Effect of the COVID-19 Pandemic on Treatment Delays in Patients with ST-Segment Elevation Myocardial Infarction

 , ,
, ,
Abstract
:1. Introduction
2. Methods
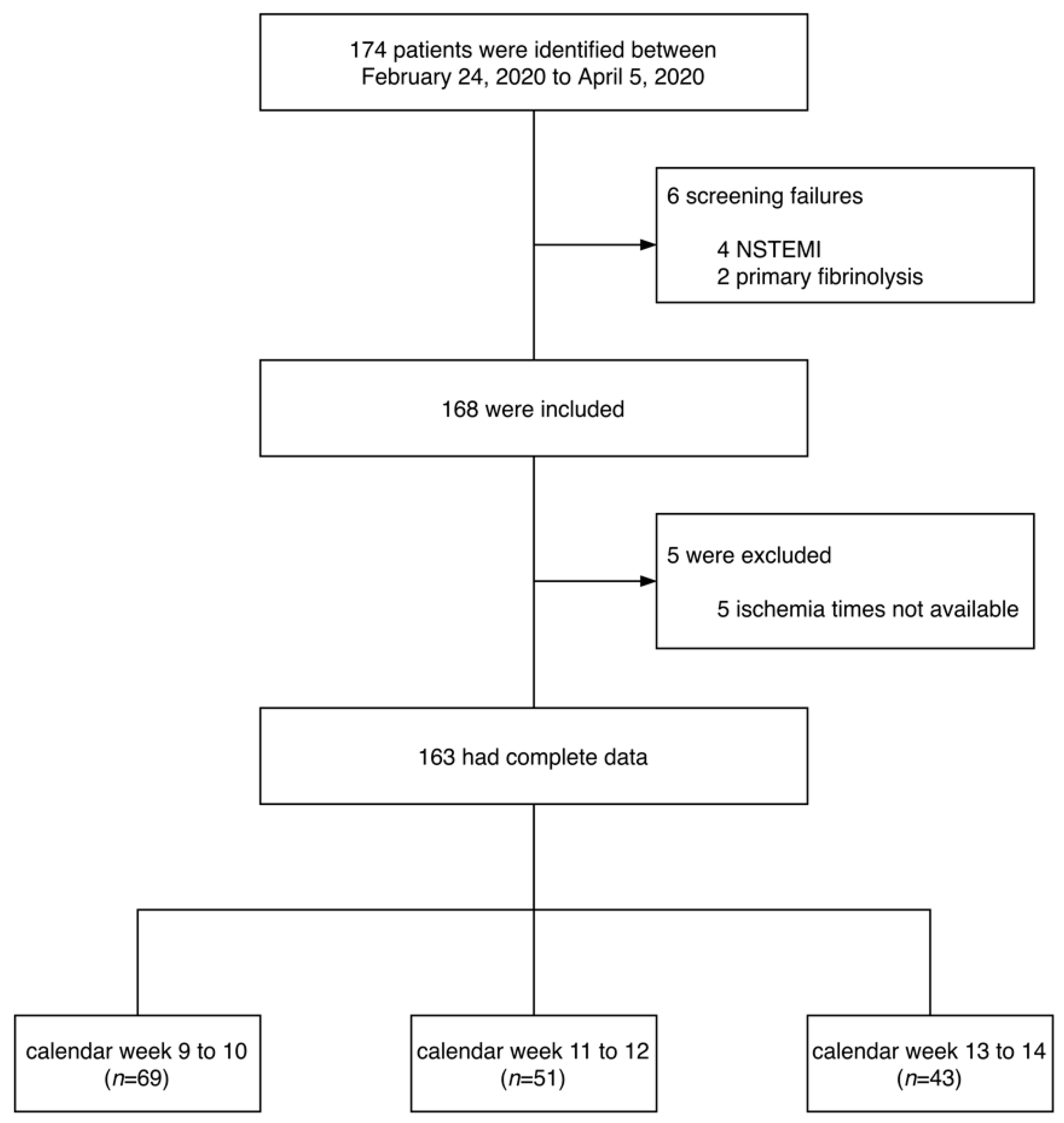
2.1. Study Design and Population
2.2. Data Collection and Study Objectives
2.3. Statistical Analysis
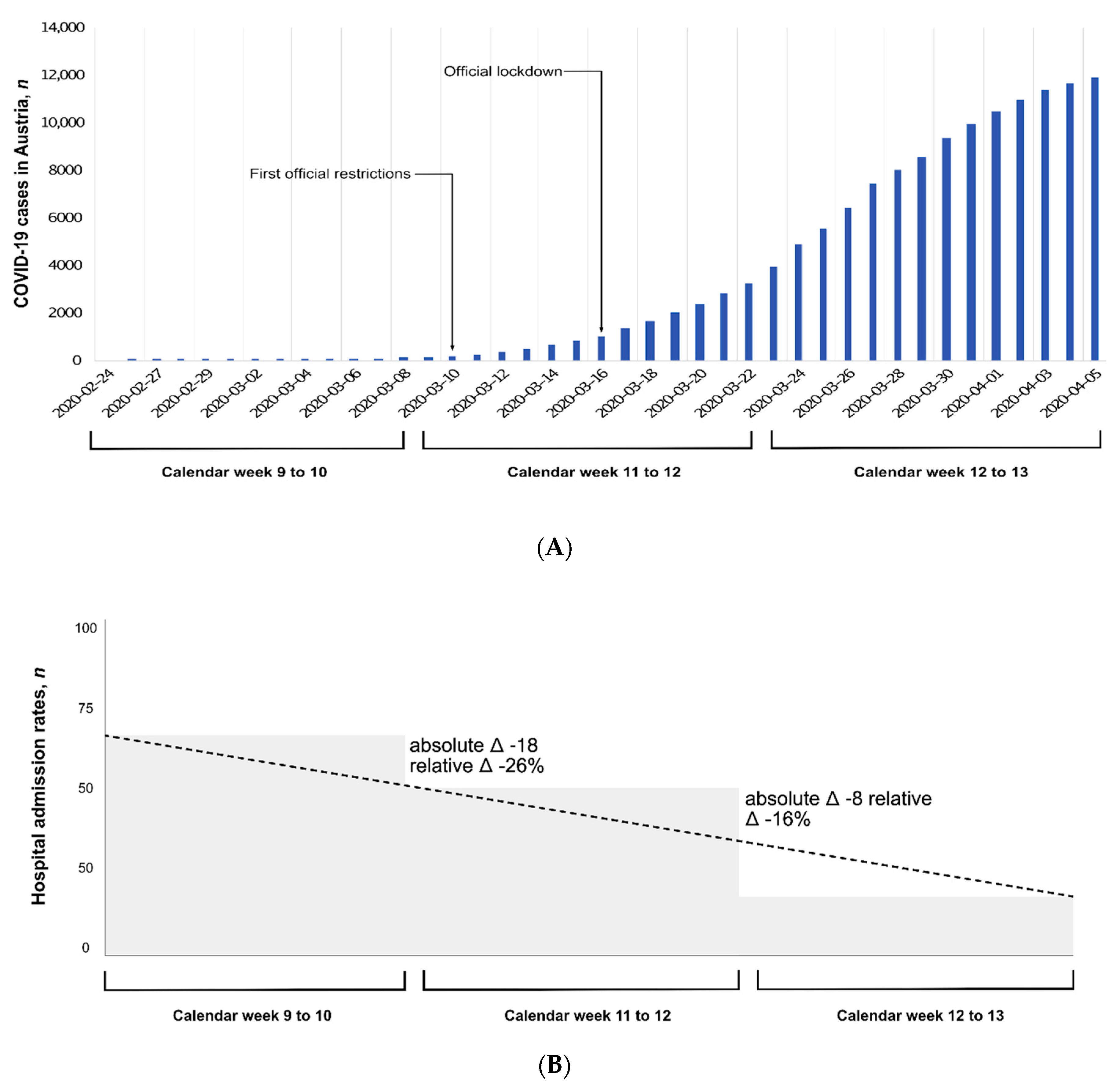
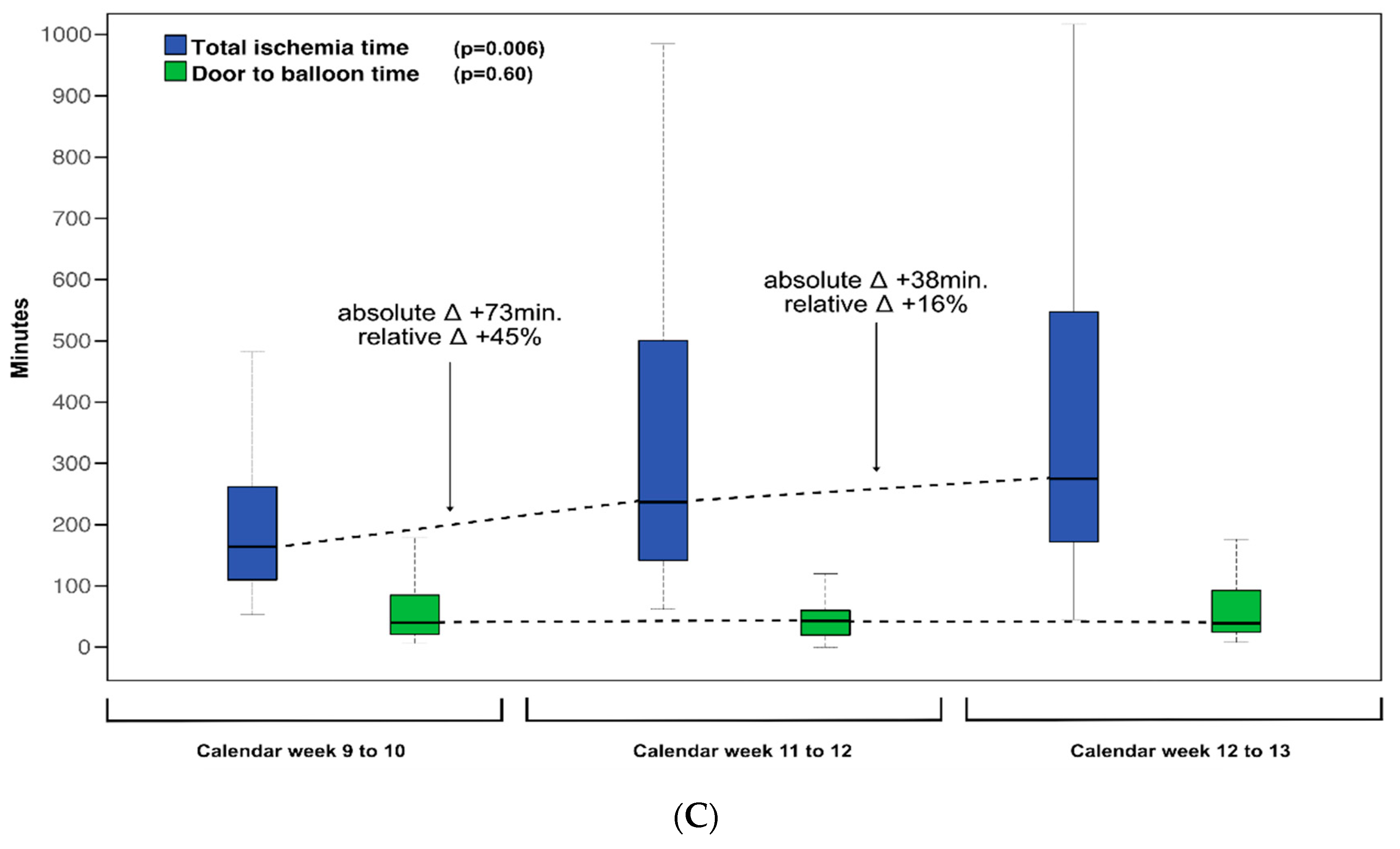
3. Results
3.1. Demographic and Clinical Characteristics
3.2. Angiographic and Troponin Findings
3.3. Adverse Events
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.C.; et al. China Medical Treatment Expert Group for C. Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Verity, R.; Okell, L.C.; Dorigatti, I.; Winskill, P.; Whittaker, C.; Imai, N.; Cuomo-Dannenburg, G.; Thompson, H.; Walker, P.G.T.; Fu, H.; et al. Estimates of the severity of coronavirus disease 2019: A model-based analysis. Lancet Infect. Dis. 2020, 20, 669–677. [Google Scholar] [CrossRef]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline Characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to ICUs of the Lombardy Region, Italy. JAMA 2020, 323, 1574–1581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ren, B.; Yan, F.; Deng, Z.; Zhang, S.; Xiao, L.; Wu, M.; Cai, L. Extremely high incidence of lower extremity deep venous thrombosis in 48 patients with severe COVID-19 in Wuhan. Circulation 2020. [Google Scholar] [CrossRef]
- Helmy, Y.A.; Fawzy, M.; Elaswad, A.; Sobieh, A.; Kenney, S.P.; Shehata, A.A. The COVID-19 pandemic: A comprehensive review of taxonomy, genetics, epidemiology, diagnosis, treatment, and control. J. Clin. Med. 2020, 9, 1225. [Google Scholar] [CrossRef]
- Sardu, C.; Gambardella, J.; Morelli, M.B.; Wang, X.; Marfella, R.; Santulli, G. Hypertension, thrombosis, kidney failure, and diabetes: Is COVID-19 an endothelial disease? A comprehensive evaluation of clinical and basic evidence. J. Clin. Med. 2020, 9, 1417. [Google Scholar] [CrossRef]
