Timing of Osteoporotic Vertebral Fractures in Lung and Heart Transplantation: A Longitudinal Study

 , ,
, ,
Abstract
:1. Introduction
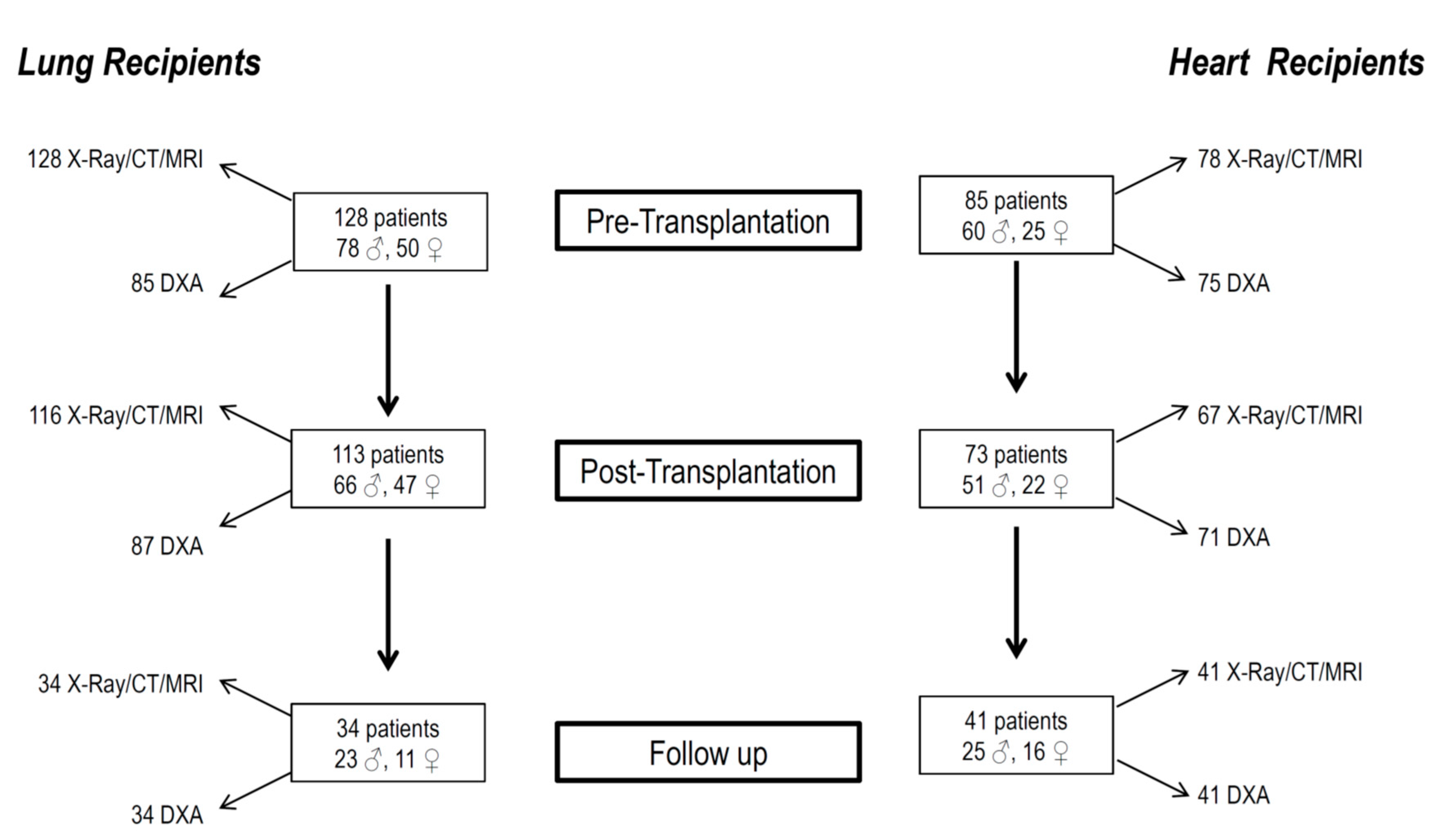
- To evaluate the prevalence of osteoporosis and fragility fractures in a population of adults before and after receiving a heart or lung transplant.
