Subacute Thyroiditis is Associated with HLA-B*18:01, -DRB1*01 and -C*04:01—The Significance of the New Molecular Background

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. HLA Typing Procedures
2.2. Statistical Analysis
2.3. Inclusion Criteria
2.4. Biochemical and Cytological Procedures
2.5. Ethics Procedures
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| CRP | C reactive protein |
| ECLIA | electrochemiluminescence immunoassay |
| ESR FT4 | erythrocyte sedimentation rate free thyroxine |
| HLA | human leukocyte antigens |
| MHC | major histocompatibility complex |
| SAT TSH | subacute thyroiditis thyroid stimulating hormone |
| US | ultrasound |
References
- Samuels, M.H. Subacute, silent, and postpartum thyroiditis. Med. Clin. N. Am. 2012, 96, 223–233. [Google Scholar] [CrossRef] [PubMed]
- Stasiak, M.; Michalak, R.; Stasiak, B.; Lewinski, A. Clinical characteristics of subacute thyroiditis is different than it used to be—Current state based on 15 years own material. Neuroendocrinol. Lett. 2019, 39, 489–495. [Google Scholar] [PubMed]
- Alfadda, A.A.; Sallam, R.M.; Elawad, G.E.; Aldhukair, H.; Alyahya, M.M. Subacute thyroiditis: Clinical presentation and long term outcome. Int. J. Endocrinol. 2014, 2014, 794943. [Google Scholar] [CrossRef] [PubMed]
- Fatourechi, V.; Aniszewski, J.P.; Fatourechi, G.Z.; Atkinson, E.J.; Jacobsen, S.J. Clinical features and outcome of subacute thyroiditis in an incidence cohort: Olmsted county, Minnesota, study. J. Clin. Endocrinol. Metab. 2003, 88, 2100–2105. [Google Scholar] [CrossRef]
- Daniels, G.H. Atypical subacute thyroiditis: Preliminary observations. Thyroid 2001, 11, 691–695. [Google Scholar] [CrossRef]
- Karachalios, G.N.; Amantos, K.; Kanakis, K.V.; Deliousis, A.; Karachaliou, I.G.; Zacharof, A.K. Subacute thyroiditis presenting as fever of unknown origin. Int. J. Clin. Pract. 2010, 64, 97–98. [Google Scholar] [CrossRef]
- Dalugama, C. Asymptomatic thyroiditis presenting as pyrexia of unknown origin: A case report. J. Med. Case Rep. 2018, 12, 51. [Google Scholar] [CrossRef] [Green Version]
- Cappelli, C.; Pirola, I.; Gandossi, E.; Formenti, A.M.; Agosti, B.; Castellano, M. Ultrasound findings of subacute thyroiditis: A single institution retrospective review. Acta Radiol. 2014, 55, 429–433. [Google Scholar] [CrossRef]
- Vural, C.; Paksoy, N.; Gök, N.D.; Yazal, K. Subacute granulomatous (De Quervain’s) thyroiditis: Fine-needle aspiration cytology and ultrasonographic characteristics of 21 cases. CytoJournal 2015, 12, 9. [Google Scholar] [CrossRef]
- Nyulassy, S.; Hnilica, P.; Stefanovic, J. The HLA system and subacute thyroiditis. A preliminary report. Tissue Antigens 1975, 6, 105–106. [Google Scholar] [CrossRef]
- Farid, N.R.; Bear, J.C. The human major histocompatibility complex and endocrine disease. Endocr. Rev. 1981, 2, 50–86. [Google Scholar] [CrossRef] [PubMed]
- Nyulassy, S.; Hnilica, P.; Buc, M.; Guman, M.; Hirschová, V.; Stefanovic, J. Subacute (de Quervain’s) thyroiditis: Association with HLA-Bw35 antigen and abnormalities of the complement system, immunoglobulins and other serum proteins. J. Clin. Endocrinol. Metab. 1977, 45, 270–274. [Google Scholar] [CrossRef] [PubMed]
