Dry Eye Disease: A Review of Epidemiology in Taiwan, and its Clinical Treatment and Merits


Abstract
:1. Introduction
2. Epidemiology
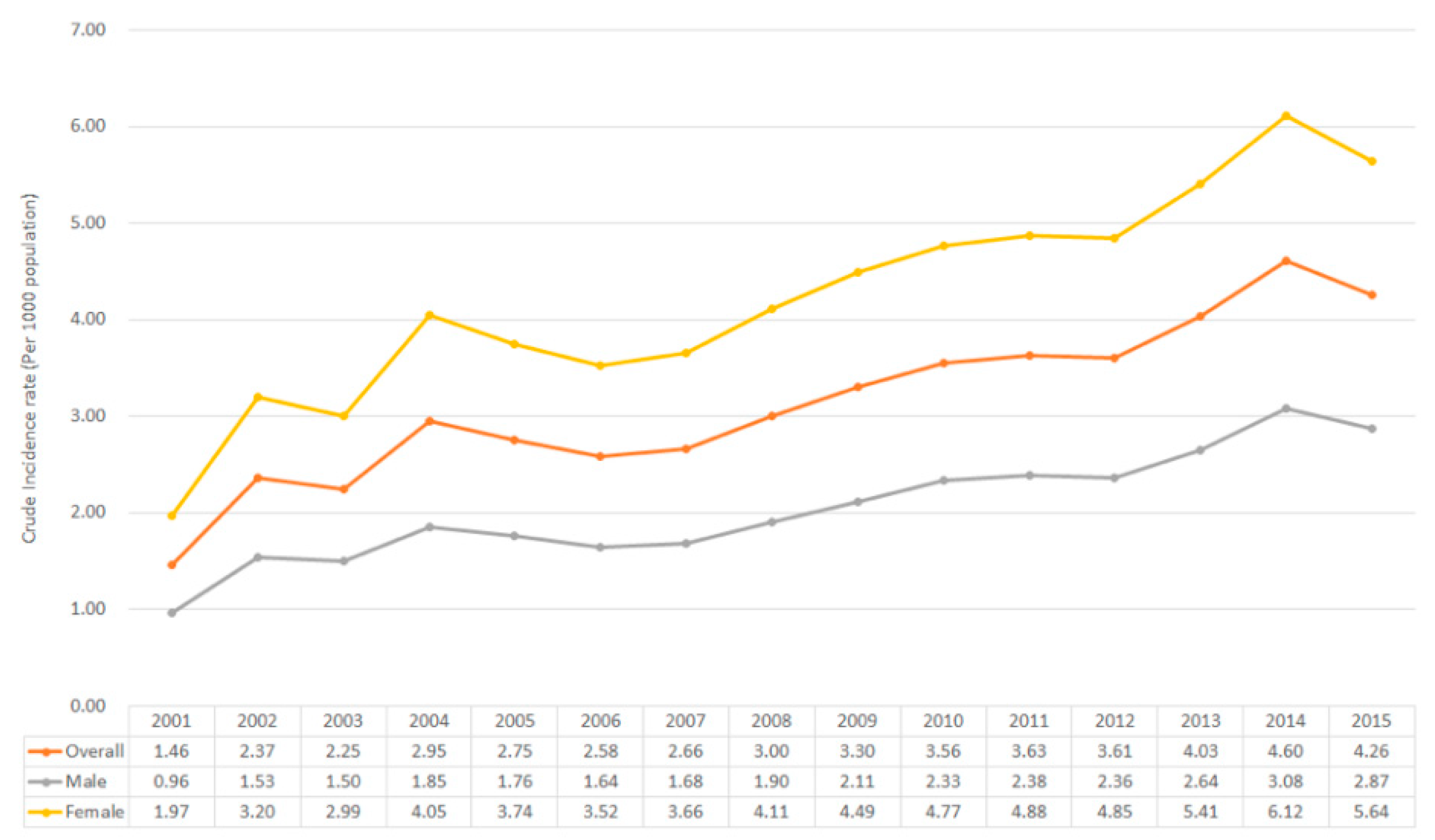
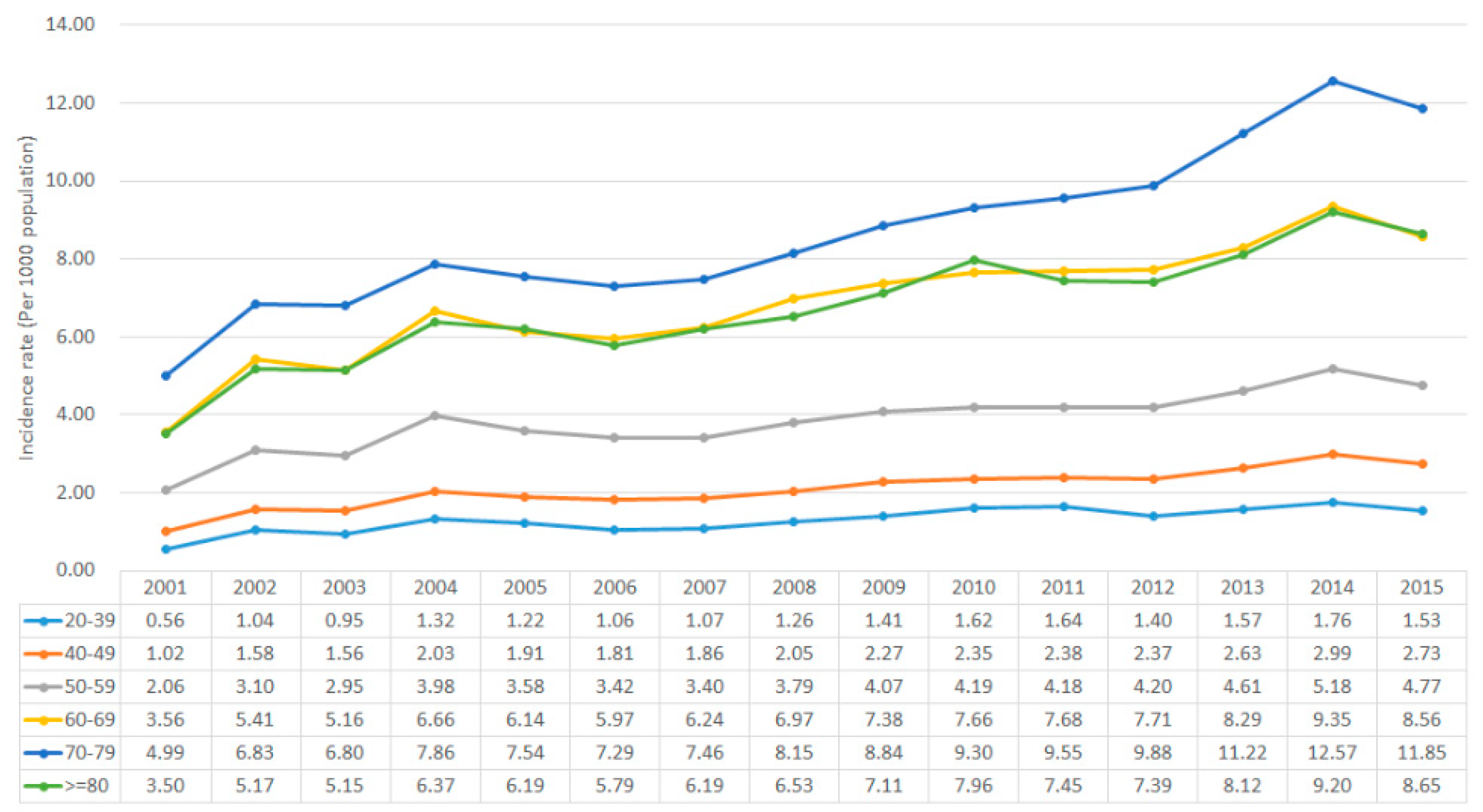
2.1. Prevalence and Incidence in Taiwan
2.2. Risk Factors
3. Pathophysiology
4. Different Subtypes of Dry Eye Disease
4.1. Lipid Anomaly Dry Eye (LADE)
4.2. Aqueous Tear Deficiency (ATD)
4.3. Allergic and Toxic Dry Eye (ADE)
4.4. Lid Surfacing or Blinking Anomalies (LSADE)
4.5. Marginal Dry Eye
4.6. Cicatricial Condition
5. Treatment and New Therapeutic Agents for DED
5.1. Artificial Tear
5.2. Artificial Solution without/with Anti-Inflammatory Drugs
5.3. Cyclosporine A
5.4. Autologous Serum
5.5. Punctal Plug
5.6. Warm Compression
5.7. Mucin Secretagogue
5.8. Anti-Inflammatory Agents (Steroid and Non-Steroid)
5.9. Other Potential Agents
6. A New Trend for Applying Nanomedicine in DED Treatment
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- O’Brien, P.D.; Collum, L.M. Dry eye: Diagnosis and current treatment strategies. Curr. Allergy Asthma Rep. 2004, 4, 314–319. [Google Scholar] [CrossRef] [PubMed]
- Craig, J.P.; Nichols, K.K.; Akpek, E.K.; Caffery, B.; Dua, H.S.; Joo, C.K.; Liu, Z.; Nelson, J.D.; Nichols, J.J.; Tsubota, K.; et al. TFOS DEWS II Definition and Classification Report. Ocul. Surf. 2017, 15, 276–283. [Google Scholar] [CrossRef] [PubMed]
- The definition and classification of dry eye disease: Report of the Definition and Classification Subcommittee of the International Dry Eye WorkShop (2007). Ocul. Surf. 2007, 5, 75–92. [CrossRef]
- Messmer, E.M. The pathophysiology, diagnosis and treatment of dry eye disease. Dtsch. Arztebl. Int. 2015, 112, 71–82. [Google Scholar] [CrossRef] [PubMed]
- Bron, A.J.; Evans, V.E.; Smith, J.A. Grading Of Corneal and Conjunctival Staining in the Context of Other Dry Eye Tests. Cornea 2003, 22, 640–650. [Google Scholar] [CrossRef]
- Miller, K.L.; Walt, J.G.; Mink, D.R.; Satram-Hoang, S.; Wilson, S.E.; Perry, H.D.; Asbell, P.A.; Pflugfelder, S.C. Minimal clinically important difference for the ocular surface disease index. Arch. Ophthalmol. (Chic. ILL. 1960) 2010, 128, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Yeh, P.T.; Chien, H.C.; Ng, K.; Tseng, S.H.; Chen, W.L.; Hou, Y.C.; Wang, I.J.; Chu, H.S.; Kao Yang, Y.H.; Hu, F.R. Concordance between patient and clinician assessment of dry eye severity and treatment response in Taiwan. Cornea 2015, 34, 500–505. [Google Scholar] [CrossRef]
- Henrich, C.F.; Ramulu, P.Y.; Akpek, E.K. Association of dry eye and inflammatory systemic diseases in a tertiary care-based sample. Cornea 2014, 33, 819–825. [Google Scholar] [CrossRef]
- Stevens, S. Schirmer’s test. Community Eye Health 2011, 24, 45. [Google Scholar]
- Benelli, U.; Nardi, M.; Posarelli, C.; Albert, T.G. Tear osmolarity measurement using the TearLab™ Osmolarity System in the assessment of dry eye treatment effectiveness. Contact Lens Anterior Eye 2010, 33, 61–67. [Google Scholar] [CrossRef]
- Yokoi, N.; Georgiev, G.A.; Kato, H.; Komuro, A.; Sonomura, Y.; Sotozono, C.; Tsubota, K.; Kinoshita, S. Classification of Fluorescein Breakup Patterns: A Novel Method of Differential Diagnosis for Dry Eye. Am. J. Ophthalmol. 2017, 180, 72–85. [Google Scholar] [CrossRef] [PubMed]
- King-Smith, P.E.; Reuter, K.S.; Braun, R.J.; Nichols, J.J.; Nichols, K.K. Tear film breakup and structure studied by simultaneous video recording of fluorescence and tear film lipid layer images. Investig. Ophthalmol. Vis. Sci. 2013, 54, 4900–4909. [Google Scholar] [CrossRef] [PubMed]
- Doane, M.G.; Lee, M.E. Tear Film Interferometry as a Diagnostic Tool for Evaluating Normal and Dry-Eye Tear Film. In Lacrimal Gland, Tear Film, and Dry Eye Syndromes 2: Basic Science and Clinical Relevance; Sullivan, D.A., Dartt, D.A., Meneray, M.A., Eds.; Springer US: Boston, MA, USA, 1998; pp. 297–303. [Google Scholar]
