Thakur (2017, CR) [67] | 22 |
| 4 | Pancreatic pseudocyst | Gastro-intestinal | Somani (2009, CR) [66] | 1 |
| 5 | Acalculous cholecystitis | Gastro-intestinal | Fujioka (2016, CR) [68] | 1 |
| 6 | Acute Graft Dysfunction | Immunology | Hillebrandt (2018, CR) [71] | 1 |
| 7 | Acute Kidney Injury | Renal | Karki (2016, CR) [61], Saarwaani (2017, CR) [60] | 2 |
| 8 | cryoglobulinemic membranoproliferative glomerulonephritis | Renal | Del Bello (2015, CR) [72], Guinault (2016, CR) [73] | 2 |
| 9 | Pleural Effusion | Respiratory | Kumar (2012, CR) [74] | 1 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rawla, P.; Raj, J.P.; Kannemkuzhiyil, A.J.; Aluru, J.S.; Thandra, K.C.; Gajendran, M. A Systematic Review of the Extra-Hepatic Manifestations of Hepatitis E Virus Infection. Med. Sci. 2020, 8, 9. https://doi.org/10.3390/medsci8010009
Rawla P, Raj JP, Kannemkuzhiyil AJ, Aluru JS, Thandra KC, Gajendran M. A Systematic Review of the Extra-Hepatic Manifestations of Hepatitis E Virus Infection. Medical Sciences. 2020; 8(1):9. https://doi.org/10.3390/medsci8010009
Chicago/Turabian StyleRawla, Prashanth, Jeffrey Pradeep Raj, Alan Jose Kannemkuzhiyil, John Sukumar Aluru, Krishna Chaitanya Thandra, and Mahesh Gajendran. 2020. "A Systematic Review of the Extra-Hepatic Manifestations of Hepatitis E Virus Infection" Medical Sciences 8, no. 1: 9. https://doi.org/10.3390/medsci8010009