- The American Heart Association′s Get With The Guidelines-Coronary Artery Disease Advisory Work Group and Mission: Lifeline Program; The American Heart Association′s Council On Clinical Cardiology; The American Heart Association′s Council On Clinical Cardiology′s Committee On Acute Cardiac Care and General Cardiology Committee; The American Heart Association′s Council On Clinical Cardiology′s Committee Interventional Cardiovascular Care Committee. Temporary emergency guidance to STEMI systems of care during the COVID-19 pandemic: AHA′s mission: Lifeline. Circulation 2020. published online ahead of print. [Google Scholar] [CrossRef]
- Anderson, J.L.; Morrow, D.A. Acute myocardial infarction. N. Engl. J. Med. 2017, 376, 2053–2064. [Google Scholar] [CrossRef] [Green Version]
- Chan, M.Y.; Sun, J.L.; Newby, L.K.; Shaw, L.K.; Lin, M.; Peterson, E.D.; Califf, R.M.; Kong, D.F.; Roe, M.T. Long-term mortality of patients undergoing cardiac catheterization for ST-elevation and non-ST-elevation myocardial infarction. Circulation 2009, 119, 3110–3117. [Google Scholar] [CrossRef]
- Thiele, H.; Kappl, M.J.; Linke, A.; Erbs, S.; Boudriot, E.; Lembcke, A.; Kivelitz, D.; Schuler, G. Influence of time-to-treatment, TIMI-flow grades, and ST-segment resolution on infarct size and infarct transmurality as assessed by delayed enhancement magnetic resonance imaging. Eur. Heart J. 2007, 28, 1433–1439. [Google Scholar] [CrossRef] [Green Version]
- Eitel, I.; Desch, S.; Fuernau, G.; Hildebrand, L.; Gutberlet, M.; Schuler, G.; Thiele, H. Prognostic significance and determinants of myocardial salvage assessed by cardiovascular magnetic resonance in acute reperfused myocardial infarction. J. Am. Coll. Cardiol. 2010, 55, 2470–2479. [Google Scholar] [CrossRef] [PubMed]
- Reindl, M.; Eitel, I.; Reinstadler, S.J. Role of cardiac magnetic resonance to improve risk prediction following acute ST-elevation myocardial infarction. J. Clin. Med. 2020, 9, 1041. [Google Scholar] [CrossRef] [Green Version]