- Arita, R.; Morishige, N.; Fujii, T.; Fukuoka, S.; Chung, J.L.; Seo, K.Y.; Itoh, K. Tear Interferometric Patterns Reflect Clinical Tear Dynamics in Dry Eye Patients. Investig. Ophthalmol. Vis. Sci. 2016, 57, 3928–3934. [Google Scholar] [CrossRef] [PubMed]
- Tomlinson, A.; Bron, A.J.; Korb, D.R.; Amano, S.; Paugh, J.R.; Pearce, E.I.; Yee, R.; Yokoi, N.; Arita, R.; Dogru, M. The international workshop on meibomian gland dysfunction: Report of the diagnosis subcommittee. Investig. Ophthalmol. Vis. Sci. 2011, 52, 2006–2049. [Google Scholar] [CrossRef] [PubMed]
- Messmer, E.M.; von Lindenfels, V.; Garbe, A.; Kampik, A. Matrix Metalloproteinase 9 Testing in Dry Eye Disease Using a Commercially Available Point-of-Care Immunoassay. Ophthalmology 2016, 123, 2300–2308. [Google Scholar] [CrossRef] [PubMed]
- Zaleska-Żmijewska, A.; Strzemecka, E.; Wawrzyniak, Z.M.; Szaflik, J.P. Extracellular MMP-9-Based Assessment of Ocular Surface Inflammation in Patients with Primary Open-Angle Glaucoma. J. Ophthalmol. 2019, 2019, 1240537. [Google Scholar] [CrossRef] [PubMed]
- Amparo, F.; Schaumberg, D.A.; Dana, R. Comparison of Two Questionnaires for Dry Eye Symptom Assessment: The Ocular Surface Disease Index and the Symptom Assessment in Dry Eye. Ophthalmology 2015, 122, 1498–1503. [Google Scholar] [CrossRef] [PubMed]
- Simpson, T.L.; Situ, P.; Jones, L.W.; Fonn, D. Dry eye symptoms assessed by four questionnaires. Optom. Vis. Sci. Off. Publ. Am. Acad. Optom. 2008, 85, 692–699. [Google Scholar] [CrossRef]
- Chalmers, R.L.; Begley, C.G.; Moody, K.; Hickson-Curran, S.B. Contact Lens Dry Eye Questionnaire-8 (CLDEQ-8) and opinion of contact lens performance. Opt. Vis. Sci. Off. Publ. Am. Acad. Optom. 2012, 89, 1435–1442. [Google Scholar] [CrossRef]
- Pflugfelder, S.C. Prevalence, burden and pharmacoeconomics of dry eye disease. Am. J. Manag. Care 2008, 14, S102–S106. [Google Scholar]
- Patel, V.D.; Watanabe, J.H.; Strauss, J.A.; Dubey, A.T. Work productivity loss in patients with dry eye disease: An online survey. Curr. Med. Res. Opin. 2011, 27, 1041–1048. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Asche, C.V.; Fairchild, C.J. The economic burden of dry eye disease in the United States: A decision tree analysis. Cornea 2011, 30, 379–387. [Google Scholar] [CrossRef] [PubMed]
- Dalzell, M.D. Dry eye: Prevalence, utilization and economic implications. Manag. care (Langhorne Pa.) 2003, 12, 9–13. [Google Scholar]
- Farrand, K.F.; Fridman, M.; Stillman, I.O.; Schaumberg, D.A. Prevalence of Diagnosed Dry Eye Disease in the United States Among Adults Aged 18 Years and Older. Am. J. Ophthalmol. 2017, 182, 90–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gayton, J.L. Etiology, prevalence and treatment of dry eye disease. Clin. Ophthalmol. (Auckland N.Z.) 2009, 3, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Han, S.B.; Hyon, J.Y.; Woo, S.J.; Lee, J.J.; Kim, T.H.; Kim, K.W. Prevalence of dry eye disease in an elderly Korean population. Arch. Ophthalmol. (Chicago ILL 1960) 2011, 129, 633–638. [Google Scholar] [CrossRef]
- Uchino, M.; Nishiwaki, Y.; Michikawa, T.; Shirakawa, K.; Kuwahara, E.; Yamada, M.; Dogru, M.; Schaumberg, D.A.; Kawakita, T.; Takebayashi, T.; et al. Prevalence and risk factors of dry eye disease in Japan: Koumi study. Ophthalmology 2011, 118, 2361–2367. [Google Scholar] [CrossRef] [PubMed]
- Lin, P.Y.; Tsai, S.Y.; Cheng, C.Y.; Liu, J.H.; Chou, P.; Hsu, W.M. Prevalence of dry eye among an elderly Chinese population in Taiwan: The Shihpai Eye Study. Ophthalmology 2003, 110, 1096–1101. [Google Scholar] [CrossRef]
- Yen, J.C.; Hsu, C.A.; Li, Y.C.; Hsu, M.H. The Prevalence of Dry Eye Syndrome’s and the Likelihood to Develop Sjogren’s Syndrome in Taiwan: A Population-Based Study. Int. J. Environ. Res. Public Health 2015, 12, 7647–7655. [Google Scholar] [CrossRef]
