
Porcine Xenograft and Epidermal Fully Synthetic Skin Substitutes in the Treatment of Partial-Thickness Burns: A Literature Review

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Retrieval
2.2. Study Selection
2.3. Exclusions
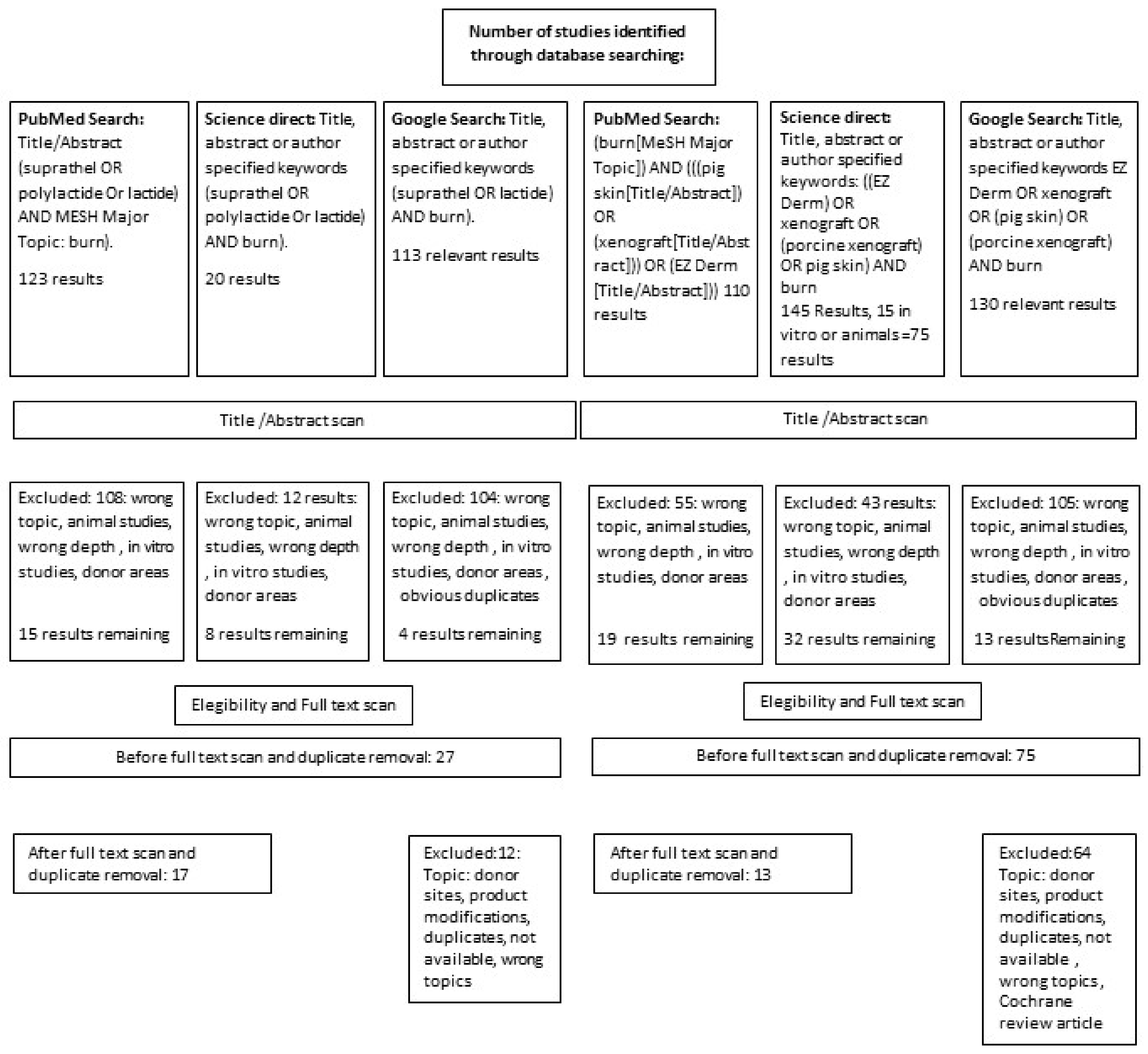
2.4. Search Method and Search Results Based on the PRISMA Flow Chart
2.5. Statistics
2.6. Effect Size of Treatment Modalities
3. Results
3.1. Quality of Studies
3.2. Inclusion Criteria
3.3. Biocompatibility and Systemic Effects
3.4. Wound Preparation
3.4.1. Wound Bed Preparation
3.4.2. Template Fixation
3.4.3. Separation Layer
3.5. Healing Time
3.5.1. Healing Time in Partial Thickness Burns
3.5.2. ST Studies
3.5.3. PX Studies
3.6. Change of the Templates or Discontinuation of Treatment
3.7. Auto-Grafting as Indicator for Burn Wound Conversion
3.8. Infection Rates in Partial Thickness Burns
3.8.1. Infection Rate ST
3.8.2. Infection Rate PX
3.9. Pain Reduction
3.10. Frequency of the Secondary Dressing Changes
3.11. Outpatient Visits and Hospital Length of Stay
3.12. Results of the Literature Review on Other Indications for Epidermal Templates in Burns Treatment
3.13. Results from the Literature on Oxidative Stress during Burns Treatment
4. Discussion
4.1. General Aspects
4.1.1. Viral and Prion Safety
4.1.2. Biocompatibility
4.1.3. Ethical and Religious Considerations for a Replacement Decision
4.2. Usability
4.2.1. The Usability in Donor Areas
4.2.2. Covering Keratinocytes
4.2.3. The Use as a Sandwich Technique
4.2.4. The Use for Preparation of the Wound Bed by Xenografts
4.3. The Use of the Products to Provide Undisturbed Wound Healing
4.3.1. Healing Time
Healing Time in Partial Thickness Burns
Mixed and Deep Partial Thickness Burns
4.3.2. Burn Wound Progression
4.3.3. Temporary Cover of Full Thickness Burns
4.3.4. Use as a Dermal Template in Supporting Tissue Replacement and to Bridge Time to Availability of Donor Skin or CEA
4.4. Pain Reduction
4.5. Infection Rates
4.6. Grafting Rates in Partial Thickness Burns
4.7. The Frequency of Outer Dressing Changes
4.8. Hospital LOS
4.9. Use of Both Product Categories in Other Fields of Trauma
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ST: | Suprathel® |
| PX: | Porcine xenograft |
| TNF-α: | Tumor Necrosis Factor Alpha |
| TEN: | Toxic Epidermal Necrolysis |
| LOS: | Length of stay |
| VAS: | Visual Analogue Scale |
| PPPM: | Parents Postoperative Pain Measurement |
| ns: | not significant |
References
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bravata, D.M.; Olkin, I. Simple pooling versus combining in meta-analysis. Eval. Health Prof. 2001, 24, 218–230. [Google Scholar]
- Two Sample T-Test (Welch’s T-test) n.d. Available online: https://www.statskingdom.com/150MeanT2uneq.html (accessed on 15 March 2021).