- To elucidate any factors which may influence fractures in heart or lung transplantation subjects.
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Maalouf, N.M.; Shane, E. Osteoporosis after solid organ transplantation. J. Clin. Endocrinol. Metab. 2005, 90, 2456–2465. [Google Scholar] [CrossRef]
- Early, C.; Stuckey, L.; Tischer, S. Osteoporosis in the adult solid organ transplant population: Underlying mechanisms and available treatment options. Osteoporos. Int. 2016, 27, 1425–1440. [Google Scholar] [CrossRef]
- Stein, E.M.; Ortiz, D.; Jin, Z.; McMahon, D.J.; Shane, E. Prevention of fractures after solid organ transplantation: A meta-analysis. J. Clin. Endocrinol. Metab. 2011, 96, 3457–3465. [Google Scholar] [CrossRef] [Green Version]
- Shane, E.; Silverberg, S.J.; Donovan, D.; Papadopoulos, M.D.A.; Staron, M.D.R.B.; Addesso, V.; Jorgesen, R.N.B.; McGregor, M.D.C.; Schulman, M.D.L. Osteoporosis in lung transplantation candidates with end-stage pulmonary disease. Am. J. Med. 1996, 101, 262–269. [Google Scholar] [CrossRef]
- Nuti, R.; Brandi, M.L.; Checchia, G.; di Munno, O.; Dominguez, L.; Falaschi, P.; Fiore, C.E.; Iolascon, G.; Maggi, S.; Michieli, R.; et al. Guidelines for the management of osteoporosis and fragility fractures. Intern. Emerg. Med. 2019, 14, 85–102. [Google Scholar] [CrossRef] [Green Version]
- Shane, E.; Mancini, D.; Aaronson, K.; Silverberg, S.J.; Seibel, M.J.; Addesso, V.; McMahon, D.J. Bone mass, vitamin D deficiency, and hyperparathyroidism in congestive heart failure. Am. J. Med. 1997, 103, 197–207. [Google Scholar] [CrossRef]
- Adachi, J.D.; Ioannidis, G.; Olszynski, W.P.; Brown, J.P.; Hanley, D.A.; Sebaldt, R.J.; Petrie, A.; Tenenhouse, A.; Stephenson, G.F.; Papaioannou, A.; et al. The impact of incident vertebral and nonvertebral fractures on health related quality of life in postmenopausal women. BMC Musculoskelet Disord. 2002, 3, 11. [Google Scholar] [CrossRef]
- Krege, J.H.; Kendler, D.; Krohn, K.; Genant, H.; Alam, J.; Berclaz, P.-Y.; Coffey, B.; Loghin, C. Relationship between Vertebral Fracture Burden, Height Loss, and Pulmonary Function in Postmenopausal Women with Osteoporosis. J. Clin. Densitom. 2015, 18, 506–511. [Google Scholar] [CrossRef] [Green Version]
- Cohen, A.; Sambrook, P.; Shane, E. Management of bone loss after organ transplantation. J. Bone Miner. Res. 2004, 19, 1919–1932. [Google Scholar] [CrossRef]
