
Insulin as Monotherapy and in Combination with Other Glucose-Lowering Drugs Is Related to Increased Risk of Diagnosis of Pneumonia: A Longitudinal Assessment over Two Years

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Baseline Characteristics
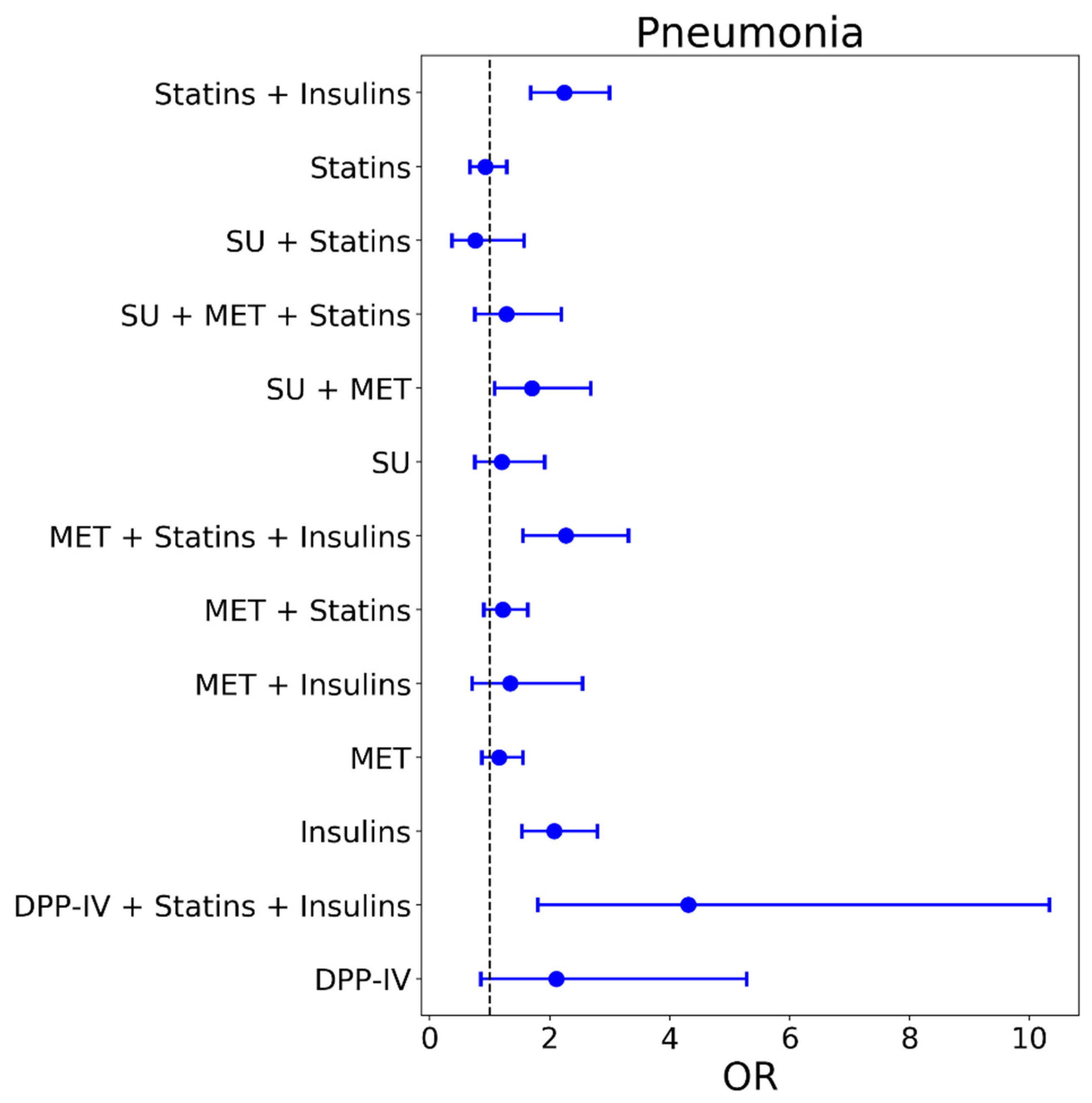
2.2. Relationship between Different Types of Glucose Lowering Drugs and Pneumonia
2.3. Sex-Specific Analysis
3. Discussion
4. Methods
4.1. Dataset and Study Population
4.2. Outcome Diagnoses, Definition of Baseline and Observational Period
4.3. Definition of Therapy Groups and Controls
4.4. Statistical Analysis
- The general model contains all patients and adjusts for sex, age and number of hospital days in baseline period (regression formula: ).