- Blome-Eberwein, S.A.A.; Amani, H.; Lozano, D.D.D.; Gogal, C.; Boorse, D.; Pagella, P. A bio-degradable synthetic membrane to treat superficial and deep second degree burn wounds in adults and children—4 year experience. Burns 2020, 46, 1571–1584. [Google Scholar] [CrossRef] [PubMed]
- Everett, M.; Massand, S.; Davis, W.; Burkey, B.; Glat, P. Use of a copolymer dressing on superficial and partial-thickness burns in a paediatric population. J. Wound Care 2015, 24, S4–S8. [Google Scholar] [CrossRef]
- Fischer, S.; Kremer, T.; Horter, J.; Schaefer, A.; Ziegler, B.; Kneser, U.; Hirche, C. Suprathel® for severe burns in the elderly: Case report and review of the literature. Burns 2016, 42, e86–e92. [Google Scholar] [CrossRef]
- Glat, P.M.; Burkey, B.; Davis, W. The use of Suprathel in the treatment of pediatric burns: Retrospective review of first pilot trial in a burn unit in the United States. J. Burn Care Res. 2014, 35, S159. [Google Scholar]
- Glik, J.; Kawecki, M.; Kitala, D.; Klama-Baryła, A.; Łabuś, W.; Grabowski, M.; Durdzińska, A.; Nowak, M.; Misiuga, M.; Kasperczyk, A. A new option for definitive burn wound closure-pair matching type of retrospective case-control study of hand burns in the hospitalised patients group in the Dr Stanislaw Sakiel Centre for Burn Treatment between 2009 and 2015. Int. Wound J. 2017, 14, 849–855. [Google Scholar] [CrossRef]
- Gürünlüoğlu, K.; Demircan, M.; Koç, A.; Koçbıyık, A.; Taşçi, A.; Durmuş, K.; Gürünlüoğlu, S.; Bağ, H.G.; Taşçı, A.; Koçbiyik, A. The effects of different burn dressings on length of telomere and expression of telomerase in children with thermal burns. J. Burn Care Res. 2019, 40, 302–311. [Google Scholar] [CrossRef]
- Highton, L.; Wallace, C.; Shah, M. Use of Suprathel® for partial thickness burns in children. Burns 2012, 39, 2–7. [Google Scholar] [CrossRef]
- Hundeshagen, G.; Collins, V.N.; Wurzer, P.; Sherman, W.; Voigt, C.D.; Cambiaso-Daniel, J.; Nunez-Lopez, O.; Sheaffer, J.; Herndon, D.N.; Finnerty, C.C.; et al. A prospective, randomized, controlled trial comparing the outpatient treatment of pediatric and adult partial-thickness burns with Suprathel or Mepilex Ag. J. Burn Care Res. 2017, 39, 261–267. [Google Scholar] [CrossRef]
- Iqbal, T.; Ali, U.; Iqbal, Z.; Fatima, Z.J.; Rehan, M.; Khan, M.S. Role of Suprathel in dermal burns in children. Emerg. Med. Investig. 2018, 6, 2–5. [Google Scholar] [CrossRef]
- Kukko, H.; Kosola, S.; Pyorala, S.; Vuola, J. Suprathel® in treatment of children’s scald injuries. Burns 2009, 35, S22. [Google Scholar] [CrossRef]
- Mądry, R.; Strużyna, J.; Stachura-Kułach, A.; Drozdz, Ł.; Bugaj, M. Effectiveness of Suprathel® application in partial thickness burns, frostbites and Lyell syndrome treatment. Pol. J. Surg. 2011, 83, 541–548. [Google Scholar] [CrossRef]
- Radu, C.; Gazyakan, E.; Germann, G.; Riedel, K.; Reichenberger, M.; Ryssel, H. Optimizing Suprathel®—Therapy by the use of Octenidine-Gel®. Burns 2011, 37, 294–298. [Google Scholar] [CrossRef]
- Rashaan, Z.M.; Krijnen, P.; Allema, J.H.; Vloemans, A.F.; Schipper, I.B.; Breederveld, R.S. Usability and effectiveness of Suprathel in partial thickness burns in children. Eur. J. Trauma Emerg. Surg. 2017, 43, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Schulz, A.; Perbix, W.; Shoham, Y.; Daali, S.; Charalampaki, C.; Fuchs, P.; Schiefer, J. Our initial learning curve in the enzymatic debridement of severely burned hands—Management and pit falls of initial treatments and our development of a post debridement wound treatment algorithm. Burns 2017, 43, 326–336. [Google Scholar] [CrossRef]
- Schriek, K.S.; Sinnig, M.M. 473 The use of caprolacton dressings in pediatric burns—A gold standard? J. Burn Care Res. 2018, 39, S209. [Google Scholar] [CrossRef]
- Schwarze, H.; Küntscher, M.; Uhlig, C.; Hierlemann, H.; Prantl, L.; Ottomann, C.; Hartmann, B. Suprathel, a new skin substitute, in the management of partial-thickness burn wounds. Ann. Plast. Surg. 2008, 60, 181–185. [Google Scholar] [CrossRef]
- Elmasry, M.; Steinvall, I.; Thorfinn, J.; Abbas, A.H.; Abdelrahman, I.; Adly, O.A.; Sjöberg, F. Treatment of children with scalds by xenografts. J. Burn Care Res. 2016, 37, e586–e591. [Google Scholar] [CrossRef]
- Hosseini, S.N.; Mousavinasab, S.N.; Fallahnezhat, M. Xenoderm dressing in the treatment of second degree burns. Burns 2007, 33, 776–781. [Google Scholar] [CrossRef]
- Karlsson, M.; Elmasry, M.; Steinvall, I.; Sjöberg, F.; Olofsson, P.; Thorfinn, J. Superiority of silver-foam over porcine xenograft dressings for treatment of scalds in children: A prospective randomised controlled trial. Burns 2019, 45, 1401–1409. [Google Scholar] [CrossRef] [PubMed]
- Hunt, T.K.; Conolly, W.B.; Aronson, S.B.; Goldstein, P. Anaerobic metabolism and wound healing: An hypothesis for the initiation and cessation of collagen synthesis in wounds. Am. J. Surg. 1978, 135, 328–332. [Google Scholar] [CrossRef]
- Wahl, P.; Bloch, W.; Mester, J. Moderne Betrachtungsweisen des Laktats: Laktat ein überschätztes und zugleich unter-schätztes Molekül. Schweiz. Z. Sportmed. Sporttraumatol. 2009, 57, 100–107. [Google Scholar]
- Philp, A.; Macdonald, A.L.; Watt, P.W. Lactate—A signal coordinating cell and systemic function. J. Exp. Biol. 2005, 208, 4561–4575. [Google Scholar] [CrossRef] [Green Version]
- Milovanova, T.N.; Bhopale, V.M.; Sorokina, E.M.; Moore, J.S.; Hunt, T.K.; Hauer-Jensen, M.; Velazquez, O.C.; Thom, S.R. Lactate Stimulates Vasculogenic Stem Cells via the Thioredoxin System and Engages an Autocrine Activation Loop Involving Hypoxia-Inducible Factor 1. Mol. Cell. Biol. 2008, 28, 6248–6261. [Google Scholar] [CrossRef] [Green Version]
