Brain Stimulation in Eating Disorders: State of the Art and Future Perspectives

 ,
,  , , , ,
, , , ,  , and
, and
Abstract
:1. Introduction
2. Methods
3. Results
3.1. rTMS in Eating Disorders
3.1.1. Anorexia Nervosa
3.1.2. Bulimia Nervosa and Binge-Eating Disorder
3.1.3. rTMS and Site of Modulation
3.2. tDCS and Eating Disorders
3.3. ECT in Eating Disorders
3.3.1. Anorexia Nervosa
3.3.2. Bulimia Nervosa and Binge Eating Disorder
3.4. VNS in Eating Disorders
3.5. Deep Brain Stimulation in Eating Disorders
3.5.1. Deep Brain Stimulation in Anorexia Nervosa
3.5.2. Deep Brain Stimulation in Bulimia Nervosa and Binge Eating Disorder
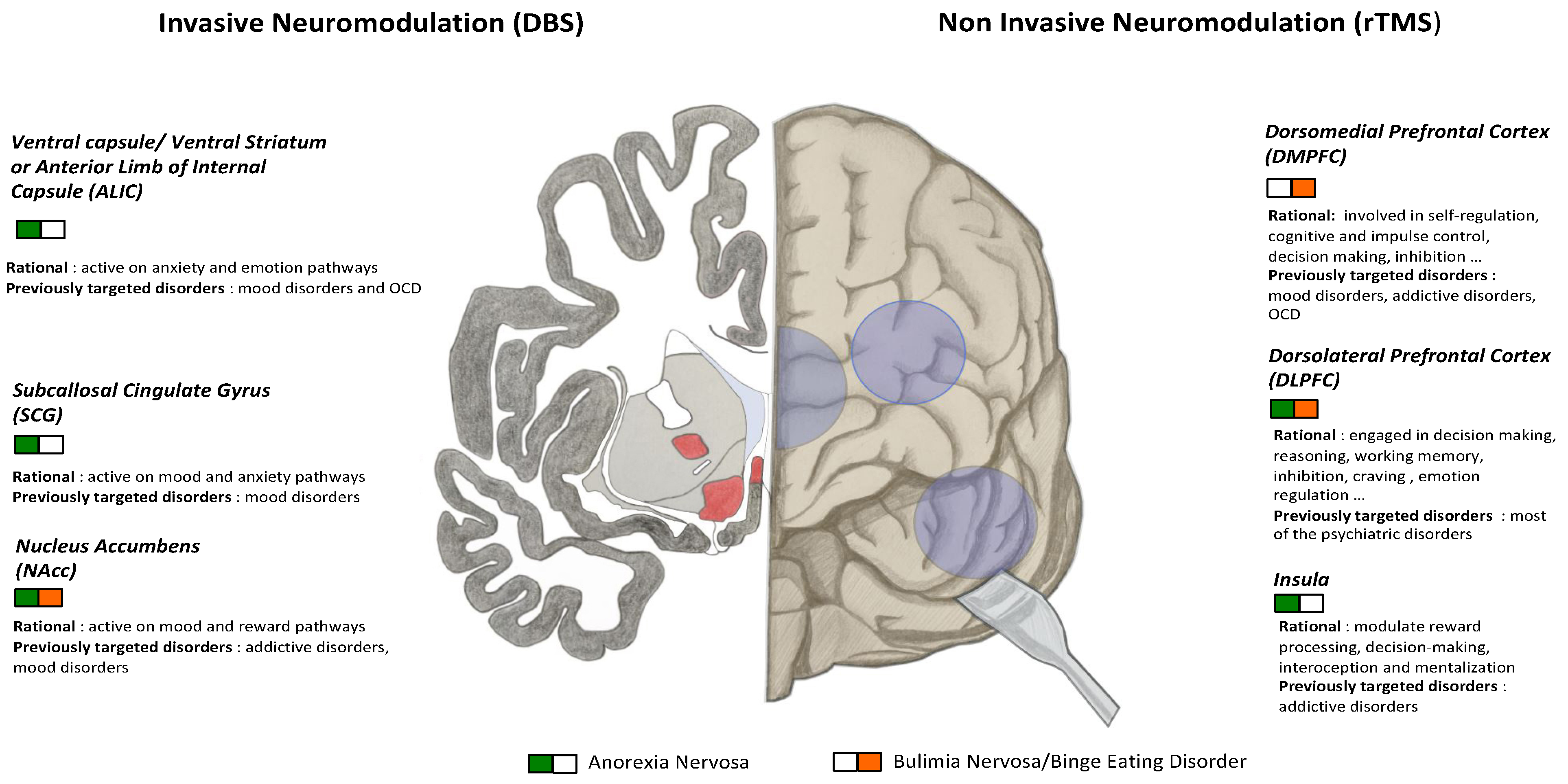
3.5.3. Neuroanatomical Targets in DBS
4. Discussion
4.1. Current Evidence and Issues
4.2. Perspectives
4.2.1. Improving Brain Stimulation Efficiency
4.2.2. Toward More Personalized Protocols
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Treasure, J.; Duarte, T.A.; Schmidt, U. Eating disorders. Lancet 2020, 395, 899–911. [Google Scholar] [CrossRef]
- Zabala, M.J.; Macdonald, P.; Treasure, J. Appraisal of caregiving burden, expressed emotion and psychological distress in families of people with eating disorders: A systematic review. Eur. Eat. Disord. Rev. Prof. J. Eat. Disord. Assoc. 2009, 17, 338–349. [Google Scholar] [CrossRef] [PubMed]
- Striegel-Moore, R.H.; DeBar, L.; Wilson, G.T.; Dickerson, J.; Rosselli, F.; Perrin, N.; Lynch, F.; Kraemer, H.C. Health services use in eating disorders. Psychol. Med. 2008, 38, 1465–1474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitchell, J.E.; Peterson, C.B. Anorexia Nervosa. N. Engl. J. Med. 2020, 382, 1343–1351. [Google Scholar] [CrossRef] [PubMed]
- Blanchet, C.; Guillaume, S.; Bat-Pitault, F.; Carles, M.E.; Clarke, J.; Dodin, V.; Duriez, P.; Gerardin, P.; Hanachi-Guidoum, M.; Iceta, S.; et al. Medication in AN: A Multidisciplinary Overview of Meta-Analyses and Systematic Reviews. J. Clin. Med. 2019, 8, 278. [Google Scholar] [CrossRef] [Green Version]
- Treasure, J.; Claudino, A.M.; Zucker, N. Eating disorders. Lancet 2015, 375, 375–583. [Google Scholar] [CrossRef]
- Eating Disorders: Recognition and Treatment (NICE Guideline 69). Available online: https://www.nice.org.uk/guidance/ng69 (accessed on 8 June 2020).