- Tam, C.F.; Cheung, K.S.; Lam, S.; Wong, A.; Yung, A.; Sze, M.; Lam, Y.M.; Chan, C.; Tsang, T.C.; Tsui, M.; et al. Impact of coronavirus disease 2019 (COVID-19) outbreak on ST-segment-elevation myocardial infarction care in Hong Kong, China. Circ. Cardiovasc. Qual. Outcomes 2020, 13, e006631. [Google Scholar] [CrossRef] [PubMed]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [PubMed] [Green Version]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D.; Group ESCSD. Fourth universal definition of myocardial infarction (2018). Eur. Heart J. 2019, 40, 237–269. [Google Scholar] [CrossRef] [Green Version]
- Bhatt, D.L. Timely PCI for STEMI—Still the treatment of choice. N. Engl. J. Med. 2013, 368, 1446–1447. [Google Scholar] [CrossRef]
- Mehta, R.H.; Harjai, K.J.; Cox, D.; Stone, G.W.; Brodie, B.; Boura, J.; O′Neill, W.; Grines, C.L. Primary angioplasty in myocardial infarction I. Clinical and angiographic correlates and outcomes of suboptimal coronary flow inpatients with acute myocardial infarction undergoing primary percutaneous coronary intervention. J. Am. Coll. Cardiol. 2003, 42, 1739–1746. [Google Scholar] [CrossRef] [Green Version]
- Mehta, R.H.; Ou, F.S.; Peterson, E.D.; Shaw, R.E.; Hillegass, W.B., Jr.; Rumsfeld, J.S.; Roe, M.T. American College of Cardiology-National Cardiovascular Database Registry I. Clinical significance of post-procedural TIMI flow in patients with cardiogenic shock undergoing primary percutaneous coronary intervention. JACC Cardiovasc. Interv. 2009, 2, 56–64. [Google Scholar] [CrossRef] [Green Version]
- Metzler, B.; Siostrzonek, P.; Binder, R.K.; Bauer, A.; Reinstadler, S.J. Decline of acute coronary syndrome admissions in Austria since the outbreak of COVID-19: The pandemic response causes cardiac collateral damage. Eur. Heart J. 2020, 41, 1852–1853. [Google Scholar] [CrossRef] [Green Version]
