1. Introduction
Nucleos(t)ide analog (NA) treatment is recommended for all patients with hepatitis B virus (HBV)-induced cirrhosis with detectable HBV-DNA [
1,
2]. Importantly, long-term NA treatment achieves viral suppression in the vast majority patients [
3,
4], while HBsAg loss [
5] as a biomarker of functional cure is rarely achieved.
Studies have demonstrated beneficial effects of NA therapy in patients with cirrhosis/advanced chronic liver disease (ACLD) such as liver fibrosis regression [
6], hepatocellular carcinoma (HCC) prevention [
7] and protection from liver-related events, i.e., hepatic decompensation, and mortality [
8]. However, the impact of NA therapy on clinically significant portal hypertension (CSPH) and disease dynamics upon suppression remain less well defined. In a small uncontrolled trial involving 19 HBV patients with cirrhosis and CSPH, i.e., a hepatic venous pressure gradient (HVPG) ≥10 mmHg, one year of lamivudine (3TC) therapy induced a decrease in HVPG in all but one patient, who had experienced viral breakthrough [
9]. In another observational study investigating the effects of different NA (including 3TC, adefovir and tenofovir disoproxilfumarate (TDF)), patients without varices at baseline rarely developed varices during follow-up, and patients who had already developed small varices prior to NA therapy showed regression in a vast majority of cases (67%) [
10]. Importantly, the worsening of CSPH, i.e., growth/progression of varices almost exclusively occurred in the context of HCC development in this study, and the risk-modifying effects of HCC diagnosis on the progression of portal hypertension in HBV-infection warrant further investigation.
In contrast to HBV, the evolution of CSPH after antiviral therapy has been extensively investigated in hepatitis C (HCV) following antiviral therapy [
11,
12]. Furthermore, NITs have been developed for ruling-in/ruling-out CSPH after antiviral therapy in HCV [
13,
14], and the use of liver stiffness measurement (LSM) via vibration-controlled transient elastography (VCTE) and platelet count (PLT) for risk stratification in patients who achieved an HCV-cure is now recommended in clinical practice [
15].
Despite the large body of evidence for beneficial effects of NA-induced HBV suppression, ACLD-specific information remains scarce. Moreover, no study has investigated the correlation between HVPG and NITs in virally suppressed patients or their use for re-stratification of risk in HBV-induced ACLD patients who are known to have had CSPH pre therapy. Thus, we aimed to investigate (i) the correlation between NITs and HVPG and (ii) the prognostic value of NITs in HBV patients with pre-treatment CSPH achieving virologic suppression during long-term NA therapy.
2. Materials and Methods
In this retrospective analysis, we included patients with HBV-induced advanced chronic liver disease (ACLD) who (i) were diagnosed with chronic HBV-infection at our center between 2007 and 2020, (ii) were under long-term (>1 year) stable NA therapy at the time of study inclusion (i.e., on-treatment LSM), and (iii) had pre-treatment CSPH as evident from varices, a history of variceal bleeding, collaterals on cross-sectional imaging, ascites, and/or pre-treatment HVPG ≥10 mmHg and (iv) underwent an on-treatment follow-up LSM examination with our without HVPG measurement.
Patients who had a history of (i) hepatocellular carcinoma (HCC), (ii) transjugular intrahepatic portosystemic shunt (TIPS) or (iii) liver transplantation were excluded.
Information on events indicating (further) hepatic decompensation, HCC, liver transplantation, or death occurring after study inclusion were recorded.
HVPG-measurements were conducted following a standardized operating procedure described elsewhere [
16]. Laboratory tests were performed at the ISO-certified Department of Laboratory Medicine of the Medical University of Vienna. LSM were conducted using the FibroScan
® (Echosens, Paris, France) system.
A history of variceal bleeding or past/current ascites/hepatic encephalopathy defined dACLD.
Clinical events during follow-up (FU) that were considered as hepatic decompensation in compensated patients comprised variceal bleeding, development of overt hepatic encephalopathy (HE), development of ascites and liver-related death. Further decompensation in patients who had already developed decompensation at baseline was defined as variceal bleeding, requirement of paracentesis, grade 3/4 HE or liver-related death. The primary outcome of this study was the incidence of first/further decompensation in the overall patient cohort.
Statistical analysis was conducted using R 4.0.2 (R Core Team, R Foundation for Statistical Computing, Vienna, Austria) and GraphPad Prism 8 (GraphPad Software, La Jolla, CA, USA). Categorial variables are presented as number and percentages of patients with the respective characteristic. Continuous variables are presented as median (25th; 75th percentile). Group comparisons were conducted by Fisher’s exact test or Wilcoxon rank-sum test as applicable. Correlations were investigated by calculating Spearman’s ρ.
Patients entered our time-to-event analysis models at the time of on-treatment LSM and were followed until the time of (further) decompensation, HCC development, liver transplantation or death. The area under the receiver operating characteristic curve (AUROC) for decompensation within the first three years of follow-up was analyzed for all investigated NITs using the r package timeROC [
17], taking into account competing risks, i.e., HCC development, liver transplantation and non-liver-related death; the optimal LSM cut-off for prognostication was derived from Youden’s index. Cumulative incidences for (further) decompensation were calculated and compared between groups using Gray’s test, and prognostic models were developed by applying competing risk regression as proposed by Fine and Gray [
18]. In all models, HCC development, liver transplantation and non-liver-related death were considered as competing risks. Univariate models incorporated variables that differed significantly between patients who developed decompensation during FU versus those who did not. Significant variables were carried on to the multivariate analyses, and the final model was restricted to two variables owing to the low incidence of events in this cohort. LSM as the NIT with the highest AUROC was adjusted separately for all other variables, resulting in three models (A–C). Variable selection was evaluated by stepwise regression analysis with backward elimination incorporating all variables that were carried on from univariate analysis, showing that model (A) had the lowest prediction error as estimated by Akaike information criterion (AIC). A two-sided
p-value < 0.05 was considered statistically significant.
