
Novel Insights into Diagnosis, Biology and Treatment of Primary Diffuse Leptomeningeal Melanomatosis

 , ,
, ,  ,
,  , , and add
Show full author list
, , and add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Material and Ethical Considerations
2.2. Case Study
2.3. Literature Review
2.4. Neuropathology
2.5. Next Generation Sequencing (NGS)
2.6. Cell Models
2.6.1. Adenosine triphosphate (ATP) Assay
2.6.2. Protein Isolation and Western Blotting
2.7. Liquid Biopsy
3. Results
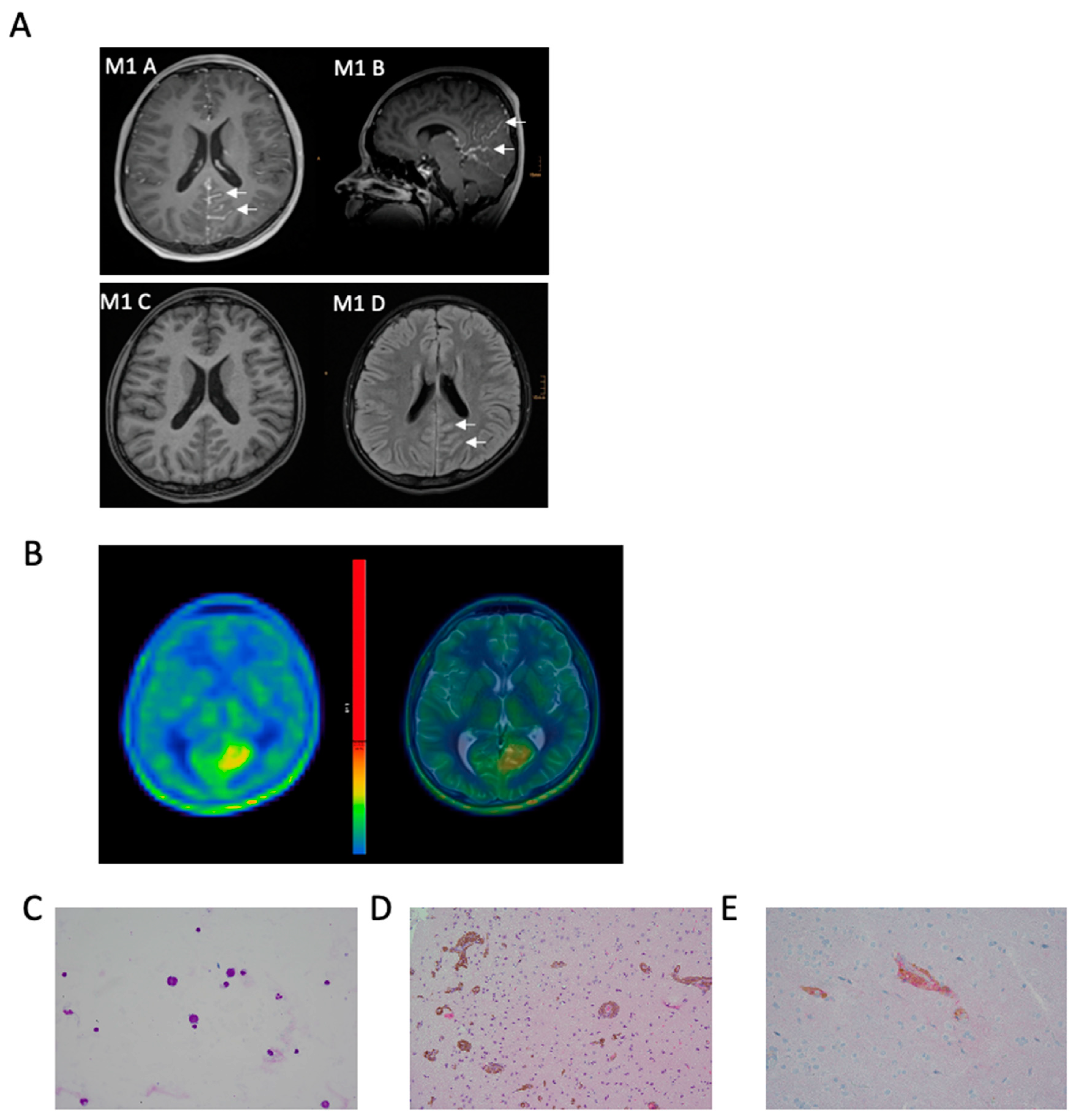
3.1. Illustrative Case
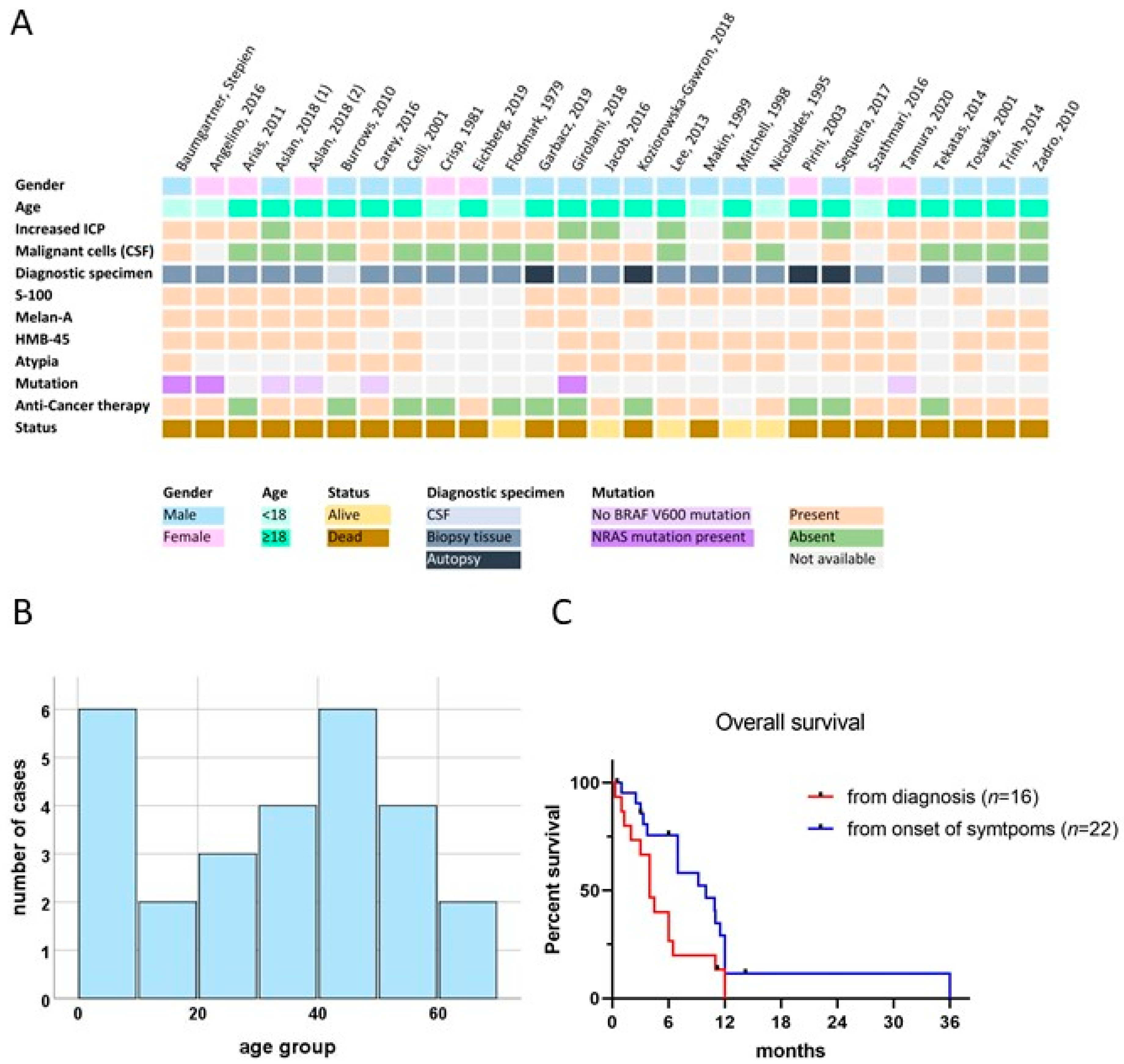
3.2. Clinical Characteristics of PDLMM
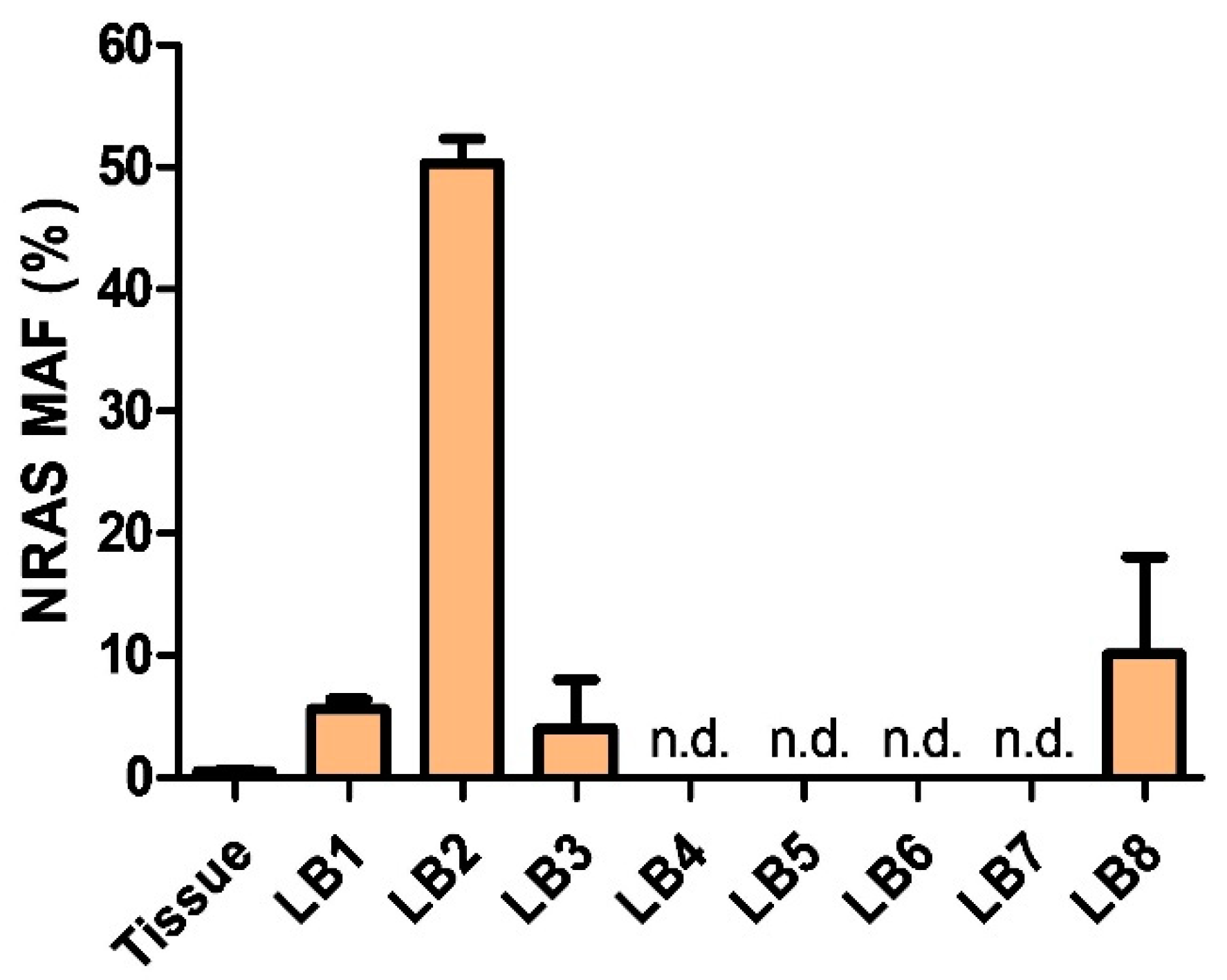
3.3. Detection of NRAS-Mutant cfDNA via Liquid Biopsy
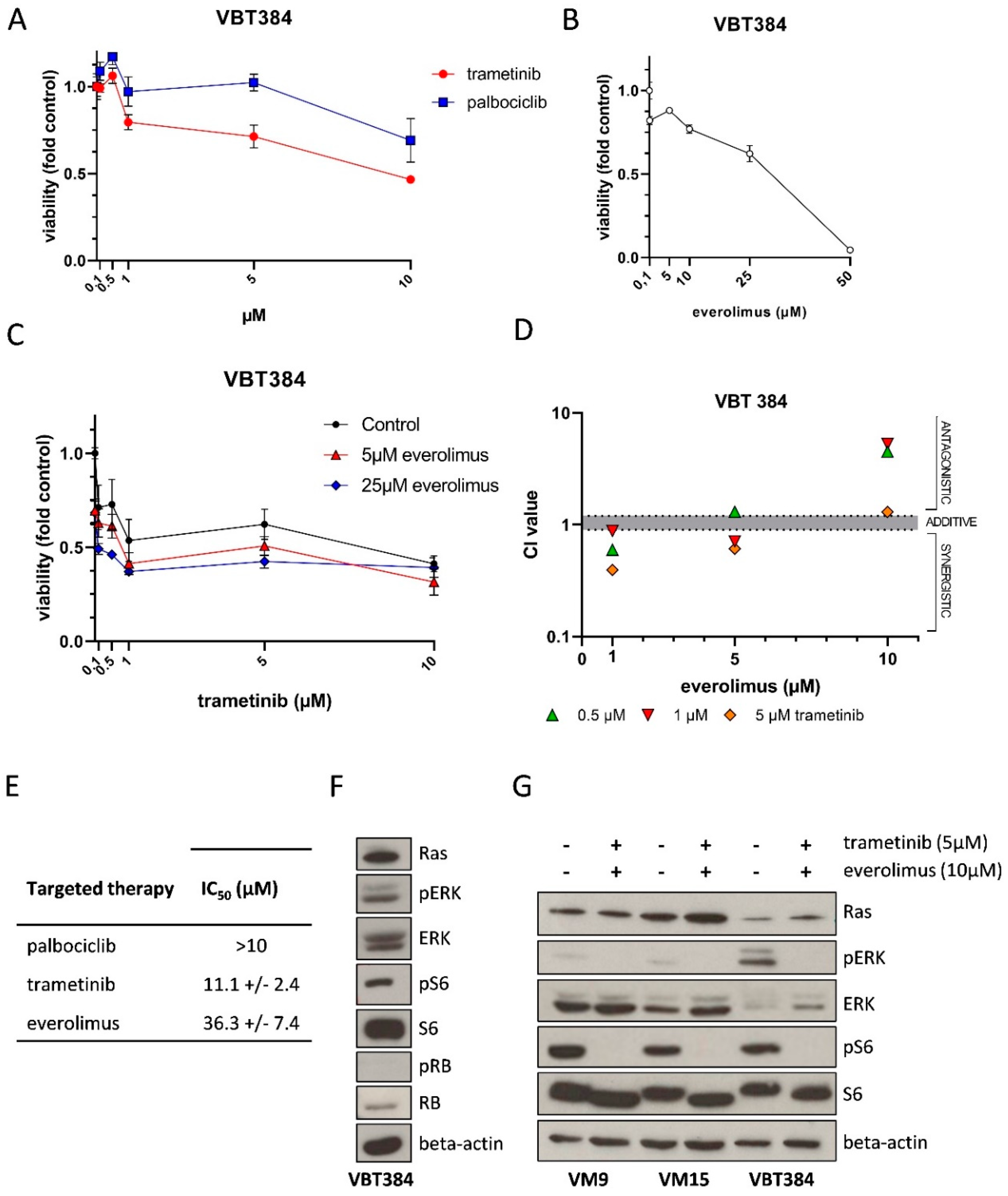
3.4. In Vitro Drug Sensitivity and Pathway Activation in Patient Derived PDLMM Cells
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Küsters-Vandevelde, H.V.; Willemsen, A.E.; Groenen, P.J.; Küsters, B.; Lammens, M.; Wesseling, P.; Djafarihamedani, M.; Rijntjes, J.; Delye, H.; Willemsen, M.A.; et al. Experimental treatment of NRAS-mutated neurocutaneous melanocytosis with MEK162, a MEK-inhibitor. Acta Neuropathol. Commun. 2014, 2, 41. [Google Scholar] [CrossRef] [Green Version]
- Louis, D.N.; Perry, A.; Reifenberger, G.; von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, E.J.; Johnson, D.B.; Sosman, J.A.; Chandra, S. Melanoma: What do all the mutations mean? Cancer 2018, 124, 3490–3499. [Google Scholar] [CrossRef] [PubMed]
- Schadendorf, D.; van Akkooi, A.C.J.; Berking, C.; Griewank, K.G.; Gutzmer, R.; Hauschild, A.; Stang, A.; Roesch, A.; Ugurel, S. Melanoma. Lancet (Lond. Engl.) 2018, 392, 971–984. [Google Scholar] [CrossRef]
- Colebatch, A.J.; Ferguson, P.; Newell, F.; Kazakoff, S.H.; Witkowski, T.; Dobrovic, A.; Johansson, P.A.; Saw, R.P.M.; Stretch, J.R.; McArthur, G.A.; et al. Molecular Genomic Profiling of Melanocytic Nevi. J. Investig. Dermatol. 2019, 139, 1762–1768. [Google Scholar] [CrossRef] [PubMed]
- Zaman, A.; Wu, W.; Bivona, T.G. Targeting Oncogenic BRAF: Past, Present, and Future. Cancers 2019, 11, 1197. [Google Scholar] [CrossRef] [Green Version]
- Grill, C.; Larue, L. NRAS, NRAS, Which Mutation Is Fairest of Them All? J. Investig. Dermatol. 2016, 136, 1936–1938. [Google Scholar] [CrossRef] [Green Version]
- Zou, Z.; Tao, T.; Li, H.; Zhu, X. mTOR signaling pathway and mTOR inhibitors in cancer: Progress and challenges. Cell Biosci. 2020, 10, 31. [Google Scholar] [CrossRef]
- Tekataş, A.; Gemici, Y.İ.; Tuncel, S.A.; Cağlı, B.; Taştekin, E.; Unlu, E.; Celik, Y. A Rare Cause of Headache and Increased Intracranial Pressure: Primary Leptomeningeal Melanomatosis. Turk Noroloji Dergisi. 2014, 20, 138–140. [Google Scholar] [CrossRef]
- Trinh, V.; Medina-Flores, R.; Taylor, C.L.; Yonas, H.; Chohan, M.O. Primary melanocytic tumors of the central nervous system: Report of two cases and review of literature. Surg. Neurol. Int. 2014, 5, 147. [Google Scholar]