- Hashemi, H.; Khabazkhoob, M.; Kheirkhah, A.; Emamian, M.H.; Mehravaran, S.; Shariati, M.; Fotouhi, A. Prevalence of dry eye syndrome in an adult population. Clin. Exp. Ophthalmol. 2014, 42, 242–248. [Google Scholar] [CrossRef]
- Lu, P.; Chen, X.; Liu, X.; Yu, L.; Kang, Y.; Xie, Q.; Ke, L.; Wei, X. Dry eye syndrome in elderly Tibetans at high altitude: A population-based study in China. Cornea 2008, 27, 545–551. [Google Scholar] [CrossRef] [PubMed]
- Bjerrum, K.B. Keratoconjunctivitis sicca and primary Sjogren’s syndrome in a Danish population aged 30-60 years. Acta Ophthalmol. Scand. 1997, 75, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Mody, G.M.; Hill, J.C.; Meyers, O.L. Keratoconjunctivitis sicca in rheumatoid arthritis. Clin. Rheumatol. 1988, 7, 237–241. [Google Scholar] [CrossRef] [PubMed]
- Lemp, M.A. Report of the National Eye Institute/Industry workshop on Clinical Trials in Dry Eyes. CLAO J. Off. Publ. Contact Lens Assoc. Ophthalmol. 1995, 21, 221–232. [Google Scholar]
- Albietz, J.M. Prevalence of dry eye subtypes in clinical optometry practice. Optom. Vis. Sci. Off. Publ. Am. Acad. Optom. 2000, 77, 357–363. [Google Scholar] [CrossRef]
- Chen, C.S.; Cheng, H.M.; Chen, H.J.; Tsai, S.Y.; Kao, C.H.; Lin, H.J.; Wan, L.; Yang, T.Y. Dry eye syndrome and the subsequent risk of chronic fatigue syndrome-a prospective population-based study in Taiwan. Oncotarget 2018, 9, 30694–30703. [Google Scholar] [CrossRef] [PubMed]
- Qin, L.; Kao, Y.W.; Lin, Y.L.; Peng, B.Y.; Deng, W.P.; Chen, T.M.; Lin, K.C.; Yuan, K.S.P.; Wu, A.T.; Shia, B.C.; et al. Combination of recurrent oral aphthae and dry eye syndrome may constitute an independent risk factor for oral cavity cancer in elderly women. Cancer Manag. Res. 2018, 10, 3273–3281. [Google Scholar] [CrossRef]
- Zhong, J.Y.; Lee, Y.C.; Hsieh, C.J.; Tseng, C.C.; Yiin, L.M. Association between Dry Eye Disease, Air Pollution and Weather Changes in Taiwan. Int. J. Environ. Res. Public Health 2018, 15, 2269. [Google Scholar] [CrossRef]
- Chen, C.H.; Yang, T.Y.; Lin, C.L.; Chen, C.S.; Lin, W.M.; Kuo, C.N.; Lin, M.C.; Kao, C.H. Dry Eye Syndrome Risks in Patients With Fibromyalgia: A National Retrospective Cohort Study. Medicine 2016, 95, e2607. [Google Scholar] [CrossRef]
- Chen, H.Y.; Lin, C.L.; Tsai, Y.Y.; Kao, C.H. Association between Glaucoma Medication Usage and Dry Eye in Taiwan. Opt. Vis. Sci. Off. Publ. Am. Acad. Opt. 2015, 92, e227–e232. [Google Scholar] [CrossRef]
- Huang, Y.C.; Chan, W.C.; Wang, J.D.; Fu, L.S.; Tsan, Y.T. Association between dry eye disease and asthma: A nationwide population-based study. Peer J. 2018, 6, e5941. [Google Scholar] [CrossRef] [PubMed]
- Jeng, Y.T.; Lin, S.Y.; Hu, H.Y.; Lee, O.K.; Kuo, L.L. Osteoporosis and dry eye syndrome: A previously unappreciated association that may alert active prevention of fall. PLoS ONE 2018, 13, e0207008. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.Y.; Chen, H.C.; Sun, C.C.; Lin, H.Y.; Lu, K.H.; Huang, J.Y.; Yeh, C.B.; Yang, S.F. Gout as a Risk Factor for Dry Eye Disease: A Population-Based Cohort Study. J. Clin. Med. 2019, 8, 62. [Google Scholar] [CrossRef] [PubMed]
- Mai, E.L.C.; Lin, C.C.; Lian, I.; Liao, R.; Chen, M.; Chang, C. Population-based study on the epidemiology of dry eye disease and its association with presbyopia and other risk factors. Int. Ophthalmol. 2019, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.H.; Chao, W.C.; Liao, T.L.; Lin, C.H.; Chen, D.Y. Risk of autoimmune rheumatic diseases in patients with palindromic rheumatism: A nationwide, population-based, cohort study. PLoS ONE 2018, 13, e0201340. [Google Scholar]
- Guo, B.; Lu, P.; Chen, X.; Zhang, W.; Chen, R. Prevalence of dry eye disease in Mongolians at high altitude in China: The Henan eye study. Ophthalmic Epidemiol. 2010, 17, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Moss, S.E.; Klein, R.; Klein, B.E. Prevalence of and risk factors for dry eye syndrome. Arch. Ophthalmol. (Chic. Ill. 1960) 2000, 118, 1264–1268. [Google Scholar] [CrossRef] [PubMed]