- Yeo, P.P.; Chan, S.H.; Aw, T.C.; Lui, K.F.; Rauff, A.; Mathew, T.; Chang, C.H.; Doraisingham, S.; Lim, P.; Cheah, J.S. HLA and Chinese patients with subacute (De Quervain’s) thyroiditis. Tissue Antigens 1981, 17, 249–250. [Google Scholar] [CrossRef]
- Goto, H.; Uno, H.; Tamai, H.; Kuma, K.; Hayashi, Y.; Matsubayashi, S.; Sasazuki, T. Genetic analysis of subacute (de Quervain’s) thyroiditis. Tissue Antigens 1985, 26, 110–113. [Google Scholar] [CrossRef] [PubMed]
- Tamai, H.; Goto, H.; Uno, H.; Sasazuki, T.; Kuma, K.; Hayashi, Y.; Matsubayashi, S. HLA in Japanese patients with subacute (De Quervain’s) thyroiditis. Tissue Antigens 1984, 24, 58–59. [Google Scholar] [CrossRef] [PubMed]
- Rubin, R.A.; Guay, A.T. Susceptibility to subacute thyroiditis is genetically influenced: Familial occurrence in identical twins. Thyroid 1991, 1, 157–161. [Google Scholar] [CrossRef]
- Zein, E.F.; Karaa, S.E.; Megarbane, A. Familial occurrence of painful subacute thyroiditis associated with human leukocyte antigen-B35. Presse Med. 2007, 36, 808–809. [Google Scholar] [CrossRef]
- Hamaguchi, E.; Nishimura, Y.; Kaneko, S.; Takamura, T. Subacute thyroiditis developed in identical twins two years apart. Endocr. J. 2005, 52, 559–562. [Google Scholar] [CrossRef] [Green Version]
- Kramer, A.B.; Roozendaal, C.; Dullaart, R.P. Familial occurrence of subacute thyroiditis associated with human leukocyte antigen-B35. Thyroid 2004, 14, 544–547. [Google Scholar] [CrossRef]
- Ohsako, N.; Tamai, H.; Sudo, T.; Mukuta, T.; Tanaka, H.; Kuma, K.; Kimura, A.; Sasazuki, T. Clinical characteristics of subacute thyroiditis classified according to human leukocyte antigen typing. J. Clin. Endocrinol. Metab. 1995, 80, 3653–3656. [Google Scholar] [CrossRef]
- Kobayashi, N.; Tamai, H.; Nagai, K.; Matsubayashi, S.; Matsuzuka, F.; Kuma, K.; Goto, H.; Uno, H.; Sasazuki, T.; Nagataki, S. Studies on the pathogenesis of subacute thyroiditis. Nihon Naibunpi Gakkai Zasshi 1985, 61, 737–743. [Google Scholar] [PubMed] [Green Version]
- Buc, M.; Nyulassy, S.; Hnilica, P.; Busová, B.; Stefanovic, J. The frequency of HLA-Dw1 determinant in subacute (de Quervain’s) thyroiditis. Tissue Antigens 1979, 14, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Stasiak, M.; Michalak, R.; Lewinski, A. Thyroid primary and metastatic malignant tumours of poor prognosis may mimic subacute thyroiditis—Time to change the diagnostic criteria: Case reports and a review of the literature. BMC Endocr. Disord. 2019, 19, 86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stasiak, M.; Michalak, R.; Stasiak, B.; Lewiński, A. Time-lag between symptom onset and diagnosis of subacute thyroiditis—How to avoid the delay of diagnosis and unnecessary overuse of antibiotics. Horm. Metab. Res. 2019, 26. [Google Scholar] [CrossRef] [PubMed]
- Available online: www.ctht.info/Table%209%20CB%20ASSOCIATIONS.pdf (accessed on 20 December 2019).