- Makin, G.W.; Eden, O.B.; Lashford, L.S.; Moppett, J.; Gerrard, M.P.; Davies, H.A.; Powell, C.V.; Campbell, A.N.; Frances, H. Leptomeningeal melanoma in childhood. Cancer 1999, 86, 878–886. [Google Scholar] [CrossRef]
- Tosaka, M.; Tamura, M.; Oriuchi, N.; Horikoshi, M.; Joshita, T.; Sugawara, K.; Kobayashi, S.; Kohga, H.; Yoshida, T.; Sasaki, T. Cerebrospinal fluid immunocytochemical analysis and neuroimaging in the diagnosis of primary leptomeningeal melanoma. Case report. J. Neurosurg. 2001, 94, 528–532. [Google Scholar] [CrossRef] [PubMed]
- Angelino, G.; De Pasquale, M.D.; De Sio, L.; Serra, A.; Massimi, L.; De Vito, R.; Marrazzo, A.; Lancella, L.; Carai, A.; Antonelli, M.; et al. NRAS(Q61K) mutated primary leptomeningeal melanoma in a child: Case presentation and discussion on clinical and diagnostic implications. BMC Cancer 2016, 16, 512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujimori, K.; Sakai, K.; Higashiyama, F.; Oya, F.; Maejima, T.; Miyake, T. Primary central nervous system malignant melanoma with leptomeningeal melanomatosis: A case report and review of the literature. Neurosurg. Rev. 2018, 41, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Garbe, C.; Amaral, T.; Peris, K.; Hauschild, A.; Arenberger, P.; Bastholt, L.; Bataille, V.; del Marmol, V.; Dréno, B.; Fargnoli, M.C.; et al. European consensus-based interdisciplinary guideline for melanoma. Part 2: Treatment–Update 2019. Eur. J. Cancer 2020, 126, 159–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dummer, R.; Schadendorf, D.; Ascierto, P.A.; Arance, A.; Dutriaux, C.; Di Giacomo, A.M.; Rutkowski, P.; Del Vecchio, M.; Gutzmer, R.; Mandala, M.; et al. Binimetinib versus dacarbazine in patients with advanced NRAS-mutant melanoma (NEMO): A multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2017, 18, 435–445. [Google Scholar] [CrossRef]
- Matter, A.V.; Micaletto, S.; Urner-Bloch, U.; Dummer, R.; Goldinger, S.M. Long-Term Response to Intermittent Binimetinib in Patients with NRAS-Mutant Melanoma. Oncologist 2020, 25, e1593–e1597. [Google Scholar] [CrossRef] [PubMed]
- Sakai, K.; Takeda, M.; Shimizu, S.; Takahama, T.; Yoshida, T.; Watanabe, S.; Iwasa, T.; Yonesaka, K.; Suzuki, S.; Hayashi, H.; et al. A comparative study of curated contents by knowledge-based curation system in cancer clinical sequencing. Sci. Rep. 2019, 9, 11340. [Google Scholar] [CrossRef]
- Berger, W.; Elbling, L.; Minai-Pour, M.; Vetterlein, M.; Pirker, R.; Kokoschka, E.-M.; Micksche, M. Intrinsic MDR-1 gene and P-glycoprotein expression in human melanoma cell lines. Int. J. Cancer 1994, 59, 717–723. [Google Scholar] [CrossRef]
- Ghassemi, S.; Vejdovszky, K.; Sahin, E.; Ratzinger, L.; Schelch, K.; Mohr, T.; Peter-Vörösmarty, B.; Brankovic, J.; Lackner, A.; Leopoldi, A.; et al. FGF5 is expressed in melanoma and enhances malignancy in vitro and in vivo. Oncotarget 2017, 8, 87750–87762. [Google Scholar] [CrossRef] [Green Version]