- Slade, E.; Keeney, E.; Mavranezouli, I.; Dias, S.; Fou, L.; Stockton, S.; Saxon, L.; Waller, G.; Turner, H.; Serpell, L.; et al. Treatments for bulimia nervosa: A network meta-analysis. Psychol. Med. 2018, 48, 2629–2636. [Google Scholar] [CrossRef]
- Luan, S.; Williams, I.; Nikolic, K.; Constandinou, T.G. Neuromodulation: Present and emerging methods. Front. Neuroeng. 2014, 7, 27. [Google Scholar] [CrossRef]
- De Pitta, M.; Brunel, N.; Volterra, A. Astrocytes: Orchestrating synaptic plasticity? Neuroscience 2016, 323, 43–61. [Google Scholar] [CrossRef] [Green Version]
- Gomez-Fernandez, L. Cortical plasticity and restoration of neurologic functions: An update on this topic. Rev. Neurol. 2000, 31, 749–756. [Google Scholar]
- Pascual-Leone, A.; Tormos-Munoz, J.M. Transcranial magnetic stimulation: The foundation and potential of modulating specific neuronal networks. Rev. Neurol. 2008, 46 (Suppl. 1), S3–S10. [Google Scholar] [PubMed]
- Lopez-Rojas, J.; Almaguer-Melian, W.; Bergado-Rosado, J.A. Synaptic tagging and memory trace. Rev. Neurol. 2007, 45, 607–614. [Google Scholar] [PubMed]
- Read, J.; Bentall, R. The effectiveness of electroconvulsive therapy: A literature review. Epidemiol. Psichiatr. Soc. 2010, 19, 333–347. [Google Scholar] [CrossRef] [PubMed]
- Klomjai, W.; Katz, R.; Lackmy-Vallee, A. Basic principles of transcranial magnetic stimulation (TMS) and repetitive TMS (rTMS). Ann. Phys. Rehabil. Med. 2015, 58, 208–213. [Google Scholar] [CrossRef]
- Impey, D.; de la Salle, S.; Knott, V. Assessment of anodal and cathodal transcranial direct current stimulation (tDCS) on MMN-indexed auditory sensory processing. Brain Cogn. 2016, 105, 46–54. [Google Scholar] [CrossRef]
- Uher, R.; Murphy, T.; Brammer, M.J.; Dalgleish, T.; Phillips, M.L.; Ng, V.W.; Andrew, C.M.; Williams, S.C.; Campbell, I.C.; Treasure, J. Medial prefrontal cortex activity associated with symptom provocation in eating disorders. Am. J. Psychiatry 2004, 161, 1238–1246. [Google Scholar] [CrossRef]
- Marangell, L.B.; Martinez, M.; Jurdi, R.A.; Zboyan, H. Neurostimulation therapies in depression: A review of new modalities. Acta Psychiatr. Scand. 2007, 116, 174–181. [Google Scholar] [CrossRef]
- Kamolz, S.; Richter, M.M.; Schmidtke, A.; Fallgatter, A.J. Transcranial magnetic stimulation for comorbid depression in anorexia. Nervenarzt 2008, 79, 1071–1073. [Google Scholar] [CrossRef]
- McClelland, J.; Bozhilova, N.; Nestler, S.; Campbell, I.C.; Jacob, S.; Johnson-Sabine, E.; Schmidt, U. Improvements in symptoms following neuronavigated repetitive transcranial magnetic stimulation (rTMS) in severe and enduring anorexia nervosa: Findings from two case studies. Eur. Eat. Disord. Rev. 2013, 21, 500–506. [Google Scholar] [CrossRef]
- Choudhary, P.; Roy, P.; Kumar Kar, S. Improvement of weight and attitude towards eating behaviour with high frequency rTMS augmentation in anorexia nervosa. Asian J. Psychiatr 2017, 28, 160. [Google Scholar] [CrossRef]
- Jassova, K.; Albrecht, J.; Papezova, H.; Anders, M. Repetitive Transcranial Magnetic Stimulation (rTMS) Treatment of Depression and Anxiety in a Patient with Anorexia Nervosa. Med. Sci. Monit. 2018, 24, 5279–5281. [Google Scholar] [CrossRef] [PubMed]
- McClelland, J.; Kekic, M.; Campbell, I.C.; Schmidt, U. Repetitive Transcranial Magnetic Stimulation (rTMS) Treatment in Enduring Anorexia Nervosa: A Case Series. Eur. Eat. Disord. Rev. 2016, 24, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Van den Eynde, F.; Guillaume, S.; Broadbent, H.; Campbell, I.C.; Schmidt, U. Repetitive transcranial magnetic stimulation in anorexia nervosa: A pilot study. Eur Psychiatry 2013, 28, 98–101. [Google Scholar] [CrossRef] [PubMed]
- McClelland, J.; Kekic, M.; Bozhilova, N.; Nestler, S.; Dew, T.; Van den Eynde, F.; David, A.S.; Rubia, K.; Campbell, I.C.; Schmidt, U. A Randomised Controlled Trial of Neuronavigated Repetitive Transcranial Magnetic Stimulation (rTMS) in Anorexia Nervosa. PLoS ONE 2016, 11, e0148606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dalton, B.; Bartholdy, S.; McClelland, J.; Kekic, M.; Rennalls, S.J.; Werthmann, J.; Carter, B.; O’Daly, O.G.; Campbell, I.C.; David, A.S.; et al. Randomised controlled feasibility trial of real versus sham repetitive transcranial magnetic stimulation treatment in adults with severe and enduring anorexia nervosa: The TIARA study. BMJ Open 2018, 8, e021531. [Google Scholar] [CrossRef]
- Bartholdy, S.; McClelland, J.; Kekic, M.; O’Daly, O.G.; Campbell, I.C.; Werthmann, J.; Rennalls, S.J.; Rubia, K.; David, A.S.; Glennon, D.; et al. Clinical outcomes and neural correlates of 20 sessions of repetitive transcranial magnetic stimulation in severe and enduring anorexia nervosa (the TIARA study): Study protocol for a randomised controlled feasibility trial. Trials 2015, 16, 548. [Google Scholar] [CrossRef] [Green Version]
- Dalton, B.; Foerde, K.; Bartholdy, S.; McClelland, J.; Kekic, M.; Grycuk, L.; Campbell, I.C.; Schmidt, U.; Steinglass, J.E. The effect of repetitive transcranial magnetic stimulation on food choice-related self-control in patients with severe, enduring anorexia nervosa. Int. J. Eat. Disord. 2020, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Woodside, D.B.; Colton, P.; Lam, E.; Dunlop, K.; Rzeszutek, J.; Downar, J. Dorsomedial prefrontal cortex repetitive transcranial magnetic stimulation treatment of posttraumatic stress disorder in eating disorders: An open-label case series. Int. J. Eat. Disord. 2017, 50, 1231–1234. [Google Scholar] [CrossRef]
- Knyahnytska, Y.O.; Blumberger, D.M.; Daskalakis, Z.J.; Zomorrodi, R.; Kaplan, A.S. Insula H-coil deep transcranial magnetic stimulation in severe and enduring anorexia nervosa (SE-AN): A pilot study. Neuropsychiatr. Dis. Treat. 2019, 15, 2247–2256. [Google Scholar] [CrossRef] [Green Version]
- Hausmann, A.; Mangweth, B.; Walpoth, M.; Hoertnagel, C.; Kramer-Reinstadler, K.; Rupp, C.I.; Hinterhuber, H. Repetitive transcranial magnetic stimulation (rTMS) in the double-blind treatment of a depressed patient suffering from bulimia nervosa: A case report. Int. J. Neuropsychopharmacol. 2004, 7, 371–373. [Google Scholar] [CrossRef] [Green Version]
- Walpoth, M.; Hoertnagl, C.; Mangweth-Matzek, B.; Kemmler, G.; Hinterholzl, J.; Conca, A.; Hausmann, A. Repetitive transcranial magnetic stimulation in bulimia nervosa: Preliminary results of a single-centre, randomised, double-blind, sham-controlled trial in female outpatients. Psychother. Psychosom. 2008, 77, 57–60. [Google Scholar] [CrossRef] [PubMed]
- Van den Eynde, F.; Claudino, A.M.; Mogg, A.; Horrell, L.; Stahl, D.; Ribeiro, W.; Uher, R.; Campbell, I.; Schmidt, U. Repetitive transcranial magnetic stimulation reduces cue-induced food craving in bulimic disorders. Biol. Psychiatry 2010, 67, 793–795. [Google Scholar] [CrossRef]
- Van den Eynde, F.; Samarawickrema, N.; Kenyon, M.; DeJong, H.; Lavender, A.; Startup, H.; Schmidt, U. A study of neurocognition in bulimia nervosa and eating disorder not otherwise specified-bulimia type. J. Clin. Exp. Neuropsychol. 2012, 34, 67–77. [Google Scholar] [CrossRef] [PubMed]
- Van den Eynde, F.; Claudino, A.M.; Campbell, I.; Horrell, L.; Andiappan, M.; Stahl, D.; Schmidt, U. Cardiac safety of repetitive transcranial magnetic stimulation in bulimic eating disorders. Brain Stimul. 2011, 4, 112–114. [Google Scholar] [CrossRef] [PubMed]
