A Pooled Analysis of Serum Phosphate Measurements and Potential Hypophosphataemia Events in 45 Interventional Trials with Ferric Carboxymaltose


 and
and
Abstract
:1. Introduction
2. Methods
3. Results
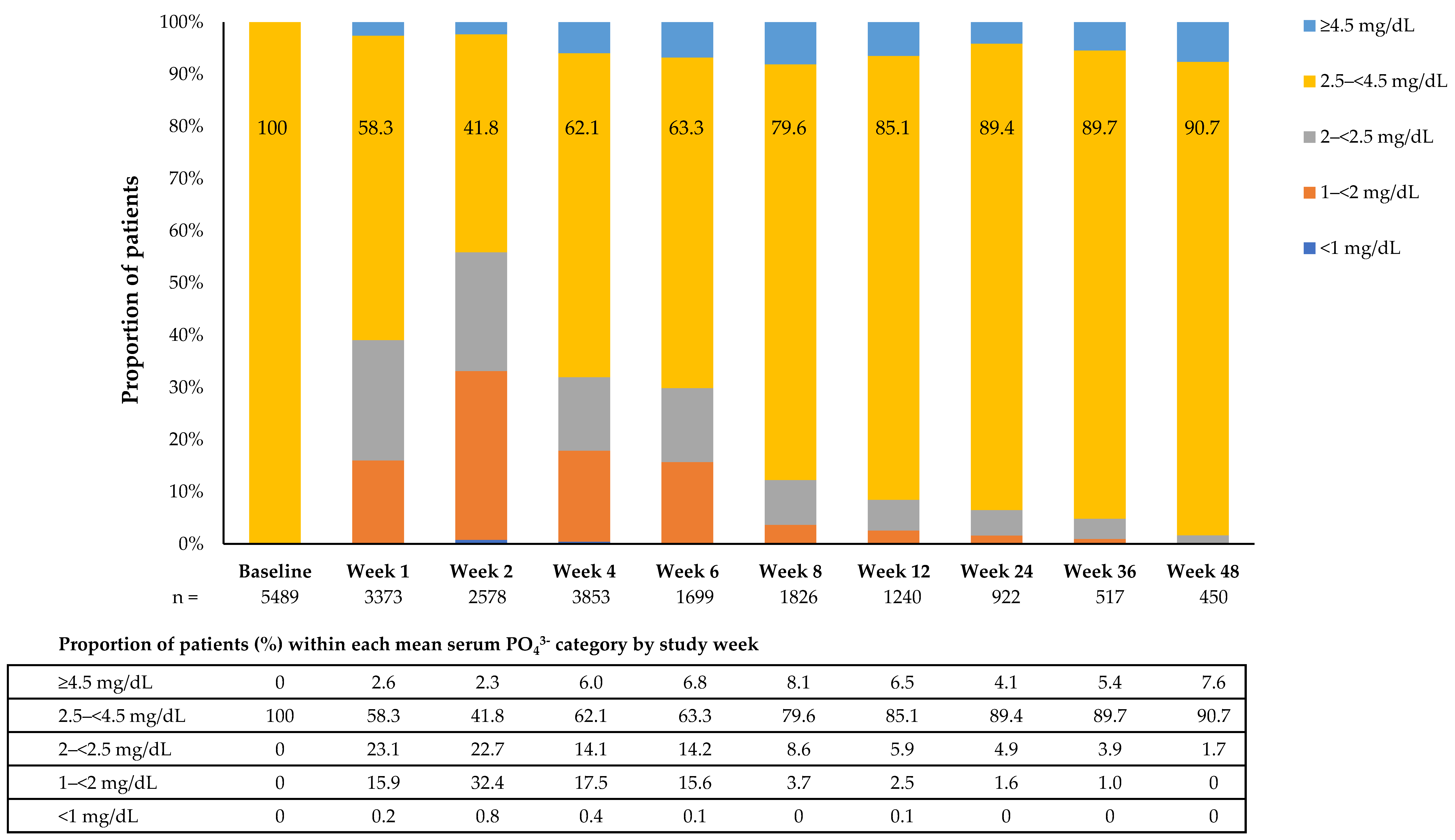
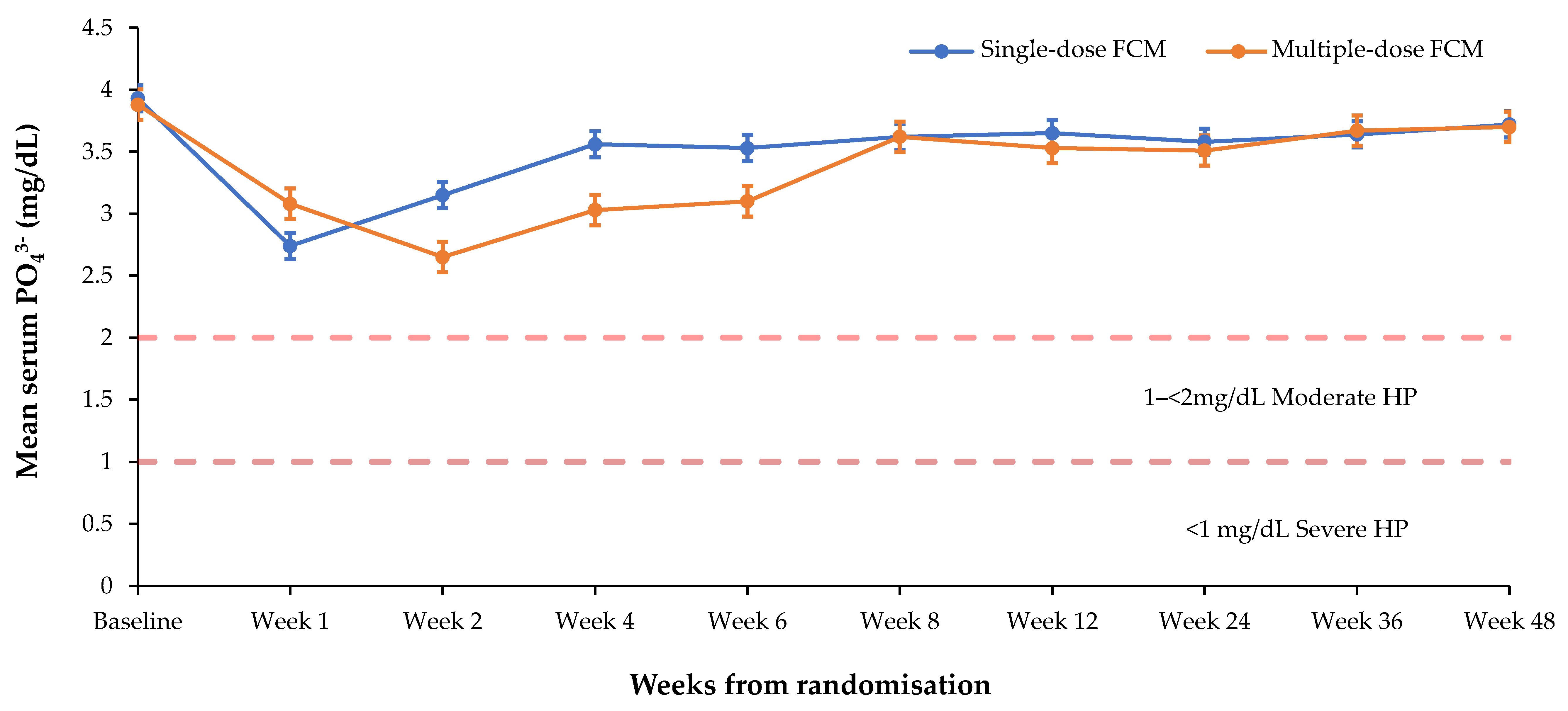
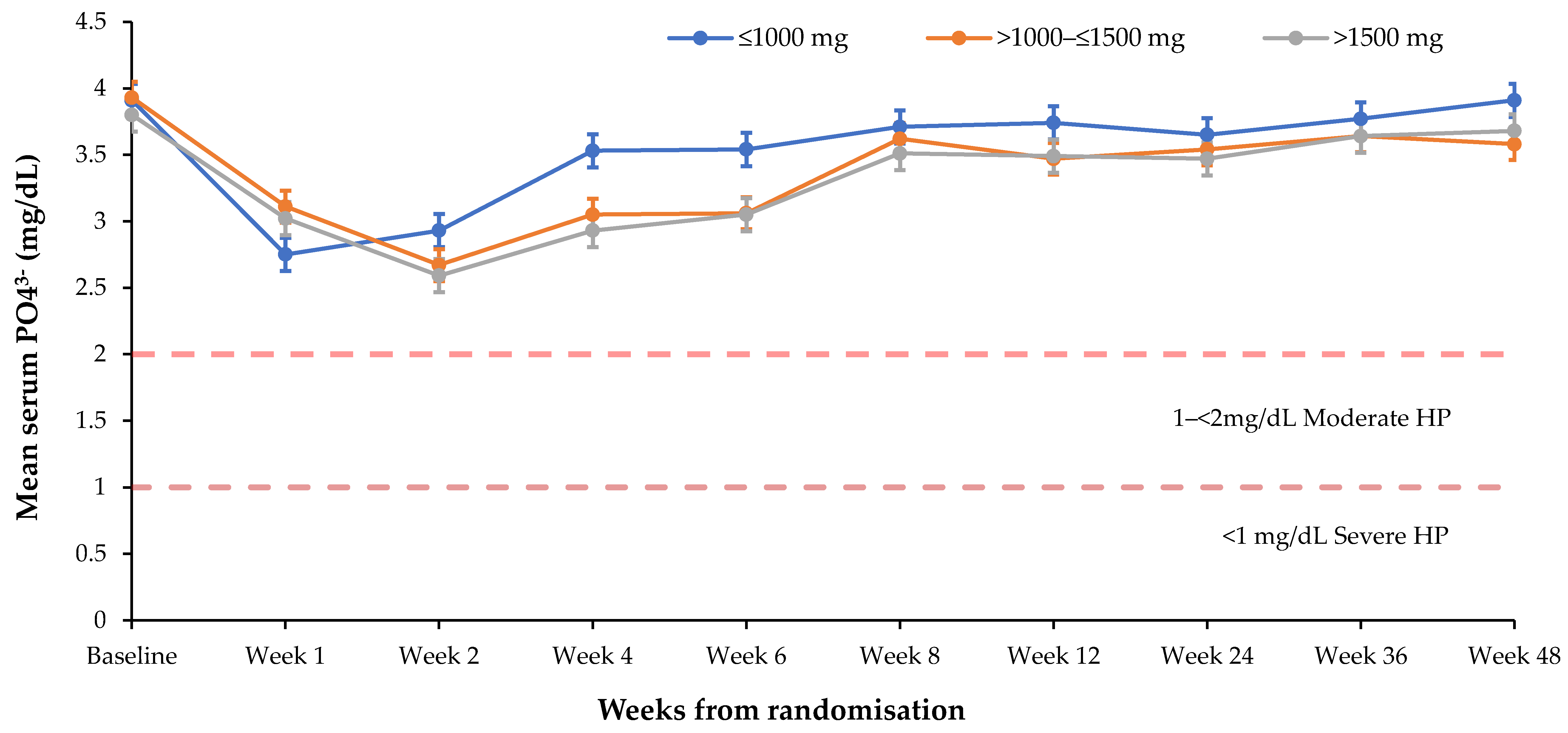
3.1. Effect of FCM on Serum PO43− Levels
3.2. Risk Factors for Hypophosphataemia
3.3. Adverse Events Possibly Associated with Hypophosphataemia
3.3.1. Investigator-Reported Adverse Events of HP
3.3.2. Clinical Signs Possibly Related to HP
3.3.3. Adjudicated Symptoms among Subjects with Investigator-Reported HP
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References and Note
- Gaasbeek, A.; Meinders, A.E. Hypophosphatemia: An update on its etiology and treatment. Am. J. Med. 2005, 118, 1094–1101. [Google Scholar] [CrossRef]
- Manghat, P.; Sodi, R.; Swaminathan, R. Phosphate homeostasis and disorders. Ann. Clin. Biochem. 2014, 51, 631–656. [Google Scholar] [CrossRef] [Green Version]
- Imel, E.A.; Econs, M.J. Approach to the hypophosphatemic patient. J. Clin. Endocrinol. Metab. 2012, 97, 696–706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carpenter, T.O. Primary Disorders of Phosphate Metabolism. In Endotext; Feingold, K.R., Anawalt, B., Boyce, A., Chrousos, G., Dungan, K., Grossman, A., Hershman, J.M., Hofland, H.J., Kaltsas, G., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2000. [Google Scholar]