- Chou, T.C. Drug combination studies and their synergy quantification using the Chou-Talalay method. Cancer Res. 2010, 70, 440–446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peyrl, A.; Chocholous, M.; Azizi, A.A.; Czech, T.; Dorfer, C.; Mitteregger, D.; Gojo, J.; Minichmayr, E.; Slavc, I. Safety of Ommaya reservoirs in children with brain tumors: A 20-year experience with 5472 intraventricular drug administrations in 98 patients. J. Neurooncol. 2014, 120, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.-J.; Rutkowski, P.; Lao, C.D.; Cowey, C.L.; Schadendorf, D.; Wagstaff, J.; Dummer, R.; et al. Five-Year Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2019, 381, 1535–1546. [Google Scholar] [CrossRef] [Green Version]
- Flodmark, O.; Fitz, C.R.; Harwood-Nash, D.C.; Chuang, S.H. Neuroradiological findings in a child with primary leptomeningeal melanoma. Neuroradiology 1979, 18, 153–156. [Google Scholar] [PubMed]
- Crisp, D.E.; Thompson, J.A. Primary Malignant Melanomatosis of the Meninges: Clinical Course and Computed Tomographic Findings in a Young Child. Arch. Neurol. 1981, 38, 528–529. [Google Scholar] [CrossRef]
- Nicolaides, P.; Newton, R.W.; Kelsey, A. Primary malignant melanoma of meninges: Atypical presentation of subacute meningitis. Pediatr. Neurol. 1995, 12, 172–174. [Google Scholar] [CrossRef]
- Mitchell, P.J.; Funt, S.A.; Gonzales, M.F.; Popovic, E.A. Primary pineal and meningeal malignant melanomatosis. J. Clin. Neurosci. Off. J. Neurosurg. Soc. Australas. 1998, 5, 353–356. [Google Scholar] [CrossRef]
- Celli, P.; Acqui, M.; Trillò, G.; Ramundo, E.O.; D’Andrea, G.; Roperto, R.; Ferrante, L. Primary leptomeningeal melanomatosis: Early leptomeningeal enhancement on MRI. J. Neurosurg. Sci. 2001, 45, 235–240. [Google Scholar]
- Pirini, M.G.; Mascalchi, M.; Salvi, F.; Tassinari, C.A.; Zanella, L.; Bacchini, P.; Bertoni, F.; D’Errico, A.; Corti, B.; Grigioni, W.F. Primary diffuse meningeal melanomatosis: Radiologic-pathologic correlation. AJNR Am. J. Neuroradiol. 2003, 24, 115–118. [Google Scholar]
- Burrows, A.M.; Smith, T.W.; Hall, W.R.; Pilitsis, J.G. Neurological picture. Ascending paralysis from malignant leptomeningeal melanomatosis. J. Neurol. Neurosurg. Psychiatry 2010, 81, 449–450. [Google Scholar] [CrossRef] [PubMed]
- Zadro, I.; Brinar, V.V.; Barun, B.; Ozretic, D.; Pažanin, L.; Grahovac, G.; Habek, M. Primary Diffuse Meningeal Melanomatosis. Neurologist 2010, 16, 115–118. [Google Scholar] [CrossRef]
- Arias, M.; Alberte-Woodward, M.; Arias, S.; Dapena, D.; Prieto, A.; Suárez-Peñaranda, J.M. Primary malignant meningeal melanomatosis: A clinical, radiological and pathologic case study. Acta Neurol. Belgica 2011, 111, 228–231. [Google Scholar]