- Claudino, A.M.; Van den Eynde, F.; Stahl, D.; Dew, T.; Andiappan, M.; Kalthoff, J.; Schmidt, U.; Campbell, I.C. Repetitive transcranial magnetic stimulation reduces cortisol concentrations in bulimic disorders. Psychol. Med. 2011, 41, 1329–1336. [Google Scholar] [CrossRef] [PubMed]
- Van den Eynde, F.; Broadbent, H.; Guillaume, S.; Claudino, A.; Campbell, I.C.; Schmidt, U. Handedness, repetitive transcranial magnetic stimulation and bulimic disorders. Eur. Psychiatry 2012, 27, 290–293. [Google Scholar] [CrossRef]
- Downar, J.; Sankar, A.; Giacobbe, P.; Woodside, B.; Colton, P. Unanticipated Rapid Remission of Refractory Bulimia Nervosa, during High-Dose Repetitive Transcranial Magnetic Stimulation of the Dorsomedial Prefrontal Cortex: A Case Report. Front. Psychiatry 2012, 3, 30. [Google Scholar] [CrossRef] [Green Version]
- Baczynski, T.P.; de Aquino Chaim, C.H.; Nazar, B.P.; Carta, M.G.; Arias-Carrion, O.; Silva, A.C.; Machado, S.; Nardi, A.E. High-frequency rTMS to treat refractory binge eating disorder and comorbid depression: A case report. CNS Neurol. Disord. Drug Targets 2014, 13, 771–775. [Google Scholar] [CrossRef]
- Dunlop, K.; Woodside, B.; Lam, E.; Olmsted, M.; Colton, P.; Giacobbe, P.; Downar, J. Increases in frontostriatal connectivity are associated with response to dorsomedial repetitive transcranial magnetic stimulation in refractory binge/purge behaviors. Neuroimage Clin. 2015, 8, 611–618. [Google Scholar] [CrossRef] [Green Version]
- Sutoh, C.; Koga, Y.; Kimura, H.; Kanahara, N.; Numata, N.; Hirano, Y.; Matsuzawa, D.; Iyo, M.; Nakazato, M.; Shimizu, E. Repetitive Transcranial Magnetic Stimulation Changes Cerebral Oxygenation on the Left Dorsolateral Prefrontal Cortex in Bulimia Nervosa: A Near-Infrared Spectroscopy Pilot Study. Eur. Eat. Disord. Rev. 2016, 24, 83–88. [Google Scholar] [CrossRef]
- Gay, A.; Jaussent, I.; Sigaud, T.; Billard, S.; Attal, J.; Seneque, M.; Galusca, B.; Van Den Eynde, F.; Massoubre, C.; Courtet, P.; et al. A Lack of Clinical Effect of High-frequency rTMS to Dorsolateral Prefrontal Cortex on Bulimic Symptoms: A Randomised, Double-blind Trial. Eur. Eat. Disord. Rev. 2016, 24, 474–481. [Google Scholar] [CrossRef] [PubMed]
- Guillaume, S.; Gay, A.; Jaussent, I.; Sigaud, T.; Billard, S.; Attal, J.; Seneque, M.; Galusca, B.; Thiebaut, S.; Massoubre, C.; et al. Improving decision-making and cognitive impulse control in bulimia nervosa by rTMS: An ancillary randomized controlled study. Int. J. Eat. Disord. 2018, 51, 1103–1106. [Google Scholar] [CrossRef] [PubMed]
- Dalton, B.; Bartholdy, S.; Campbell, I.C.; Schmidt, U. Neurostimulation in Clinical and Sub-clinical Eating Disorders: A Systematic Update of the Literature. Curr. Neuropharmacol. 2018, 16, 1174–1192. [Google Scholar] [CrossRef] [PubMed]
- Uher, R.; Yoganathan, D.; Mogg, A.; Eranti, S.V.; Treasure, J.; Campbell, I.C.; McLoughlin, D.M.; Schmidt, U. Effect of left prefrontal repetitive transcranial magnetic stimulation on food craving. Biol. Psychiatry 2005, 58, 840–842. [Google Scholar] [CrossRef]
- Maranhao, M.F.; Estella, N.M.; Cury, M.E.; Amigo, V.L.; Picasso, C.M.; Berberian, A.; Campbell, I.; Schmidt, U.; Claudino, A.M. The effects of repetitive transcranial magnetic stimulation in obese females with binge eating disorder: A protocol for a double-blinded, randomized, sham-controlled trial. BMC Psychiatry 2015, 15, 194. [Google Scholar] [CrossRef] [Green Version]
- Titova, O.E.; Hjorth, O.C.; Schioth, H.B.; Brooks, S.J. Anorexia nervosa is linked to reduced brain structure in reward and somatosensory regions: A meta-analysis of VBM studies. BMC Psychiatry 2013, 13, 110. [Google Scholar] [CrossRef] [Green Version]
- Kaye, W.H.; Wierenga, C.E.; Bischoff-Grethe, A.; Berner, L.A.; Ely, A.V.; Bailer, U.F.; Paulus, M.P.; Fudge, J.L. Neural Insensitivity to the Effects of Hunger in Women Remitted From Anorexia Nervosa. Am. J. Psychiatry 2020. [Google Scholar] [CrossRef]
- Steward, T.; Menchon, J.M.; Jimenez-Murcia, S.; Soriano-Mas, C.; Fernandez-Aranda, F. Neural Network Alterations Across Eating Disorders: A Narrative Review of fMRI Studies. Curr. Neuropharmacol. 2018, 16, 1150–1163. [Google Scholar] [CrossRef]
- Cha, J.; Ide, J.S.; Bowman, F.D.; Simpson, H.B.; Posner, J.; Steinglass, J.E. Abnormal reward circuitry in anorexia nervosa: A longitudinal, multimodal MRI study. Hum. Brain Mapp. 2016, 37, 3835–3846. [Google Scholar] [CrossRef] [Green Version]
- Ruffini, C.; Locatelli, M.; Lucca, A.; Benedetti, F.; Insacco, C.; Smeraldi, E. Augmentation effect of repetitive transcranial magnetic stimulation over the orbitofrontal cortex in drug-resistant obsessive-compulsive disorder patients: A controlled investigation. Prim. Care Companion J. Clin. Psychiatry 2009, 11, 226–230. [Google Scholar] [CrossRef]
- Rose, J.E.; McClernon, F.J.; Froeliger, B.; Behm, F.M.; Preud’homme, X.; Krystal, A.D. Repetitive transcranial magnetic stimulation of the superior frontal gyrus modulates craving for cigarettes. Biol. Psychiatry 2011, 70, 794–799. [Google Scholar] [CrossRef] [PubMed]
- Hanlon, C.A.; Dowdle, L.T.; Austelle, C.W.; DeVries, W.; Mithoefer, O.; Badran, B.W.; George, M.S. What goes up, can come down: Novel brain stimulation paradigms may attenuate craving and craving-related neural circuitry in substance dependent individuals. Brain Res. 2015, 1628, 199–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hecht, D. Transcranial direct current stimulation in the treatment of anorexia. Med. Hypotheses 2010, 74, 1044–1047. [Google Scholar] [CrossRef]
- Khedr, E.M.; Elfetoh, N.A.; Ali, A.M.; Noamany, M. Anodal transcranial direct current stimulation over the dorsolateral prefrontal cortex improves anorexia nervosa: A pilot study. Restor. Neurol. Neurosci. 2014, 32, 789–797. [Google Scholar] [CrossRef] [PubMed]
- Strumila, R.; Thiebaut, S.; Jaussent, I.; Seneque, M.; Attal, J.; Courtet, P.; Guillaume, S. Safety and efficacy of transcranial direct current stimulation (tDCS) in the treatment of Anorexia Nervosa. The open-label STAR study. Brain Stimul. 2019, 12, 1325–1327. [Google Scholar] [CrossRef]
- Phillipou, A.; Kirkovski, M.; Castle, D.J.; Gurvich, C.; Abel, L.A.; Miles, S.; Rossell, S.L. High-definition transcranial direct current stimulation in anorexia nervosa: A pilot study. Int. J. Eat. Disord. 2019, 52, 1274–1280. [Google Scholar] [CrossRef]
- Burgess, E.E.; Sylvester, M.D.; Morse, K.E.; Amthor, F.R.; Mrug, S.; Lokken, K.L.; Osborn, M.K.; Soleymani, T.; Boggiano, M.M. Effects of transcranial direct current stimulation (tDCS) on binge eating disorder. Int. J. Eat. Disord. 2016, 49, 930–936. [Google Scholar] [CrossRef]
- Kekic, M.; McClelland, J.; Bartholdy, S.; Boysen, E.; Musiat, P.; Dalton, B.; Tiza, M.; David, A.S.; Campbell, I.C.; Schmidt, U. Single-Session Transcranial Direct Current Stimulation Temporarily Improves Symptoms, Mood, and Self-Regulatory Control in Bulimia Nervosa: A Randomised Controlled Trial. PLoS ONE 2017, 12, e0167606. [Google Scholar] [CrossRef]