- Land, J.M.; Kemp, G.J.; Taylor, D.J.; Standing, S.J.; Radda, G.K.; Rajagopalan, B. Oral phosphate supplements reverse skeletal muscle abnormalities in a case of chronic fatigue with idiopathic renal hypophosphatemia. Neuromuscul. Disord. 1993, 3, 223–225. [Google Scholar] [CrossRef]
- O’Connor, L.R.; Wheeler, W.S.; Bethune, J.E. Effect of hypophosphatemia on myocardial performance in man. N. Engl. J. Med. 1977, 297, 901–903. [Google Scholar] [CrossRef]
- Singhal, P.C.; Kumar, A.; Desroches, L.; Gibbons, N.; Mattana, J. Prevalence and predictors of rhabdomyolysis in patients with hypophosphatemia. Am. J. Med. 1992, 92, 458–464. [Google Scholar] [CrossRef]
- De Oliveira Iglesias, S.B.; Pons Leite, H.; de Carvalho, W.B. Hypophosphatemia-induced seizure in a child with diabetic ketoacidosis. Pediatr. Emerg. Care 2009, 25, 859–861. [Google Scholar] [CrossRef]
- Poesen, R.; Dierickx, D.; Evenepoel, P. Hemolytic anemia associated with severe hypophosphatemia in a renal transplant recipient. Transpl. Int. 2012, 25, e27–e28. [Google Scholar] [CrossRef]
- Goldsweig, B.K.; Carpenter, T.O. Hypophosphatemic rickets: Lessons from disrupted FGF23 control of phosphorus homeostasis. Curr. Osteoporos. Rep. 2015, 13, 88–97. [Google Scholar] [CrossRef]
- Felsenfeld, A.J.; Levine, B.S. Approach to treatment of hypophosphatemia. Am. J. Kidney Dis. 2012, 60, 655–661. [Google Scholar] [CrossRef]
- Camp, M.A.; Allon, M. Severe hypophosphatemia in hospitalized patients. Miner. Electrolyte Metab. 1990, 16, 365–368. [Google Scholar] [PubMed]