- Herrmann, H.C.; Lu, J.; Brodie, B.R.; Armstrong, P.W.; Montalescot, G.; Betriu, A.; Neuman, F.J.; Effron, M.B.; Barnathan, E.S.; Topol, E.J.; et al. Benefit of facilitated percutaneous coronary intervention in high-risk ST-segment elevation myocardial infarction patients presenting to nonpercutaneous coronary intervention hospitals. JACC Cardiovasc. Interv. 2009, 2, 917–924. [Google Scholar] [CrossRef] [Green Version]
- Denktas, A.E.; Athar, H.; Henry, T.D.; Larson, D.M.; Simons, M.; Chan, R.; Niles, N.W.; Thiele, H.; Schuler, G.; Ahn, C.; et al. Reduced-dose fibrinolytic acceleration of ST-segment elevation myocardial infarction treatment coupled with urgent percutaneous coronary intervention compared to primary percutaneous coronary intervention alone results of the AMICO (Alliance for Myocardial Infarction Care Optimization) Registry. JACC Cardiovasc. Interv. 2008, 1, 504–510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhatt, D.L.; Flather, M.D.; Hacke, W.; Berger, P.B.; Black, H.R.; Boden, W.E.; Cacoub, P.; Cohen, E.A.; Creager, M.A.; Easton, J.D.; et al. Patients with prior myocardial infarction, stroke, or symptomatic peripheral arterial disease in the CHARISMA trial. J. Am. Coll. Cardiol. 2007, 49, 1982–1988. [Google Scholar] [CrossRef] [PubMed]
- Solhpour, A.; Chang, K.W.; Arain, S.A.; Balan, P.; Loghin, C.; McCarthy, J.J.; Anderson, H.V.; Smalling, R.W. Ischemic time is a better predictor than door-to-balloon time for mortality and infarct size in ST-elevation myocardial infarction. Catheter. Cardiovasc. Interv. 2016, 87, 1194–1200. [Google Scholar] [CrossRef] [PubMed]
- Daniels, M.J.; Cohen, M.G.; Bavry, A.A.; Kumbhani, D.J. Reperfusion of ST-segment-elevation myocardial infarction in the COVID-19 era: Business as usual? Circulation 2020, 141, 1948–1950. [Google Scholar] [CrossRef] [Green Version]