- Sreeraj, V.S.; Masali, M.; Shivakumar, V.; Bose, A.; Venkatasubramanian, G. Clinical Utility of Add-On Transcranial Direct Current Stimulation for Binge Eating Disorder with Obesity in Schizophrenia. Indian J. Psychol. Med. 2018, 40, 487–490. [Google Scholar] [CrossRef]
- Pacilio, R.M.; Livingston, R.K.; Gordon, M.R. The Use of Electroconvulsive Therapy in Eating Disorders: A Systematic Literature Review and Case Report. J. ECT 2019, 35, 272–278. [Google Scholar] [CrossRef]
- Shilton, T.; Enoch-Levy, A.; Giron, Y.; Yaroslavsky, A.; Amiaz, R.; Gothelf, D.; Weizman, A.; Stein, D. A retrospective case series of electroconvulsive therapy in the management of comorbid depression and anorexia nervosa. Int. J. Eat. Disord. 2020, 53, 210–218. [Google Scholar] [CrossRef] [PubMed]
- Naguy, A.; Al-Tajali, A.; Alamiri, B. An Adolescent Case of Treatment-Refractory Anorexia Nervosa Favorably Responded to Electroconvulsive Therapy. J. ECT 2019, 35, 217–218. [Google Scholar] [CrossRef] [PubMed]
- Duriez, P.; Ramoz, N.; Gorwood, P.; Viltart, O.; Tolle, V. A Metabolic Perspective on Reward Abnormalities in Anorexia Nervosa. Trends Endocrinol. Metab. 2019, 30, 915–928. [Google Scholar] [CrossRef] [PubMed]
- Davis, H.K. Anorexia nervosa: Treatment with hypnosis and ECT. Dis. Nerv. Syst. 1961, 22, 627–631. [Google Scholar] [PubMed]
- Bernstein, I.C. Anorexia Nervosa Treated Successfully with Electroshock Therapy and Subsequently Followed by Pregnancy. Am. J. Psychiatry 1964, 120, 1023–1024. [Google Scholar] [CrossRef]
- Bernstein, I.C. Anorexia nervosa, 94-year-old woman treated with electroshock. Minn. Med. 1972, 55, 552–553. [Google Scholar]
- Ferguson, J.M. The use of electroconvulsive therapy in patients with intractable anorexia nervosa. Int. J. Eat. Disord. 1993, 13, 195–201. [Google Scholar] [CrossRef]
- Bek, R.; Hotujak, L. Clinical characteristics of female patients suffering from anorexia nervosa. Soc. Psihijat. 1996, 24, 159–161. [Google Scholar]
- Hill, R.; Haslett, C.; Kumar, S. Anorexia nervosa in an elderly woman. Aust. N. Z. J. Psychiatry 2001, 35, 246–248. [Google Scholar] [CrossRef]
- Poutanen, O.; Huuhka, K.; Perko, K. Severe anorexia nervosa, co-occurring major depressive disorder and electroconvulsive therapy as maintenance treatment: A case report. Cases J. 2009, 2, 9362. [Google Scholar] [CrossRef] [Green Version]
- Andrews, J.T.; Seide, M.; Guarda, A.S.; Redgrave, G.W.; Coffey, D.B. Electroconvulsive therapy in an adolescent with severe major depression and anorexia nervosa. J. Child. Adolesc. Psychopharmacol. 2014, 24, 94–98. [Google Scholar] [CrossRef] [PubMed]
- Andersen, L.; LaRosa, C.; Gih, D.E. Reexamining the Role of Electroconvulsive Therapy in Anorexia Nervosa in Adolescents. J. ECT 2017, 33, 294–296. [Google Scholar] [CrossRef] [PubMed]
- Saglam, T.; Aksoy Poyraz, C.; Poyraz, B.C.; Tosun, M. Successful use of electroconvulsive therapy in a patient with anorexia nervosa and severe acute-onset obsessive-compulsive disorder. Int. J. Eat. Disord. 2018, 51, 1026–1028. [Google Scholar] [CrossRef] [PubMed]
- Duriez, P.; Maatoug, R.; Verbe, J. Failure of Electroconvulsive Therapy to Improve Anorexia Nervosa in the Absence of Other Psychiatric Comorbidities: A Case Report. J. ECT 2020. [Google Scholar] [CrossRef] [PubMed]
- Rapinesi, C.; Del Casale, A.; Serata, D.; Caccia, F.; Di Pietro, S.; Scatena, P.; Carbonetti, P.; Fensore, C.; Angeletti, G.; Tatarelli, R.; et al. Electroconvulsive therapy in a man with comorbid severe obesity, binge eating disorder, and bipolar disorder. J. ECT 2013, 29, 142–144. [Google Scholar] [CrossRef] [PubMed]
- Jaite, C.; Hoffmann, F.; Glaeske, G.; Bachmann, C.J. Prevalence, comorbidities and outpatient treatment of anorexia and bulimia nervosa in German children and adolescents. Eat. Weight Disord. 2013, 18, 157–165. [Google Scholar] [CrossRef]
- Val-Laillet, D.; Aarts, E.; Weber, B.; Ferrari, M.; Quaresima, V.; Stoeckel, L.E.; Alonso-Alonso, M.; Audette, M.; Malbert, C.H.; Stice, E. Neuroimaging and neuromodulation approaches to study eating behavior and prevent and treat eating disorders and obesity. Neuroimage Clin. 2015, 8, 1–31. [Google Scholar] [CrossRef]
- McClelland, J.; Bozhilova, N.; Campbell, I.; Schmidt, U. A systematic review of the effects of neuromodulation on eating and body weight: Evidence from human and animal studies. Eur. Eat. Disord. Rev. 2013, 21, 436–455. [Google Scholar] [CrossRef]
- Badran, B.W.; Dowdle, L.T.; Mithoefer, O.J.; LaBate, N.T.; Coatsworth, J.; Brown, J.C.; DeVries, W.H.; Austelle, C.W.; McTeague, L.M.; George, M.S. Neurophysiologic effects of transcutaneous auricular vagus nerve stimulation (taVNS) via electrical stimulation of the tragus: A concurrent taVNS/fMRI study and review. Brain Stimul. 2018, 11, 492–500. [Google Scholar] [CrossRef]
- Dietrich, S.; Smith, J.; Scherzinger, C.; Hofmann-Preiss, K.; Freitag, T.; Eisenkolb, A.; Ringler, R. A novel transcutaneous vagus nerve stimulation leads to brainstem and cerebral activations measured by functional MRI. Biomed. Tech. 2008, 53, 104–111. [Google Scholar] [CrossRef]
- Yakunina, N.; Kim, S.S.; Nam, E.C. Optimization of Transcutaneous Vagus Nerve Stimulation Using Functional MRI. Neuromodulation 2017, 20, 290–300. [Google Scholar] [CrossRef] [PubMed]
- Villani, V.; Tsakiris, M.; Azevedo, R.T. Transcutaneous vagus nerve stimulation improves interoceptive accuracy. Neuropsychologia 2019, 134, 107201. [Google Scholar] [CrossRef] [PubMed]
- Kaye, W.H.; Wagner, A.; Fudge, J.L.; Paulus, M. Neurocircuity of eating disorders. Curr. Top. Behav. Neurosci. 2011, 6, 37–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khalsa, S.S.; Adolphs, R.; Cameron, O.G.; Critchley, H.D.; Davenport, P.W.; Feinstein, J.S.; Feusner, J.D.; Garfinkel, S.N.; Lane, R.D.; Mehling, W.E.; et al. Interoception and Mental Health: A Roadmap. Biol Psychiatry Cogn. Neurosci. Neuroimaging 2018, 3, 501–513. [Google Scholar] [CrossRef] [PubMed]
- Berner, L.A.; Simmons, A.N.; Wierenga, C.E.; Bischoff-Grethe, A.; Paulus, M.P.; Bailer, U.F.; Kaye, W.H. Altered anticipation and processing of aversive interoceptive experience among women remitted from bulimia nervosa. Neuropsychopharmacology 2019, 44, 1265–1273. [Google Scholar] [CrossRef]
- Sobstyl, M.; Stapinska-Syniec, A.; Sokol-Szawlowska, M.; Kupryjaniuk, A. Deep brain stimulation for the treatment of severe intractable anorexia nervosa. Br. J. Neurosurg. 2019, 33, 601–607. [Google Scholar] [CrossRef] [PubMed]
- Israel, M.; Steiger, H.; Kolivakis, T.; McGregor, L.; Sadikot, A.F. Deep brain stimulation in the subgenual cingulate cortex for an intractable eating disorder. Biol. Psychiatry 2010, 67, e53–e54. [Google Scholar] [CrossRef]
- Barbier, J.; Gabriels, L.; van Laere, K.; Nuttin, B. Successful anterior capsulotomy in comorbid anorexia nervosa and obsessive-compulsive disorder: Case report. Neurosurgery 2011, 69, E745–E751, discussion E751. [Google Scholar] [CrossRef]
- McLaughlin, N.C.; Didie, E.R.; Machado, A.G.; Haber, S.N.; Eskandar, E.N.; Greenberg, B.D. Improvements in anorexia symptoms after deep brain stimulation for intractable obsessive-compulsive disorder. Biol. Psychiatry 2013, 73, e29–e31. [Google Scholar] [CrossRef]
- Blomstedt, P.; Naesstrom, M.; Bodlund, O. Deep brain stimulation in the bed nucleus of the stria terminalis and medial forebrain bundle in a patient with major depressive disorder and anorexia nervosa. Clin. Case Rep. 2017, 5, 679–684. [Google Scholar] [CrossRef]