- The sex-specific model adjusts for age and number of hospital days in the baseline period, with separate regression models for female and male patients (regression formula: ).
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pick, H.; Daniel, P.; Rodrigo, C.; Bewick, T.; Ashton, D.; Lawrence, H.; Baskaran, V.; Edwards-Pritchard, R.C.; Sheppard, C.; Eletu, S.D.; et al. Pneumococcal serotype trends, surveillance and risk factors in UK adult pneumonia, 2013–2018. Thorax 2020, 75, 38–49. [Google Scholar] [CrossRef] [PubMed]
- Carey, I.M.; Critchley, J.A.; DeWilde, S.; Harris, T.; Hosking, F.J.; Cook, D.G. Risk of Infection in Type 1 and Type 2 Diabetes Compared With the General Population: A Matched Cohort Study. Diabetes Care 2018, 41, 513–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daryabor, G.; Atashzar, M.R.; Kabelitz, D.; Meri, S.; Kalantar, K. The Effects of Type 2 Diabetes Mellitus on Organ Metabolism and the Immune System. Front. Immunol. 2020, 11, 1582. [Google Scholar] [CrossRef] [PubMed]
- Leutner, M.; Haug, N.; Bellach, L.; Dervic, E.; Kautzky, A.; Klimek, P.; Kautzky-Willer, A. Risk of Typical Diabetes-Associated Complications in Different Clusters of Diabetic Patients: Analysis of Nine Risk Factors. J. Pers. Med. 2021, 11, 328. [Google Scholar] [CrossRef]
- Muller, L.M.; Gorter, K.J.; Hak, E.; Goudzwaard, W.L.; Schellevis, F.G.; Hoepelman, A.I.; Rutten, G.E. Increased risk of common infections in patients with type 1 and type 2 diabetes mellitus. Clin. Infect. Dis. 2005, 41, 281–288. [Google Scholar] [CrossRef] [Green Version]
- Shah, B.R.; Hux, J.E. Quantifying the risk of infectious diseases for people with diabetes. Diabetes Care 2003, 26, 510–513. [Google Scholar] [CrossRef] [Green Version]
- Kornum, J.B.; Thomsen, R.W.; Riis, A.; Lervang, H.H.; Schonheyder, H.C.; Sorensen, H.T. Type 2 diabetes and pneumonia outcomes: A population-based cohort study. Diabetes Care 2007, 30, 2251–2257. [Google Scholar] [CrossRef] [Green Version]
- Kornum, J.B.; Thomsen, R.W.; Riis, A.; Lervang, H.H.; Schonheyder, H.C.; Sorensen, H.T. Diabetes, glycemic control, and risk of hospitalization with pneumonia: A population-based case-control study. Diabetes Care 2008, 31, 1541–1545. [Google Scholar] [CrossRef] [Green Version]
- Berrou, J.; Fougeray, S.; Venot, M.; Chardiny, V.; Gautier, J.-F.; Dulphy, N.; Toubert, A.; Peraldi, M.-N. Natural Killer Cell Function, an Important Target for Infection and Tumor Protection, Is Impaired in Type 2 Diabetes. PLoS ONE 2013, 8, e62418. [Google Scholar] [CrossRef] [Green Version]
- Ma, H.; Liu, G.; Ding, W.; Wu, Y.; Cai, L.; Zhao, Y. Diabetes-induced alteration of F4/80+ macrophages: A study in mice with streptozotocin-induced diabetes for a long term. J. Mol. Med. 2008, 86, 391–400. [Google Scholar] [CrossRef]