- Lee, H.J.; Ahn, B.C.; Hwang, S.W.; Cho, S.K.; Kim, H.W.; Lee, S.W.; Hwang, J.H.; Lee, J. F-18 fluorodeoxyglucose PET/CT and post hoc PET/MRI in a case of primary meningeal melanomatosis. Korean J. Radiol. 2013, 14, 343–349. [Google Scholar] [CrossRef]
- Carey, A.R.; Bermudez-Magner, J.A.; Dubovy, S.R.; Schatz, N.J.; Sternau, L.L.; Sklar, E.M.; Lam, B.L. “TB or Not TB?” That is the Question. J. Neuro Ophthalmol. 2016, 36, 2472. [Google Scholar] [CrossRef] [PubMed]
- Jacob, M.; Delfort, F.; Heliette, C.; Renard, D. Brain 18F-choline PET/CT in primary diffuse leptomeningeal melanomatosis. Acta Neurol. Belgica 2016, 116, 647–648. [Google Scholar] [CrossRef] [PubMed]
- Szathmari, A.; Perbet, R.; Hermier, M.; Di Rocco, F.; Frappaz, D.; Mottolese, C. Primary Amelanotic Leptomeningeal Melanomatosis in a Child: A Rare but Severe Disease. World Neurosurg. 2016, 92, 581.e515–581.e520. [Google Scholar] [CrossRef] [PubMed]
- Sequeira, P.; Souto, A.; Coelho, H.; Oliveira, J.; Nogueira, J.; Oliveira, A. The dark side of the brain-an autopsy case. Virchows Arch. 2017, 471, S292. [Google Scholar]
- Aslan, S.; Gocmen, R.; Acar, N.P.; Khasiyev, F.; Gumeler, E.; Soylemezoglu, F.; Tuncer, A.; Arsava, E.M.; Topçuoglu, M.A.; Unal Cevik, I. Two cases of primary leptomeningeal melanomatosis mimicking subacute meningitis. Neuroradiol. J. 2018, 31, 42–46. [Google Scholar] [CrossRef] [Green Version]
- Girolami, I.; Cima, L.; Ghimenton, C.; Zannoni, M.; Mombello, A.; Riva, G.; Cirielli, V.; Corradi, G.; Vogrig, A.; Di Stefano, G.; et al. NRAS(Q61K) mutated diffuse leptomeningeal melanomatosis in an adult patient with a brief review of the so-called "forme fruste" of neurocutaneous melanosis. Brain Tumor Pathol. 2018, 35, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Koziorowska-Gawron, E.; Kaczorowski, M.; Bladowska, J.; Budrewicz, S.; Koszewicz, M.; Hałoń, A. Diagnostic Difficulties in Primary Pauci-Melanotic Leptomeningeal Melanomatosis. Eur. Neurol. 2018, 80, 68–70. [Google Scholar] [CrossRef]
- Eichberg, D.G.; Achua, J.K.; Locatelli, E.; Shah, A.H.; Komotar, R.J.; Ghods, A.J. Primary Diffuse Leptomeningeal Melanomatosis: Case Report and Review of the Literature. World Neurosurg. 2019, 122, 648–655. [Google Scholar] [CrossRef] [PubMed]
- Garbacz, T.; Osuchowski, M.; Bartosik-Psujek, H. Primary diffuse meningeal melanomatosis-a rare form of meningeal melanoma: Case report. BMC Neurol. 2019, 19, 271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tamura, Y.; Umeda, Y.; Umeda, M.; Oyake, M.; Usuda, H.; Fujita, N. A case of meningeal melanomatosis diagnosed by immunostaining of cerebrospinal fluid. Rinsho Shinkeigaku Clin. Neurol. 2020, 60, 565–568. [Google Scholar] [CrossRef] [PubMed]