- Geerse, D.A.; Bindels, A.J.; Kuiper, M.A.; Roos, A.N.; Spronk, P.E.; Schultz, M.J. Treatment of hypophosphatemia in the intensive care unit: A review. Crit. Care 2010, 14, R147. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Xiao, C.; Chen, L.; Zhang, X.; Kou, Q. Impact of hypophosphatemia on outcome of patients in intensive care unit: A retrospective cohort study. BMC Anesthesiol. 2019, 19, 86. [Google Scholar] [CrossRef] [PubMed]
- Roldan, C.J. A case of near-fatal hypophosphatemia. J. Emerg. Med. 2004, 26, 241–242. [Google Scholar] [CrossRef] [PubMed]
- Brautbar, N.; Baczynski, R.; Carpenter, C.; Massry, S.G. Effects of phosphate depletion on the myocardium. Adv. Exp. Med. Biol. 1982, 151, 199–207. [Google Scholar]
- Vifor Pharma UK Ltd. Ferinject (ferric carboxymaltose) summary of product characteristics. 20 October 2020. Available online: https://www.medicines.org.uk/emc/product/5910/smpc#gref (accessed on 4 November 2020).
- Kalra, P.A.; Bhandari, S.; Saxena, S.; Agarwal, D.; Wirtz, G.; Kletzmayr, J.; Thomsen, L.L.; Coyne, D.W. A randomized trial of iron isomaltoside 1000 versus oral iron in non-dialysis-dependent chronic kidney disease patients with anaemia. Nephrol. Dial. Transplant. 2016, 31, 646–655. [Google Scholar] [CrossRef] [Green Version]
- Muras-Szwedziak, K.; Nowicki, M. Associations Between Intravenous Iron, Inflammation and FGF23 in Non-Dialysis Patients with Chronic Kidney Disease Stages 3–5. Kidney Blood Press. Res. 2018, 43, 143–151. [Google Scholar] [CrossRef]
