Comparison of the Meibomian Gland Openings by Optical Coherence Tomography in Obstructive Meibomian Gland Dysfunction and Normal Patients

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Meibography
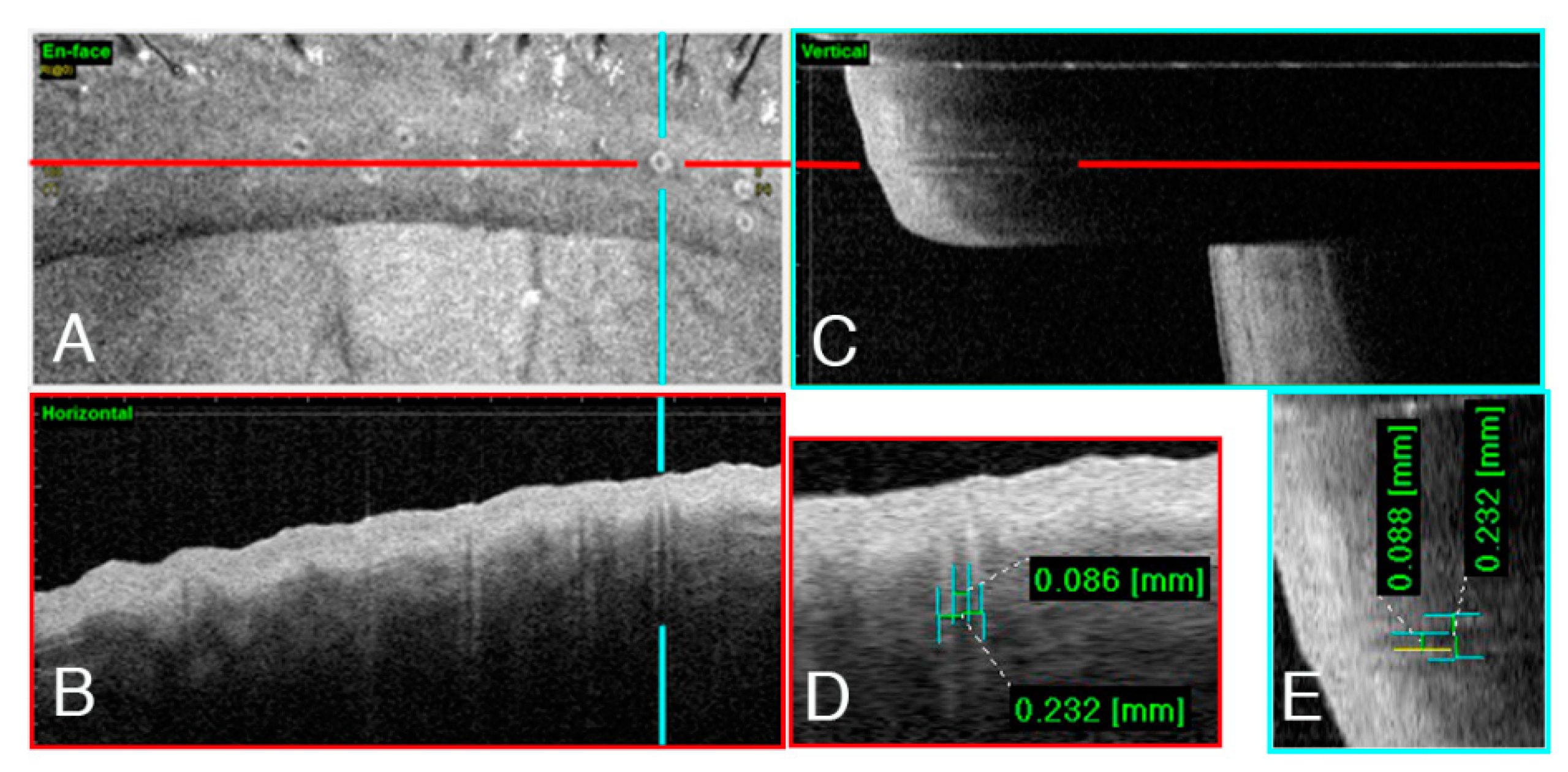
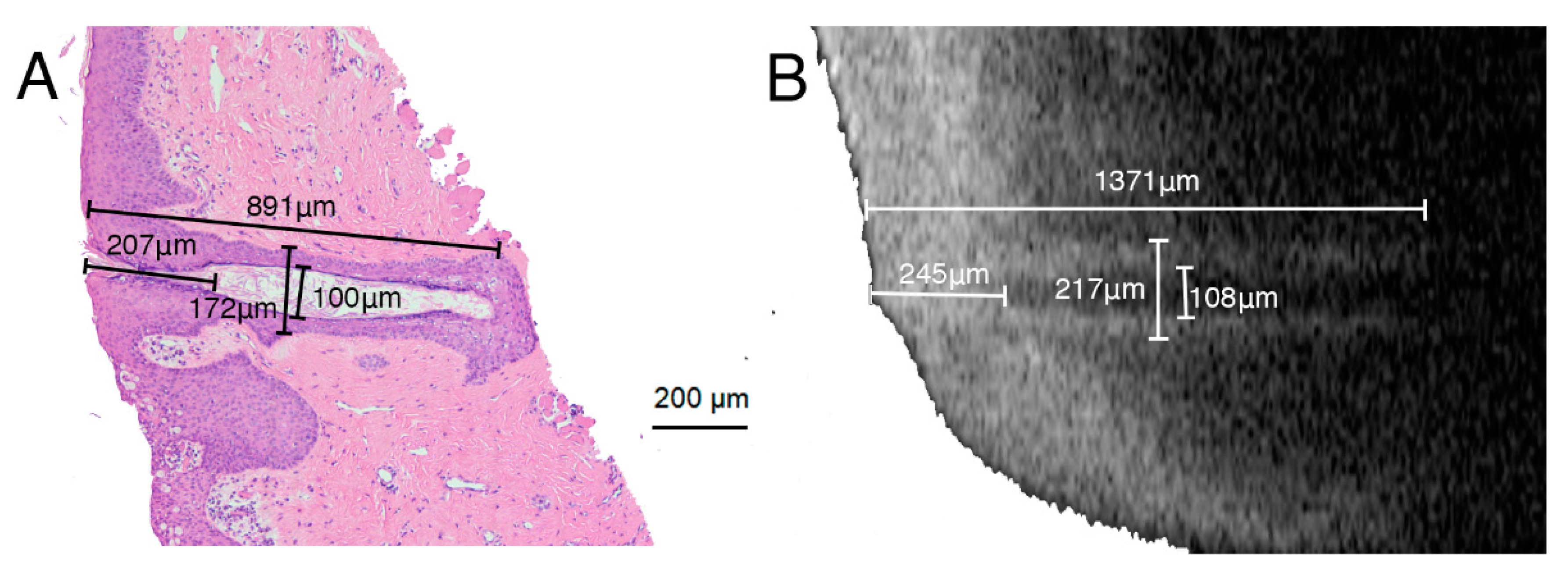
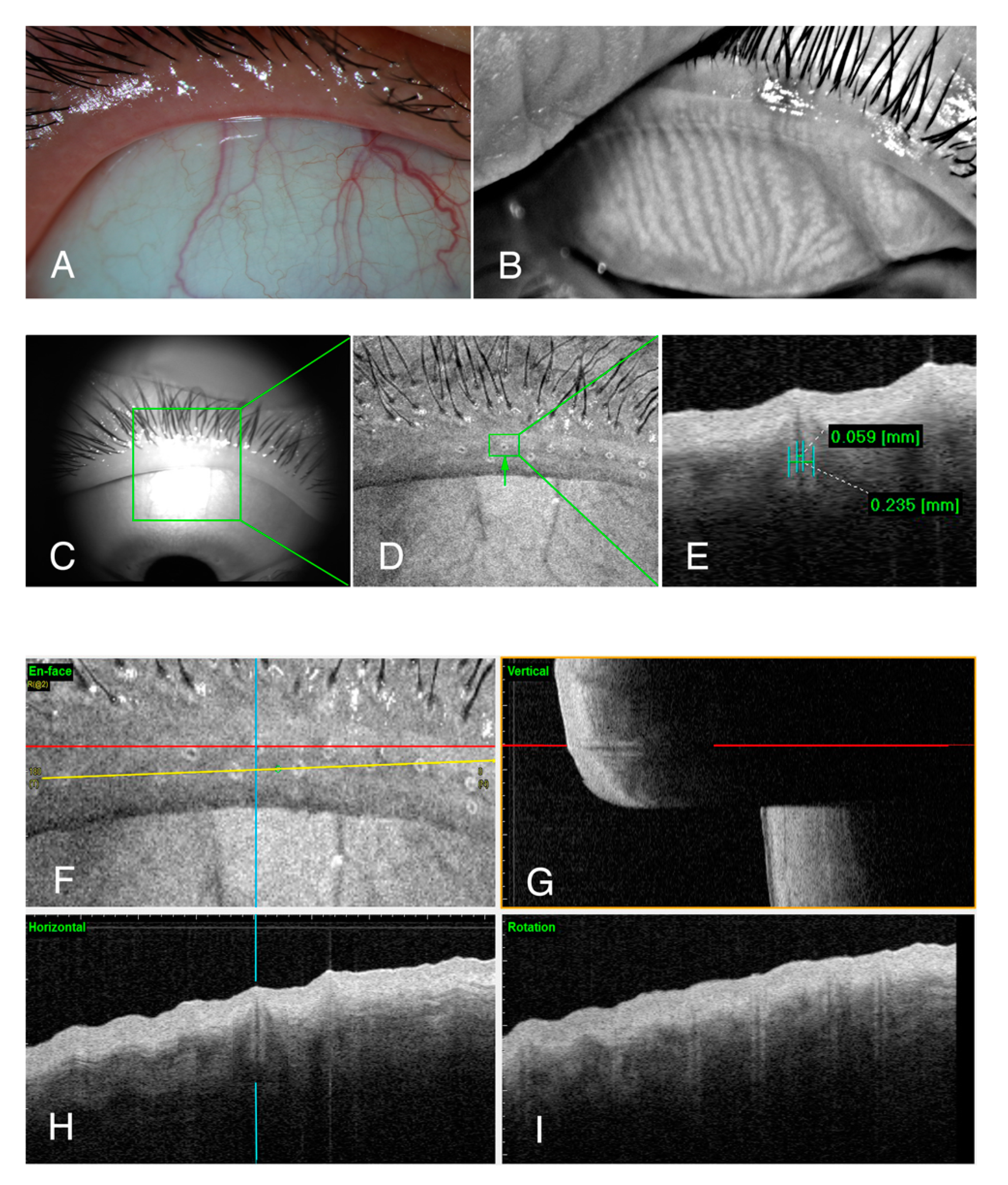
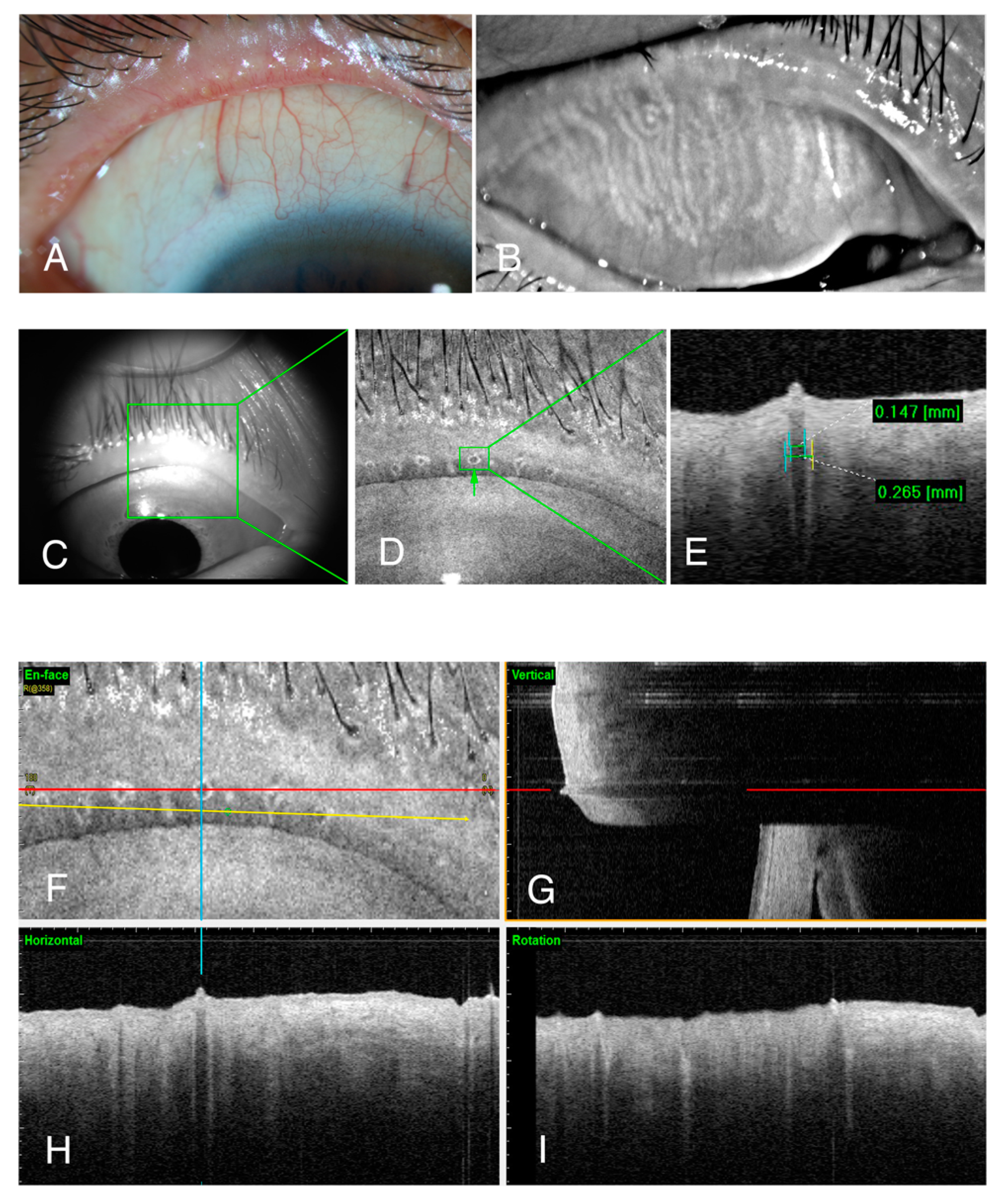
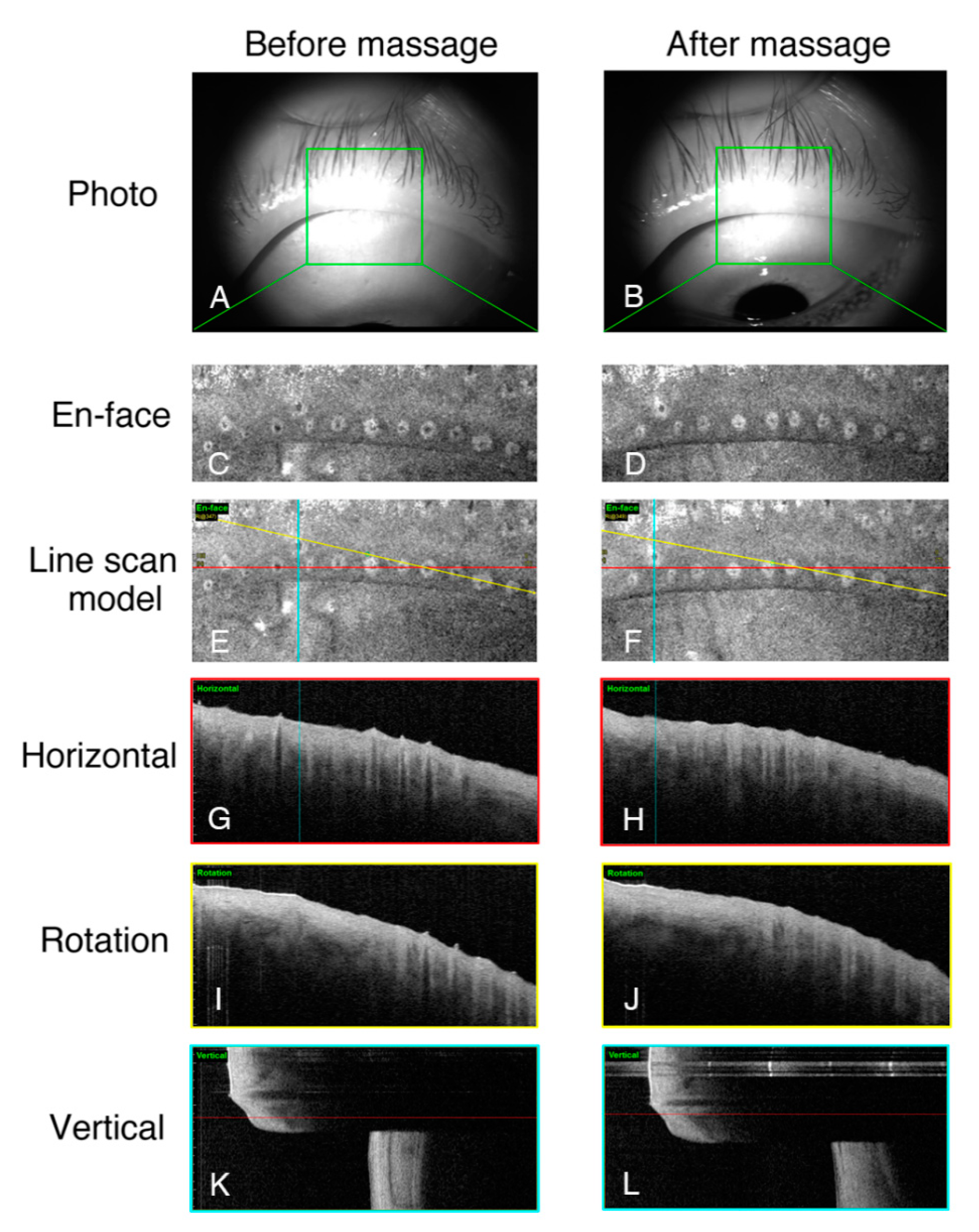
2.3. Swept-Source Anterior Segment Optical Coherence Tomography
2.4. Meibomian Gland Compress
2.5. Statistical Analysis
3. Results
3.1. Morphology of the Meibomian Gland Openings
3.2. Comparison of Meibomian Gland Openings in Patients with MGD and Normal Subjects
3.3. Changes in Meibomian Gland Openings in Patients with MGD before and after Massage
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Declarations
Abbreviations
| OCT | optical coherence tomography |
| MGD | meibomian gland dysfunction |
| TBUT | tear film break-up time |
| IVCM | in vivo laser scanning confocal microscopy |
| BCVA | best-corrected visual acuity |
| OSDI | ocular surface disease index |
References