- Paulsen, A.J.; Cruickshanks, K.J.; Fischer, M.E.; Huang, G.H.; Klein, B.E.; Klein, R.; Dalton, D.S. Dry eye in the beaver dam offspring study: Prevalence, risk factors and health-related quality of life. Am. J. Ophthalmol. 2014, 157, 799–806. [Google Scholar] [CrossRef] [PubMed]
- Song, P.; Xia, W.; Wang, M.; Chang, X.; Wang, J.; Jin, S.; Wang, J.; Wei, W.; Rudan, I. Variations of dry eye disease prevalence by age, sex and geographic characteristics in China: A systematic review and meta-analysis. J. Glob. Health 2018, 8, 020503. [Google Scholar] [CrossRef]
- Clayton, J.A. Dry Eye. New Engl. J. Med. 2018, 378, 2212–2223. [Google Scholar] [CrossRef]
- McCulley, J.P.; Shine, W.E. Meibomian gland function and the tear lipid layer. Ocul. Surf. 2003, 1, 97–106. [Google Scholar] [CrossRef]
- Georgiev, G.A.; Eftimov, P.; Yokoi, N. Structure-function relationship of tear film lipid layer: A contemporary perspective. Exp. Eye Res. 2017, 163, 17–28. [Google Scholar] [CrossRef] [PubMed]
- Sledge, S.M.; Khimji, H.; Borchman, D.; Oliver, A.L.; Michael, H.; Dennis, E.K.; Gerlach, D.; Bhola, R.; Stephen, E. Evaporation and Hydrocarbon Chain Conformation of Surface Lipid Films. Ocul. Surf. 2016, 14, 447–459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Georgiev, G.A.; Yokoi, N.; Ivanova, S.; Tonchev, V.; Nencheva, Y.; Krastev, R. Surface relaxations as a tool to distinguish the dynamic interfacial properties of films formed by normal and diseased meibomian lipids. Soft Matter 2014, 10, 5579–5588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green-Church, K.B.; Butovich, I.; Willcox, M.; Borchman, D.; Paulsen, F.; Barabino, S.; Glasgow, B.J. The international workshop on meibomian gland dysfunction: Report of the subcommittee on tear film lipids and lipid–protein interactions in health and disease. Investig. ophthalmol. Vis. Sci. 2011, 52, 1979–1993. [Google Scholar] [CrossRef] [PubMed]
- King-Smith, P.E.; Fink, B.A.; Nichols, J.J.; Nichols, K.K.; Braun, R.J.; McFadden, G.B. The contribution of lipid layer movement to tear film thinning and breakup. Investig. Ophthalmol. Vis. Sci. 2009, 50, 2747–2756. [Google Scholar] [CrossRef] [PubMed]
- Knop, E.; Knop, N.; Schirra, F. Meibomian glands. Part II: Physiology, characteristics, distribution and function of meibomian oil. Der Ophthalmol. Z. Der Dtsch. Ophthalmol. Ges. 2009, 106, 884–892. [Google Scholar]
- Murube, J. The origin of tears. III. The lipid component in the XIX and XX centuries. Ocul. Surf. 2012, 4, 200–209. [Google Scholar] [CrossRef]
- Conrady, C.D.; Joos, Z.P.; Patel, B.C. Review: The Lacrimal Gland and Its Role in Dry Eye. J. Ophthalmol. 2016, 2016, 7542929. [Google Scholar] [CrossRef]
- Dartt, D.A.; Willcox, M.D.P. Complexity of the tear film: Importance in homeostasis and dysfunction during disease. Exp. Eye Res. 2013, 117, 1–3. [Google Scholar] [CrossRef] [Green Version]
- Phadatare, S.P.; Momin, M.; Nighojkar, P.; Askarkar, S.; Singh, K.K. A Comprehensive Review on Dry Eye Disease: Diagnosis, Medical Management, Recent Developments and Future Challenges. Adv. Pharm. 2015, 2015, 12. [Google Scholar] [CrossRef]
- Zhang, X.; Vimalin, M.J.; Qu, Y.; He, X.; Ou, S.; Bu, J.; Jia, C.; Wang, J.; Wu, H.; Liu, Z.; et al. Dry Eye Management: Targeting the Ocular Surface Microenvironment. Int. J. Mol. Sci. 2017, 18, 1398. [Google Scholar] [CrossRef] [PubMed]
- Kunert, K.S.; Tisdale, A.S.; Stern, M.E.; Smith, J.A.; Gipson, I.K. Analysis of topical cyclosporine treatment of patients with dry eye syndrome: Effect on conjunctival lymphocytes. Arch. Ophthalmol. (Chic. Ill. 1960) 2000, 118, 1489–1496. [Google Scholar] [CrossRef] [PubMed]