This study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (IRB) of the Medical University of Vienna (No. 1515/2020, date of approval: 30 June 2020). No written informed consent was required for this retrospective analysis.
3. Results
3.1. Patient/Treatment Characteristics
Forty-two patients with HBV-induced pre-treatment CPSH were included. Detailed information on patient/treatment characteristics is provided in the
Supplementary Materials (Table S1). As per inclusion criteria, on-treatment LSM was available in all patients, whereas HVPG measurements were conducted in
n = 17 (40.5%) patients.
The median time between NA-therapy initiation and follow-up characterization was 2.5 (1.2; 4.9) years. All patients were virally suppressed by NA therapy with no viral breakthroughs.
Twelve (28.6%) patients had a history of hepatic decompensation. Metabolic cofactors were common: alcohol consumption (above 30 g/d for men and 20 g/d for women) and diabetes mellitus were present in 21.4% and 28.6% of patients, respectively.
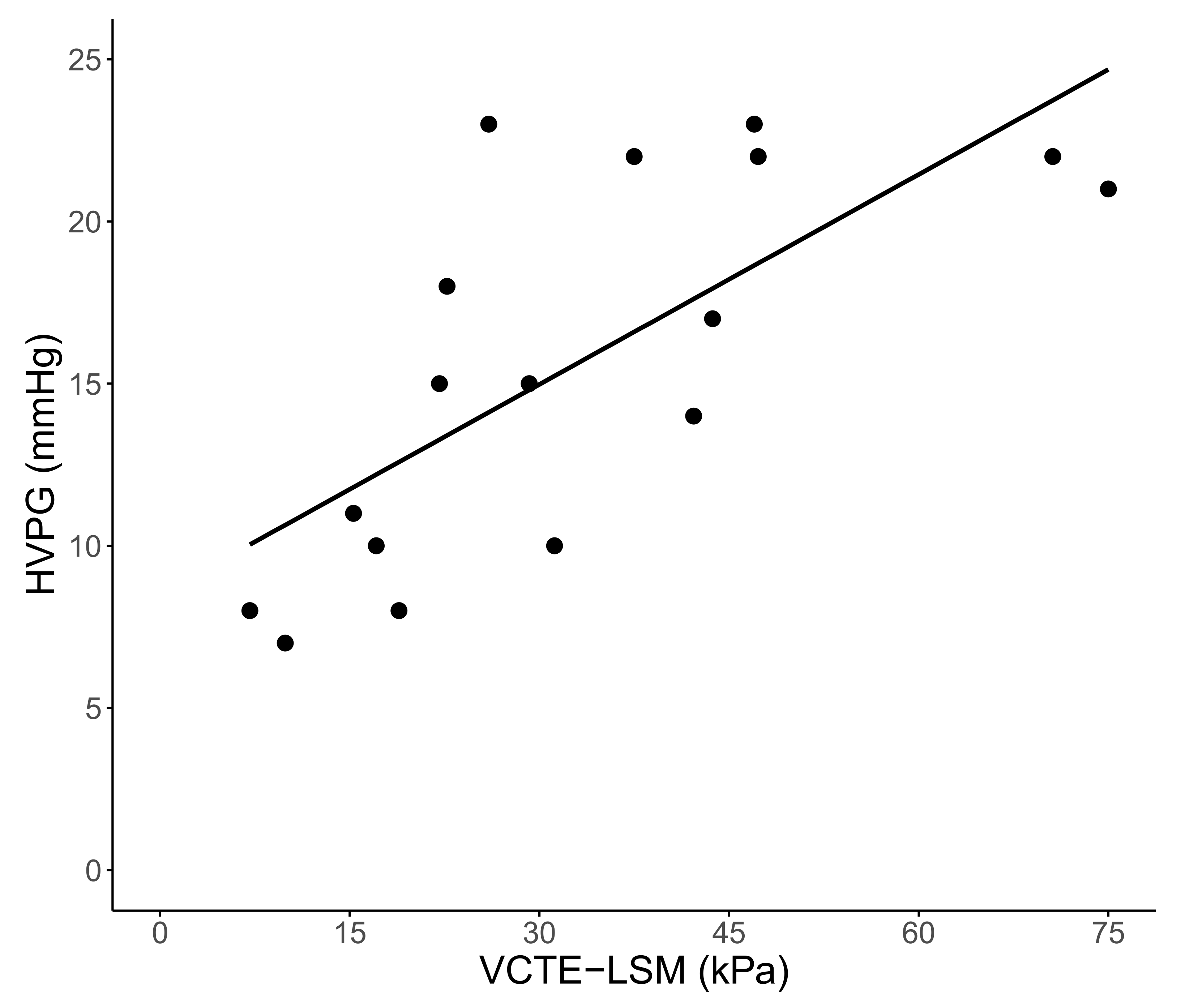
3.2. Correlation of HVPG with VCTE-LSM and Biomarkers of Disease Severity
LSM and HVPG correlated strongly (ρ: 0.725,
p < 0.001) in the
n = 17 patients who also underwent HVPG measurement, as shown in
Figure 1. In contrast, HVPG did not correlate with PLT (ρ: −0.117,
p = 0.655), nor with MELD (ρ: 0.048,
p = 0.856). In the overall cohort, correlations of moderate strength were found between LSM and MELD (ρ: 0.459,
p = 0.002), and LSM and PLT (ρ: −0.474,
p = 0.001).
3.3. Clinical FU
Patients were followed for a median of 2.1 (0.6; 5.3) years. Twelve (28.6%) patients developed one or more events of (further) decompensation: Development/worsening of ascites was seen in eight, development/worsening of HE in seven, and variceal (re-)bleeding in two patients. Notably, decompensation was preceded by an HBV-DNA flare (without ALT-elevation) in one patient, while no other HBV-DNA-/ALT-flares associated with decompensation were observed in our cohort during follow-up. HCC was diagnosed in 6 (14.3%) patients. Four (9.5%) patients underwent liver transplantation. Finally, nine (21.4%) and four (9.5%) patients died of liver-related and non-liver-related causes, respectively.