- Cohen, A.; Shane, E. Osteoporosis after solid organ and bone marrow transplantation. Osteoporos. Int. 2003, 14, 617–630. [Google Scholar] [CrossRef]
- Lan, G.B.; Xie, X.B.; Peng, L.K.; Liu, L.; Song, L.; Dai, H.L. Current Status of Research on Osteoporosis after Solid Organ Transplantation: Pathogenesis and Management. Biomed Res. Int. 2015, 2015, 413169. [Google Scholar] [CrossRef] [Green Version]
- Genant, H.K.; Wu, C.Y.; van Kuijk, C.; Nevitt, M.C. Vertebral fracture assessment using a semiquantitative technique. J. Bone Min. Res. 1993, 8, 1137–1148. [Google Scholar] [CrossRef]
- Yu, T.M.; Lin, C.L.; Chang, S.N.; Sung, F.C.; Huang, S.T.; Kao, C.H. Osteoporosis and fractures after solid organ transplantation: A nationwide population-based cohort study. Mayo Clin. Proc. 2014, 89, 888–895. [Google Scholar] [CrossRef]
- Ebeling, P.R. Transplantation osteoporosis. In Primer on the Metabolic Bone Diseases and Disorders of Mineral Metabolism, American Society for Bone and Mineral Research; Rosen, C., Ed.; Wiley-Blackwell: Hoboken, NJ, USA, 2013; pp. 495–507. [Google Scholar]
- Wang, T.K.; O′Sullivan, S.; Gamble, G.D.; Ruygrok, P.N. Bone density in heart or lung transplant recipients-A longitudinal study. Transpl. Proc. 2013, 45, 2357–2365. [Google Scholar] [CrossRef]
- Kulak, C.A.; Borba, V.Z.; Kulak Júnior, J.; Custódio, M.R. Bone disease after transplantation: Osteoporosis and fractures risk. Arq. Bras. Endocrinol. Metab. 2014, 58, 484–492. [Google Scholar] [CrossRef] [Green Version]
- Hariman, A.; Alex, C.; Heroux, A.; Camacho, P. Incidence of fractures after cardiac and lung transplantation: A single center experience. J. Osteoporos. 2014, 2014, 573041. [Google Scholar] [CrossRef]
- Anastasilakis, A.D.; Tsourdi, E.; Makras, P.; Polyzos, S.A.; Meier, C.; McCloskey, E.V.; Pepe, J.; Zillikens, M.C. Bone disease following solid organ transplantation: A narrative review and recommendations for management from The European Calcified Tissue Society. Bone 2019, 127, 401–418. [Google Scholar] [CrossRef]
- Lakey, W.C.; Spratt, S.; Vinson, E.N.; Gesty-Palmer, D.; Weber, T.; Palmer, S. Osteoporosis in lung transplant candidates compared to matched healthy controls. Clin. Transpl. 2011, 25, 426–435. [Google Scholar] [CrossRef]