- Solomon, A.; Dursun, D.; Liu, Z.; Xie, Y.; Macri, A.; Pflugfelder, S.C. Pro- and anti-inflammatory forms of interleukin-1 in the tear fluid and conjunctiva of patients with dry-eye disease. Investig. Ophthalmol. Vis. Sci. 2001, 42, 2283–2292. [Google Scholar]
- Cejkova, J.; Ardan, T.; Simonova, Z.; Cejka, C.; Malec, J.; Jirsova, K.; Filipec, M.; Dotrelova, D.; Brunova, B. Nitric oxide synthase induction and cytotoxic nitrogen-related oxidant formation in conjunctival epithelium of dry eye (Sjogren’s syndrome). Nitric. Oxide Biol. Chem. 2007, 17, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Hessen, M.; Akpek, E.K. Dry eye: An inflammatory ocular disease. J. Ophthalmic Vis.Res. 2014, 9, 240–250. [Google Scholar] [PubMed]
- Stern, M.E.; Gao, J.; Schwalb, T.A.; Ngo, M.; Tieu, D.D.; Chan, C.C.; Reis, B.L.; Whitcup, S.M.; Thompson, D.; Smith, J.A. Conjunctival T-cell subpopulations in Sjogren’s and non-Sjogren’s patients with dry eye. Investig. Ophthalmol. Vis. Sci. 2002, 43, 2609–2614. [Google Scholar]
- Wei, Y.; Asbell, P.A. The core mechanism of dry eye disease is inflammation. Eye Contact Lens 2014, 40, 248–256. [Google Scholar] [CrossRef] [PubMed]
- Hom, M.M.; Martinson, J.R.; Knapp, L.L.; Paugh, J.R. Prevalence of Meibomian gland dysfunction. Optom. Vis. Sci. Off. Publ. Am. Acad Optom. 1990, 67, 710–712. [Google Scholar] [CrossRef]
- Foulks, G.N.; Bron, A.J. Meibomian Gland Dysfunction: A Clinical Scheme for Description, Diagnosis, Classification and Grading. Ocul. Surf. 2003, 1, 107–126. [Google Scholar] [CrossRef]
- Foulks, G.N. The correlation between the tear film lipid layer and dry eye disease. Surv. Ophthalmol. 2007, 52, 369–374. [Google Scholar] [CrossRef] [PubMed]
- Rege, A.; Kulkarni, V.; Puthran, N.; Khandgave, T. A Clinical Study of Subtype-based Prevalence of Dry Eye. J. Clin. Diagn. Res. JCDR 2013, 7, 2207–2210. [Google Scholar] [CrossRef] [PubMed]
- Albietz, J.M.; Schmid, K.L. Intense pulsed light treatment and meibomian gland expression for moderate to advanced meibomian gland dysfunction. Clin. Exp. Optom. 2018, 101, 23–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blackie, C.A.; Carlson, A.N.; Korb, D.R. Treatment for meibomian gland dysfunction and dry eye symptoms with a single-dose vectored thermal pulsation: A review. Curr. Opin. Ophthalmol. 2015, 26, 306–313. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.H.; Kang, Y.S.; Lee, H.S.; Choi, W.; You, I.C.; Yoon, K.C. Effectiveness of Combined Tear Film Therapy in Patients with Evaporative Dry Eye with Short Tear Film Breakup Time. J. Ocul. Pharmacol. Ther. Off. J. Assoc. Ocul. Pharmacol. Ther. 2017, 33, 635–643. [Google Scholar] [CrossRef] [PubMed]
- Qiao, J.; Yan, X. Emerging treatment options for meibomian gland dysfunction. Clin. Ophthalmol. (Auckl. N.Z.) 2013, 7, 1797–1803. [Google Scholar]
- Zhao, Y.; Veerappan, A.; Yeo, S.; Rooney, D.M.; Acharya, R.U.; Tan, J.H.; Tong, L. Clinical Trial of Thermal Pulsation (LipiFlow) in Meibomian Gland Dysfunction With Preteatment Meibography. Eye Contact Lens 2016, 42, 339–346. [Google Scholar] [CrossRef] [Green Version]
- Pang, S.P.; Chen, Y.T.; Tam, K.W.; Lin, I.C.; Loh, E.W. Efficacy of Vectored Thermal Pulsation and Warm Compress Treatments in Meibomian Gland Dysfunction: A Meta-Analysis of Randomized Controlled Trials. Cornea 2019, 39, 690–697. [Google Scholar] [CrossRef]
- Borchman, D. The optimum temperature for the heat therapy for meibomian gland dysfunction. Ocul. Surf. 2019, 17, 360–364. [Google Scholar] [CrossRef]
- Garcia, D.M.; Reis de Oliveira, F.; Módulo, C.M.; Faustino, J.; Barbosa, A.P.; Alves, M.; Rocha, E.M. Is Sjögren’s syndrome dry eye similar to dry eye caused by other etiologies? Discriminating different diseases by dry eye tests. PLoS ONE 2018, 13, e0208420. [Google Scholar] [CrossRef]
- Chen, K.; Jiang, M.; Li, C.; Liu, O.; Tsai, C.S. Discrimination between Sjögren’s and Non-Sjögren’s Sicca Syndrome by Sialoscintigraphy and Antibodies against α-Fodrin and Ro/La Autoantigens. J. Int. Med. Res. 2009, 37, 1088–1096. [Google Scholar] [CrossRef] [PubMed]