3.4. Comparison of Characteristics between Patients with or without (Further) Decompensation during FU
Patients who showed (further) decompensation during FU were more likely to have a history of previous decompensation, most importantly ascites (58.3% versus 13.3% of patients without decompensation during FU,
p = 0.008), as shown in
Table 1. Accordingly, they had more advanced disease, i.e., higher MELD (11 (10; 12) versus 8 (7; 10) points,
p = 0.002) and lower levels of serum albumin (34.6 (29.8; 36.3) versus 39.8 (37.5; 43.7) g/L,
p = 0.001). Regarding portal hypertension, HVPG (available in
n = 17) was higher (22 (21; 22) versus 12 (9; 16) mmHg,
p = 0.023) in patients with decompensation during FU. Similarly, LSM was considerably higher in the latter group of patients (47.7 (31.7; 75.0) versus 16.3 (10.0; 24.2) kPa,
p < 0.001) who also had lower PLT levels (63 (48; 119) versus 146 (91; 195) G/L,
p = 0.010). The metabolic profile (BMI, prevalence of diabetes and alcohol intake) was similar between the two groups.
Notably, patients with decompensation during FU were characterized significantly earlier than patients who remained compensated during FU (time from NA initiation to LSM/HVPG-measurement: 1.1 (1.1; 1.7) versus 4.3 (2.2; 5.3) years, p = 0.002).
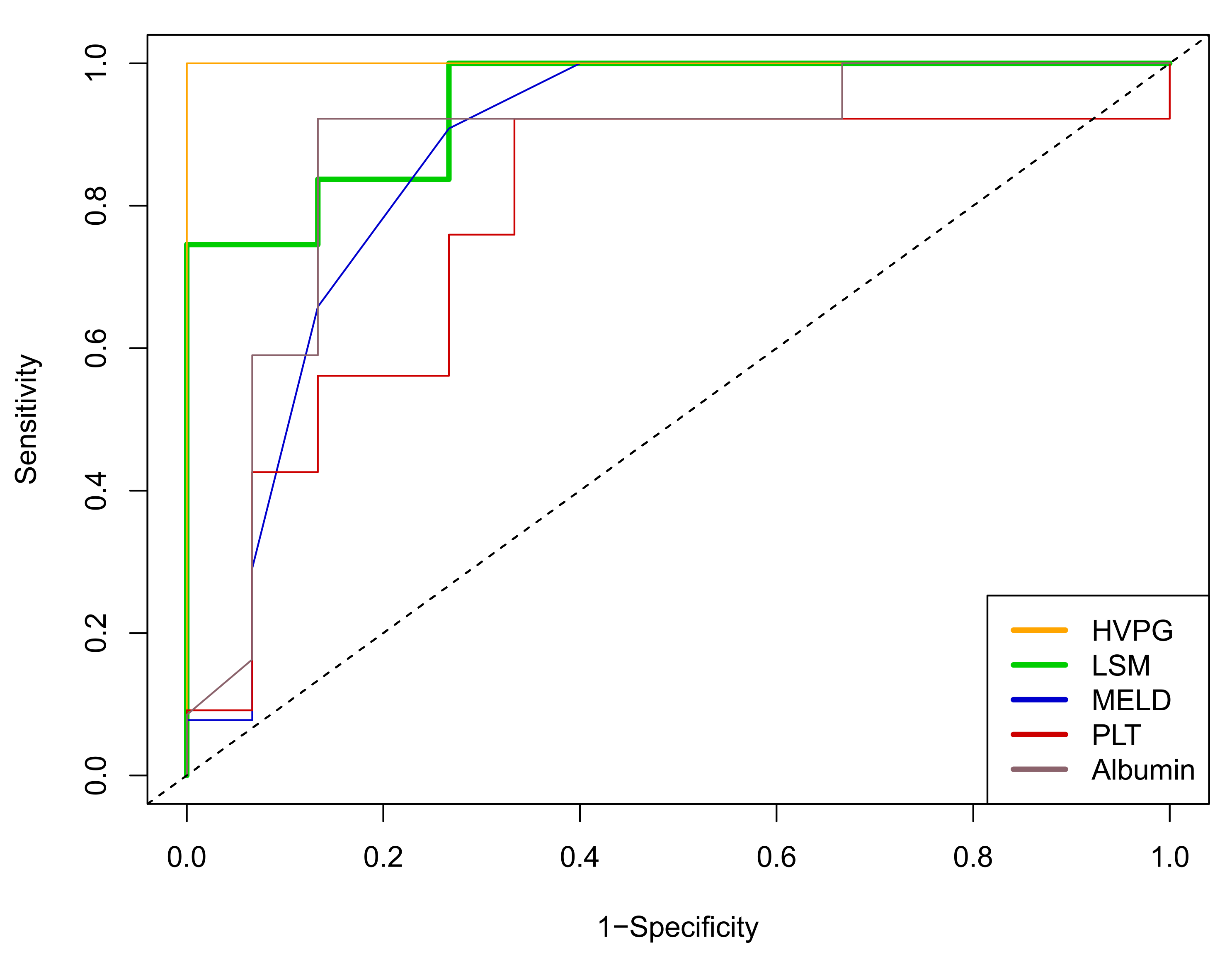
3.5. Prognostic Value of Patient Characteristics for (Further) Decompensation during FU
In the cohort of patients who underwent HVPG measurements (
n = 17), HVPG values had an area under the receiver operated characteristics curve (AUROC) of 1.000 (95% CI: 1.000–1.000) for the prediction of (further) decompensation during follow-up. In the overall cohort, LSM, MELD, and albumin levels showed robust prognostic performances (AUROC for all: >0.850), while PLT was less predictive, as shown in
Figure 2.