- Cruz, R.S.D.O.; De Aguiar, R.A.; Turnes, T.; Penteado Dos Santos, R.; Fernandes Mendes De Oliveira, M.; Caputo, F. Intracellular shuttle: The lactate aerobic metabolism. Sci. World J. 2012, 2012. [Google Scholar] [CrossRef] [Green Version]
- Groussard, C.; Morel, I.; Chevanne, M.; Monnier, M.; Cillard, J.; Delamarche, A. Free radical scavenging and antioxidant effects of lactate ion: An in vitro study. J. Appl. Physiol. 2000, 89, 169–175. [Google Scholar] [CrossRef]
- Gürünlüoğlu, K.; Demircan, M.; Taşçı, A.; Üremiş, M.M.; Türköz, Y.; Bağ, H.G.; Ercan, B. The effects of two different burn dressings on serum oxidative stress indicators in children with partial burn. J. Burn Care Res. 2019, 40, 444–450. [Google Scholar] [CrossRef]
- Demircan, M.; Gürünlüoğlu, K.; Bayrakçı, E.; Taşçı, A. Effects of Suprathel®, Aquacel® Ag or auto-grafting on human telomerase reverse transcriptase expression in the healing skin in children with partial thickness burn. Ann. Burn. Fire Disasters 2017, 48, 49. [Google Scholar]
- Burkey, B.; Davis, W.; Glat, P.M. Porcine xenograft treatment of superficial partial-thickness burns in paediatric patients. J. Wound Care 2016, 25, 10–15. [Google Scholar] [CrossRef]
- Troy, J.; Karlnoski, R.; Downes, K.; Brown, K.S.; Cruse, C.W.; Smith, D.J.; Payne, W.G. The use of EZ Derm® in partial-thickness burns: An institutional review of 157 patients. Eplasty 2013, 13, 14. [Google Scholar]
- Fabia, R.; Groner, J.I. Advances in the care of children with burns. Adv. Pediatr. 2009, 56, 219–248. [Google Scholar] [CrossRef]
- Chiu, T.; Burd, A. “Xenograft” dressing in the treatment of burns. Clin. Dermatol. 2005, 23, 419–423. [Google Scholar] [CrossRef]
- Duteille, F.; Perrot, P. Management of 2nd-degree facial burns using the Versajet® hydrosurgery system and xenograft: A prospective evaluation of 20 cases. Burns 2012, 38, 724–729. [Google Scholar] [CrossRef]
- Klosová, H.; Klein, L.; Bláha, J. Analysis of a retrospective double-centre data-collection for the treatment of burns using biological cover xe-derma. Ann. Burn. Fire Disasters 2014, 27, 171–174. [Google Scholar]
- Keck, M.; Selig, H.; Lumenta, D.; Kamolz, L.; Mittlbock, M.; Frey, M. The use of Suprathel® in deep dermal burns: First results of a prospective study. Burns 2012, 38, 388–395. [Google Scholar] [CrossRef]
- Bukovčan, P.; Koller, J. Treatment of partial-thickness scalds by skin xenografts—A retrospective study of 109 cases in a three-year period. Acta Chir. Plast. 2010, 52, 7–12. [Google Scholar] [CrossRef]
- Diegidio, P.; Hermiz, S.J.; Ortiz-Pujols, S.; Jones, S.W.; Van Duin, D.; Weber, D.J.; Cairns, B.A.; Hultman, C.S. Even better than the real thing? Xenografting in pediatric patients with scald injury. Clin. Plast. Surg. 2017, 44, 651–656. [Google Scholar] [CrossRef]
- Healy, C.; Boorman, J. Comparison of E-Z Derm and Jelonet dressings for partial skin thickness burns. Burns 1989, 15, 52–54. [Google Scholar] [CrossRef]
- Priebe, C.; Friedman, R.; Noble, G.; Martucci, G.; Driessnack, M.; Soroff, H. Treatment of second-degree burns with porcine xenografts versus silver sulfadiazine cream: A study of pain and wound healing. J. Pediatr. Surg. 1992, 27, 390–391. [Google Scholar] [CrossRef]
- Rodriguez-Ferreyra, P. The use of xenograft to manage extensive but superficial burns. Burns 2007, 33, S91. [Google Scholar] [CrossRef]
- Burleson, R.; Eiseman, B. Nature of the bond between partial-thickness skin and wound granulations. Plast. Reconstr. Surg. 1973, 51, 353. [Google Scholar] [CrossRef]
- Rappaport, I.; Pepino, A.; Dietrick, W. Early use of xenografts as a biologic dressing in burn trauma. Am. J. Surg. 1970, 120, 144–148. [Google Scholar] [CrossRef]
- Zajicek, R.; Matouskova, E.; Broz, L.; Kubok, R.; Waldauf, P.; Königova, R. New biological temporary skin cover Xe-Derma® in the treatment of superficial scald burns in children. Burns 2011, 37, 333–337. [Google Scholar] [CrossRef]
- Esteban-Vives, R.; Young, M.T.; Ziembicki, J.; Corcos, A.; Gerlach, J.C. Effects of wound dressings on cultured primary keratinocytes. Burns 2016, 42, 81–90. [Google Scholar] [CrossRef]
- Hartmann, B.; Ekkernkamp, A.; Johnen, C.; Gerlach, J.C.; Belfekroun, C.; Küntscher, M.V. Sprayed cultured epithelial autografts for deep dermal burns of the face and neck. Ann. Plast. Surg. 2007, 58, 70–73. [Google Scholar] [CrossRef]
- Sander, F.; Haller, H.; Belfekroun, C.; Hartmann, B. Suprathel und gesprühte Keratinozyten—Eine retrospektive Qualitätssicherungsstudie. Ger. Med. Sci. 2019, 36–37. [Google Scholar] [CrossRef]
- Wood, F.; Martin, L.; Lewis, D.; Rawlins, J.; McWilliams, T.; Burrows, S.; Rea, S. A prospective randomised clinical pilot study to compare the effectiveness of Biobrane® synthetic wound dressing, with or without autologous cell suspension, to the local standard treatment regimen in paediatric scald injuries. Burns 2012, 38, 830–839. [Google Scholar] [CrossRef]
- Wood, F.; Kolybaba, M.; Allen, P. The use of cultured epithelial autograft in the treatment of major burn wounds: Eleven years of clinical experience. Burns 2006, 32, 538–544. [Google Scholar] [CrossRef]
- Tan, A.; Whybro, N.; Frew, Q.; Barnes, D.; Philp, B.; Dziewulski, P. The use of Recell® in a regional burn service. Ann. Burn. Fire Disasters 2015, 28, 1–2. [Google Scholar]