- Forsythe, R.O.; Brownrigg, J.; Hinchliffe, R.J. Peripheral arterial disease and revascularization of the diabetic foot. Diabetes Obes. Metab. 2015, 17, 435–444. [Google Scholar] [CrossRef] [PubMed]
- Kolahian, S.; Leiss, V.; Nürnberg, B. Diabetic lung disease: Fact or fiction? Rev. Endocr. Metab. Disord. 2019, 20, 303–319. [Google Scholar] [CrossRef] [PubMed]
- Holman, N.; Knighton, P.; Kar, P.; O’Keefe, J.; Curley, M.; Weaver, A.; Barron, E.; Bakhai, C.; Khunti, K.; Wareham, N.J.; et al. Risk factors for COVID-19-related mortality in people with type 1 and type 2 diabetes in England: A population-based cohort study. Lancet Diabetes Endocrinol. 2020, 8, 823–833. [Google Scholar] [CrossRef]
- Khan, A.; Uddin, S.; Srinivasan, U. Comorbidity network for chronic disease: A novel approach to understand type 2 diabetes progression. Int. J. Med. Inform. 2018, 115, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Mortensen, E.M.; Nakashima, B.; Cornell, J.; Copeland, L.A.; Pugh, M.J.; Anzueto, A.; Good, C.; Restrepo, M.I.; Downs, J.R.; Frei, C.R.; et al. Population-based study of statins, angiotensin II receptor blockers, and angiotensin-converting enzyme inhibitors on pneumonia-related outcomes. Clin. Infect. Dis. 2012, 55, 1466–1473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torres, A.; Blasi, F.; Dartois, N.; Akova, M. Which individuals are at increased risk of pneumococcal disease and why? Impact of COPD, asthma, smoking, diabetes, and/or chronic heart disease on community-acquired pneumonia and invasive pneumococcal disease. Thorax 2015, 70, 984–989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, B.; Li, C.; Sun, Y.; Wang, D.W. Insulin Treatment Is Associated with Increased Mortality in Patients with COVID-19 and Type 2 Diabetes. Cell Metab. 2021, 33, 65–77.e2. [Google Scholar] [CrossRef] [PubMed]
- Cariou, B.; Hadjadj, S.; Wargny, M.; Pichelin, M.; Al-Salameh, A.; Allix, I.; Amadou, C.; Arnault, G.; Baudoux, F.; Bauduceau, B.; et al. Phenotypic characteristics and prognosis of inpatients with COVID-19 and diabetes: The CORONADO study. Diabetologia 2020, 63, 1500–1515. [Google Scholar] [CrossRef]
- McGurnaghan, S.J.; Weir, A.; Bishop, J.; Kennedy, S.; Blackbourn, L.A.K.; McAllister, D.A.; Hutchinson, S.; Caparrotta, T.M.; Mellor, J.; Jeyam, A.; et al. Risks of and risk factors for COVID-19 disease in people with diabetes: A cohort study of the total population of Scotland. Lancet Diabetes Endocrinol. 2021, 9, 82–93. [Google Scholar] [CrossRef]