- Cao, K.; Hollenbach, J.; Shi, X.; Shi, W.; Chopek, M.; Fernández-Viña, M.A. Analysis of the frequencies of HLA-A, B, and C alleles and alleles in the five major ethnic groups of the United States reveals high levels of diversity in these loci and contrasting distribution patterns in these populations. Hum. Immunol. 2001, 62, 1009–1030. [Google Scholar] [CrossRef]
- Stasiak, M.; Tymoniuk, B.; Adamczewski, Z.; Stasiak, B.; Lewiński, A. Sonographic pattern of subacute thyroiditis is HLA-dependent. Front. Endocrinol. (Lausanne) 2019, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stasiak, M.; Tymoniuk, B.; Stasiak, B.; Lewiński, A. The risk of recurrence of subacute thyroiditis is HLA-dependent. Int. J. Mol. Sci. 2019, 3, 20. [Google Scholar] [CrossRef] [Green Version]
- Vita, R.; Di Bari, F.; Perelli, S.; Capodicasa, G.; Benvenga, S. Thyroid vascularization is an important ultrasonographic parameter in untreated Graves’ disease patients. J. Clin. Transl. Endocrinol. 2019, 15, 65–69. [Google Scholar] [CrossRef]
- Vita, R.; Lapa, D.; Trimarchi, F.; Vita, G.; Fallahi, P.; Antonelli, A.; Benvenga, S. Certain HLA alleles are associated with stress-triggered Graves’ disease and influence its course. Endocrine 2017, 55, 93–100. [Google Scholar] [CrossRef]


{kind=link}
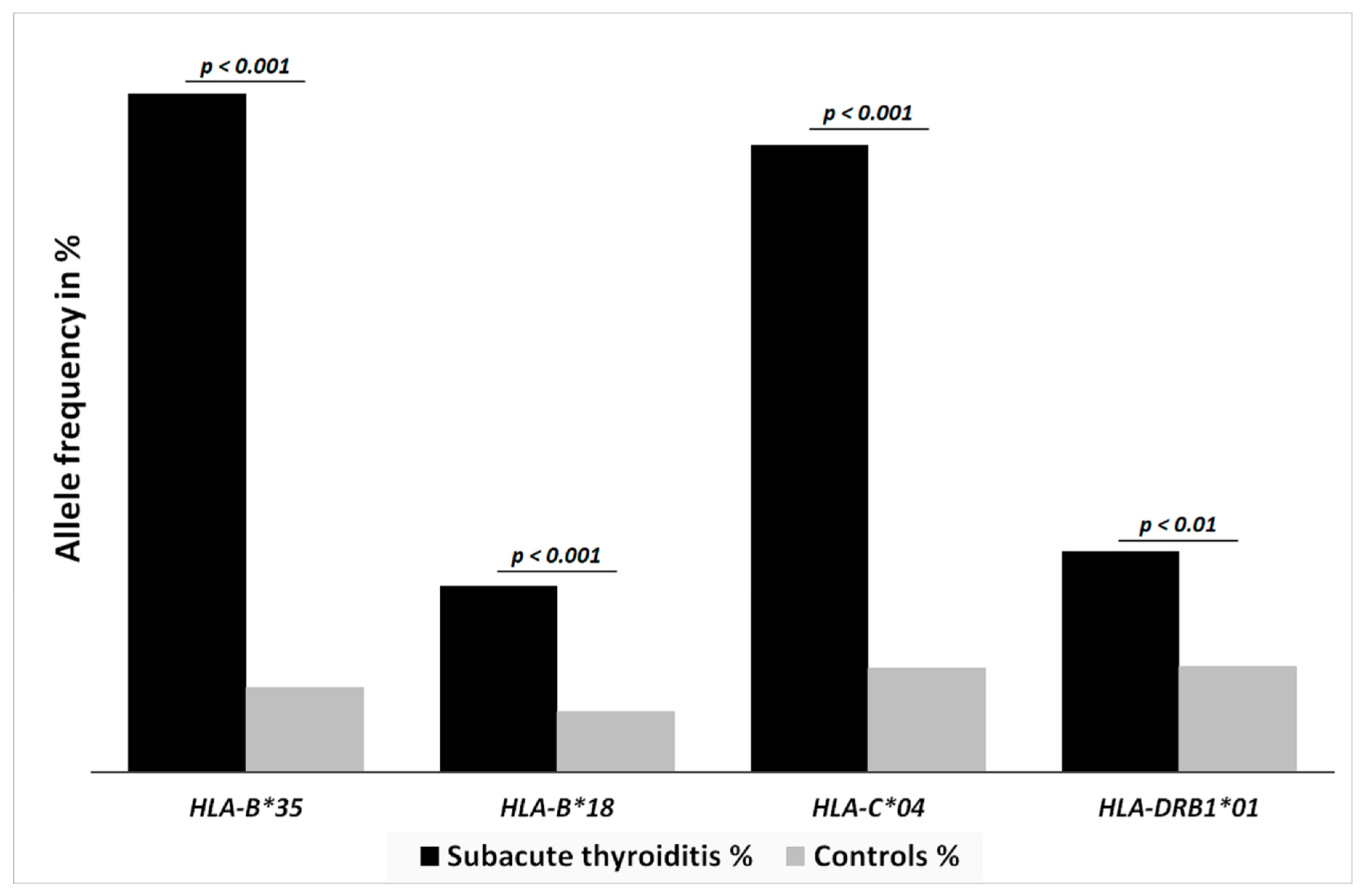
| HLA Allele | Subacute Thyroiditis % (No of Patients) | Healthy Controls % (No of Patients) | p-Value |
|---|---|---|---|
| HLA-B*35:01 | 38.8 (23) | 5.2 (53) | p < 0.0001 |
| HLA-B*35:02 | 11.7 (7) | 1.2 (12) | p < 0.0001 |