- Hardy, S.; Vandemergel, X. Intravenous iron administration and hypophosphatemia in clinical practice. Int. J. Rheumatol. 2015, 2015, 468675. [Google Scholar] [CrossRef] [Green Version]
- Edmonston, D.; Wolf, M. FGF23 at the crossroads of phosphate, iron economy and erythropoiesis. Nat. Rev. Nephrol. 2020, 16, 7–19. [Google Scholar] [CrossRef]
- Wolf, M.; White, K.E. Coupling fibroblast growth factor 23 production and cleavage: Iron deficiency, rickets, and kidney disease. Curr. Opin. Nephrol. Hypertens. 2014, 23, 411–419. [Google Scholar] [CrossRef]
- Megapanou, E.; Florentin, M.; Milionis, H.; Elisaf, M.; Liamis, G. Drug-Induced Hypophosphatemia: Current Insights. Drug Saf. 2019, 43, 197–210. [Google Scholar] [CrossRef]
- Schouten, B.J.; Hunt, P.J.; Livesey, J.H.; Frampton, C.M.; Soule, S.G. FGF23 elevation and hypophosphatemia after intravenous iron polymaltose: A prospective study. J. Clin. Endocrinol. Metab. 2009, 94, 2332–2337. [Google Scholar] [CrossRef] [Green Version]
- Wolf, M.; Koch, T.A.; Bregman, D.B. Effects of iron deficiency anemia and its treatment on fibroblast growth factor 23 and phosphate homeostasis in women. J. Bone Miner. Res. 2013, 28, 1793–1803. [Google Scholar] [CrossRef] [PubMed]
- Bishay, R.H.; Ganda, K.; Seibel, M.J. Long-term iron polymaltose infusions associated with hypophosphataemic osteomalacia: A report of two cases and review of the literature. Ther. Adv. Endocrinol. Metab. 2017, 8, 14–19. [Google Scholar] [CrossRef] [Green Version]
- Vifor Pharma Ltd. Data on File.