- Chhadva, P.; Goldhardt, R.; Galor, A. Meibomian Gland Disease: The Role of Gland Dysfunction in Dry Eye Disease. Ophthalmology 2017, 124, S20–S26. [Google Scholar] [CrossRef] [PubMed]
- Nichols, K.K.; Foulks, G.N.; Bron, A.J.; Glasgow, B.J.; Dogru, M.; Tsubota, K.; Lemp, M.A.; Sullivan, D.A. The international workshop on meibomian gland dysfunction: Executive summary. Investig. Ophthalmol. Vis. Sci. 2011, 52, 1922–1929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nelson, J.D.; Shimazaki, J.; Benitez-del-Castillo, J.M.; Craig, J.P.; McCulley, J.P.; Den, S.; Foulks, G.N. The international workshop on meibomian gland dysfunction: Report of the definition and classification subcommittee. Investig. Ophthalmol. Vis. Sci. 2011, 52, 1930–1937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knop, E.; Knop, N.; Millar, T.; Obata, H.; Sullivan, D.A. The international workshop on meibomian gland dysfunction: Report of the subcommittee on anatomy, physiology, and pathophysiology of the meibomian gland. Investig. Ophthalmol. Vis. Sci. 2011, 52, 1938–1978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gilbard, J.P.; Rossi, S.R.; Heyda, K.G. Tear