- Kwong, J.C.; Schwartz, K.L.; Campitelli, M.A. Acute myocardial infarction after laboratory-confirmed influenza infection. N. Engl. J. Med. 2018, 378, 2540–2541. [Google Scholar] [CrossRef]
- Garcia, S.; Albaghdadi, M.S.; Meraj, P.M.; Schmidt, C.; Garberich, R.; Jaffer, F.A.; Dixon, S.; Rade, J.J.; Tannenbaum, M.; Chambers, J.; et al. Reduction in ST-segment elevation cardiac catheterization laboratory activations in the United States during COVID-19 pandemic. J. Am. Coll. Cardiol. 2020, 75, 2871–2872. [Google Scholar] [CrossRef] [PubMed]
- Willich, S.N.; Lewis, M.; Lowel, H.; Arntz, H.R.; Schubert, F.; Schroder, R. Physical exertion as a trigger of acute myocardial infarction. Triggers and mechanisms of myocardial infarction study group. N. Engl. J. Med. 1993, 329, 1684–1690. [Google Scholar] [CrossRef] [PubMed]
- Widimsky, P.; Wijns, W.; Fajadet, J.; De Belder, M.; Knot, J.; Aaberge, L.; Andrikopoulos, G.; Baz, J.A.; Betriu, A.; Claeys, M.; et al. Reperfusion therapy for ST elevation acute myocardial infarction in Europe: Description of the current situation in 30 countries. Eur. Heart J. 2010, 31, 943–957. [Google Scholar] [CrossRef] [Green Version]
- Gorenek, B.; Blomstrom Lundqvist, C.; Brugada Terradellas, J.; Camm, A.J.; Hindricks, G.; Huber, K.; Kirchhof, P.; Kuck, K.H.; Kudaiberdieva, G.; Lin, T.; et al. Cardiac arrhythmias in acute coronary syndromes: Position paper from the joint EHRA, ACCA, and EAPCI task force. EP Europace 2014, 16, 1655–1673. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Total Population (n = 163) |
|---|---|
| Age, years (IQR) | 61 (55–74) |
| Female, n (%) | 44 (27) |
| Body weight, kg (IQR) | 81 (70–90) |
| Height, cm (IQR) | 174 (168–180) |
| Body mass index, kg/m2 (IQR) | 26.7 (24.2–29.8) |
| Diabetes mellitus, n (%) | 32 (20) |
| Current smoker, n (%) | 71 (44) |
| Hypercholesterolemia, n (%) | 132 (81) |
| Hypertension, n (%) | 103 (63) |
| Previous myocardial infarction, n (%) | 21 (13) |