In univariate competing risk regression models considering (further) decompensation as the outcome of interest and HCC development, liver transplantation and non-liver-related mortality as competing risks (liver transplantation was always preceded by further decompensation or HCC development), LSM values, (a history of or current) ascites and MELD score (all
p < 0.001) as well as serum albumin levels (
p = 0.002) had strong prognostic implications, while PLT count was of no prognostic value in this context (
p = 0.140), as shown in
Table S2.
Owing to the low (
n = 12) number of events, multivariate models were restricted to two variables. As determined by stepwise regression using backward elimination (
Table S3), the best model was Model comprised LSM with an adjusted subdistribution hazard ratio (aSHR) of 1.03 per kPa (95% confidence interval (95%CI): 1.01–1.06,
p = 0.006) and ascites (aSHR: 3.43 (95%CI: 0.93–12.63).
p = 0.064). LSM showed prognostic value that was also independent from all other markers that were carried on from univariate analysis, as shown in
Table 2 as Models (A–C).
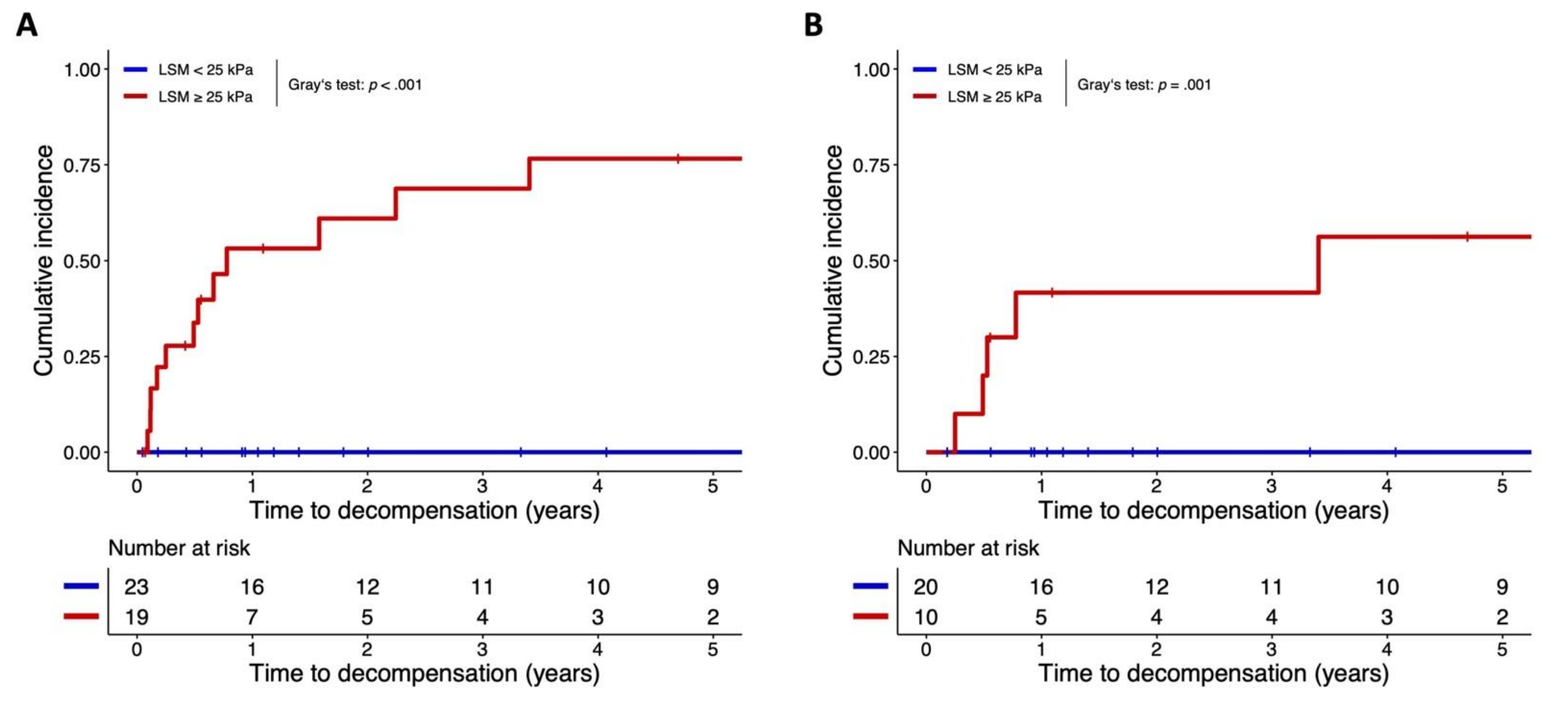
The ideal cut-off for prognostication of decompensation during FU via LSM as estimated by Youden’s index was 26.0 kPa; however, we applied a cut-off of 25 kPa (as recently proposed for ruling-in CSPH by the unpublished Baveno VII Consensus) that also showed 100% negative predictive value for decompensation during FU.
3.6. FU Data Stratified by VCTE-LSM ≥ 25 kPa versus <25 kPa
Decompensation during FU occurred exclusively in the 19 patients with LSM ≥ 25 kPa (
n = 12, 63.2%), while the 23 patients with liver stiffness < 25 kPa were protected from decompensation (
n = 0, 0.0%); the respective cumulative incidences are shown in
Figure 3 (Gray’s test:
p < 0.001). Four (21.1%) and two (8.7%) of patients with LSM ≥ 25 or <25 kPa developed HCC during FU, respectively. Liver transplantation was performed in four (21.1%) patients with ≥25 kPa, while none of the patients with lower liver stiffness underwent transplantation. Finally, liver-related death occurred in nine (47.4%) of the patients with high LSM values (zero non-liver-related deaths were observed), while zero (0%) liver-related and four (17.4%) non-liver-related deaths were recorded in the patients with VCTE-LSM < 25 kPa.