- Hardy, R.S.; Zhou, H.; Seibel, M.J.; Cooper, M.S. Glucocorticoids and Bone: Consequences of Endogenous and Exogenous Excess and Replacement Therapy. Endocr. Rev. 2018, 39, 519–548. [Google Scholar] [CrossRef] [Green Version]
- Vrieze, A.; de Greef, M.H.; Wijkstra, P.J.; Wempe, J.B. Low bone mineral density in COPD patients related to worse lung function, low weight and decreased fat-free mass. Osteoporos. Int. 2007, 18, 1197–1202. [Google Scholar] [CrossRef] [Green Version]
- Da Costa, T.M.R.L.; Costa, F.M.; Hoffman Jonasson, T.; Moreira, C.A.; Boguszewski, C.L.; Borges, J.L.C.; Borba, V.Z.C. Bone mineral density and vertebral fractures and their relationship with pulmonary dysfunction in patients with chronic obstructive pulmonary disease. Osteoporos. Int. 2018, 29, 2537–2543. [Google Scholar] [CrossRef]
- Graumam, R.Q.; Pinheiro, M.M.; Nery, L.E.; Castro, C.H.M. Increased rate of osteoporosis, low lean mass, and fragility fractures in COPD patients: Association with disease severity. Osteoporos. Int. 2018, 29, 1457–1468. [Google Scholar] [CrossRef]
- Ferrari, S.L.; Nicod, L.P.; Hamacher, J.; Spiliopoulos, A.; Slosman, D.O.; Rochat, T.; Bonjour, J.P.; Rizzoli, R. Osteoporosis in patients undergoing lung transplantation. Eur. Respir. J. 1996, 9, 2378–2382. [Google Scholar] [CrossRef] [Green Version]
- Shane, E.; Papadopoulos, A.; Staron, R.B.; Addesso, V.; Donovan, D.; McGregor, C.; Schulman, L.L. Bone loss and fracture after lung transplantation. Clin. Transplant. 1999, 68, 220–227. [Google Scholar] [CrossRef]
- Spira, A.; Gutierrez, C.; Chaparro, C.; Hutcheon, M.A.; Chan, C.K. Osteoporosis and lung transplantation: A prospective study. Chest 2000, 117, 476–481. [Google Scholar] [CrossRef] [Green Version]
- Cairoli, E.; Eller-Vainicher, C.; Morlacchi, L.C.; Tarsia, P.; Rossetti, V.; Pappalettera, M.; Arosio, M.; Chiodini, I.; Blasi, F. Bone involvement in young adults with cystic fibrosis awaiting lung transplantation for end-stage respiratory failure. Osteoporos. Int. 2019, 30, 1255–1263. [Google Scholar] [CrossRef]
- Van Cleemput, J.; Daenen, W.; Nijs, J.; Geusens, P.; Dequeker, J.; Vanhaecke, J. Timing and quantification of bone loss in cardiac transplant recipients. Transpl. Int. 1995, 8, 196–200. [Google Scholar] [CrossRef]
- Ebeling, P.R. Approach to the patient with transplantation-related bone loss. J. Clin. Endocrinol. Metab. 2009, 94, 1483–1490. [Google Scholar] [CrossRef] [Green Version]