- Park, R.J.; Singh, I.; Pike, A.C.; Tan, J.O. Deep Brain Stimulation in Anorexia Nervosa: Hope for the Hopeless or Exploitation of the Vulnerable? The Oxford Neuroethics Gold Standard Framework. Front. Psychiatry 2017, 8, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lipsman, N.; Lam, E.; Volpini, M.; Sutandar, K.; Twose, R.; Giacobbe, P.; Sodums, D.J.; Smith, G.S.; Woodside, D.B.; Lozano, A.M. Deep brain stimulation of the subcallosal cingulate for treatment-refractory anorexia nervosa: 1 year follow-up of an open-label trial. Lancet Psychiatry 2017, 4, 285–294. [Google Scholar] [CrossRef]
- Wu, H.; Van Dyck-Lippens, P.J.; Santegoeds, R.; van Kuyck, K.; Gabriels, L.; Lin, G.; Pan, G.; Li, Y.; Li, D.; Zhan, S.; et al. Deep-brain stimulation for anorexia nervosa. World Neurosurg. 2013, 80, S29.e1–S29.e10. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Chang, C.; Geng, N.; Wang, X.; Gao, G. Treatment of intractable anorexia nervosa with inactivation of the nucleus accumbens using stereotactic surgery. Stereotact. Funct. Neurosurg. 2013, 91, 364–372. [Google Scholar] [CrossRef]
- Lipsman, N.; Woodside, D.B.; Giacobbe, P.; Lozano, A.M. Neurosurgical treatment of anorexia nervosa: Review of the literature from leucotomy to deep brain stimulation. Eur. Eat. Disord. Rev. 2013, 21, 428–435. [Google Scholar] [CrossRef]
- Zhang, H.W.; Li, D.Y.; Zhao, J.; Guan, Y.H.; Sun, B.M.; Zuo, C.T. Metabolic imaging of deep brain stimulation in anorexia nervosa: A 18F-FDG PET/CT study. Clin. Nucl. Med. 2013, 38, 943–948. [Google Scholar] [CrossRef]
- Liu, W.; Zhan, S.; Li, D.; Lin, Z.; Zhang, C.; Wang, T.; Pan, S.; Zhang, J.; Cao, C.; Jin, H.; et al. Deep brain stimulation of the nucleus accumbens for treatment-refractory anorexia nervosa: A long-term follow-up study. Brain Stimul. 2020, 13, 643–649. [Google Scholar] [CrossRef] [Green Version]
- Sun, B.; Liu, W. Stereotactic surgery for eating disorders. Surg. Neurol. Int. 2013, 4, S164–S169. [Google Scholar] [CrossRef]
- Hayes, D.J.; Lipsman, N.; Chen, D.Q.; Woodside, D.B.; Davis, K.D.; Lozano, A.M.; Hodaie, M. Subcallosal Cingulate Connectivity in Anorexia Nervosa Patients Differs From Healthy Controls: A Multi-tensor Tractography Study. Brain Stimul. 2015, 8, 758–768. [Google Scholar] [CrossRef] [Green Version]
- Manuelli, M.; Franzini, A.; Galentino, R.; Bidone, R.; Dell’Osso, B.; Porta, M.; Servello, D.; Cena, H. Changes in eating behavior after deep brain stimulation for anorexia nervosa. A case study. Eat. Weight Disord. 2019. [Google Scholar] [CrossRef]
- Villalba Martinez, G.; Justicia, A.; Salgado, P.; Gines, J.M.; Guardiola, R.; Cedron, C.; Polo, M.; Delgado-Martinez, I.; Medrano, S.; Manero, R.M.; et al. A Randomized Trial of Deep Brain Stimulation to the Subcallosal Cingulate and Nucleus Accumbens in Patients with Treatment-Refractory, Chronic, and Severe Anorexia Nervosa: Initial Results at 6 Months of Follow Up. J. Clin. Med. 2020, 9, 1946. [Google Scholar] [CrossRef] [PubMed]
- Whiting, D.M.; Tomycz, N.D.; Bailes, J.; de Jonge, L.; Lecoultre, V.; Wilent, B.; Alcindor, D.; Prostko, E.R.; Cheng, B.C.; Angle, C.; et al. Lateral hypothalamic area deep brain stimulation for refractory obesity: A pilot study with preliminary data on safety, body weight, and energy metabolism. J. Neurosurg. 2013, 119, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Tronnier, V.M.; Rasche, D.; Thorns, V.; Alvarez-Fischer, D.; Munte, T.F.; Zurowski, B. Massive weight loss following deep brain stimulation of the nucleus accumbens in a depressed woman. Neurocase 2018, 24, 49–53. [Google Scholar] [CrossRef] [PubMed]
- Formolo, D.A.; Gaspar, J.M.; Melo, H.M.; Eichwald, T.; Zepeda, R.J.; Latini, A.; Okun, M.S.; Walz, R. Deep Brain Stimulation for Obesity: A Review and Future Directions. Front. Neurosci. 2019, 13, 323. [Google Scholar] [CrossRef] [PubMed]
- Mayberg, H.S.; Liotti, M.; Brannan, S.K.; McGinnis, S.; Mahurin, R.K.; Jerabek, P.A.; Silva, J.A.; Tekell, J.L.; Martin, C.C.; Lancaster, J.L.; et al. Reciprocal limbic-cortical function and negative mood: Converging PET findings in depression and normal sadness. Am. J. Psychiatry 1999, 156, 675–682. [Google Scholar] [CrossRef]
- Lipsman, N.; Woodside, D.B.; Lozano, A.M. Neurocircuitry of limbic dysfunction in anorexia nervosa. Cortex 2015, 62, 109–118. [Google Scholar] [CrossRef]
- Lebow, M.A.; Chen, A. Overshadowed by the amygdala: The bed nucleus of the stria terminalis emerges as key to psychiatric disorders. Mol. Psychiatry 2016, 21, 450–463. [Google Scholar] [CrossRef]
- Coenen, V.A.; Panksepp, J.; Hurwitz, T.A.; Urbach, H.; Madler, B. Human medial forebrain bundle (MFB) and anterior thalamic radiation (ATR): Imaging of two major subcortical pathways and the dynamic balance of opposite affects in understanding depression. J. Neuropsychiatry Clin. Neurosci. 2012, 24, 223–236. [Google Scholar] [CrossRef]
- van der Plasse, G.; Schrama, R.; van Seters, S.P.; Vanderschuren, L.J.; Westenberg, H.G. Deep brain stimulation reveals a dissociation of consummatory and motivated behaviour in the medial and lateral nucleus accumbens shell of the rat. PLoS ONE 2012, 7, e33455. [Google Scholar] [CrossRef]
- Guercio, L.A.; Schmidt, H.D.; Pierce, R.C. Deep brain stimulation of the nucleus accumbens shell attenuates cue-induced reinstatement of both cocaine and sucrose seeking in rats. Behav. Brain Res. 2015, 281, 125–130. [Google Scholar] [CrossRef] [Green Version]
- Steding, J.; Boehm, I.; King, J.A.; Geisler, D.; Ritschel, F.; Seidel, M.; Doose, A.; Jaite, C.; Roessner, V.; Smolka, M.N.; et al. Goal-directed vs. habitual instrumental behavior during reward processing in anorexia nervosa: An fMRI study. Sci. Rep. 2019, 9, 13529. [Google Scholar] [CrossRef] [PubMed]
- Foldi, C.J.; Milton, L.K.; Oldfield, B.J. The Role of Mesolimbic Reward Neurocircuitry in Prevention and Rescue of the Activity-Based Anorexia (ABA) Phenotype in Rats. Neuropsychopharmacology 2017, 42, 2292–2300. [Google Scholar] [CrossRef]
- Joshi, S.H.; Espinoza, R.T.; Pirnia, T.; Shi, J.; Wang, Y.; Ayers, B.; Leaver, A.; Woods, R.P.; Narr, K.L. Structural Plasticity of the Hippocampus and Amygdala Induced by Electroconvulsive Therapy in Major Depression. Biol. Psychiatry 2016, 79, 282–292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zangen, A.; Roth, Y.; Voller, B.; Hallett, M. Transcranial magnetic stimulation of deep brain regions: Evidence for efficacy of the H-coil. Clin. Neurophysiol. 2005, 116, 775–779. [Google Scholar] [CrossRef] [PubMed]
- Gearhardt, A.N.; White, M.A.; Potenza, M.N. Binge eating disorder and food addiction. Curr. Drug Abuse Rev. 2011, 4, 201–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Volkow, N.D.; Wang, G.J.; Fowler, J.S.; Tomasi, D.; Baler, R. Food and drug reward: Overlapping circuits in human obesity and addiction. Curr. Top. Behav. Neurosci. 2012, 11, 1–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bayes, A.J.; Parker, G.B. Comparison of guidelines for the treatment of unipolar depression: A focus on pharmacotherapy and neurostimulation. Acta Psychiatr. Scand. 2018, 137, 459–471. [Google Scholar] [CrossRef]