3.7. Prognostication in Patients with Compensated Advanced Chronic Liver Disease (cACLD)
In the subgroup of patients with cACLD at the time of on-treatment LSM (
n = 30), LSM (and other NITs) conferred similar prognostic value in AUROC analysis and competing risk regression in comparison to the overall cohort, as shown in
Table S4 and Figure S1. Only univariate analyses were conducted, owing to the low number (
n = 5) of events in the cACLD cohort. Again, events were exclusively recorded in patients that surpassed the ≥25 kPa threshold (
n = 5 (50.0%) developed first decompensation during FU), as compared to zero events in the <25 kPa group (Gray’s test:
p = 0.001); the cumulative incidences are shown in
Figure 3.
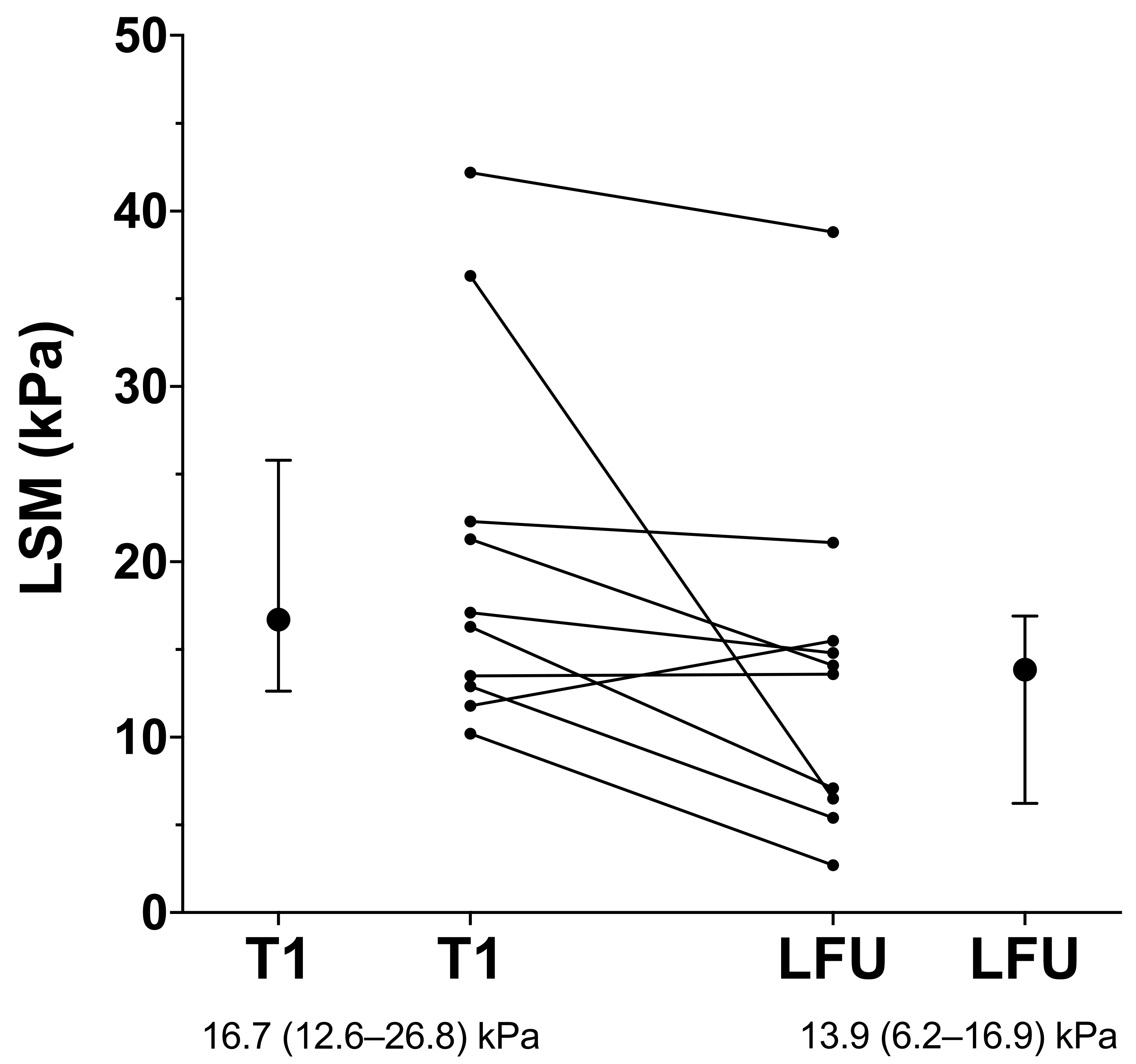
3.8. Patients with Additional LSM Values
Ten (23.8%) patients underwent additional LSM, with the last examination occurring after a median of 2.9 (1.2; 5.5) years of FU. Except for one patient, who was diagnosed with HCC shortly afterwards, all patients showed further decreases in liver stiffness, as shown in
Figure 4. Notably, the decreases in LSM values observed in nine patients were accompanied by in improvement in MELD (7 (6; 8) points during follow-up versus 8 (7; 11) points at baseline;
p = 0.087), and two patients regressed from Child-B to Child-A cirrhosis, while the other patients already had Child-A cirrhosis at baseline and remained stable.
4. Discussion
In our cohort of 42 thoroughly characterized cirrhotic HBV patients with pre-treatment CSPH, broadly available NITs—most importantly LSM—performed upon long-term stable viral suppression accurately predicted risk for decompensation, including liver-related mortality. LSM showed an excellent correlation with HVPG, whilst also being weakly associated with liver dysfunction, i.e., MELD, and PLT levels.