| Previous diagnosis of CCS, n (%) | 34 (21) |
| Previous CABG, n (%) | 5 (3) |
| Heart rate, bpm (IQR) | 73 (62–91) |
| Sinus rhythm, n (%) | 146 (90) |
| Systolic blood pressure, mmHg (IQR) | 130 (110–150) |
| Diastolic blood pressure, mmHg (IQR) | 75 (64–90) |
| Killip class >I, n (%) | 50 (31) |
| Peak troponin, x-fold increase of ULN (IQR) | 271 (108–578) |
| Total ischemic time, min (IQR) | 201 (130–405) |
| Door-to-balloon time, min (IQR) | 40 (21–81) |
| Culprit lesion, n (%) | |
| RCA | 58 (36) |
| LAD | 78 (48) |
| LCX | 19 (12) |
| RI | 2 (1) |
| LM | 5 (3) |
| Bypass graft | 1 (1) |
| Pre-interventional TIMI flow grade 0, n (%) | 95 (58) |
| Post-interventional TIMI flow grade 3, n (%) | 145 (89) |
| Calendar week 9–10 (n = 69, 42%) | Calendar week 11–12 (n = 51, 31%) | Calendar week 13–14 (n = 43, 26%) | p-Value | |
|---|---|---|---|---|
| Age, years (IQR) | 61 (54–72) | 63 (55–76) | 60 (56–71) | 0.60 |
| Female, n (%) | 21 (30) | 12 (24) | 11 (26) | 0.68 |
| Body weight, kg (IQR) | 80 (70–90) | 80 (70–90) | 85 (73–99) | 0.26 |
| Height, cm (IQR) | 174 (165–180) | 176 (169–180) | 172 (166–178) | 0.26 |
| Body mass index, kg/m2 (IQR) | 26.3 (24.2–29.5) | 26.1 (23.6–28.7) | 28.1 (24.4–31.8) | 0.11 |
| Diabetes mellitus, n (%) | 13 (19) | 8 (16) | 11 (26) | 0.44 |
| Current smoker, n (%) | 27 (39) | 24 (47) | 20 (47) | 0.63 |
| Hypercholesterolemia, n (%) | 55 (80) | 40 (78) | 37 (86) | 0.46 |
| Hypertension, n (%) | 45 (65) | 31 (61) | 27 (63) | 0.85 |
| Previous myocardial infarction, n (%) | 8 (12) | 8 (16) | 5 (12) | 0.67 |
| Previous diagnosis of CCS, n (%) | 16 (23) | 13 (25) | 5 (12) | 0.31 |
| Previous CABG, n (%) | 2 (3) | 2 (4) | 1 (2) | 0.91 |
| Heart rate, bpm (IQR) | 74 (65–90) | 70 (60–85) | 78 (60–97) | 0.52 |
| Sinus rhythm, n (%) | 59 (86) | 47 (92) | 40 (93) | 0.48 |
| Systolic blood pressure, mmHg (IQR) | 135 (108–151) | 127 (108–140) | 130 (114–152) | 0.44 |