- Pan, L.A.; Martin, P.; Zimmer, T.; Segreti, A.M.; Kassiff, S.; McKain, B.W.; Baca, C.A.; Rengasamy, M.; Hyland, K.; Walano, N.; et al. Neurometabolic Disorders: Potentially Treatable Abnormalities in Patients With Treatment-Refractory Depression and Suicidal Behavior. Am. J. Psychiatry 2017, 174, 42–50. [Google Scholar] [CrossRef]
- Schwieler, L.; Samuelsson, M.; Frye, M.A.; Bhat, M.; Schuppe-Koistinen, I.; Jungholm, O.; Johansson, A.G.; Landen, M.; Sellgren, C.M.; Erhardt, S. Electroconvulsive therapy suppresses the neurotoxic branch of the kynurenine pathway in treatment-resistant depressed patients. J. Neuroinflamm. 2016, 13, 51. [Google Scholar] [CrossRef] [Green Version]
- Romano, S.J.; Halmi, K.A.; Sarkar, N.P.; Koke, S.C.; Lee, J.S. A placebo-controlled study of fluoxetine in continued treatment of bulimia nervosa after successful acute fluoxetine treatment. Am. J. Psychiatry 2002, 159, 96–102. [Google Scholar] [CrossRef]
- Roberts, M.E.; Tchanturia, K.; Stahl, D.; Southgate, L.; Treasure, J. A systematic review and meta-analysis of set-shifting ability in eating disorders. Psychol. Med. 2007, 37, 1075–1084. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lang, K.; Lopez, C.; Stahl, D.; Tchanturia, K.; Treasure, J. Central coherence in eating disorders: An updated systematic review and meta-analysis. World J. Biol. Psychiatry 2014, 15, 586–598. [Google Scholar] [CrossRef] [PubMed]
- Guillaume, S.; Gorwood, P.; Jollant, F.; Van den Eynde, F.; Courtet, P.; Richard-Devantoy, S. Impaired decision-making in symptomatic anorexia and bulimia nervosa patients: A meta-analysis. Psychol. Med. 2015, 45, 3377–3391. [Google Scholar] [CrossRef] [PubMed]
- Leppanen, J.; Adamson, J.; Tchanturia, K. Impact of Cognitive Remediation Therapy on Neurocognitive Processing in Anorexia Nervosa. Front. Psychiatry 2018, 9, 96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brevet-Aeby, C.; Brunelin, J.; Iceta, S.; Padovan, C.; Poulet, E. Prefrontal cortex and impulsivity: Interest of noninvasive brain stimulation. Neurosci. Biobehav. Rev. 2016, 71, 112–134. [Google Scholar] [CrossRef]
- Gordon, G.; Brockmeyer, T.; Schmidt, U.; Campbell, I.C. Combining cognitive bias modification training (CBM) and transcranial direct current stimulation (tDCS) to treat binge eating disorder: Study protocol of a randomised controlled feasibility trial. BMJ Open 2019, 9, e030023. [Google Scholar] [CrossRef]
- Dinur-Klein, L.; Dannon, P.; Hadar, A.; Rosenberg, O.; Roth, Y.; Kotler, M.; Zangen, A. Smoking cessation induced by deep repetitive transcranial magnetic stimulation of the prefrontal and insular cortices: A prospective, randomized controlled trial. Biol. Psychiatry 2014, 76, 742–749. [Google Scholar] [CrossRef]
- Karas, P.J.; Lee, S.; Jimenez-Shahed, J.; Goodman, W.K.; Viswanathan, A.; Sheth, S.A. Deep Brain Stimulation for Obsessive Compulsive Disorder: Evolution of Surgical Stimulation Target Parallels Changing Model of Dysfunctional Brain Circuits. Front. Neurosci. 2018, 12, 998. [Google Scholar] [CrossRef]
- Grossman, N.; Bono, D.; Dedic, N.; Kodandaramaiah, S.B.; Rudenko, A.; Suk, H.J.; Cassara, A.M.; Neufeld, E.; Kuster, N.; Tsai, L.H.; et al. Noninvasive Deep Brain Stimulation via Temporally Interfering Electric Fields. Cell 2017, 169, 1029–1041. [Google Scholar] [CrossRef] [Green Version]
- Lozano, A.M. Waving Hello to Noninvasive Deep-Brain Stimulation. N. Engl. J. Med. 2017, 377, 1096–1098. [Google Scholar] [CrossRef]
- Delbeke, J.; Hoffman, L.; Mols, K.; Braeken, D.; Prodanov, D. And Then There Was Light: Perspectives of Optogenetics for Deep Brain Stimulation and Neuromodulation. Front. Neurosci. 2017, 11, 663. [Google Scholar] [CrossRef] [Green Version]
- Gradinaru, V.; Mogri, M.; Thompson, K.R.; Henderson, J.M.; Deisseroth, K. Optical deconstruction of parkinsonian neural circuitry. Science 2009, 324, 354–359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Treasure, J.; Stein, D.; Maguire, S. Has the time come for a staging model to map the course of eating disorders from high risk to severe enduring illness? An examination of the evidence. Early Interv. Psychiatry 2015, 9, 173–184. [Google Scholar] [CrossRef] [PubMed]
- Dunlop, K.A.; Woodside, B.; Downar, J. Targeting Neural Endophenotypes of Eating Disorders with Non-invasive Brain Stimulation. Front. Neurosci. 2016, 10, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wildes, J.E.; Marcus, M.D. Application of the Research Domain Criteria (RDoC) framework to eating disorders: Emerging concepts and research. Curr. Psychiatry Rep. 2015, 17, 30. [Google Scholar] [CrossRef] [PubMed]
- Kearney-Ramos, T.E.; Dowdle, L.T.; Mithoefer, O.J.; Devries, W.; George, M.S.; Hanlon, C.A. State-Dependent Effects of Ventromedial Prefrontal Cortex Continuous Thetaburst Stimulation on Cocaine Cue Reactivity in Chronic Cocaine Users. Front. Psychiatry 2019, 10, 317. [Google Scholar] [CrossRef] [Green Version]
- Wonderlich, S.A.; Bulik, C.M.; Schmidt, U.; Steiger, H.; Hoek, H.W. Severe and enduring anorexia nervosa: Update and observations about the current clinical reality. Int. J. Eat. Disord. 2020. [Google Scholar] [CrossRef]


{kind=link}
| Reference | Type of Study | Participants | Modulation Target | Treatment Characteristics | Main Results |
|---|---|---|---|---|---|
| Anorexia Nervosa | |||||
| Kamolz et al., 2008 [19] | Case report | 24-year-old female with AN | Left DLPFC Manual targeting | 41 sessions 100 × 2 s trains/10 s inter-train interval at 10 Hz = 2000 pulses per session, 110 % MT | Full remission |
| Van den Eynde et al., 2013 [24] | Case series (pilot study) | 10 patients with AN | Left DLPFC Manual targeting | 1 session, 20 × 5 s trains/55 s inter-train interval, 10 Hz, intensity of 110% MT, 1000 pulses over 20 min | Reduced levels of feeling full, feeling fat, and feeling anxious |
| McClelland et al., 2013 [20] | Case report | 23-year-old and 52-year-old women with AN 1 | Left DLPFC Neuronavigation | 20 and 19 sessions 20 × 5 s trains/55 s inter-train interval, 10 Hz, intensity of 110% MT, 1000 pulses over 20 min within each session | Significant improvement |
| McClelland et al., 2016 [23] | Case series | 5 women with AN 1 | Left DLPFC Neuronavigation | ~20 sessions, 20 × 5 s trains/55 s inter-train interval, 10 Hz, intensity of 110% MT, 1000 pulses over 20 min within each session | Significant improvement of ED and affective symptoms after 6 months, but positive results waned at 12 months follow-up |
| McClelland et al., 2016 [25] | RCT | 49 patients with AN 1 | Left DLPFC Neuronavigation | 1 session 5 s trains/55 s inter-train interval, 10 Hz, intensity of 110% MT, 1000 pulses over 20 min | No significant effect on core symptoms of ED compared to sham rTMS, but improvement in individuals who received real rTMS when compared before and after the session and the results persisted at 24 h of follow-up |
| Choudhary et al., 2017 [21] | Case report | 23-year-old female with AN | Left DLPFC Manual targeting | 21 sessions High-frequency rTMS (10 Hz) at 110% of resting MT, 1000 pulses | Significant improvement |
| Jaššová et al., 2018 [22] | Case report | 25-year-old female with AN | Left DLPFC Targeting method not available | 10 sessions, 10 Hz, 15 trains/day, 100 pulses/train, intertrain interval 107 s | No improvement of ED, anxiety, or depression |