- Harstad, L.; Hess, K.R.; Groves, M.D. Prognostic factors and outcomes in patients with leptomeningeal melanomatosis. Neuro. Oncol. 2008, 10, 1010–1018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slavc, I.; Schuller, E.; Falger, J.; Günes, M.; Pillwein, K.; Czech, T.; Dietrich, W.; Rössler, K.; Dieckmann, K.; Prayer, D.; et al. Feasibility of long-term intraventricular therapy with mafosfamide (n = 26) and etoposide (n = 11): Experience in 26 children with disseminated malignant brain tumors. J. Neurooncol. 2003, 64, 239–247. [Google Scholar] [CrossRef]
- Peyrl, A.; Sauermann, R.; Chocholous, M.; Azizi, A.A.; Jäger, W.; Höferl, M.; Slavc, I. Pharmacokinetics and toxicity of intrathecal liposomal cytarabine in children and adolescents following age-adapted dosing. Clin. Pharmacokinet. 2014, 53, 165–173. [Google Scholar] [CrossRef]
- Küsters-Vandevelde, H.V.; Küsters, B.; van Engen-van Grunsven, A.C.; Groenen, P.J.; Wesseling, P.; Blokx, W.A. Primary melanocytic tumors of the central nervous system: A review with focus on molecular aspects. Brain Pathol. (Zurich Switzerland) 2015, 25, 209–226. [Google Scholar] [CrossRef] [PubMed]
- Kinsler, V.A.; Thomas, A.C.; Ishida, M.; Bulstrode, N.W.; Loughlin, S.; Hing, S.; Chalker, J.; McKenzie, K.; Abu-Amero, S.; Slater, O.; et al. Multiple congenital melanocytic nevi and neurocutaneous melanosis are caused by postzygotic mutations in codon 61 of NRAS. J. Investig. Dermatol. 2013, 133, 2229–2236. [Google Scholar] [CrossRef] [Green Version]
- Salgado, C.M.; Basu, D.; Nikiforova, M.; Bauer, B.S.; Johnson, D.; Rundell, V.; Grunwaldt, L.J.; Reyes-Múgica, M. BRAF mutations are also associated with neurocutaneous melanocytosis and large/giant congenital melanocytic nevi. Pediatric Dev. Pathol. Off. J. Soc. Pediatric Pathol. Paediatric Pathol. Soc. 2015, 18, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Arsene, D.; Ardeleanu, C.; Balescu, C.; Nistorescu, A. Meningeal melanocytosis in a young patient--an autopsy diagnosis. Clin. Neuropathol. 2007, 26, 294–298. [Google Scholar] [CrossRef]
- Brunsvig, K.L.; Zenobi, M.; Rilliet, B.; El Hassani, Y.; de Haller, R.; Ansari, M.; Lobrinus, J.A.; Hanquinet, S.; Fluss, J. Primary leptomeningeal melanocytosis in a 10-year-old girl: A challenging diagnosis with a poor prognosis. J. Child Neurol. 2011, 26, 1444–1448. [Google Scholar] [CrossRef] [PubMed]
- Grini-Mazouzi, M.; Thouvenot, E.; Sabaah, M.; Rigau, V.; Charif, M. Leptomeningeal melanocytosis: A fatal course of a benign tumor. Revue Neurol. 2012, 168, 461–463. [Google Scholar] [CrossRef]
- Nikola, Z.; Dragan, M.; Mijović, Z.; Milentijević, M.J. Primary leptomeningeal melanocytosis--a case report with an autopsy diagnosis. Vojnosanit. Pregl. 2012, 69, 631–634. [Google Scholar] [PubMed]
- Martínez-Sáez, E.; Monlleó Neila, L.; Sánchez-Montañez, A.; Poca, M.A.; Roig, M.; Ortega Aznar, A. Chronic headache as presentation of an uncommon disease in a 15-year-old boy. Clin. Neuropathol. 2013, 32, 538–539. [Google Scholar]