film and ocular surface changes after closure of the meibomian gland orifices in the rabbit. Ophthalmology 1989, 96, 1180–1186. [Google Scholar] [CrossRef]
- Cox, S.M.; Berntsen, D.A.; Chatterjee, N.; Hickson-Curran, S.B.; Jones, L.W.; Moezzi, A.M.; Morgan, P.B.; Nichols, J.J. Eyelid Margin and Meibomian Gland Characteristics and Symptoms in Lens Wearers. Optom. Vis. Sci. 2016, 93, 901–908. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arita, R.; Itoh, K.; Inoue, K.; Amano, S. Noncontact infrared meibography to document age-related changes of the meibomian glands in a normal population. Ophthalmolgy 2008, 115, 911–915. [Google Scholar] [CrossRef] [PubMed]
- Villani, E.; Canton, V.; Magnani, F.; Viola, F.; Nucci, P.; Ratiglia, R. The aging Meibomian gland: An in vivo confocal study. Investig. Ophthalmol. Vis. Sci. 2013, 54, 4735–4740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villani, E.; Ceresara, G.; Beretta, S.; Magnani, F.; Viola, F.; Ratiglia, R. In vivo confocal microscopy of meibomian glands in contact lens wearers. Investig. Ophthalmol. Vis. Sci. 2011, 