| Woodside et al., 2017 [29] | Case series | Fourteen subjects with eating disorders (6 AN, 5 BN, and 3 ednos) and comorbid PTSD | DMPFC Neuronavigation | 20–30 sessions 120% resting MT, at 10 Hz, 5 s on, 10 s off, 3000 pulses/hemisphere, with left then right lateralized coil orientation | Improvement in emotional regulation and PTSD symptoms |
| Dalton et al., 2018 [26] | RCT | 30 patients (16 real, 14 sham) with AN 2 | Left DLPF CNeuronavigation | 20 sessions, 20 × 5 s trains/55 s inter-train interval, 10 Hz, intensity of 110% MT, 1000 pulses over 20 min within each session | Between-group effect sizes of change scores (baseline to follow-up) were small for BMI (d = 0.2, 95% CI −0.49 to 0.90) and eating disorder symptoms (d = 0.1, 95% CI −0.60 to 0.79), medium for quality of life and moderate to large (d = 0.61 to 1.0) for mood outcomes, all favoring rTMS over sham |
| Knyahnytska et al., 2019 [30] | Case series (pilot study) | 8 women with AN | Insula Manual targeting | 42 sessions, H-coil dTMS 18 Hz, 2 s on, 20 s off, number of pulses 36, number of trains 80, over 20 min | Reduction in AN-related obsessions and compulsions, as well as depression and anxiety scores |
| Dalton et al., 2020 [28] | RCT | 34 anorexic female patients (17 real, 17 sham) vs. 30 healthy controls 2 | Left DLPFC Neuronavigation | 20 sessions 20 × 5 s trains/55 s inter-train interval, 10 Hz, intensity of 110% MT, 1000 pulses over 20 min within each session | No significant effect of rTMS nor time on food choices related to fat content. Among AN participants who received real rTMS, there was a decrease in self-controlled food choices at post-treatment |
| Bulimic Disorders (Bulimia and/or Binge Eating Disorders) | |||||
| Hausmann et al., 2004 [31] | Case report | One woman with BN and depression | Left DLPFC Neuronavigation | 10 sessions, 20 × 5 s trains/55 s inter-train interval, 10 Hz, intensity of 110% MT | Significant improvement in BN symptoms |
| Walpoth et al., 2008 [32] | RCT | 14 females with BN | Left DLPFC Manual targeting | 15 sessions, 10 × 10 s trains/60 s inter-train interval at 20 Hz, = 2000 pulses; 120% MT | No difference between real and sham group |
| Van den Eynde et al., 2010 [33] | RCT | 38 females with BN 3 | Left DLPFC Manual targeting | 1 session, 20 × 5 s trains/55 s inter-train interval, 10 Hz, intensity of 110% MT, 1000 pulses over 20 min | Real rTMS associated with a decrease in self-reported urge to eat and binge eating |
| Van den Eynde et al., 2011 [34] | RCT | 33 females with BN 3 | Left DLPFC Manual targeting | 1 session, 20 × 5 s trains/55 s inter-train interval, 10 Hz, intensity of 110% MT, 1000 pulses over 20 min | No differences between the real and sham groups on stroop task |
| Van den Eynde et al., 2011 [35] | RCT | 38 females with BN 3 | Left DLPFC Manual targeting | 1 session, 20 × 5 s trains/55 s inter-train interval, 10 Hz, intensity of 110% MT, 1000 pulses over 20 min | TMS did not alter blood pressure or heart rate |
| Claudino et al., 2011 [36] | RCT | 22 patients (11 real, 11 sham) with BN 3 | Left DLPFC Manual targeting | 1 session, 20 × 5 s trains/55 s inter-train interval, 10 Hz, intensity of 110% MT, 1000 pulses over 20 min | Decreased salivary cortisol concentrations compared with sham rTMS |
| Van den Eynde et al., 2012 [37] | Case series | 7 left-handed females with BN | Left DLPFCM anual targeting | 1 session, 20 × 5 s trains/55 s inter-train interval, 10 Hz, intensity of 110% MT, 1000 pulses over 20 min | Different effects in left- and right-handed people |
| Downar et al., 2012 [38] | Case report | One woman with severe refractory BN and depression | DMPFC Neuronavigation | 2 × 20 sessions 60 trains of 10 Hz stimulation at 120% of resting motor threshold in 5 s trains with a 10-s inter-train interval | Significant improvement in BN symptoms |
| Baczynski et al., 2014 [39] | Case report | One woman with BED and comorbid depression | Left DLPFC Manual targeting | 20 sessions 20 × 4 s trains/26 s inter-train interval, 10 Hz, intensity of 110% MT | Improvement in binge eating scale |
| Dunlop, 2015 [40] | Case series | 28 subjects with anorexia nervosa, binge-purge subtype or bulimia nervosa | DMPFC Neuronavigation | 20–30 sessions 120% resting MT, at 10 Hz, 5 s on, 10 s off, 3000 pulses/hemisphere, with left then right lateralized coil orientation | Enhanced frontostriatal connectivity was associated with responders to DMPFC-rTMS for binge/purge behavior |
| Sutoh et al., 2016 [41] | Case series (pilot study) | 8 women with BN | Left DLPFC Manual targeting | 1 session, 15 × 5 s trains/55 s inter-train interval, 10 Hz, intensity of 110% MT, 1000 pulses over 20 min within each session | Significant reduction of food craving and decrease in cerebral oxygenation of the left DLPFC |
| Gay et al., 2016 [42] | RCT | 47 women (23 real, 24 sham) with BN 4 | Left DLPFC Manual targeting | 10 sessions, 20 × 5 s trains/55 s inter-train interval, 10 Hz intensity of 110% MT, 1000 pulses over 20 min within each session | No significant improvement of bingeing or purging |
| Guillaume et al., 2018 [43] | RCT | 39 patients (22 real, 17 sham) with BN 4 | Left DLPFC Manual targeting | 10 sessions, 20 × 5 s trains/55 s inter-train interval, 10 Hz, intensity of 110% MT | Improvement of inhibitory control and decision-making |
| Reference | Type of Study | Participants | Modulation Target | Treatment Characteristics | Main Results |
|---|---|---|---|---|---|
| Khedr et al., 2014 [55] | Open-label, single arm study (pilot study) | 7 patients with AN | Left DLPFC | 10 sessions Anodal tDCS for 25 min at 2 mA (15 s ramp in and 15 s ramp out) | Immediate improvement in 3 patients after the sessions on eating and depressive symptoms, with one patient maintaining the response at 1 month |
| Burgess et al., 2016 [58] | RCT (proof-of-concept study) | 30 participants with BED | Right DLPFC | 1 session, 2 mA, 20 min | Decreased craving for sweets, savory proteins, and an all-foods category, with strongest reductions in men |
| Kekic et al., 2017 [59] | RCT | 39 patients (2 male) with BN | Right and left DLPFC (3 montages: AR/CL; AL/CR; sham) | 1 session 20 min, 2 mA, 10 s ramp on/off | Reduction in ED cognitions with AR/CL tDCS Suppression of urge to binge-eat and increased self-regulatory control with both active montages Improvement of mood with AR/CL |
| Sreeraj et al., 2018 [60] | Case report | 37 year old female with schizophrenia and binge-eating | Right DLPFC | 10 sessions, 2 mA, 30 min | Improvement in subjective reporting on cognitive restraint and control over eating as well as feeling of satiation and ability to eat after exposure to cues 3 kg weight loss by the end of the treatment, 7 kg at 10-month follow-up |
| Strumila et al., 2019 [56] | Open-label study | 10 females with AN | Anode over left DLPFC and cathode over right DLPFC | 20 sessions of anodal 2 mA stimulation during a period of two weeks | Improvement of anorexic and depressive symptoms |
| Reference | Type of Study | Participants | Modulation Target | Treatment Characteristics | Main Results |
|---|---|---|---|---|---|