- Rapp, M.; Schappacher, R.; Liener, U. Zweizeitige Deckung von Spalthaut-Meek-Inseln nach 7–10 Tagen mit einer Polylactid-Membran (Suprathel). In Proceedings of the DAV 2020, Schladming, Austria, 15–18 January 2020. [Google Scholar] [CrossRef]
- Feng, X.S.; Pan, Y.G.; Tan, J.J.; Wu, Q.H.; Shen, R.; Ruan, S.B.; Chen, X.D.; Zhang, F.G.; Lin, Z.P.; Du, Y.L. Treatment of deep partial thickness burns by a single dressing of porcine acellular dermal matrix. Chin. J. Surg. 2006, 44, 467–470. [Google Scholar] [PubMed]
- Iwase, H.; Ekser, B.; Zhou, H.; Liu, H.; Satyananda, V.; Humar, R.; Humar, P.; Hara, H.; Long, C.; Bhama, J.K.; et al. Further evidence for sustained systemic inflammation in xenograft recipients (SIXR). Xenotransplantation 2015, 22, 399–405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demircan, M.; Gürünlüoğlu, K.; Bag, H.G.G.; Koçbıyık, A.; Gül, M.; Uremis, N.; Gul, S.; Gürünlüoğlu, S.; Türköz, Y.; Taşçı, A. Impaction of the polylactic membrane or hydrofiber with silver dressings on the Interleukin-6, Tumor necrosis factor-α, Transforming growth factor-3 levels in the blood and tissues of pediatric patients with burns. Turk. J. Trauma Emerg. Surg. 2021, 27, 122–131. [Google Scholar] [CrossRef]
- Wurzer, P.; Keil, H.; Branski, L.K.; Parvizi, D.; Clayton, R.P.; Finnerty, C.C.; Herndon, D.N.; Kamolz, L.P. The use of skin substitutes and burn care—A survey. J. Surg. Res. 2016, 201, 293–298. [Google Scholar] [CrossRef]
- Jin, R.; Greenwald, A.; Peterson, M.D.; Waddell, T.K. Human Monocytes Recognize Porcine Endothelium via the Interaction of Galectin 3 and α-GAL. J Immunol. 2006, 177, 1289–1295. [Google Scholar] [CrossRef] [Green Version]
- Schechter, I. Prolonged retention of glutaraldehyde-treated skin allografts and xenografts. Ann. Surg. 1975, 182, 699–704. [Google Scholar] [CrossRef]
- Cooke, A.; Oliver, R.F.; Edward, M. An in vitro cytotoxicity study of aldehyde-treated pig dermal collagen. Br. J. Exp. Pathol. 1983, 64, 172–176. [Google Scholar]
- El-Khatib, H.A.; Hammouda, A.; Al-Ghol, A.; Habib, B. Aldehyde-treated porcine skin versus biobrane as biosynthetic skin substitutes for excised burn wounds: Case series and review of the literature. Ann. Burn. Fire Disasters 2007, 20, 78–82. [Google Scholar]
- Yamamoto, T.; Iwase, H.; King, T.W.; Hara, H.; Cooper, D.K. Skin xenotransplantation: Historical review and clinical potential. Burns 2018, 44, 1738–1749. [Google Scholar] [CrossRef]
- Salisbury, R.E.; Wilmore, D.W.; Silverstein, P.; Pruitt, B.A. Biological dressings for skin graft donor sites. Arch. Surg. 1973, 106, 705–706. [Google Scholar] [CrossRef]
- Vanstraelen, P. Comparison of calcium sodium alginate (KALTOSTAT) and porcine xenograft (E-Z DERM) in the healing of split-thickness skin graft donor sites. Burns 1992, 18, 145–148. [Google Scholar] [CrossRef]
- Barone, A.A.L.; Mastroianni, M.; Farkash, E.A.; Mallard, C.; Albritton, A.; Torabi, R.; Leonard, D.A.; Kurtz, J.M.; Sachs, D.H.; Cetrulo, C.L., Jr. Genetically modified porcine split-thickness skin grafts as an alternative to allograft for provision of temporary wound coverage: Preliminary characterization. Burns 2015, 41, 565–574. [Google Scholar] [CrossRef]
- Leonard, D.; Mallard, C.; Albritton, A.; Torabi, R.; Mastroianni, M.; Sachs, D.; Kurtz, J.; Cetrulo, C. Skin grafts from genetically modified α-1,3-galactosyltransferase knockout miniature swine: A functional equivalent to allografts. Burns 2017, 43, 1717–1724. [Google Scholar] [CrossRef] [Green Version]
- Janich, E.J. Safety of Xenotransplantation: Development of Screening Methods and Testing for Porcine Viruses. Ph.D. Thesis, Freie Universität, Berlin, Germany, 2017. [Google Scholar]
- Hume, A.J.; Ames, J.; Rennick, L.J.; Duprex, W.P.; Marzi, A.; Tonkiss, J.; Mühlberger, E. Inactivation of RNA viruses by gamma irradiation: A study on mitigating factors. Viruses 2016, 8, 204. [Google Scholar] [CrossRef]
- Feng, X.; Shen, R.; Tan, J.; Chen, X.; Pan, Y.; Ruan, S.; Zhang, F.; Lin, Z.; Zeng, Y.; Wang, X.; et al. The study of inhibiting systematic inflammatory response syndrome by applying xenogenic (porcine) acellular dermal matrix on second-degree burns. Burns 2007, 33, 477–479. [Google Scholar] [CrossRef]
- Eriksson, A.; Burcharth, J.; Rosenberg, J. Animal derived products may conflict with religious patients’ beliefs. BMC Med. Ethics 2013, 14, 48. [Google Scholar] [CrossRef] [Green Version]
- Jenkins, E.D.; Yip, M.; Melman, L.; Frisella, M.M.; Matthews, B.D. Informed consent: Cultural and religious issues associated with the use of allogeneic and xenogeneic mesh products. J. Am. Coll. Surg. 2010, 210, 402–410. [Google Scholar] [CrossRef]
- Brady, S.C.; Snelling, C.F.T.; Chow, G. Comparison of donor site dressings. Ann. Plast. Surg. 1980, 5, 238–245. [Google Scholar] [CrossRef]
- Schwarze, H.; Küntscher, M.; Uhlig, C.; Hierlemann, H.; Prantl, L.; Noack, N.; Hartmann, B. Suprathel®, a new skin substitute, in the management of donor sites of split-thickness skin grafts: Results of a clinical study. Burns 2007, 33, 850–854. [Google Scholar] [CrossRef] [PubMed]
- Kaartinen, I.S.; Kuokkanen, O.H. Suprathel® causes less bleeding and scarring than Mepilex® Transfer in the treatment of donor sites of split-thickness skin grafts. J. Plast. Surg. Hand Surg. 2011, 45, 200–203. [Google Scholar] [CrossRef] [PubMed]
- Grigg, M.; Brown, J.T.C. Donor Site Dressings: How Much Do They Affect Pain? EJCB 2020, 1, 88. Available online: www.mendeley.com/reference-manager/reader/8ea85f41-059c-3096-ab92-ee76df2b04e4/1e556e1f-5932-1173-6f10-287641fb2542/ (accessed on 15 May 2020).