52, 5215–5219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, S.; Robertson, D.M. Wide-Field In Vivo Confocal Microscopy of Meibomian Gland Acini and Rete Ridges in the Eyelid Margin. Investig. Ophthalmol. Vis. Sci. 2018, 59, 4249–4257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsubota, K.; Yokoi, N.; Shimazaki, J.; Watanabe, H.; Dogru, M.; Yamada, M.; Kinoshita, S.; Kim, H.M.; Tchah, H.W.; Hyon, J.Y.; et al. New Perspectives on Dry Eye Definition and Diagnosis: A Consensus Report by the Asia Dry Eye Society. Ocul. Surf. 2017, 15, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Liang, Q.; Pan, Z.; Zhou, M.; Zhang, Y.; Wang, N.; Li, B.; Baudouin, C.; Labbe, A. Evaluation of Optical Coherence Tomography Meibography in Patients with Obstructive Meibomian Gland Dysfunction. Cornea 2015, 34, 1193–1199. [Google Scholar] [CrossRef]
- Abdelfattah, N.S.; Dastiridou, A.; Sadda, S.R.; Lee, O.L. Noninvasive Imaging of Tear Film Dynamics in Eyes with Ocular Surface Disease. Cornea 2015, 34 (Suppl. 10), S48–S52. [Google Scholar] [CrossRef]