| HLA-B*35:03 | 35 (21) | 3.4 (35) | p < 0.0001 |
| HLA-B*35:08 | 3.3 (2) | 0.4 (4) | p < 0.0367 |
| HLA-B*35:01/02/03/08 | 81.7 (49) | 10.2 (104) | p < 0.0001 |
| HLA-B*18:01 | 23.3 (14) | 7.2 (74) | p = 0.0001 |
| HLA-C*04:01 | 75.5 (45) | 12.5 (128) | p < 0.0001 |
| HLA-DRB1*01:01 | 25 (15) | 12.0 (130) | p = 0.0126 |
| HLA-DRB1*01:02 | 1.7 (1) | 0.1 (1) | p = 0.2286 |
| HLA-DRB1*01:03 | 1.7 (1) | 0.1 (1) | p = 0.2286 |
| HLA-DRB1*01:01/02/03 | 28.3 (17) | 12.9 (132) | p = 0.007 |
| HLA-C*03 | 11.7 (7) | 10 (102) | p = 0.8386 |
| HLA-DRB1*08 | 6.7 (4) | 3.4 (35) | p = 0.3397 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stasiak, M.; Tymoniuk, B.; Michalak, R.; Stasiak, B.; Kowalski, M.L.; Lewiński, A. Subacute Thyroiditis is Associated with HLA-B*18:01, -DRB1*01 and -C*04:01—The Significance of the New Molecular Background. J. Clin. Med. 2020, 9, 534. https://doi.org/10.3390/jcm9020534
Stasiak M, Tymoniuk B, Michalak R, Stasiak B, Kowalski ML, Lewiński A. Subacute Thyroiditis is Associated with HLA-B*18:01, -DRB1*01 and -C*04:01—The Significance of the New Molecular Background. Journal of Clinical Medicine. 2020; 9(2):534. https://doi.org/10.3390/jcm9020534
Chicago/Turabian StyleStasiak, Magdalena, Bogusław Tymoniuk, Renata Michalak, Bartłomiej Stasiak, Marek L. Kowalski, and Andrzej Lewiński. 2020. "Subacute Thyroiditis is Associated with HLA-B*18:01, -DRB1*01 and -C*04:01—The Significance of the New Molecular Background" Journal of Clinical Medicine 9, no. 2: 534. https://doi.org/10.3390/jcm9020534