| Diastolic blood pressure, mmHg (IQR) | 74 (62–90) | 75 (65–89) | 80 (64–94) | 0.64 |
| Killip class > I, n (%) | 20 (29) | 16 (31) | 14 (33) | 0.85 |
| Peak troponin, x-fold increase of ULN (IQR) | 268 (138–580) | 295 (85–636) | 272 (108–255) | 0.97 |
| Total ischemic time, min (IQR) | 164 (107–281) | 237 (141–560) | 275 (170–590) | 0.006 |
| Door-to-balloon time, min (IQR) | 40 (21–85) | 43 (20–60) | 39 (24–94) | 0.60 |
| Culprit lesion, n (%) | 0.34 | |||
| RCA | 23 (33) | 18 (35) | 17 (40) | |
| LAD | 35 (51) | 23 (45) | 20 (46) | |
| LCX | 9 (13) | 6 (12) | 4 (9) | |
| RI | 0 (0) | 0 (0) | 2 (5) | |
| LM | 2 (3) | 3 (6) | 0 (0) | |
| Bypass graft | 0 (0) | 1 (2) | 0 (0) | |
| Pre-interventional TIMI flow 0, n (%) | 39 (57) | 28 (55) | 28 (65) | 0.60 |
| Post-interventional TIMI flow 3, n (%) | 67 (97) | 43 (84) | 35 (81) | 0.02 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reinstadler, S.J.; Reindl, M.; Lechner, I.; Holzknecht, M.; Tiller, C.; Roithinger, F.X.; Frick, M.; Hoppe, U.C.; Jirak, P.; Berger, R.; et al. Effect of the COVID-19 Pandemic on Treatment Delays in Patients with ST-Segment Elevation Myocardial Infarction. J. Clin. Med. 2020, 9, 2183. https://doi.org/10.3390/jcm9072183
Reinstadler SJ, Reindl M, Lechner I, Holzknecht M, Tiller C, Roithinger FX, Frick M, Hoppe UC, Jirak P, Berger R, et al. Effect of the COVID-19 Pandemic on Treatment Delays in Patients with ST-Segment Elevation Myocardial Infarction. Journal of Clinical Medicine. 2020; 9(7):2183. https://doi.org/10.3390/jcm9072183
Chicago/Turabian StyleReinstadler, Sebastian J., Martin Reindl, Ivan Lechner, Magdalena Holzknecht, Christina Tiller, Franz Xaver Roithinger, Matthias Frick, Uta C. Hoppe, Peter Jirak, Rudolf Berger, and et al. 2020. "Effect of the COVID-19 Pandemic on Treatment Delays in Patients with ST-Segment Elevation Myocardial Infarction" Journal of Clinical Medicine 9, no. 7: 2183. https://doi.org/10.3390/jcm9072183