- Arita, R.; Fukuoka, S.; Morishige, N. New insights into the morphology and function of meibomian glands. Exp. Eye Res. 2017, 163, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Tomlinson, A.; Bron, A.J.; Korb, D.R.; Amano, S.; Paugh, J.R.; Pearce, E.I.; Yee, R.; Yokoi, N.; Arita, R.; Dogru, M. The international workshop on meibomian gland dysfunction: Report of the diagnosis subcommittee. Investig. Ophthalmol. Vis. Sci. 2011, 52, 2006–2049. [Google Scholar] [CrossRef] [PubMed]
- Bron, A.J.; Benjamin, L.; Snibson, G.R. Meibomian gland disease. Classification and grading of lid changes. Eye 1991, 5 Pt 4, 395–411. [Google Scholar] [CrossRef]
- Jester, J.V.; Nicolaides, N.; Smith, R.E. Meibomian gland studies: Histologic and ultrastructural investigations. Investig. Ophthalmol. Vis. Sci. 1981, 20, 537–547. [Google Scholar]
- Foulks, G.N.; Bron, A.J. Meibomian gland dysfunction: A clinical scheme for description, diagnosis, classification, and grading. Ocul. Surf. 2003, 1, 107–126. [Google Scholar] [CrossRef]
- Eom, Y.; Han, J.Y.; Kang, B.; Hwang, H.S.; Lee, H.K.; Kim, H.M.; Song, J.S. Meibomian Glands and Ocular Surface Changes after Closure of Meibomian Gland Orifices in Rabbits. Cornea 2018, 37, 218–226. [Google Scholar] [CrossRef] [PubMed]