- Uhlig, C.; Rapp, M.; Hartmann, B.; Hierlemann, H.; Planck, H.; Dittel, K.-K. Suprathel®—An innovative, resorbable skin substitute for the treatment of burn victims. Burns 2007, 33, 221–229. [Google Scholar] [CrossRef]
- Markl, P.; Prantl, L.; Schreml, S.; Babilas, P.; Landthaler, M.; Schwarze, H. Management of split-thickness donor sites with synthetic wound dressings. Ann. Plast. Surg. 2010, 65, 490–496. [Google Scholar] [CrossRef]
- Griggs, C.; Goverman, J.; Bittner, E.A.; Levi, B. Sedation and Pain Management in Burn Patients. Clin. Plast. Surg. 2017, 44, 535–540. [Google Scholar] [CrossRef]
- Lamy, J.; Yassine, A.-H.; Gourari, A.; Forme, N.; Zakine, G. Place des substituts cutanés dans le traitement chirurgical des grands brûlés sur plus de 60% de la Surface corporelle. Revue de patients sur 11 ans dans le centre des brûlés adultes du CHRU de Tours. Ann. Chir. Plast. Esthét. 2015, 60, 131–139. [Google Scholar] [CrossRef]
- Shubitidze, D.K. Prospektive Multicenterstudie für Eine Neue Lokaltherapie des Ulcus Cruris Mit Einer Resorbierbaren Wundabdeckung (Suprathel®). Ph.D. Thesis, Eberhard Karls Universität, Tubingen, Germany, 2016. [Google Scholar]
- Uhlig, C.; Rapp, M.; Dittel, K.-K. Neue Strategien zur Behandlung thermisch geschädigter Hände unter Berücksichtigung des Epithelersatzes Suprathel®. Handchir. Mikrochir. Plast. Chir. 2007, 39, 314–319. [Google Scholar] [CrossRef]
- Kloeters, O.; Schierle, C.; Tandara, A.; Mustoe, T.A. The use of a semiocclusive dressing reduces epidermal inflammatory cytokine expression and mitigates dermal proliferation and inflammation in a rat incisional model. Wound Repair Regen. 2008, 16, 568–575. [Google Scholar] [CrossRef] [Green Version]
- Ogawa, R. Keloid and hypertrophic scars are the result of chronic inflammation in the reticular dermis. Int. J. Mol. Sci. 2017, 18, 606. [Google Scholar] [CrossRef] [Green Version]
- Ziegler, B.; Hundeshagen, G.; Cordts, T.; Kneser, U.; Hirche, C. State of the art in enzymatic debridement. Plast. Aesthet. Res. 2018, 5, 33. [Google Scholar] [CrossRef] [Green Version]
- Blome-Eberwein, S.; Pagella, P.; Boorse, D.; Amani, H. Results from Application of an Absorbable Synthetic Membrane to Superficial and Deep Second Degree Burn Wounds. In Proceedings of the 7th World Congress on Pediatric Burns, Boston, MA, USA, 29 August–1 September 2014; Available online: http://www.silon.com/wp-content/uploads/2014/09/ECPB2014-Results-from-Application-of-an-Absorbable-Synthetic-Membrane.pdf (accessed on 20 December 2020).
- Mu, X.X. Treatment of full-thickness burn by planned replacement using glutaraldehyde porcine skin with an autograft. Chin. J. Plast. Surg. Burn. 1989, 5, 193–196. [Google Scholar]
- Middelkoop, E.; Sheridan, R.L. Skin substitutes and ‘the next level’. In Total Burn Care, 5th ed.; Elsevier: Amsterdam, The Netherlands, 2018. [Google Scholar]
- Saffle, J.R. Closure of the Excised Burn Wound: Temporary Skin Substitutes. Clin. Plast. Surg. 2009, 36, 627–641. [Google Scholar] [CrossRef]
- Zuo, H.; Song, G.; Shi, W.; Jia, J.; Zhang, Y. Observation of viable alloskin vs. xenoskin grafted onto subcutaneous tissue wounds after tangential excision in massive burns. Burn. Trauma 2016, 4, 23. [Google Scholar] [CrossRef] [Green Version]
- Reumuth, G.; Schulz, T.; Reichelt, B.; Corterier, C.; Siemers, F. Die Temporäre Anwendung Eines Alloplastischen Hautersatzes—SUPRATHEL®—Bei Drittgradiger Verbrennung Fallbericht. In Proceedings of the DAV 2019, Schladming, Austria, 9–12 January 2019; Available online: https://www.egms.de/static/en/meetings/dav2019/19dav51.shtml (accessed on 4 December 2020).
- Haller, L.H.; Hafner, R.; Giretzlehner, M.; Thumfart, S.; Ottomann, C.; Hartmann, B.; Rapp, M.; Sander, F.; Lumenta, D.; Katzensteiner, K. Suprathel More Than a Dressing?! Ann. Burn. Fire Disasters 2015, 28, 173. [Google Scholar]
- Schneider, J.; Biedermann, T.; Widmer, D.; Montano, I.; Meuli, M.; Reichmann, E.; Schiest, C. Matriderm® versus Integra®: A comparative experimental study. Burns 2009, 35, 51–57. [Google Scholar] [CrossRef]
- Phillips, G.S.A.; Nizamoglu, M.; Wakure, A.; Barnes, D.; El-Muttardi, N.; Dziewulski, P. The use of dermal regeneration templates for primary burns surgery in a UK regional burns centre. Ann. Burn. Fire Disasters 2020, 33, 245–252. [Google Scholar]
- Baur, J.O.; Rahmanian-Schwarz, A.; Held, M.; Schiefer, J.; Daigeler, A.; Eisler, W. Evaluation of a cross-linked versus non-cross-linked collagen matrix in full-thickness skin defects. Burns 2021, 47, 150–156. [Google Scholar] [CrossRef]
- Greenwood, J.E.; Wagstaff, M.J. Changing Practice in the Surgical Management of Major Burns—Delayed Definitive Closure. J. Burn Care Res. 2018, 39 (Suppl. S1), S231–S232. [Google Scholar] [CrossRef]
- SkinTE For Providers: PolarityTE, Inc. (PTE): PolarityTE, Inc. (PTE) n.d. Available online: https://www.polarityte.com/products/skinte-providers (accessed on 13 May 2020).