- Khunti, K.; Knighton, P.; Zaccardi, F.; Bakhai, C.; Barron, E.; Holman, N.; Kar, P.; Meace, C.; Sattar, N.; Sharp, S.; et al. Prescription of glucose-lowering therapies and risk of COVID-19 mortality in people with type 2 diabetes: A nationwide observational study in England. Lancet Diabetes Endocrinol. 2021, 9, 293–303. [Google Scholar] [CrossRef]
- Mertz, D.; Kim, T.H.; Johnstone, J.; Lam, P.P.; Science, M.; Kuster, S.P.; Fadel, S.A.; Tran, D.; Fernandez, E.; Bhatnagar, N.; et al. Populations at risk for severe or complicated influenza illness: Systematic review and meta-analysis. BMJ 2013, 347, f5061. [Google Scholar] [CrossRef] [Green Version]
- Sharifipour, E.; Shams, S.; Esmkhani, M.; Khodadadi, J.; Fotouhi-Ardakani, R.; Koohpaei, A.; Doosti, Z.; Ej Golzari, S. Evaluation of bacterial co-infections of the respiratory tract in COVID-19 patients admitted to ICU. BMC Infect. Dis. 2020, 20, 646. [Google Scholar] [CrossRef]
- van Niekerk, G.; Christowitz, C.; Conradie, D.; Engelbrecht, A.M. Insulin as an immunomodulatory hormone. Cytokine Growth Factor Rev. 2020, 52, 34–44. [Google Scholar] [CrossRef]
- Tsai, S.; Clemente-Casares, X.; Zhou, A.C.; Lei, H.; Ahn, J.J.; Chan, Y.T.; Choi, O.; Luck, H.; Woo, M.; Dunn, S.E.; et al. Insulin Receptor-Mediated Stimulation Boosts T Cell Immunity during Inflammation and Infection. Cell Metab. 2018, 28, 922–934.e4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dandona, P.; Ghanim, H.; Bandyopadhyay, A.; Korzeniewski, K.; Ling Sia, C.; Dhindsa, S.; Chaudhuri, A. Insulin suppresses endotoxin-induced oxidative, nitrosative, and inflammatory stress in humans. Diabetes Care 2010, 33, 2416–2423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kidd, L.B.; Schabbauer, G.A.; Luyendyk, J.P.; Holscher, T.D.; Tilley, R.E.; Tencati, M.; Mackman, N. Insulin activation of the phosphatidylinositol 3-kinase/protein kinase B (Akt) pathway reduces lipopolysaccharide-induced inflammation in mice. J. Pharmacol. Exp. Ther. 2008, 326, 348–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dror, E.; Dalmas, E.; Meier, D.T.; Wueest, S.; Thevenet, J.; Thienel, C.; Timper, K.; Nordmann, T.M.; Traub, S.; Schulze, F.; et al. Postprandial macrophage-derived IL-1beta stimulates insulin, and both synergistically promote glucose disposal and inflammation. Nat. Immunol. 2017, 18, 283–292. [Google Scholar] [CrossRef] [Green Version]
- Filgueiras, L.R.; Capelozzi, V.L.; Martins, J.O.; Jancar, S. Sepsis-induced lung inflammation is modulated by insulin. BMC Pulm. Med. 2014, 14, 177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, A.; Shi, M.; Wu, H.; Lau, E.S.H.; Ma, R.C.W.; Kong, A.P.S.; So, W.Y.; Luk, A.O.Y.; Chan, J.C.N.; Chow, E. Long-term metformin use and risk of pneumonia and related death in type 2 diabetes: A registry-based cohort study. Diabetologia 2021, 64, 1760–1765. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Walther, F.J.; Sengers, R.M.; Laghmani, E.H.; Salam, A.; Folkerts, G.; Pera, T.; Wagenaar, G.T. Metformin attenuates hyperoxia-induced lung injury in neonatal rats by reducing the inflammatory response. Am. J. Physiol. Lung Cell Mol. Physiol. 2015, 309, L262–L270. [Google Scholar] [CrossRef] [Green Version]