- Ng, R.Y.; Siu, D.Y.; Wong, G.K.; Ng, H.K.; Poon, W.S. An uncommon mimic of spontaneous subarachnoid haemorrhage. Hong Kong Med J. Xianggang Yi Xue Za Zhi 2013, 19, 80–81. [Google Scholar]
- Honigberg, M.C.; Papavassiliou, E.; Cohen, Y.Z. Primary leptomeningeal melanocytosis presenting as chronic meningitis. J. Clin. Neurosci. Off. J. Neurosurg. Soc. Australas. 2014, 21, 1056–1058. [Google Scholar] [CrossRef] [PubMed]
- Noronha, C.; Rocha, L. Meningeal melanocytosis: A challenging diagnosis. Lancet. Oncol. 2019, 20, e343. [Google Scholar] [CrossRef]
- Hossain, F.A.; Marquez, H.J.; Veltkamp, D.L.; Xie, S.Q.; Klesse, L.J.; Timmons, C.F.; Pfeifer, C.M. CT and MRI findings in leptomeningeal melanocytosis. Radiol. Case Rep. 2020, 15, 186–189. [Google Scholar] [CrossRef]
- Tawbi, H.A.; Forsyth, P.A.; Algazi, A.; Hamid, O.; Hodi, F.S.; Moschos, S.J.; Khushalani, N.I.; Lewis, K.; Lao, C.D.; Postow, M.A.; et al. Combined Nivolumab and Ipilimumab in Melanoma Metastatic to the Brain. N. Engl. J. Med. 2018, 379, 722–730. [Google Scholar] [CrossRef]
- Queirolo, P.; Boutros, A.; Tanda, E.; Spagnolo, F.; Quaglino, P. Immune-checkpoint inhibitors for the treatment of metastatic melanoma: A model of cancer immunotherapy. Semin. Cancer Biol. 2019, 59, 290–297. [Google Scholar] [CrossRef]
- Rose, A.A.N.; Armstrong, S.M.; Hogg, D.; Butler, M.O.; Saibil, S.D.; Arteaga, D.P.; Pimentel Muniz, T.; Kelly, D.; Ghazarian, D.; King, I.; et al. Biologic subtypes of melanoma predict survival benefit of combination anti-PD1+anti-CTLA4 immune checkpoint inhibitors versus anti-PD1 monotherapy. J. Immunother. Cancer 2021, 9. [Google Scholar] [CrossRef]
- Long, G.V.; Atkinson, V.; Lo, S.; Sandhu, S.; Guminski, A.D.; Brown, M.P.; Wilmott, J.S.; Edwards, J.; Gonzalez, M.; Scolyer, R.A.; et al. Combination nivolumab and ipilimumab or nivolumab alone in melanoma brain metastases: A multicentre randomised phase 2 study. Lancet Oncol. 2018, 19, 672–681. [Google Scholar] [CrossRef]
- Guida, M.; Bartolomeo, N.; Quaglino, P.; Madonna, G.; Pigozzo, J.; Di Giacomo, A.M.; Minisini, A.M.; Tucci, M.; Spagnolo, F.; Occelli, M.; et al. No Impact of NRAS Mutation on Features of Primary and Metastatic Melanoma or on Outcomes of Checkpoint Inhibitor Immunotherapy: An Italian Melanoma Intergroup (IMI) Study. Cancers 2021, 13, 475. [Google Scholar] [CrossRef]
- Pasquali, S.; Hadjinicolaou, A.V.; Chiarion Sileni, V.; Rossi, C.R.; Mocellin, S. Systemic treatments for metastatic cutaneous melanoma. Cochrane Database Syst. Rev. 2018, 2, Cd011123. [Google Scholar] [CrossRef]
- Becco, P.; Gallo, S.; Poletto, S.; Frascione, M.P.M.; Crotto, L.; Zaccagna, A.; Paruzzo, L.; Caravelli, D.; Carnevale-Schianca, F.; Aglietta, M. Melanoma Brain Metastases in the Era of Target Therapies: An Overview. Cancers 2020, 12, 1640. [Google Scholar] [CrossRef]