- Shane, E.; Rivas, M.; Staron, R.B.; Silverberg, S.J.; Seibel, M.J.; Kuiper, J.; Mancini, D.; Addesso, V.; Michler, R.E.; Factor-Litvak, P. Fracture after cardiac transplantation: A prospective longitudinal study. J. Clin. Endocrinol. Metab. 1996, 81, 1740–1746. [Google Scholar]
- Kerschan-Schindl, K.; Ruzicka, M.; Mahr, S.; Paireder, M.; Krestan, C.; Gleiss, A.; Bieglmayer, C.; Fialka-Moser, V.; Pacher, R.; Grimm, M.; et al. Unexpected low incidence of vertebral fractures in heart transplant recipients: Analysis of bone turnover. Transpl. Int. 2008, 21, 255–262. [Google Scholar] [CrossRef]
- Leidig-Bruckner, G.; Hosch, S.; Dodidou, P.; Ritschel, D.; Conradt, C.; Klose, C.; Otto, G.; Lange, R.; Theilmann, L.; Zimmerman, R.; et al. Frequency and predictors of osteoporotic fractures after cardiac or liver transplantation: A follow-up study. Lancet 2001, 357, 342–347. [Google Scholar] [CrossRef]
- Hofle, G.; Saely, C.H.; Tautermann, G.; Aczel, S.; Holzmuller, H.; Drexel, H. Relationship between various measures of bone mineral density and vertebral fractures in cardiac transplant recipients. Swiss Med. Wkly. 2004, 134, 215–220. [Google Scholar] [PubMed]
- Pisani, B.; Mullen, G.M. Prevention of osteoporosis in cardiac transplant recipients. Curr. Opin. Cardiol. 2002, 17, 160–164. [Google Scholar] [CrossRef]
- Bowman, A.R.; Sass, D.A.; Dissanayake, I.R.; Ma, Y.F.; Liang, H.; Yuan, Z.; Jee, W.S.; Epstein, S. The role of testosterone in cyclosporine-induced osteopenia. J. Bone Min. Res. 1997, 12, 607–615. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Lung Recipients | Heart Recipients | ||||
|---|---|---|---|---|---|---|
| Pre-Transplantation (n = 128) | Post-Transplantation (n = 113) | Follow Up (n = 34) | Pre-Trapnsplantation (n = 85) | Post-Transplantation (n = 73) | Follow Up (n = 41) | |
| Age (y) | 50.7 ± 11.8 | 52.9 ± 11.7 | 55.2 ± 13.5 | 51.1 ± 10.4 | 53.9 ± 10.3 | 56.9 ± 10.5 |
| Weight (kg) | 69.8 ± 15.1 | 70.9 ± 15.4 | 69.4 ± 11.7 | 73.7 ± 10.1 | 74.9 ± 11.9 | 72.9 ± 11.3 |
| Height (cm) | 168.1 ± 7.8 ° | 165.9 ± 16.1 * | 167.7 ± 6.6 ^ | 172.8 ± 9.4 | 172.0 ± 8.1 | 169.3 ± 7.2 |
| BMI (kg/m2) | 24.7 ± 4.7 | 24.9 ± 4.4 | 24.6 ± 3.6 | 24.5 ± 2.9 | 25.4 ± 3.9 | 25.9 ± 3.9 |
| Calcium (mg/dL) | 9.2 ± 0.5 | 9.1 ± 0.6 | 9.3 ± 0.4 | 9.1 ± 0.7 | 9.4 ± 0.6 | 9.2 ± 0.5 |