- Scott, L.J. Ferric Carboxymaltose: A Review in Iron Deficiency. Drugs 2018, 78, 479–493. [Google Scholar] [CrossRef]
- Keating, G.M. Ferric carboxymaltose: A review of its use in iron deficiency. Drugs 2015, 75, 101–127. [Google Scholar] [CrossRef]
- Rognoni, C.; Venturini, S.; Meregaglia, M.; Marmifero, M.; Tarricone, R. Efficacy and Safety of Ferric Carboxymaltose and Other Formulations in Iron-Deficient Patients: A Systematic Review and Network Meta-analysis of Randomised Controlled Trials. Clin. Drug Investig. 2016, 36, 177–194. [Google Scholar] [CrossRef] [Green Version]
- Aksan, A.; Isik, H.; Radeke, H.H.; Dignass, A.; Stein, J. Systematic review with network meta-analysis: Comparative efficacy and tolerability of different intravenous iron formulations for the treatment of iron deficiency anaemia in patients with inflammatory bowel disease. Aliment. Pharmacol. Ther. 2017, 45, 1303–1318. [Google Scholar] [CrossRef]
- Ehlken, B.; Nathell, L.; Gohlke, A.; Bocuk, D.; Toussi, M.; Wohlfeil, S. Evaluation of the Reported Rates of Severe Hypersensitivity Reactions Associated with Ferric Carboxymaltose and Iron (III) Isomaltoside 1000 in Europe Based on Data from EudraVigilance and VigiBase between 2014 and 2017. Drug Saf. 2019, 42, 463–471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nathell, L.; Gohlke, A.; Wohlfeil, S. Reported Severe Hypersensitivity Reactions after Intravenous Iron Administration in the European Economic Area (EEA) before and after Implementation of Risk Minimization Measures. Drug Saf. 2020, 43, 35–43. [Google Scholar] [CrossRef] [Green Version]
- Common Terminology Criteria for Adverse Events. Version 5.0: National Institute of Health, National Cancer Institute. 2017. Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/CTCAE_v5_Quick_Reference_5x7.pdf (accessed on 4 November 2020).
- Common Terminology Criteria for Adverse Events. Version 4.0: National Institute of Health, National Cancer Institute. 2009. Available online: https://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03/CTCAE_4.03_2010-06-14_QuickReference_8.5x11.pdf (accessed on 4 November 2020).
- Chand, S.; Ward, D.G.; Ng, Z.Y.; Hodson, J.; Kirby, H.; Steele, P.; Rooplal, I.; Bantugon, F.; Iqbal, T.; Tselepis, C.; et al. Serum hepcidin-25 and response to intravenous iron in patients with non-dialysis chronic kidney disease. J. Nephrol. 2015, 28, 81–88. [Google Scholar] [CrossRef]
- Ikuta, K.; Hanashi, H.; Hirai, K.; Ota, Y.; Matsuyama, Y.; Shimura, A.; Terauchi, M.; Momoeda, M. Comparison of efficacy and safety between intravenous ferric carboxymaltose and saccharated ferric oxide in Japanese patients with iron-deficiency anemia due to hypermenorrhea: A multi-center, randomized, open-label noninferiority study. Int. J. Hematol. 2019, 109, 41–49. [Google Scholar] [CrossRef]
- Stohr, R.; Sandstede, L.; Heine, G.H.; Marx, N.; Brandenburg, V. High-Dose Ferric Carboxymaltose in Patients With HFrEF Induces Significant Hypophosphatemia. J. Am. Coll. Cardiol. 2018, 71, 2270–2271. [Google Scholar] [CrossRef]
- Bager, P.; Hvas, C.L.; Dahlerup, J.F. Drug-specific hypophosphatemia and hypersensitivity reactions following different intravenous iron infusions. Br. J. Clin. Pharmacol. 2017, 83, 1118–1125. [Google Scholar] [CrossRef] [Green Version]