- ClinicalTrials.gov. Study with an Autologous Dermo-epidermal Skin Substitute for the Treatment of Full-Thickness Skin Defects in Adults and Children—Full Text View—ClinicalTrials.gov n.d. Available online: https://clinicaltrials.gov/ct2/show/NCT03394612?term=denovoSkin&draw=2&rank=2 (accessed on 13 May 2020).
- Martinson, M.; Martinson, N. A comparative analysis of skin substitutes used in the management of diabetic foot ulcers. J. Wound Care 2016, 25, S8–S17. [Google Scholar] [CrossRef]
- Boyce, S.T.; Simpson, P.S.; Rieman, M.T.; Warner, P.M.; Yakuboff, K.P.; Bailey, J.K.; Nelson, J.K.; Fowler, L.A.; Kagan, R.J. Randomized, Paired-Site Comparison of Autologous Engineered Skin Substitutes and Split-Thickness Skin Graft for Closure of Extensive, Full-Thickness Burns. J. Burn Care Res. 2017, 38, 61–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roy, M.; King, T.W. Epidermal growth factor regulates NIKS keratinocyte proliferation through Notch signaling. J. Surg. Res. 2013, 185, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Centanni, J.M.; Straseski, J.A.; Wicks, A.; Hank, J.A.; Rasmussen, C.A.; Lokuta, M.A.; Schurr, M.J.; Foster, K.N.; Faucher, L.D.; Caruso, D.M.; et al. Stratagraft skin substitute is well-tolerated and is not acutely immunogenic in patients with traumatic wounds: Results from a prospective, randomized, controlled dose escalation trial. Ann. Surg. 2011, 253, 672–683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rapp, M.; Al-Shukur, F.-F.; Liener, U.C. Der Einsatz des Alloplastischen Epithelersatzes Suprathel® bei Großflächigen Gemischt 2.-Gradigen Verbrennungen Über 25% KOF—Das Stuttgarter Konzept. (DAV 2010). 2010. Available online: https://www.egms.de/static/en/meetings/dav2010/10dav18.shtml (accessed on 27 November 2020).
- Tsuchiya, S.; Ohmori, M.; Hara, K.; Fujio, M.; Ikeno, M.; Hibi, H.; Ueda, M. An Experimental Study on Guided Bone Regeneration Using a Polylactide-co-glycolide Membrane–Immobilized Conditioned Medium. Int. J. Oral Maxillofac. Implant. 2015, 30, 1175–1186. [Google Scholar] [CrossRef] [Green Version]
- Ronga, M.; Cherubino, M.; Corona, K.; Fagetti, A.; Bertani, B.; Valdatta, L.; Mora, R.; Cherubino, P. Induced membrane technique for the treatment of severe acute tibial bone loss: Preliminary experience at medium-term follow-up. Int. Orthop. 2019, 43, 209–215. [Google Scholar] [CrossRef]
- Lindford, A.J.; Kaartinen, I.S.; Virolainen, S.; Vuola, J. Comparison of Suprathel® and allograft skin in the treatment of a severe case of toxic epidermal necrolysis. Burns 2011, 37, e67–e72. [Google Scholar] [CrossRef]
- Morris, C.; Emsley, P.; Meuleneire, F.; White, R.; Marland, E. Use of wound dressings with soft silicone adhesive technology. Paediatr. Nurs. 2009, 21, 38–43. [Google Scholar] [CrossRef] [Green Version]
- Hobby, J.A.; Levick, P.L. Clinical evaluation of porcine xenograft dressings. Burns 1978, 4, 188–192. [Google Scholar] [CrossRef]
- Sun, T.; Han, Y.; Chai, J.; Yang, H. Transplantation of microskin autografts with overlaid selectively decellularized split-thickness porcine skin in the repair of deep burn wounds. J. Burn Care Res. 2011, 32, e67–e73. [Google Scholar] [CrossRef]
- Haller, H.; Held-Föhn, E. 654 Investigation of germ patency of a polylactic acid-based membrane for the treatment of burns. J. Burn Care Res. 2020, 41, S173. [Google Scholar] [CrossRef]
- Deitch, E.A.; Wheelahan, T.M.; Rose, M.P.; Clothier, J.; Cotter, J. Hypertrophic burn scars. J. Trauma Inj. Infect. Crit. Care 1983, 23, 895–898. [Google Scholar] [CrossRef]
- Kraemer, B.; Wallwiener, M.; Brochhausen, C.; Planck, C.; Hierlemann, H.; Isaacson, K.B.; Rajab, T.K.; Wallwiener, C. A Pilot Study of Laparoscopic Adhesion Prophylaxis after Myomectomy with a Copolymer Designed for Endoscopic Application. J. Minim. Invasive Gynecol. 2010, 17, 222–227. [Google Scholar] [CrossRef]
- Al-Saidi, A.A.M. Myokardiale Adhäsionsprophylaxe am Schweinemodell Mittels Antiadhäsiver Bioresorbierbarer Polymerfolien. Ph.D. Thesis, Eberhard Karls Universität zu Tübingen, Tuebingen, Germany, 2018. [Google Scholar]


{kind=link}
| Healing Time | Infected % | Grafted % | Dressing Changes | |
|---|---|---|---|---|
| Mean ST | 13.59 | 3.83 | 2.50 | 4.38 |
| Mean PX | 7.03 | 7.04 | 8.36 | 4.79 |
| Stdev ST | 1.86 | 6.44 | 4.05 | 1.83 |
| Stdev PX | 2.09 | 15.62 | 13.14 | 4.28 |
| Sample size ST | 371 | 625 | 681 | 398 |
| Sample size PX | 143 | 1124 | 1136 | 286 |
| Standardized Effectsize at 95% Confidence Intervall | 0.19 | 0.2 | 0.52 | 0.13 |
| Name of the First Study Author | Number of Patients | Study Design | Age | TBSA | Inclusion | Healing Time Days |
|---|---|---|---|---|---|---|
| Blome Eberwein [4] | 229 | Retro | P (Pediatric): 138, a (adults): 91 | Ø 8.6 1–60.5 | Superficial and deep second degree | Mean 13.7 d (days) p: 11.9 d A: 14.7 d |
| Everett [5] | 17 | Retro | P, Ø 33 m (months) | Ø 5% | Superficial and partial thickness | Mean 9.4 (5–24) d |
| Fischer [6] | 1 | Case report | A, 81 a | 51% | Partial thickness | 14 d |
| Glat [7] | 12 | Prospective | Ø 3.6 y (years) | Ø 5.5% | Superficial and mixed | Mean 8.4 d |
| Glik [8] | 24 | Retrospective unblinded pair control | Ø 48 y (21–86 y) | Ø 23.8 | Burns of both hands to minimize differences | From Figure 1: complete healing d 20 |