- Cameron, A.R.; Morrison, V.L.; Levin, D.; Mohan, M.; Forteath, C.; Beall, C.; McNeilly, A.D.; Balfour, D.J.; Savinko, T.; Wong, A.K.; et al. Anti-Inflammatory Effects of Metformin Irrespective of Diabetes Status. Circ. Res. 2016, 119, 652–665. [Google Scholar] [CrossRef] [Green Version]
- Seabold, S.; Perktold, J. statsmodels: Econometric and statistical modeling with python. In Proceedings of the 9th Python in Science Conference, Austin, TX, USA, 28 June–3 July 2010. [Google Scholar]
- McKinney, W. Data structures for statistical computing in python. In Proceedings of the 9th Python in Science Conference, Austin, TX, USA, 28 June–3 July 2010; Volume 445, pp. 51–56. [Google Scholar]


{kind=link}
| Therapy Group | Number of Patients in Therapy Group | % of Patients with Outcome in Observation Period | Mean Age at End of Baseline Period | Sex Distribution (% Females/% Males) |
|---|---|---|---|---|
| MET 1 | 6798 | 1.37 | 67.83 ± 10.83 | 49%/51% |
| MET + Statins | 5865 | 1.52 | 69.85 ± 9.18 | 48%/52% |
| Statins | 3872 | 1.55 | 73.56 ± 8.55 | 50%/50% |
| Insulin | 3720 | 2.45 | 66.57 ± 9.72 | 42%/58% |
| Insulin + Statins | 2939 | 3.27 | 70.62 ± 8.95 | 43%/57% |
| MET + Insulin + Statins | 1596 | 2.69 | 68.27 ± 8.86 | 49%/51% |
| MET + SU 2 | 1122 | 2.14 | 70.25 ± 10.36 | 52%/48% |
| SU | 1091 | 2.02 | 74.63 ± 11.19 | 55%/45% |
| MET + SU + Statins | 882 | 1.81 | 71.87 ± 8.62 | 47%/53% |
| MET + Insulin | 722 | 1.52 | 66.50 ± 11.48 | 56%/44% |
| SU + Statins | 555 | 1.44 | 76.38 ± 8.89 | 54%/46% |
| MET + TZD 3 + Statins | 201 | 0.5 | 69.06 ± 8.24 | 49%/51% |
| DPP-IV 4 | 191 | 2.62 | 69.44 ± 10.41 | 56%/44% |
| MET + DPP-IV + Statins | 189 | 2.12 | 69.19 ± 9.10 | 52%/48% |
| DPP-IV + Statins | 183 | 1.64 | 72.47 ± 9.63 | 53%/47% |
| MET + TZD | 158 | 1.9 | 67.51 ± 7.94 | 49%/51% |
| DPP-IV + SU | 140 | 2.14 | 73.63 ± 10.19 | 49%/51% |
| DPP-IV + SU + Statins | 134 | 0.75 | 76.28 ± 8.04 | 55%/45% |
| MET + DPP-IV | 137 | 1.46 | 64.28 ± 9.89 | 45%/55% |
| TZD | 116 | 0.86 | 70.09 ± 9.98 | 44%/56% |
| TZD + Statins | 105 | 2.86 | 70.99 ± 8.96 | 49%/51% |
| MET + other-AD 5 | 96 | 3.12 | 69.74 ± 9.56 | 46%/54% |
| DPP-IV + Insulins + Statins | 92 | 6.52 | 72.48 ± 7.62 | 60%/40% |
| TZD + SU | 86 | 1.16 | 74.59 ± 9.74 | 57%/43% |
| TZD + SU + Statins | 78 | 2.56 | 75.13 ± 7.01 | 54%/46% |
| MET + TZD + SU | 70 | 4.29 | 70.99 ± 8.71 | 50%/50% |
| Other-AD + Statins | 62 | 3.23 | 73.77 ± 8.28 | 36%/64% |