Most of the investigated NITs (LSM, MELD, and albumin levels) performed well in AUROC analyses for the prediction of decompensation during long-term HBV suppression, except for PLT count. Notably, the prognostic value of HVPG was excellent in the subgroup of patients who underwent hepatic vein catheterization, indicating the crucial pathomechanistic role of portal hypertension for decompensation in HBV patients with suppressed viral replication, which complements findings from HCV patients after direct acting antiviral (DAA) therapy [
11,
19].
The high cumulative incidence of (further) hepatic decompensation of 28.6% under chronic HBV suppression in our cohort is explained by the fact that patients who underwent liver vein catheterization had HVPG values that were mostly well above the CSPH threshold of ≥10 mmHg, with almost 50% surpassing the 16 mmHg threshold indicating severe portal hypertension [
20], and some patients already experienced decompensation events prior to NA treatment initiation. Overall, patients who developed (further) decompensation during FU had worse liver function, i.e., higher MELD, and more severe portal hypertension, i.e., higher HVPG and lower PLT, all of which correlated with LSM.
In competing risk regression, on-treatment LSM had prognostic value for hepatic decompensation during FU in analyses adjusted for either ascites, MELD or albumin.
Importantly, an LSM cut-off at 25 kPa (derived from Youden’s index and recently proposed by the unpublished Baveno VII Consensus for ruling-in CSPH after etiological cure) accurately assigned patients to a low-risk group (without hepatic decompensation during FU, negative predictive value: 100%) and a high-risk group for hepatic decompensation despite NA-induced HBV suppression. Notably, HCC occurred in both groups, highlighting the need for maintaining HCC screening in cirrhotic patients with pre-treatment CSPH who achieve HBV suppression.
Next, the findings regarding the prognostic performance of the investigated NITs were confirmed in a sensitivity analysis restricted to the patients with cACLD, suggesting that the NITs are more than mere reflections of the underlying disease status and—after further validation—may be applied in clinical practice as prognostic markers.
Lastly, our observation of regressing risk for decompensation in patients with NA-induced suppression of HBV and pretreatment CSPH was confirmed in a subset of patients who underwent an additional (‘last’) LSM during long-term FU. Except for patients developing HCC, continued decreases in liver stiffness were seen in all HBV-infected patients under NA-induced virologic suppression.
A major strength of our study is the validation of the correlation of NITs with the diagnostic gold standard for prognostication in portal hypertension, i.e., invasively measured HVPG. Interestingly, LSM conferred a similar prognostic value to HVPG. Importantly, we did not evaluate the prognostic value of pre-treatment levels of NITs; however, it was demonstrated in HCV patients after antiviral therapy that (standalone) post-treatment levels of NITs more accurately predict outcome [
14]. Patients with pre-therapy CSPH that show high LSM levels despite long-term NA-induced suppression of HBV should thus be carefully monitored, and preventive treatment, most importantly non-selective betablockers (NSBB), should be initiated/maintained to prevent decompensation [
21,
22], also due to recently described beneficial non-hemodynamic effects on systemic inflammation [
23,
24] that has been identified as a key driver of decompensation in advanced cirrhosis [
25].
Some limitations of this study need to be addressed: First, the low sample size and the unstandardized timepoints of follow-up LSM limit the conclusions that can be drawn from our study. However, strong signals were observed despite the low number of patients, which argues for the strength of the reported associations. Second, HVPG measurements were only conducted in a subgroup of patients. Those patients were generally more advanced, which may be explained by referral bias because clinicians are more likely to refer patients to an invasive re-evaluation if complications occur or liver function deteriorates despite etiological control. This also explains why only three out of 17 patients who underwent hepatic vein catheterization showed on-treatment HVPG levels below 10 mmHg as definite proof of resolution of CSPH induced by NA. However, LSM showed a strong correlation with (i) HVPG and (ii) outcome, and thus it may be assumed that a high proportion of the 54.8% of patients with LSM < 25 kPa (and thus protection from deleterious outcomes) had in fact resolved CSPH. Third, no definite conclusions regarding causality may be drawn from this retrospective analysis.
5. Conclusions
In summary, our study demonstrated that on-treatment LSM is a valuable, readily available tool for risk stratification in HBV-infected patients with pre-treatment CSPH and NA-induced viral suppression. LSM correlates well with portal hypertension in suppressed HBV patients with cirrhosis and CSPH, and an LSM cut-off at <25 kPa identified patients who were protected from decompensation or liver-related mortality during long-term FU. Patients that fail to improve to LSM < 25 kPa need close surveillance, and NSBB-treatment of portal hypertension, preferably with carvedilol [
21].
Supplementary Materials
The following supporting information can be downloaded at:
https://www.mdpi.com/article/10.3390/jpm12020239/s1, Table S1: Comparison of patient characteristics of the overall cohort of patients under long-term chronic NA therapy (i.e., at the time of FU assessment); Table S2: Univariate competing risk regression models for the overall cohort with (further) hepatic decompensation as outcome of interest and diagnosis of hepatocellular carcinoma and non-liver-related death as competing risks; Table S3: Results of a stepwise competing risk regression with backward elimination aiming at selecting a final mode with minimal Akaike information criterion (AIC); Table S4: Univariate competing risk regression models for the subcohort of patients with compensated advanced chronic liver disease (cACLD) with first hepatic decompensation as outcome of interest and diagnosis of hepatocellular carcinoma and non-liver-related death as competing risks; Figure S1: Time-dependent receiver operating characteristic curves for the prediction of first hepatic decompensation in the subcohort of patients with compensated advanced chronic liver disease (cACLD) within three years of follow-up by HVPG (AUROC = 1.000 (95% CI 1.000–1.000); available in
n = 11 patients), LSM (0.899 (0.757–1.000)), MELD (0.765 (0.533–0.996)), PLT (0.114 (0.000–0.277), inverse association) and albumin levels (0.084 (0.000–0.210), inverse association).