| Gürünlüoglu [9] | 20 | Prospective randomized | 4.9 ± 3.8 y | Ø 31.95 ± 4.43% | Acute burns, 1–60 y, 20–50% including deep burns 5–10% | Median 13.5 d (range 9–21 d) Mean 14.25 ±3.46 d |
| Highton [10] | 33 | Prospective | P: Ø 29 m (5 m–11 y) | Ø 4 (1–13)% | Superficial partial n = 24 mid-dermal: n = 19 deep n = 10, >21 d and infection | Median 16 (range 9–38) d; Mean 19.5 ± 8.4 d |
| Hundeshagen [11] | 30 | Prospective randomized | A: Ø 24.0 ± 23.0 | Ø 5.5 ± 4.6% | Partial thickness, FT excl. | Median 12.0 d, |
| Iqbal [12] | 65 | Prospective | Ø 4.9 y (4 m–11 y) | Ø 23.6% (8–45) | Superficial dermal 16, mid-dermal 34, deep-dermal 15 | Mean 15 (10–35) d |
| Kukko [13] | 8 | Retrospective | Ø 18 mo, range 10–39 | Ø 7.6 Stdev. missing | Scald injuries | All burns healed by the end of the third week. |
| Madry [14] | 15 | Retrospective | 1 p, 14 a | Not defined | partial thickness within 96 h after injury | Application: (a) ≤24 hs; (b) 24–48 h; (c) >48 h |
| Radu [15] | 30 | Prospective randomized | Median 42 y, (range 18–80 years) | Ø 18% (range 6–36) | Superficial partial thickness burn >3% | Not defined |
| Rashaan [16] | 21 | Prospective observational | Median 2.4 y (range 5 m–14 y) | 4.0% (range 1–18) | All consecutive partial thickness burns < 48 h after injury and age < 18 years SPTB: 12 DPTB: 9 | Median 13 (range 7–29); without bacterial contamination: 13 (7–18); with bacterial contamination 15 (9–29) Mean: 15.5 ± 6.36 d |
| Schiefer [17] | 24 | Prospective randomized | Ø 39.8 ± 18 y | 0.5 ± 3.0% | All patients with superficial partial thickness burn of the hands | All patients after 7 to 10 days healed completely |
| Schriek [18] | 149 (last year) | Retrospective | Pediatric | Not defined | All partial thickness burns | After 10–12 days, 7–9% grafted |
| Schwarze [19] | 30 | Prospective, randomized bicentric | a | 1.5% | 0 |
| The Name of the First Study Author | Number of Patients | Study Design | Age | TBSA | Inclusion | Healing Time |
|---|---|---|---|---|---|---|
| Bukovcan [38] | 109 | Retrospective | Ø 7.6 ± 15.3 | Ø 13 ± 8.2% | Superficial and partial thickness burns | Ø 15.1 d ± 11.6 total |
| Burkey [31] | 164 | Retrospective | Pediatric | Ø 5.8 ± 4.4% | Superficial partial thickness burns | Not described |
| Chiu [34] | 2 | Case reports | Ø 14 | Not described | Partial thickness burns of the face, mesh graft pattern | Healed after 10 days |
| Diegidio [39] | 534 | Retrospective | Ø 3.41 | Ø 8.41% | Scalds from ABA and own registry | Not described |
| Duteille [35] | 20 | Prospective | Ø 16.45% range | Ø 27.75% | Intermediary 2nd-degree facial burns | Initial healing time after excision: Ø 13.4 d, 3 grafted |
| Elmasry [20] | 67 | Retrospective | Median: 1 y, IQR 1–2 | Median 6.2IQR 4–11 | Scalds treated with xenograft (deep and FT) | Not defined |
| Healy [40] | 16 | Prospective randomized | Ø 2.6 y ± 7.0 | Ø 1.8 ± 0.8% | Partial- thickness burns < 10% BSA | 12.9 days in spontaneously healed patients (=47%) |
| Karlsson [22] | 58 | Prospective randomized | Ø 21 m (11–59) | Median 5% (3–22) | Partial thickness, <72 h after injury, 6 m–6 y | Median 97% healing 15 d (range 9–29) Ø 17 Median 100% healing: 20.5 range 11–42 |
| Klosova [36] | 91 | Retrospective | 2.5 | 1–20% | Partial thickness and burn center admission | 12–14 d |
| Klosova | 10 | Retrospective | 42 | 1–20% | Partial thickness and burn center admission | |
| Priebe [41] | 17 | Prospective | 15 < 28 m | Not defined | Areas with comparable aspects of 2nd degree | 13 of 17 healed in 15 days, |
| Rodriguez Ferreyra [42] | 20 | Not defined | Ø 19.2 y | Ø 14.8, no std | Not described | No healing time described. |
| Troy [32] | 133 | Retrospective | Ø 17.7, range | Ø 16 ± 37.7% | partial thickness burns, no hands, no pediatric pat | Not described |
| ST® | Xenograft | ||||
|---|---|---|---|---|---|
| First Author | ST® | Comment | First Author | Xenografts Change or Diss. | Comment |
| Blome Eberwein [4] | No change and no autografts. | In 5.2% failure or progression to full thickness, residual defects treated conservatively | Burkey [31] | 11% of 164 not anticipated autografting + prolonged topical wound care in 6 pat. (3.7%) not anticipated and 22 (14%) anticipated | 14.7% (in a total of not anticipated autografting or prolonged wound care) |
| Everett [5] | No change | Burleson [43] cited by Chiu [34] | Change every two days | Partial-thickness porcine split skin | |
| Fischer [6] | No change | Duteille [35] | EZ derm in place after surgery for three days, followed by grafting or topical wound care | Grafting in 3 patients, | |
| Gürünüloglu [9] | No change | Elmasry [20] | 20% needed an operation | No use in hands | |
| Klosova [36] | 19% (81% no signs of dissolution) | XE derma | |||
| Hundeshagen [11] | No change | Priebe [41] | EZ Derm replaced every third day | ||
| Madry [14] | No change | One dressing removal necessary when ST applied at 24–48 h; 2 removals necessary, applied >48 h after injury (reasons nor specified). | Rappaport [44] cited by Chiu [34] | Daily change of xenograft | Deep Frozen pigskin |