- Nakayama, N.; Kawashima, M.; Kaido, M.; Arita, R.; Tsubota, K. Analysis of Meibum before and after Intraductal Meibomian Gland Probing in Eyes with Obstructive Meibomian Gland Dysfunction. Cornea 2015, 34, 1206–1208. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Control Group (n = 54) | MGD Group (n = 49) | t-Value | p-Value |
|---|---|---|---|---|
| Age (years) | 46.35 ± 14.4 | 51.16 ± 12.97 | −1.775 | 0.079 |
| Sex | 20 M/34 F | 13 M/36 F | −1.142 | 0.256 |
| Orifices 1 | 9.74 ± 2.36 | 9.24 ± 2.30 | 1.080 | 0.283 |
| Mean 2 (μm) | 100.96 ± 20.30 | 120.22 ± 27.92 | −4.031 | <0.001 * |
| Max 3 (μm) | 157.89 ± 4.03 | 224.17 ± 94.47 | −4.420 | <0.001 * |
| Min 4 (μm) | 59.82 ± 21.26 | 64.90 ± 18.94 | −1.274 | 0.206 |
| Var 5 (μm) | 33.03 ± 15.81 | 51.70 ± 3.51 | −4.252 | <0.001 * |
| Variable | Before Massage | After Massage | t-Value | p-Value |
|---|---|---|---|---|
| Orifices 1 | 9.98 ± 2.74 | 10.54 ± 2.42 | −2.527 | 0.018 * |
| Mean 2 (μm) | 133.73 ± 27.81 | 102.26 ± 24.30 | 6.297 | 0.000 * |