- Fairchild, C.J.; Chalmers, R.L.; Begley, C.G. Clinically important difference in dry eye: Change in IDEEL-symptom bother. Optom. Vis. Sci. Off. Publ. Am. Acad. Optom. 2008, 85, 699–707. [Google Scholar] [CrossRef] [PubMed]
- Javadi, M.A.; Feizi, S. Dry eye syndrome. J. Ophthalmic. Vis. Res. 2011, 6, 192–198. [Google Scholar] [PubMed]
- Christodoulou, M.I.; Kapsogeorgou, E.K.; Moutsopoulos, H.M. Characteristics of the minor salivary gland infiltrates in Sjogren’s syndrome. J. Autoimmun. 2010, 34, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Coursey, T.G.; de Paiva, C.S. Managing Sjögren’s Syndrome and non-Sjögren Syndrome dry eye with anti-inflammatory therapy. Clin. Ophthalmol. (Auckl. N.Z.) 2014, 8, 1447–1458. [Google Scholar]
- Dart, J. Cicatricial pemphigoid and dry eye. Semin. Ophthalmol. 2005, 20, 95–100. [Google Scholar] [CrossRef]
- Salzano, U.S.; Arduino, P.; Zambruno, G.; Di Zenzo, G.; Baldovino, S.; Roccatello, D.; Conrotto, D.; Carrozzo, M. OC9 Successful use of mycophenolate mofetil in combination with minocycline in a woman with severe predominantly oral mucous membrane pemphigoid: A case report. Oral. Dis. 2006, 12, 11. [Google Scholar] [CrossRef]
- McCluskey, P.; Chang, J.H.; Singh, R.; Wakefield, D. Methotrexate therapy for ocular cicatricial pemphigoid. Ophthalmology 2004, 111, 796–801. [Google Scholar] [CrossRef]
- Neff, A.G.; Turner, M.; Mutasim, D.F. Treatment strategies in mucous membrane pemphigoid. Ther. Clin. Risk Manag. 2008, 4, 617–626. [Google Scholar] [CrossRef]
- Heffernan, M.P.; Bentley, D.D. Successful treatment of mucous membrane pemphigoid with infliximab. Arch. Dermatol. 2006, 142, 1268–1270. [Google Scholar] [CrossRef]
- Foster, C.S.; Sainz De La Maza, M. Ocular cicatricial pemphigoid review. Curr. Opin. Allergy Clin. Immunol. 2004, 4, 435–439. [Google Scholar] [CrossRef] [PubMed]
- Donnenfeld, E.D.; Perry, H.D.; Wallerstein, A.; Caronia, R.M.; Kanellopoulos, A.J.; Sforza, P.D.; D’Aversa, G. Subconjunctival mitomycin C for the treatment of ocular cicatricial pemphigoid. Ophthalmology 1999, 106, 72–79. [Google Scholar] [CrossRef]
- Juri, M.C.; Fernandez Romero, D.S.; Devoto, M.H.; Georgiett, D.; Zarate, J.O.; Malbran, A. Systemic treatment of ocular cicatricial pemphigoid. Medicina 2012, 72, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; You, C.; Hernandez, M.; Maleki, A.; Lasave, A.; Schmidt, A.; Stephenson, A.; Zhao, T.; Anesi, S.; Foster, C.S. Management of Ocular Cicatricial Pemphigoid with Intravenous Immunoglobulin Monotherapy. Ocul. Immunol. Inflamm. 2018, 27, 636–642. [Google Scholar] [CrossRef] [PubMed]
- Tsubota, K.; Satake, Y.; Ohyama, M.; Toda, I.; Takano, Y.; Ono, M.; Shinozaki, N.; Shimazaki, J.U.N. Surgical Reconstruction of the Ocular Surface in Advanced Ocular Cicatricial Pemphigoid and Stevens-Johnson Syndrome. Am. J. Ophthalmol. 1996, 122, 38–52. [Google Scholar] [CrossRef]
- Baudouin, C.; Labbe, A.; Liang, H.; Pauly, A.; Brignole-Baudouin, F. Preservatives in eyedrops: The good, the bad and the ugly. Prog. Retin. Eye Res. 2010, 29, 312–334. [Google Scholar] [CrossRef] [PubMed]
- Fujishima, H.; Toda, I.; Shimazaki, J.; Tsubota, K. Allergic conjunctivitis and dry eye. Br. J. Ophthalmol. 1996, 80, 994–997. [Google Scholar] [CrossRef] [PubMed]
- Toda, I.; Shimazaki, J.; Tsubota, K. Dry eye with only decreased tear break-up time is sometimes associated with allergic conjunctivitis. Ophthalmology 1995, 102, 302–309. [Google Scholar] [CrossRef]
- Akil, H.; Celik, F.; Ulas, F.; Kara, I.S. Dry Eye Syndrome and Allergic Conjunctivitis in the Pediatric Population. Middle East Afr. J. Ophthalmol. 2015, 22, 467–471. [Google Scholar] [CrossRef] [PubMed]