| Alpha-Gluc.-Inh. 6 | 46 | 2.17 | 70.35 ± 14.36 | 65%/35% |
| Alpha-Gluc.-Inh. + Statins | 37 | 2.7 | 74.44 ± 10.01 | 45%/55% |
| DPP-IV + Insulin | 31 | 3.23 | 69.78 ± 11.42 | 72%/28% |
| Insulin + SU | 26 | 3.85 | 68.49 ± 11.00 | 65%/35% |
| MET + Alpha-Gluc.-Inh. | 23 | 8.7 | 69.39 ± 13.11 | 52%/48% |
| DPP-IV + Other-AD + Statins | 13 | 7.69 | 67.31 ± 9.99 | 38%/62% |
| MET + Alpha-Gluc.-Inh. + Statins | 11 | 9.09 | 75.18 ± 6.27 | 73%/27% |
| DPP-IV + Other-AD | 10 | 10 | 69.91 ± 11.94 | 100%/0% |
| Controls | 6568 | 1.55 | 72.83 ± 9.96 | 58%/42% |
| Therapy Group | OR (Confidence Interval) | p-Value |
|---|---|---|
| MET | 1.15 (0.78–1.71) | 0.48 |
| MET + Statins | 1.31 (0.88–1.94) | 0.19 |
| Statins | 1.18 (0.79–1.78) | 0.42 |
| Insulin | 2.02 (1.35–3.03) | <0.001 |
| Statins + Insulin | 2.38 (1.61–3.51) | <0.001 |
| MET + Statins + Insulin | 2.44 (1.46–4.07) | <0.001 |
| MET + SU | 1.53 (0.80–2.91) | 0.20 |
| SU | 1.61 (0.89–2.91) | 0.12 |
| MET + Statins + SU | 1.18 (0.57–2.42) | 0.66 |
| MET + Insulin | 1.28 (0.50–3.33) | 0.61 |
| Statins + SU | 1.06 (0.45–2.50) | 0.90 |
| Therapy Group | OR (CI) | p-Value |
|---|---|---|
| MET | 1.17 (0.75–1.82) | 0.49 |
| MET + Statins | 1.09 (0.70–1.71) | 0.70 |
| Statins | 0.61 (0.35–1.07) | 0.09 |
| Insulin | 2.17 (1.40–3.37) | <0.001 |
| Statins + Insulin | 2.12 (1.37–3.29) | <0.001 |
| MET + Statins + Insulin | 2.08 (1.17–3.70) | 0.012 |
| MET + SU | 1.91 (1.00–3.64) | 0.048 |
| SU | 0.80 (0.36–1.78) | 0.59 |
| MET + Statins + SU | 1.45 (0.65–3.23) | 0.36 |
| MET + Insulin | 1.41 (0.59–3.35) | 0.43 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leutner, M.; Kaleta, M.; Bellach, L.; Kautzky, A.; Thurner, S.; Klimek, P.; Kautzky-Willer, A. Insulin as Monotherapy and in Combination with Other Glucose-Lowering Drugs Is Related to Increased Risk of Diagnosis of Pneumonia: A Longitudinal Assessment over Two Years. J. Pers. Med. 2021, 11, 984. https://doi.org/10.3390/jpm11100984
Leutner M, Kaleta M, Bellach L, Kautzky A, Thurner S, Klimek P, Kautzky-Willer A. Insulin as Monotherapy and in Combination with Other Glucose-Lowering Drugs Is Related to Increased Risk of Diagnosis of Pneumonia: A Longitudinal Assessment over Two Years. Journal of Personalized Medicine. 2021; 11(10):984. https://doi.org/10.3390/jpm11100984
Chicago/Turabian StyleLeutner, Michael, Michaela Kaleta, Luise Bellach, Alexander Kautzky, Stefan Thurner, Peter Klimek, and Alexandra Kautzky-Willer. 2021. "Insulin as Monotherapy and in Combination with Other Glucose-Lowering Drugs Is Related to Increased Risk of Diagnosis of Pneumonia: A Longitudinal Assessment over Two Years" Journal of Personalized Medicine 11, no. 10: 984. https://doi.org/10.3390/jpm11100984