- Delyon, J.; Lebbe, C.; Dumaz, N. Targeted therapies in melanoma beyond BRAF: Targeting NRAS-mutated and KIT-mutated melanoma. Curr. Opin. Oncol. 2020, 32, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Posch, C.; Ortiz-Urda, S. NRAS mutant melanoma—Undrugable? Oncotarget 2013, 4, 494–495. [Google Scholar] [CrossRef] [Green Version]
- Tolcher, A.W.; Bendell, J.C.; Papadopoulos, K.P.; Burris, H.A., 3rd; Patnaik, A.; Jones, S.F.; Rasco, D.; Cox, D.S.; Durante, M.; Bellew, K.M.; et al. A phase IB trial of the oral MEK inhibitor trametinib (GSK1120212) in combination with everolimus in patients with advanced solid tumors. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2015, 26, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Mayr, L.; Gunter, A.S.; Madlener, S.; Schmook, M.T.; Peyrl, A.; Azizi, A.; Dieckmann, K.; Reisinger, D.; Stepien, N.; Schramm, K.; et al. Cerebrospinal Fluid Penetration and Combination Therapy of Entrectinib for Disseminated ROS1/NTRK-Fusion Positive Pediatric High-Grade Gliome. J. Pers. Med. 2020, 10, 290. [Google Scholar] [CrossRef] [PubMed]
- Kinsler, V.A.; O’Hare, P.; Jacques, T.; Hargrave, D.; Slater, O. MEK inhibition appears to improve symptom control in primary NRAS-driven CNS melanoma in children. Br. J. Cancer 2017, 116, 990–993. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galldiks, N.; Kocher, M.; Ceccon, G.; Werner, J.M.; Brunn, A.; Deckert, M.; Pope, W.B.; Soffietti, R.; Le Rhun, E.; Weller, M.; et al. Imaging challenges of immunotherapy and targeted therapy in patients with brain metastases: Response, progression, and pseudoprogression. Neuro. Oncol. 2020, 22, 17–30. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.K.; Hoon, D.S.B. Liquid biopsy utility for the surveillance of cutaneous malignant melanoma patients. Mol. Oncol. 2016, 10, 450–463. [Google Scholar] [CrossRef]
- Velazquez-Campoy, A.; Vega, S.; Sanchez-Gracia, O.; Lanas, A.; Rodrigo, A.; Kaliappan, A.; Hall, M.B.; Nguyen, T.Q.; Brock, G.N.; Chesney, J.A.; et al. Thermal liquid biopsy for monitoring melanoma patients under surveillance during treatment: A pilot study. Biochim. Biophys. Gen. Subj. 2018, 1862, 1701–1710. [Google Scholar] [CrossRef]
- Sacco, A.; Forgione, L.; Carotenuto, M.; Luca, A.; Ascierto, P.A.; Botti, G.; Normanno, N. Circulating Tumor DNA Testing Opens New Perspectives in Melanoma Management. Cancers 2020, 12, 2914. [Google Scholar] [CrossRef] [PubMed]
- Boire, A.; Brandsma, D.; Brastianos, P.K.; Le Rhun, E.; Ahluwalia, M.; Junck, L.; Glantz, M.; Groves, M.D.; Lee, E.Q.; Lin, N.; et al. Liquid biopsy in central nervous system metastases: A RANO review and proposals for clinical applications. Neuro. Oncol. 2019, 21, 571–584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madlener, S.; Gojo, J. Liquid Biomarkers for Pediatric Brain Tumors: Biological Features, Advantages and Perspectives. J. Pers. Med. 2020, 10, 254. [Google Scholar] [CrossRef]