Author Contributions
Conceptualization; data curation, M.J., L.H., D.B., B.S., A.F.S., R.S., M.T., M.M. and T.R.; formal analysis and visualization, M.J. and T.R.; writing of the original draft, M.J., M.M. and T.R.; reviewing and editing, all authors; supervision, T.R. and M.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of the Medical University of Vienna (protocol code 1515/202, approved: 30 June 2020).
Informed Consent Statement
Patient consent was waived due to the retrospective nature of this study.
Data Availability Statement
Data can be obtained by contacting the corresponding author upon reasonable request.
Conflicts of Interest
M.J. served as a speaker for Gilead. L.H. declares no conflicts of interest. A.F.S. served as a speaker and/or consultant and/or advisory board member for Boehringer Ingelheim, Gilead and MSD. M.T. served as a speaker and/or consultant and/or advisory board member for Albireo, BiomX, Boehringer Ingelheim, Bristol-Myers Squibb, Falk, Genfit, Gilead, Intercept, Janssen, MSD, Novartis, Phenex, Regulus and Shire and received travel support from AbbVie, Falk, Gilead and Intercept, as well as grants/research support from Albireo, Cymabay, Falk, Gilead, Intercept, MSD and Takeda. Moreover, he is a co-inventor of patents on the medical use of 24-norursodeoxycholic acid. M.M. served as a speaker and/or consultant and/or advisory board member for AbbVie, Bristol-Myers Squibb, Gilead, Collective Acumen and W. L. Gore and Associates and received travel support from AbbVie, Bristol-Myers Squibb and Gilead. T.R. served as a speaker and/or consultant and/or advisory board member for AbbVie, Bayer, Boehringer Ingelheim, Gilead, Intercept, MSD, Siemens, and W. L. Gore and Associates and received grants/research support from AbbVie, Boehringer Ingelheim, Gilead, MSD and Philips.
References
- Lampertico, P.; Agarwal, K.; Berg, T.; Buti, M.; Janssen, H.L.; Papatheodoridis, G.; Zoulim, F.; Tacke, F. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J. Hepatol. 2017, 67, 370–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terrault, N.A.; Lok, A.S.; McMahon, B.J.; Chang, K.-M.; Hwang, J.; Jonas, M.M.; Brown, R.S., Jr.; Bzowej, N.H.; Wong, J.B. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology 2018, 67, 1560–1599. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.-L.; Shouval, D.; Lok, A.S.; Chang, T.-T.; Cheinquer, H.; Goodman, Z.; Dehertogh, D.; Wilber, R.; Zink, R.C.; Cross, A.; et al. Entecavir versus Lamivudine for Patients with HBeAg-Negative Chronic Hepatitis B. N. Engl. J. Med. 2006, 354, 1011–1020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marcellin, P.; Heathcote, E.J.; Buti, M.; Gane, E.; De Man, R.A.; Krastev, Z.; Germanidis, G.; Lee, S.S.; Flisiak, R.; Kaita, K.; et al. Tenofovir Disoproxil Fumarate versus Adefovir Dipivoxil for Chronic Hepatitis B. N. Engl. J. Med. 2008, 359, 2442–2455. [Google Scholar] [CrossRef]
- Kosi, L.; Reiberger, T.; Payer, B.A.; Grabmeier-Pfistershammer, K.; Strassl, R.; Rieger, A.; Peck-Radosavljevic, M. Five-year on-treatment efficacy of lamivudine-, tenofovir- and tenofovir + emtricitabine-based HAART in HBV-HIV-coinfected patients. J. Viral Hepat. 2012, 19, 801–810. [Google Scholar] [CrossRef]
- Marcellin, P.; Gane, E.; Buti, M.; Afdhal, N.; Sievert, W.; Jacobson, I.M.; Washington, M.K.; Germanidis, G.; Flaherty, J.F.; Schall, R.A.; et al. Regression of cirrhosis during treatment with tenofovir disoproxil fumarate for chronic hepatitis B: A 5-year open-label follow-up study. Lancet 2013, 381, 468–475. [Google Scholar] [CrossRef]
- Papatheodoridis, G.V.; Chan, H.L.-Y.; Hansen, B.E.; Janssen, H.L.; Lampertico, P. Risk of hepatocellular carcinoma in chronic hepatitis B: Assessment and modification with current antiviral therapy. J. Hepatol. 2015, 62, 956–967. [Google Scholar] [CrossRef] [Green Version]
- Su, T.-H.; Hu, T.-H.; Chen, C.-Y.; Huang, Y.-W.; Chuang, W.-L.; Lin, C.-C.; Wang, C.-C.; Su, W.-W.; Chen, M.-Y.; Peng, C.-Y.; et al. Four-year entecavir therapy reduces hepatocellular carcinoma, cirrhotic events and mortality in chronic hepatitis B patients. Liver Int. 2016, 36, 1755–1764. [Google Scholar] [CrossRef]
- Manolakopoulos, S.; Triantos, C.; Theodoropoulos, J.; Vlachogiannakos, J.; Kougioumtzan, A.; Papatheodoridis, G.; Tzourmakliotis, D.; Karamanolis, D.; Burroughs, A.K.; Archimandritis, A.; et al. Antiviral therapy reduces portal pressure in patients with cirrhosis due to HBeAg-negative chronic hepatitis B and significant portal hypertension. J. Hepatol. 2009, 51, 468–474. [Google Scholar] [CrossRef]