| Rashaan [16] | No change, early detachment in 43% treated conservatively | 33% contamination before ST®, detachment is linked to the method of debridement and topical wound care when detached. | Troy [32] | 6.8% with premature graft separation, 15% lost for follow-up | After separation, local wound care |
| Schiefer [17] | No change | ||||
| Schwarze [19] | No change | ||||
| ST® | PX | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Study | n= | % Grafted | n= | Type of Burn | Study | n= | % Grafted | Number of Grafted | Type of Burn |
| Blome Eberwein [4] | 229 | 0% | 0 | 2nd degree burns superficial and partial | Bukovcan [38] | 109 | 3.7% | 4 | superficial partial scald burns |
| Everett [5] | 17 | 0% | 0 | Partial thickness within 6 h | Burkey [31] | 167 | 5.5% unexpected | 3 + 21 | Superficial partial-thickness inclusion |
| Fischer [6] | 1 | 0% | 0 | Partial thickness | Duteille [35] | 20 | 15% | 3 | Intermediate face burns |
| Gürünlüoglu [9] | 20 | 0% | 0 | Superficial and deep partial thickness burns | Elmasry [20] | 67 | 30% | 20 | Only superficial partial-thickness burns |
| Hundeshagen [11] | 30 | 6.6% | 1 | Partial thickness burns | Healy [40] | 32 | 7 out of 16 EZ Derm 44% | 7 | Partial, no hands or faces |
| Iqbal [12] | 65 | 0% | 0 | Partial-thickness burns | Karlsson [22] | 29 | 13% | 6 | No palms, soles, or faces |
| Madry [14] | 15 | 26% | 2 | Children, Flame and scald burns | Klosova [36] | 91 children | 30% | 27 | Partial thickness burns and full thickness |
| Rashaan [16] | 21 | 14% | 3 | Superficial. and deep partial, 7% of all patients colonization before ST® | Klosova [36] | 10 adults | 90% | 9 | Partial thickness burns and full thickness |
| Schulz [17] | 24 | 0% | 0 | Partial thickness | Priebe [41] | 15 | 13% | 2 | Scald burns, children |
| Schriek and Sinnig [18] | 149 | 9% | 11 last year of table | Superficial and partial deep burns | Rodriguez Ferreyra [42] | 20 | 0% | 0 | superficial |
| Schwarze [19] | 30 | 0% | Superficial or mid dermal burns | Troy [32] | 157 | 8.6% | 6.8 + 4.5 + 2.2 Partial, no hands, no faces | ||
| ST | Xenograft | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| First Author | N= | Infections | Infect. % | Healing Time | First Author | N= | Infections | Infect. % | Healing Time |
| Blome Eberwein [4] | 138 p 91 a | 0 8 | 0 8.8% | 13.9 14.70 | Bukovcan [38] | 109 p | 4 | 4% | 15.10 |
| Everett [5] | 17 p | 0 | 0 | 9.40 | Burkey [31] | 167 p | 4 | 2% | insuff. Data |
| Glat [7] | 12 p | 0 | 0 | 8.40 | Diegidio [39] | 534 p | 3 | 0.01% | Insuff. Data |
| Hundeshagen [11] | 31 a | 1 | 6.45% | Duteille [35] | 20 a | 3 | 15% | insuff. Data | |
| Iqbal [12] | 65 p | 13 | 20% | 15.00 | Elmasry [20] | 20 p | 7 | 35% | insuff. Data |
| Rashaan [16] | 21 p | 1 | 4.76% | 15.56 | Healy [40] | 16 a | 7 | 43% | insuff. Data |
| Schwarze [19] | 30 a | 0 | 0 | 10.20 | Karlsson [22] | 58 p | 9 | 16% | 17.00 |
| Klosova [36] | 101 p + a | 5 | 5% | Nd | |||||
| Priebe [41] | 15 p | Nd (Not defined) | Nd | ||||||
| Rodriguez Ferreyra [42] | 20 p + a | 0 | 0% | insuff. Data | |||||
| Troy [32] | 15 a | 2 | 13% | insuff. Data | |||||
| Average per study | 3.83% | ±6.34 | Average per studies | 7.039 | 15.62 | ||||
| ST Studies, First Author | Outer Dc Every Day | Approx. Healing Time | Total Number of DC | PX Studies, First Author | Outer Dc Every Day | Approx. Healing Time | Total Number of DC |
|---|---|---|---|---|---|---|---|
| Blome Eberwein [4] | 1–4 (2.5) | 14.2 | 5.68 | Burkey [31] | Average DC 1.6 | Healing time not described | 1.6 |
| Everett [5] | 5–7 (6) | 9.5 | 1.59 | Bukovcan [38] | 2 | 15.1 | 7.6 |
| Hundeshagen [11] | 3–5 (4) | 12 | 3 | Elmasry [20] * | 1 | 12.2 | 12 |
| Iqbal [12] | 4–5 (4.5) | 15 | 3.33 | Duteille [35] | 3 days then moistened gauze | 3 * | * excluded |
| Rashaan [16] | 3 | 15 | 5 | Karlsson [22] | 3 regularly, up to three times a week, Number of DC: 5 (−9), time for DC 20 min (10–50) | Time to 95% healing 15 days | 5 |
| Priebe [41] | 3 | 15 | 5 | ||||
| The average number of dressing changes during Healing time and | 13.61 | 3.43 ± 1.46 Median 3.165 Range 4.09 | 14.33 | 7.4 ± 2.86 Median 5 Range 10.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haller, H.L.; Blome-Eberwein, S.E.; Branski, L.K.; Carson, J.S.; Crombie, R.E.; Hickerson, W.L.; Kamolz, L.P.; King, B.T.; Nischwitz, S.P.; Popp, D.; et al. Porcine Xenograft and Epidermal Fully Synthetic Skin Substitutes in the Treatment of Partial-Thickness Burns: A Literature Review. Medicina 2021, 57, 432. https://doi.org/10.3390/medicina57050432
Haller HL, Blome-Eberwein SE, Branski LK, Carson JS, Crombie RE, Hickerson WL, Kamolz LP, King BT, Nischwitz SP, Popp D, et al. Porcine Xenograft and Epidermal Fully Synthetic Skin Substitutes in the Treatment of Partial-Thickness Burns: A Literature Review. Medicina. 2021; 57(5):432. https://doi.org/10.3390/medicina57050432
Chicago/Turabian StyleHaller, Herbert L., Sigrid E. Blome-Eberwein, Ludwik K. Branski, Joshua S. Carson, Roselle E. Crombie, William L. Hickerson, Lars Peter Kamolz, Booker T. King, Sebastian P. Nischwitz, Daniel Popp, and et al. 2021. "Porcine Xenograft and Epidermal Fully Synthetic Skin Substitutes in the Treatment of Partial-Thickness Burns: A Literature Review" Medicina 57, no. 5: 432. https://doi.org/10.3390/medicina57050432