- Hom, M.M.; Nguyen, A.L.; Bielory, L. Allergic conjunctivitis and dry eye syndrome. Ann. Allergy Asthma Immunol. Off. Publ. Am. College Allergy Asthma Immunol. 2012, 108, 163–166. [Google Scholar] [CrossRef]
- Cardona, G.; Garcia, C.; Seres, C.; Vilaseca, M.; Gispets, J. Blink rate, blink amplitude and tear film integrity during dynamic visual display terminal tasks. Curr. Eye Res. 2011, 36, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Himebaugh, N.L.; Begley, C.G.; Bradley, A.; Wilkinson, J.A. Blinking and tear break-up during four visual tasks. Optom. Vis. Sci. Off. Publ. Am. Acad. Optom. 2009, 86, E106–E114. [Google Scholar] [CrossRef] [PubMed]
- White, R.; Rodriguez, J.; Lane, K.; Johnston, P.; Angjeli, E.; Abelson, M. Blink Patterns in Normal and Dry Eye Subjects; Beyond Blink Rate. Investig. Ophthalmol. Vis. Sci. 2010, 51, 3366. [Google Scholar]
- Nomura, R.; Okada, T. Assessing the appeal power of narrative performance by using eyeblink synchronization among audience. In Computational and Cognitive Approaches to Narratology; Ogata, T.A., Taisuke, Eds.; Information Science Reference (IGI Global): Hershey, PA, USA, 2016; pp. 304–321. [Google Scholar]
- Johnston, P.R.; Rodriguez, J.; Lane, K.J.; Ousler, G.; Abelson, M.B. The interblink interval in normal and dry eye subjects. Clin. Ophthalmol. (Auckl. N.Z.) 2013, 7, 253–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ousler, G.W., 3rd; Abelson, M.B.; Johnston, P.R.; Rodriguez, J.; Lane, K.; Smith, L.M. Blink patterns and lid-contact times in dry-eye and normal subjects. Clin. Ophthalmol. (Auckl. N.Z.) 2014, 8, 869–874. [Google Scholar] [CrossRef] [PubMed]
- Pult, H.; Riede-Pult, B.H.; Murphy, P.J. The relation between blinking and conjunctival folds and dry eye symptoms. Optom. Vis. Sci. Off Publ. Am. Acad. Optom. 2013, 90, 1034–1039. [Google Scholar] [CrossRef] [PubMed]
- McMonnies, C.; Ho, A.; Wakefield, D. Optimum dry eye classification using questionnaire responses. Adv. Exp. Med. Biol. 1998, 438, 835–838. [Google Scholar] [PubMed]
- Gilbert, C. The eye signs of vitamin A deficiency. Community Eye Health 2013, 26, 66–67. [Google Scholar] [PubMed]
- Sommer, A. Treatment of corneal xerophthalmia with topical retinoic acid. Am. J. Ophthalmol. 1983, 95, 349–352. [Google Scholar] [CrossRef]
- Ubels, J.L.; Edelhauser, H.F.; Foley, K.M.; Liao, J.C.; Gressel, P. The efficacy of retinoic acid ointment for treatment of xerophthalmia and corneal epithelial wounds. Curr. Eye Research 1985, 4, 1049–1057. [Google Scholar] [CrossRef]
- Hatchell, D.L.; Faculjak, M.; Kubicek, D. Treatment of xerophthalmia with retinol, tretinoin and etretinate. Arch. Ophthalmol. (Chic. Ill. 1960) 1984, 102, 926–927. [Google Scholar] [CrossRef] [PubMed]
- Taylor, H.R.; West, S.K.; Mmbaga, B.B.; Katala, S.J.; Turner, V.; Lynch, M.; Munoz, B.; Rapoza, P.A. Hygiene factors and increased risk of trachoma in central Tanzania. Arch. Ophthalmol. (Chic. Ill. 1960) 1989, 107, 1821–1825. [Google Scholar] [CrossRef] [PubMed]
- Patel, D.B.; Brahmbhatta, J.N.; Jasani, H.V.; Desai, A.P.; Mehta, P.K. A study of prevalence of dry eye in relation to trachoma. Indian J. Clin. Exp. Ophthalmol. 2017, 3, 342–345. [Google Scholar]
- Bowman, R.J.; Sillah, A.; Van Dehn, C.; Goode, V.M.; Muqit, M.M.; Johnson, G.J.; Milligan, P.; Rowley, J.; Faal, H.; Bailey, R.L. Operational comparison of single-dose azithromycin and topical tetracycline for trachoma. Investig. Ophthalmol. Vis. Sci. 2000, 41, 4074–4079. [Google Scholar]
- Baudouin, C.; de la Maza, M.S.; Amrane, M.; Garrigue, J.S.; Ismail, D.; Figueiredo, F.C.; Leonardi, A. One-Year Efficacy and Safety of 0.1% Cyclosporine a Cationic Emulsion in the Treatment of Severe Dry Eye Disease. Eur. J. Ophthalmol. 2017, 27, 678–685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, Y.; Song, J.S.; Choi, C.Y.; Yoon, K.C.; Lee, H.K.; Kim, H.S. A Randomized Multicenter Study Comparing 0.1%, 0.15%, and 0.3% Sodium Hyaluronate with 0.05% Cyclosporine in the Treatment of Dry Eye. J. Ocul. Pharmacol. Ther. Off. J. Assoc. Ocul. Pharmacol. Ther. 2017, 33, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.C.; Choi, J.S.; Joo, C.K. A comparison of vitamin a and cyclosporine a 0.05% eye drops for treatment of dry eye syndrome. Am. J. Ophthalmol. 2009, 147, 206–213. [Google Scholar] [CrossRef]