- Zheng, M.M.; Li, Y.S.; Jiang, B.Y.; Tu, H.Y.; Tang, W.F.; Yang, J.J.; Zhang, X.C.; Ye, J.Y.; Yan, H.H.; Su, J.; et al. Clinical Utility of Cerebrospinal Fluid Cell-Free DNA as Liquid Biopsy for Leptomeningeal Metastases in ALK-Rearranged NSCLC. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2019, 14, 924–932. [Google Scholar] [CrossRef]
- Ge, M.; Zhan, Q.; Zhang, Z.; Ji, X.; Zhou, X.; Huang, R.; Liang, X. Different next-generation sequencing pipelines based detection of tumor DNA in cerebrospinal fluid of lung adenocarcinoma cancer patients with leptomeningeal metastases. BMC Cancer 2019, 19, 143. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | ||
|---|---|---|
| Sex | n | % |
| Male | 19 | 70 |
| Female | 8 | 30 |
| Age | n | % |
| 0 to 10 | 6 | 22 |
| 10 to 20 | 2 | 7 |
| 20 to 30 | 3 | 11 |
| 30 to 40 | 4 | 15 |
| 40 to 50 | 6 | 22 |
| 50 to 60 | 4 | 15 |
| >60 | 2 | 7 |
| years | ||
| Median age | 36 | |
| Age range | 2.3–68 | |
| Symptoms | n | % |
| Nausea/vomiting | 20 | 77 |
| Headache | 18 | 69 |
| Cognitive deficits | 11 | 42 |
| Paresthesia | 7 | 27 |
| Cranial nerve palsy | 6 | 23 |
| Anorexia | 6 | 23 |
| Seizures | 5 | 19 |
| Amnesia | 5 | 19 |
| Peripheral paresis/plegia | 4 | 15 |
| Ataxia | 3 | 12 |
| Fever | 3 | 12 |
| Any pain | 2 | 7 |
| Fatigue | 1 | 4 |
| Increased intracranial pressure | n | % |
| Yes | 18 | 67 |
| No | 7 | 26 |
| Unknown | 2 | 7 |
| Intervention for increased ICP | n | % |
| Yes | 15 | 56 |
| No | 12 | 44 |
| CSF values | n | % |
| Pleocytosis | 18 | 86 |
| Elevated protein | 14 | 67 |
| Low glucose | 16 | 76 |
| Malignant cells in CSF | n | % |
| Yes | 7 | 33 |
| No | 14 | 67 |
| Anti-tumor therapy | n | % |
| Irradiation | 5 | 20 |
| Chemotherapy | 10 | 40 |
| Targeted therapy | 1 | 4 |
| Immunotherapy | 5 | 20 |
| Intraventricular therapy | 2 | 8 |
| Anti-tumor therapy (total) | 14 | 56 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baumgartner, A.; Stepien, N.; Mayr, L.; Madlener, S.; Dorfer, C.; Schmook, M.T.; Traub-Weidinger, T.; Lötsch-Gojo, D.; Kirchhofer, D.; Reisinger, D.; et al. Novel Insights into Diagnosis, Biology and Treatment of Primary Diffuse Leptomeningeal Melanomatosis. J. Pers. Med. 2021, 11, 292. https://doi.org/10.3390/jpm11040292
Baumgartner A, Stepien N, Mayr L, Madlener S, Dorfer C, Schmook MT, Traub-Weidinger T, Lötsch-Gojo D, Kirchhofer D, Reisinger D, et al. Novel Insights into Diagnosis, Biology and Treatment of Primary Diffuse Leptomeningeal Melanomatosis. Journal of Personalized Medicine. 2021; 11(4):292. https://doi.org/10.3390/jpm11040292
Chicago/Turabian StyleBaumgartner, Alicia, Natalia Stepien, Lisa Mayr, Sibylle Madlener, Christian Dorfer, Maria T. Schmook, Tatjana Traub-Weidinger, Daniela Lötsch-Gojo, Dominik Kirchhofer, Dominik Reisinger, and et al. 2021. "Novel Insights into Diagnosis, Biology and Treatment of Primary Diffuse Leptomeningeal Melanomatosis" Journal of Personalized Medicine 11, no. 4: 292. https://doi.org/10.3390/jpm11040292