| Max 3 (μm) | 271.02 ± 114.78 | 193.50 ± 70.24 | 4.098 | 0.000 * |
| Min 4 (μm) | 62.77 ± 22.55 | 53.81 ± 19.26 | 1.737 | 0.095 |
| Var 5 (μm) | 69.43 ± 38.91 | 45.20 ± 21.18 | 3.596 | 0.001 * |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cui, X.; Wu, Q.; Zhai, Z.; Yang, Y.; Wei, A.; Xu, J.; Hong, J. Comparison of the Meibomian Gland Openings by Optical Coherence Tomography in Obstructive Meibomian Gland Dysfunction and Normal Patients. J. Clin. Med. 2020, 9, 3181. https://doi.org/10.3390/jcm9103181
Cui X, Wu Q, Zhai Z, Yang Y, Wei A, Xu J, Hong J. Comparison of the Meibomian Gland Openings by Optical Coherence Tomography in Obstructive Meibomian Gland Dysfunction and Normal Patients. Journal of Clinical Medicine. 2020; 9(10):3181. https://doi.org/10.3390/jcm9103181
Chicago/Turabian StyleCui, Xinhan, Qingfan Wu, Zimeng Zhai, Yujing Yang, Anji Wei, Jianjiang Xu, and Jiaxu Hong. 2020. "Comparison of the Meibomian Gland Openings by Optical Coherence Tomography in Obstructive Meibomian Gland Dysfunction and Normal Patients" Journal of Clinical Medicine 9, no. 10: 3181. https://doi.org/10.3390/jcm9103181