- Wolf, M.; Rubin, J.; Achebe, M.; Econs, M.J.; Peacock, M.; Imel, E.A.; Thomsen, L.L.; Carpenter, T.O.; Weber, T.; Brandenburg, V.; et al. Effects of Iron Isomaltoside vs Ferric Carboxymaltose on Hypophosphatemia in Iron-Deficiency Anemia: Two Randomized Clinical Trials. JAMA 2020, 323, 432–443. [Google Scholar] [CrossRef]
- Detlie, T.E.; Lindstrom, J.C.; Jahnsen, M.E.; Finnes, E.; Zoller, H.; Moum, B.; Jahnsen, J. Incidence of hypophosphatemia in patients with inflammatory bowel disease treated with ferric carboxymaltose or iron isomaltoside. Aliment. Pharmacol. Ther. 2019, 50, 397–406. [Google Scholar] [CrossRef] [PubMed]
- Glaspy, J.A.; Lim-Watson, M.Z.; Libre, M.A.; Karkare, S.S.; Hadker, N.; Bajic-Lucas, A.; Strauss, W.E.; Dahl, N.V. Hypophosphatemia Associated with Intravenous Iron Therapies for Iron Deficiency Anemia: A Systematic Literature Review. Ther. Clin. Risk Manag. 2020, 16, 245–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaefer, B.; Glodny, B.; Zoller, H. Blood and Bone Loser. Gastroenterology 2017, 152, e5–e6. [Google Scholar] [CrossRef] [Green Version]
- Bartko, J.; Roschger, P.; Zandieh, S.; Brehm, A.; Zwerina, J.; Klaushofer, K. Hypophosphatemia, Severe Bone Pain, Gait Disturbance, and Fatigue Fractures after Iron Substitution in Inflammatory Bowel Disease: A Case Report. J. Bone Miner. Res. 2018, 33, 534–539. [Google Scholar] [CrossRef]
- Urbina, T.; Belkhir, R.; Rossi, G.; Carbonnel, F.; Pavy, S.; Collins, M.; Mariette, X.; Seror, R. Iron Supplementation-Induced Phosphaturic Osteomalacia: FGF23 is the Culprit. J. Bone Miner. Res. 2018, 33, 540–542. [Google Scholar] [CrossRef] [Green Version]
- Klein, K.; Asaad, S.; Econs, M.; Rubin, J.E. Severe FGF23-based hypophosphataemic osteomalacia due to ferric carboxymaltose administration. BMJ Case Rep. 2018, 2018. [Google Scholar] [CrossRef]
- Tournis, S.; Michopoulos, S.; Makris, K.; Terpos, E. Re: Hypophosphatemia, Severe Bone Pain, Gait Disturbance, and Fatigue Fractures After Iron Substitution in Inflammatory Bowel Disease: A Case Report. J. Bone Miner. Res. 2018, 33, 543–545. [Google Scholar] [CrossRef] [PubMed]
- Moore, K.L.; Kildahl-Andersen, O.; Kildahl-Andersen, R.; Tjonnfjord, G.E. Uncommon adverse effect of a common medication. Tidsskrift den Norske Legeforening 2013, 133, 165. [Google Scholar] [CrossRef] [Green Version]
- Fang, W.; McMahon, L.P.; Bloom, S.; Garg, M. Symptomatic severe hypophosphatemia after intravenous ferric carboxymaltose. JGH Open 2019, 3, 438–440. [Google Scholar] [CrossRef]
- Roman-Gimeno, S.; Ortez-Toro, J.J.; Peteiro-Miranda, C.M.; Sanz-Martin, B.; Urdaniz-Borque, R. Case report: A rare cause of severe hypophosphatemia. Ann. Endocrinol. 2020. [Google Scholar] [CrossRef]
- Goto, N.A.; Weststrate, A.C.G.; Oosterlaan, F.M.; Verhaar, M.C.; Willems, H.C.; Emmelot-Vonk, M.H.; Hamaker, M.E. The association between chronic kidney disease, falls, and fractures: A systematic review and meta-analysis. Osteoporos. Int. 2020, 31, 13–29. [Google Scholar] [CrossRef] [Green Version]
- Damasiewicz, M.J.; Nickolas, T.L. Rethinking Bone Disease in Kidney Disease. JBMR Plus 2018, 2, 309–322. [Google Scholar] [CrossRef]
- Zoller, H.; Schaefer, B.; Glodny, B. Iron-induced hypophosphatemia: An emerging complication. Curr. Opin. Nephrol. Hypertens. 2017, 26, 266–275. [Google Scholar] [CrossRef]