| Anorexia Nervosa | |||||
| Davis et al., 1961 [65] | Case report | 12-year-old girl with AN-R | - | 12 sessions (bilateral) | Weight gain and discharge |
| Bernstein et al., 1964 [66] | Case report | 20-year-old female with AN-R and personality disorder | - | 21 sessions followed by maintenance ECT | Weight gain and mood improvement |
| Bernstein et al., 1972 [67] | Case report | 94-year-old female with AN-R and psychotic disorder | - | 5 sessions | Short term weight gain |
| Ferguson et al., 1993 [68] | Case series | 3 patients with AN and MDD | - | 11, 8 and 16 sessions (bilateral) | Transient improvement on weight and symptomatology for 2/3 patients |
| Bek et al., 1996 [69] | Case series | 8 females with AN, one had psychosis and five had personality disorders | - | 11 sessions | Modest weight gain |
| Hill et al., 2001 [70] | Case report | 77-year-old female with AN-R and MDD | - | 9 sessions | Modest weight gain and mood improvement |
| Poutanen et al., 2009 [71] | Case report | 21-year-old female with AN-B/P and MDD | - | 45 sessions in three courses (bilateral) | Modest thymic and eating amelioration. Cognitive impairment. |
| Andrews et al., 2014 [72] | Case report | 17-year-old with AN-B/P, MDD, and NSSI | - | 10 unilateral and 21 bilateral sessions/13 weeks | Mood improvement |
| Andersen et al., 2017 [73] | Case report | 14-year-old girl with AN-R, MDD, and GAD | - | 22 sessions (bilateral) | Weight gain |
| Saglam et al., 2018 [74] | Case report | 24-year-old male with AN-B/P, OCD, and MDD | - | 12 sessions (bitemporal) | Weight restoration and OCD improvement, stopped diuretic and laxative abuse. |
| Pacillio et al., 2019 [61] | Case report | 30-year-old female patient with AN and MDD | - | 11 sessions (unilateral) | Modest increase of eating disorder, mood improvement |
| Naguy et al., 2019 [63] | Case report | 16-year-old female with AN and personality disorder | - | 6 sessions (bitemporal) | Weight gain and improvement in eating behavior |
| Duriez et al., 2020 [75] | Case report | 19-year-old female with AN | - | 10 sessions | No improvement of AN symptoms |
| Shilton et al., 2020 [62] | Case series | 30 female adolescents with AN and MDD | - | - | Mood improvement, treatment well tolerated, no specific improvement for eating disorder symptoms |
| Bulimic Disorders (Bulimia and/or Binge Eating Disorders) | |||||
| Rapinesi et al., 2013 [76] | Case report | 41-year-old male with BED and bipolar disorder. Personal history of AN | - | 8 sessions (bitemporal) | Important weight loss and decrease of psychotic symptoms |
| Reference | Type of Study | Participants | Modulation Target | Treatment Characteristics * | Main Results |
|---|---|---|---|---|---|
| Anorexia Nervosa | |||||
| Israël et al., 2010 [88] | Case report | 56-year-old female with AN and severe depression | SCC (bilateral) | Intermittent stimulation 2 min on/1 min off 5 mA/91 µs/130 Hz | Maintenance of normal BMI (average 19.1 kg/m2) at 3 years, normal scores in restraint and weight and shape concerns |
| Barbier et al., 2011 [89] | Case report | 39-year-old female with AN and severe OCD | ALIC and BNST (bilateral) | Unknown | Full recovery of AN and strong improvement of OCD |
| McLaughlin et al., 2012 [90] | Case report | 52-year-old female with refractory OCD and AN | Ventral capsule and ventral striatum (bilateral) | Left unilateral, monopolar 7.5 V/120 µs/120 Hz | Significant weight improvement, reduction in AN-related obsession and patient can go out to eat |
| Wu et al., 2013 and Sun et al., 2012 [94,99] | Case series | 4 females with AN (3 OCD, 1 GAD) 1 | NAcc (bilateral) | Unknown | Full remission of AN, restoration of menstrual cycle and return to school for 3 patients |
| Wang et al., 2013 [95] | Case series | 2 females with AN, depression, and OCD | NAcc (bilateral) | 2.5–3.8 V/120–210 µs/135–185 Hz | Significant weight gain and affective improvement |
| Lipsman et al., 2013 [96] | Open label clinical trial | 6 females with AN, 5 with psychiatric comorbidities (MDD, OCD, SUD, PTSD) 2 | SCC (bilateral) | 5–7 V/90 µs/130 Hz | Weight gain in 3 patients, changes in brain metabolism |
| Hayes et al., 2015 [100] | Ancillary Study | 8 females with AN, 7 with psychiatric comorbidities (MDD, OCD, GAD, PTSD, BPD) 2 | SCC (bilateral) | Unknown | Weight loss in 3 patients, weight gain in 5 patients |
| Lipsman et al., 2017 [93] | Open label clinical trial | 16 females with AN, 14 with psychiatric comorbidities (MDD, OCD, SUD, PTSD, GAD, BPD) 2 | SCC (bilateral) | 5–6.5 V/90 µs/130 Hz | Significant weight gain for 8 patients Adverse effects: 1 surgical-site infection, 2 devices explanted at patient request, 1 seizure |
| Blomstedt et al., 2017 [91] | Case report | 60-year-old female with AN and depression | MFB (bilateral) and subsequent BNST (bilateral) | Bipolar MFB stimulation 3 V/60 µs/130 Hz two years later: monopolar BNST stimulation 4.3 V/120 µs/130 Hz | Improvement of affective symptoms Weight stabilization Target change due to blurred vision |
| Manuelli et al., 2019 [101] | Case report | 37-year-old female with AN-BP | BNST (bilateral) | 4 V/60 µs/130 Hz | Full weight restoration after 4 months |
| Wei Liu et al., 2020 [98] | Open label clinical trial | 29 females with AN, 28 with psychiatric comorbidities (12 MDD, 9 OCD, 7 GAD) | NAcc (bilateral) | 2.5–4 V/120–150 µs/160–180 Hz | 12 patients obtained full weight restoration and 5 significant weight increase after 2 years of follow up Less effective with AN-BP than AN-R |
| Martinez et al., 2020 [102] | Open label clinical trial 3 | 7 female and 1 male with AN, 4 with affective disorder and 4 with anxiety disorder as main psychiatric comorbidities | SCC (bilateral) or NAcc (bilateral) | 7–8 mA/90 µs/130 Hz | No weight gain. Subjective improvement of quality of life |
| Bulimic Disorders (Bulimia and/or Binge Eating Disorders) | |||||
| Whiting et al., 2013 [103] | Case series | 3 patients with BED | LHA (bilateral) | Monopolar unknown V/90 µs/185 Hz | 1/3 significantly improvement in binge eating Significant weight loss in 2/3 |
| Tronnier et al., 2018 [104] | Case report | 47-year-old female with BED and severe depression | NAcc (bilateral) | Bipolar 3 V/90 µs/130 Hz | Weight loss (2.8 kg/month), affective improvement and decrease of binge eating behaviors |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duriez, P.; Bou Khalil, R.; Chamoun, Y.; Maatoug, R.; Strumila, R.; Seneque, M.; Gorwood, P.; Courtet, P.; Guillaume, S. Brain Stimulation in Eating Disorders: State of the Art and Future Perspectives. J. Clin. Med. 2020, 9, 2358. https://doi.org/10.3390/jcm9082358
Duriez P, Bou Khalil R, Chamoun Y, Maatoug R, Strumila R, Seneque M, Gorwood P, Courtet P, Guillaume S. Brain Stimulation in Eating Disorders: State of the Art and Future Perspectives. Journal of Clinical Medicine. 2020; 9(8):2358. https://doi.org/10.3390/jcm9082358
Chicago/Turabian StyleDuriez, Philibert, Rami Bou Khalil, Yara Chamoun, Redwan Maatoug, Robertas Strumila, Maude Seneque, Philip Gorwood, Philippe Courtet, and Sébastien Guillaume. 2020. "Brain Stimulation in Eating Disorders: State of the Art and Future Perspectives" Journal of Clinical Medicine 9, no. 8: 2358. https://doi.org/10.3390/jcm9082358