| Phosphorus (mg/dL) | 3.5 ± 0.6 | 3.6 ± 0.7 | 3.4 ± 0.7 | 3.5 ± 0.6 | 3.3 ± 0.6 | 3.3 ± 0.5 |
| Creatinine (mg/dL) | 0.9 ± 0.2 °° | 1.3 ± 0.5 ** | 1.3 ± 0.5 §§ | 1.2 ± 0.3 | 1.3 ± 0.4 | 1.4 ± 0.5 |
| Alkaline phosphatase (UI/L) | 80.5 ± 48.3 | 72.8 ± 36.7 | 71.1 ± 29.6 | 90.5 ± 31.2 | 85.2 ± 39.1 | 73.2 ± 21.4 |
| 25OHD (ng/mL) | 19.1 ± 11.8 | 21.6 ± 9.9 | 21.2 ± 9.3 | 22.4 ± 14.7 | 19.9 ± 14.6 | 23.8 ± 13.6 |
| PTH (pg/mL) | 42.7. ± 14.7 | 56.0 ± 46.1 | 57.8 ± 24.3 | 46.2 ± 35.2 | 76.9 ± 29.5 | 71.8 ± 39.6 |
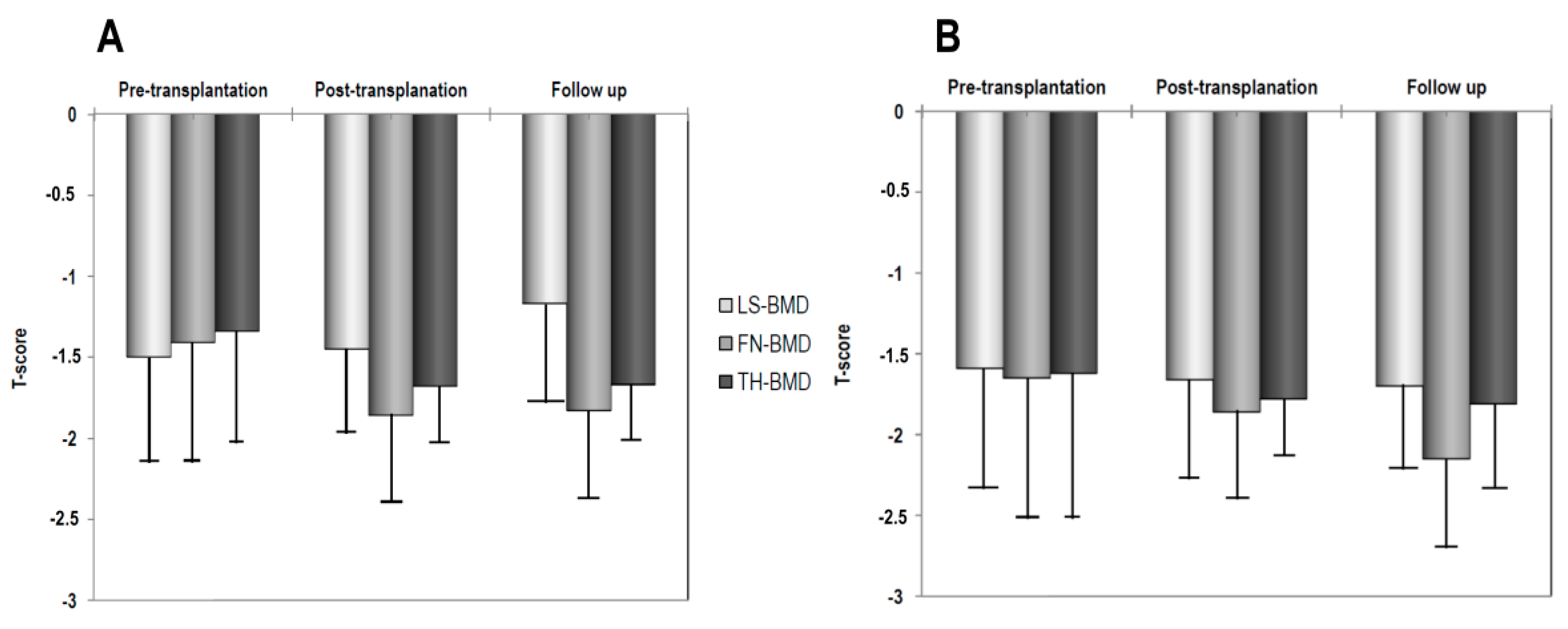
| LS-BMD (g/cm2) | 1.011 ± 0.182 | 1.000 ± 0.194 | 1.025 ± 0.177 §,^ | 0.988 ± 0.151 | 0.982 ± 0.155 | 0.964 ± 0.210 § ^ |
| FN-BMD (g/cm2) | 0.839 ± 0.167 | 0.765 ± 0.162 ** | 0.767 ± 0.121 § | 0.797 ± 0.140 | 0.779 ± 0.134 | 0.728 ± 0.135 ^ |
| TH-BMD (g/cm2) | 0.863 ± 0.172 | 0.818 ± 0.157 ** | 0.819 ± 0.138 § | 0.838 ± 0.112 | 0.811 ± 0.126 * | 0.798 ± 0.102 ^ |
| Variable | Undestandardized Coefficient, b | 95%CI | p |
|---|---|---|---|
| Lung | |||
| Vertebral fracture | |||
| Age | 0.018 | 0.006 to 0.029 | 0.003 |
| TH-BMD | −1.421 | −2.284 to −0.558 | 0.002 |
| History of fracture | 0.382 | 0.003 to 0.760 | 0.048 |
| Heart | |||
| Vertebral fracture | |||
| History of fracture | 0.867 | 0.510 to 1.224 | <0.01 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caffarelli, C.; Tomai Pitinca, M.D.; Alessandri, M.; Cameli, P.; Bargagli, E.; Bennett, D.; Fossi, A.; Bernazzali, S.; Gonnelli, S. Timing of Osteoporotic Vertebral Fractures in Lung and Heart Transplantation: A Longitudinal Study. J. Clin. Med. 2020, 9, 2941. https://doi.org/10.3390/jcm9092941
Caffarelli C, Tomai Pitinca MD, Alessandri M, Cameli P, Bargagli E, Bennett D, Fossi A, Bernazzali S, Gonnelli S. Timing of Osteoporotic Vertebral Fractures in Lung and Heart Transplantation: A Longitudinal Study. Journal of Clinical Medicine. 2020; 9(9):2941. https://doi.org/10.3390/jcm9092941
Chicago/Turabian StyleCaffarelli, Carla, Maria D. Tomai Pitinca, Mario Alessandri, Paolo Cameli, Elena Bargagli, David Bennett, Antonella Fossi, Sonia Bernazzali, and Stefano Gonnelli. 2020. "Timing of Osteoporotic Vertebral Fractures in Lung and Heart Transplantation: A Longitudinal Study" Journal of Clinical Medicine 9, no. 9: 2941. https://doi.org/10.3390/jcm9092941