- Huang, L.L.; Lee, D.; Troster, S.M.; Kent, A.B.; Roberts, M.A.; Macdougall, I.C.; McMahon, L.P. A controlled study of the effects of ferric carboxymaltose on bone and haematinic biomarkers in chronic kidney disease and pregnancy. Nephrol. Dial. Transplant. 2018, 33, 1628–1635. [Google Scholar] [CrossRef] [Green Version]
- Wolf, M.; Chertow, G.M.; Macdougall, I.C.; Kaper, R.; Krop, J.; Strauss, W. Randomized trial of intravenous iron-induced hypophosphatemia. JCI Insight 2018, 3. [Google Scholar] [CrossRef] [Green Version]
- Garagarza, C.; Valente, A.; Caetano, C.; Oliveira, T.; Ponce, P.; Silva, A.P. Hypophosphatemia: Nutritional status, body composition, and mortality in hemodialysis patients. Int. Urol. Nephrol. 2017, 49, 1243–1250. [Google Scholar] [CrossRef] [PubMed]
- Shen, G.; Zhang, Y.; Hu, S.; Liu, B.; Kuang, A. Adult-onset hypophosphatemic osteomalacia associated with Sjogren syndrome: Clinical case report. Medicine 2017, 96, e6493. [Google Scholar] [CrossRef]
- Bernstein, C.N.; Leslie, W.D.; Leboff, M.S. AGA technical review on osteoporosis in gastrointestinal diseases. Gastroenterology 2003, 124, 795–841. [Google Scholar] [CrossRef]
- Jahnsen, J.; Falch, J.A.; Aadland, E.; Mowinckel, P. Bone mineral density is reduced in patients with Crohn’s disease but not in patients with ulcerative colitis: A population based study. Gut 1997, 40, 313–319. [Google Scholar] [CrossRef]
- Lamb, C.A.; Kennedy, N.A.; Raine, T.; Hendy, P.A.; Smith, P.J.; Limdi, J.K.; Hayee, B.; Lomer, M.C.E.; Parkes, G.C.; Selinger, C.; et al. British Society of Gastroenterology consensus guidelines on the management of inflammatory bowel disease in adults. Gut 2019, 68 (Suppl. 3), s1–s106. [Google Scholar] [CrossRef] [Green Version]
- Andrews, N.C. Disorders of iron metabolism. N. Engl. J. Med. 1999, 341, 1986–1995. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Intervention (n) | Mean Serum PO43− at Baseline Mean (SD) | Change from Baseline at Week 2 Mean (95% CI) | Change from Baseline at Week 4 Mean (95% CI) |
|---|---|---|---|
| FCM (6879) | 3.90 (0.88) | −1.24 (−1.27–−1.21) | −0.71 (−0.74–−0.69) |
| Other IV iron (1844) | 3.97 (0.81) | −0.28 (−0.31–−0.24) | −0.22 (−0.26–−0.18) |
| Oral iron (1354) | 3.86 (0.67) | 0.06 (0.01–0.10) | 0.03 (−0.05–0.07) |
| Placebo (575) | 3.61 (0.61) | 0.03 (−0.15–0.21) | 0.04 (−0.05–0.14) |
| Standard medical care (2041) | 3.93 (0.79) | −0.02 (−0.08–0.05) | −0.05 (−0.08–−0.01) |
| Baseline | <1 mg/dL | 1–<2 mg/dL | 2–<2.5 mg/dL | 2.5–<4.5 mg/dL | ≥4.5 mg/dL | Missing Values | Total |
|---|---|---|---|---|---|---|---|
| Total | 0 | 7 | 33 | 1826 | 493 | 12 | 2371/2371 (100%) |
| <1 mg/dL | 0 | 0 | 2 | 0 | 0 | 0 | 2/2371 (0.1%) |
| 1–<2 mg/dL | 0 | 3 | 6 | 67 | 2 | 2 | 80/2371 (3.4%) |
| 2–<2.5 mg/dL | 0 | 2 | 11 | 157 | 6 | 1 | 177/2371 (7.5%) |
| 2.5–<4.5 mg/dL | 0 | 1 | 14 | 1454 | 249 | 9 | 1727/2371 (72.8%) |
| ≥4.5 mg/dL | 0 | 1 | 0 | 148 | 236 | 0 | 385/2371 (16.2%) |
| Odds Ratio (95% CI) | p-Value | |
|---|---|---|
| Moderate HP (1–<2.5 mg/dL) | ||
| Therapeutic area: neurology vs. women’s health | 10.274 (0.831–126.95) | <0.0001 |
| Therapeutic area: gastroenterology vs. women’s health | 2.728 (2.199–3.385) | <0.0001 |
| Therapeutic area: other vs. women’s health | 2.424 (1.925–3.052 | <0.0001 |
| Iron parameters: baseline ferritin (10 µg/L increase) | 0.922 (0.904–0.940) | <0.0001 |
| Dosing scheme: FCM multiple dose vs. FCM single dose | 2.453 (1.615–3.727) | <0.0001 |