- Lampertico, P.; Invernizzi, F.; Viganò, M.; Loglio, A.; Mangia, G.; Facchetti, F.; Primignani, M.; Jovani, M.; Iavarone, M.; Fraquelli, M.; et al. The long-term benefits of nucleos(t)ide analogs in compensated HBV cirrhotic patients with no or small esophageal varices: A 12-year prospective cohort study. J. Hepatol. 2015, 63, 1118–1125. [Google Scholar] [CrossRef]
- Mandorfer, M.; Kozbial, K.; Schwabl, P.; Chromy, D.; Semmler, G.; Stättermayer, A.F.; Pinter, M.; Hernández-Gea, V.; Fritzer-Szekeres, M.; Steindl-Munda, P.; et al. Changes in Hepatic Venous Pressure Gradient Predict Hepatic Decompensation in Patients Who Achieved Sustained Virologic Response to Interferon—Free Therapy. Hepatology 2020, 71, 1023–1036. [Google Scholar] [CrossRef] [Green Version]
- Mandorfer, M.; Kozbial, K.; Schwabl, P.; Freissmuth, C.; Schwarzer, R.; Stern, R.; Chromy, D.; Stättermayer, A.F.; Reiberger, T.; Beinhardt, S.; et al. Sustained virologic response to interferon-free therapies ameliorates HCV-induced portal hypertension. J. Hepatol. 2016, 65, 692–699. [Google Scholar] [CrossRef] [PubMed]
- Mandorfer, M.; Hernández-Gea, V.; García-Pagán, J.C.; Reiberger, T. Noninvasive Diagnostics for Portal Hypertension: A Comprehensive Review. Semin. Liver Dis. 2020, 40, 240–255. [Google Scholar] [CrossRef] [PubMed]
- Semmler, G.; Binter, T.; Kozbial, K.; Schwabl, P.; Hametner-Schreil, S.; Zanetto, A.; Gavasso, S.; Chromy, D.; Bauer, D.J.; Simbrunner, B.; et al. Noninvasive Risk Stratification After HCV Eradication in Patients With Advanced Chronic Liver Disease. Hepatology 2021, 73, 1275–1289. [Google Scholar] [CrossRef] [PubMed]
- De Franchis, R.; Bosch, J.; Garcia-Tsao, G.; Reiberger, T.; Ripoll, C.; Abraldes, J.G.; Albillos, A.; Baiges, A.; Bajaj, J.; Bañares, R.; et al. Baveno VII—Renewing consensus in portal hypertension. J. Hepatol. 2021, in press. [Google Scholar] [CrossRef]
- Reiberger, T.; Schwabl, P.; Trauner, M.; Peck-Radosavljevic, M.; Mandorfer, M. Measurement of the Hepatic Venous Pressure Gradient and Transjugular Liver Biopsy. J. Vis. Exp. 2020, 160, e58819. [Google Scholar] [CrossRef]
- Blanche, P.; Dartigues, J.-F.; Jacqmin-Gadda, H. Estimating and comparing time-dependent areas under receiver operating characteristic curves for censored event times with competing risks. Stat. Med. 2013, 32, 5381–5397. [Google Scholar] [CrossRef]
- Fine, J.P.; Gray, R.J. A Proportional Hazards Model for the Subdistribution of a Competing Risk. J. Am. Stat. Assoc. 1999, 94, 496–509. [Google Scholar] [CrossRef]
- Lens, S.; Baiges, A.; Alvarado-Tapias, E.; Llop, E.; Martinez, J.; Fortea, J.I.; Ibáñez-Samaniego, L.; Mariño, Z.; Rodríguez-Tajes, S.; Gallego, A.; et al. Clinical outcome and hemodynamic changes following HCV eradication with oral antiviral therapy in patients with clinically significant portal hypertension. J. Hepatol. 2020, 73, 1415–1424. [Google Scholar] [CrossRef]
- Bosch, J.; Gonzalez-Abraldes, J.; Berzigotti, A.; Garcia-Pagan, J.C. The clinical use of HVPG measurements in chronic liver disease. Nat. Rev. Gastroenterol. Hepatol. 2009, 6, 573–582. [Google Scholar] [CrossRef]
- Villanueva, C.; Albillos, A.; Genescà, J.; Garcia-Pagan, J.C.; Calleja, J.L.; Aracil, C.; Bañares, R.; Morillas, R.M.; Poca, M.; Peñas, B.; et al. β blockers to prevent decompensation of cirrhosis in patients with clinically significant portal hypertension (PREDESCI): A randomised, double-blind, placebo-controlled, multicentre trial. Lancet 2019, 393, 1597–1608. [Google Scholar] [CrossRef]
- Jachs, M.; Reiberger, T. Prevention of Variceal Bleeding and Rebleeding by Nonselective Beta-Blockers. Clin. Liver Dis. 2021, 25, 311–326. [Google Scholar] [CrossRef] [PubMed]
- Jachs, M.; Hartl, L.; Schaufler, D.; Desbalmes, C.; Simbrunner, B.; Eigenbauer, E.; Bauer, D.J.M.; Paternostro, R.; Schwabl, P.; Scheiner, B.; et al. Amelioration of systemic inflammation in advanced chronic liver disease upon beta-blocker therapy translates into improved clinical outcomes. Gut 2021, 70, 1758–1767. [Google Scholar] [CrossRef] [PubMed]
- Jachs, M.; Hartl, L.; Simbrunner, B.; Bauer, D.; Paternostro, R.; Scheiner, B.; Schwabl, P.; Stättermayer, A.F.; Pinter, M.; Eigenbauer, E.; et al. Decreasing von Willebrand Factor Levels Upon Nonselective Beta Blocker Therapy Indicate a Decreased Risk of Further Decompensation, Acute-on-chronic Liver Failure, and Death. Clin. Gastroenterol. Hepatol. 2021, in press. [Google Scholar] [CrossRef]
- Costa, D.; Simbrunner, B.; Jachs, M.; Hartl, L.; Bauer, D.; Paternostro, R.; Schwabl, P.; Scheiner, B.; Stättermayer, A.F.; Pinter, M.; et al. Systemic inflammation increases across distinct stages of advanced chronic liver disease and correlates with decompensation and mortality. J. Hepatol. 2021, 74, 819–828. [Google Scholar] [CrossRef]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 




{kind=link}
{kind=link}
{kind=link}
{kind=link}