| Dosing scheme: FCM cumulative dose >1000–≤1500 mg vs. ≤1000 mg | 1.972 (1.311–2.968) | 0.0007 |
| Dosing scheme: FCM cumulative dose >1500 mg vs. ≤1000 mg | 2.248 (1.483–3.407) | 0.0007 |
| Dosing scheme: FCM maximum single dose >500–≤750 mg vs. ≤500 mg | 2.279 (1.688–3.077) | <0.0001 |
| Dosing scheme: FCM maximum single dose >750 mg vs. ≤500 mg | 1.920 (1.429–2.578) | <0.0001 |
| Intrinsic factors: BMI class (overweight vs. normal) | 0.860 (0.724–1.023) | <0.0001 |
| Intrinsic factors: BMI class (obese vs. normal) | 0.559 (0.472–0.663) | <0.0001 |
| Intrinsic factors: race (Black or African American vs. White) | 2.719 (2.291–3.227) | <0.0001 |
| Intrinsic factors: age <18 years vs. 18–<65 years | 0.075 (0.010–0.555) | 0.0017 |
| Intrinsic factors: age 65–<75 years vs. 18–<65 years | 1.079 (0.845–1.379) | 0.0017 |
| Intrinsic factors: age ≥75 years vs. 18–<65 years | 1.424 (1.121–1.810) | 0.0017 |
| Severe HP (<1 mg/dL) | ||
| Therapeutic area: gastroenterology vs. women’s health | 4.601 (2.093–10.111) | <0.0001 |
| Therapeutic area: cardiology vs. women’s health | 0.259 (0.030–2.228) | <0.0001 |
| Therapeutic area: nephrology vs. women’s health | 0.162 (0.032–0.820) | <0.0001 |
| Iron parameters: baseline ferritin (10 µg/L increase) | 0.871 (0.742–1.024) | 0.0949 |
| Dosing scheme: FCM cumulative dose >1000 mg–≤1500 mg vs. ≤1000 mg | 5.867 (2.514–13.694) | 0.0002 |
| Dosing scheme: FCM cumulative dose >1500 mg vs. ≤1000 mg | 4.093 (1.499–11.180) | 0.0002 |
| Intrinsic factors: sex | 0.512 (0.249–1.052) | 0.0684 |
| Cases with Potential Signs and Symptoms of HP | FCM (n = 8245) n (%) | Other IV Iron (n = 1998) n (%) | Oral Iron (n = 1621) n (%) | Placebo (n = 616) n (%) | Standard Medical Care (n = 2600) n (%) |
|---|---|---|---|---|---|
| All | 726 (8.8) | 249 (12.5) | 140 (8.6) | 86 (14.0) | 109 (4.2) |
| Treatment related | 125 (1.5) | 36 (1.8) | 5 (0.3) | 5 (0.8) | 19 (0.7) |
| Severe | 132 (1.6) | 81 (4.1) | 25 (1.5) | 19 (3.1) | 15 (0.6) |
| Treatment related | 6 (<0.1) | 3 (0.2) | 0 | 0 | 1 (<0.1) |
| Serious | 130 (1.6) | 69 (3.5) | 32 (2.0) | 43 (7.0) | 17 (0.7) |
| Treatment related | 1 (<0.1) | 0 | 0 | 1 (0.2) | 0 |
| Leading to withdrawal | 23 (0.3) | 4 (0.2) | 8 (0.5) | 10 (1.6) | 3 (0.1) |
| Treatment related | 8 (<0.1) | 1 (<0.1) | 1 (<0.1) | 0 | 2 (<0.1) |
| Resulting in death | 14 (0.2) | 6 (0.3) | 2 (0.1) | 9 (1.5) | 2 (<0.1) |
| Treatment related | 0 | 0 | 0 | 0 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rosano, G.; Schiefke, I.; Göhring, U.-M.; Fabien, V.; Bonassi, S.; Stein, J. A Pooled Analysis of Serum Phosphate Measurements and Potential Hypophosphataemia Events in 45 Interventional Trials with Ferric Carboxymaltose. J. Clin. Med. 2020, 9, 3587. https://doi.org/10.3390/jcm9113587
Rosano G, Schiefke I, Göhring U-M, Fabien V, Bonassi S, Stein J. A Pooled Analysis of Serum Phosphate Measurements and Potential Hypophosphataemia Events in 45 Interventional Trials with Ferric Carboxymaltose. Journal of Clinical Medicine. 2020; 9(11):3587. https://doi.org/10.3390/jcm9113587
Chicago/Turabian StyleRosano, Giuseppe, Ingolf Schiefke, Udo-Michael Göhring, Vincent Fabien, Stefano Bonassi, and Jürgen Stein. 2020. "A Pooled Analysis of Serum Phosphate Measurements and Potential Hypophosphataemia Events in 45 Interventional Trials with Ferric Carboxymaltose" Journal of Clinical Medicine 9, no. 11: 3587. https://doi.org/10.3390/jcm9113587