- Essa, L.; Laughton, D.; Wolffsohn, J.S. Can the optimum artificial tear treatment for dry eye disease be predicted from presenting signs and symptoms? Contact Lens Anterior Eye J. Br. Contact Lens Assoc. 2018, 41, 60–68. [Google Scholar] [CrossRef] [Green Version]
- Simmons, P.; Gilbert, M.; Lai, F.; Vehige, J. Artificial Tear Use Improves Objective Signs and Visual Symptoms of Dry Eye. Investig. Ophthalmol. Vis. Sci. 2009, 50, 4646. [Google Scholar]
- Lievens, C.; Berdy, G.; Douglass, D.; Montaquila, S.; Lin, H.; Simmons, P.; Carlisle-Wilcox, C.; Vehige, J.; Haque, S. Evaluation of an enhanced viscosity artificial tear for moderate to severe dry eye disease: A multicenter, double-masked, randomized 30-day study. Contact Lens Anterior Eye 2019, 42, 443–449. [Google Scholar] [CrossRef] [Green Version]
- Diaz-Llopis, M.; Pinazo-Duran, M.D.; Diaz-Guinon, L.; Rahhal-Ortuno, M.; Perez-Ramos, M.; Bosch, R.; Gallego-Pinazo, R.; Dolz-Marco, R.; Diaz-Guinon, T.; Diaz, M.; et al. A randomized multicenter study comparing seawater washes and carmellose artificial tears eyedrops in the treatment of dry eye syndrome. Clin. Ophthalmol. 2019, 13, 483–490. [Google Scholar] [CrossRef] [PubMed]
- Aragona, P.; Papa, V.; Micali, A.; Santocono, M.; Milazzo, G. Long term treatment with sodium hyaluronate-containing artificial tears reduces ocular surface damage in patients with dry eye. Br. J. Ophthalmol. 2002, 86, 181–184. [Google Scholar] [CrossRef] [PubMed]
- You, I.C.; Li, Y.; Jin, R.; Ahn, M.; Choi, W.; Yoon, K.C. Comparison of 0.1%, 0.18%, and 0.3% Hyaluronic Acid Eye Drops in the Treatment of Experimental Dry Eye. J. Ocul. Pharmacol. Ther. Off. J. Assoc. Ocul. Pharmacol. Ther. 2018, 34, 557–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tseng, C.L.; Hung, Y.J.; Chen, Z.Y.; Fang, H.W.; Chen, K.H. Synergistic Effect of Artificial Tears Containing Epigallocatechin Gallate and Hyaluronic Acid for the Treatment of Rabbits with Dry Eye Syndrome. PLoS ONE 2016, 11, e0157982. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Choi, J.H.; Oh, H.J.; Park, S.H.; Lee, J.B.; Yoon, K.C. Effects of eye drops containing a mixture of omega-3 essential fatty acids and hyaluronic acid on the ocular surface in desiccating stress-induced murine dry eye. Curr.Eye Res. 2014, 39, 871–878. [Google Scholar] [CrossRef] [PubMed]
- Borel, J.F.; Baumann, G.; Beveridge, T. Cyclosporine. In Encyclopedia of Immunology, 2nd ed.; Delves, P.J., Ed.; Elsevier: Oxford, UK, 1998; pp. 686–689. [Google Scholar]
- Shah, V.V.; Reddy, S.P.; Lin, E.J.; Wu, J.J. Chapter 6-Cyclosporine. In Therapy for Severe Psoriasis; Wu, J.J., Feldman, S.R., Lebwohl, M.G., Eds.; Elsevier: Amsterdam, The Netherlands, 2016; pp. 63–73. [Google Scholar]
- Kahn, D.; Mazzaferro, V.; Cervio, G.; Venkataramanan, R.; Makowka, L.; Van Thiel, D.H.; Starzl, T.E. Correlation between dose and level of cyclosporine after orthotopic liver transplantation. Transplant. Proc. 1989, 21, 2240–2241. [Google Scholar]
- Canafax, D.M.; Ascher, N.L. Cyclosporine immunosuppression. Clin. Pharm. 1983, 2, 515–524. [Google Scholar] [CrossRef]
- Rhee, M.K.; Mah, F.S. Clinical utility of cyclosporine (CsA) ophthalmic emulsion 0.05% for symptomatic relief in people with chronic dry eye: A review of the literature. Clin. Ophthalmol. 2017, 11, 1157–1166. [Google Scholar] [CrossRef]
- Kymionis, G.D.; Bouzoukis, D.I.; Diakonis, V.F.; Siganos, C. Treatment of chronic dry eye: Focus on cyclosporine. Clin. Ophthalmol. (Auckl. N.Z.) 2008, 2, 829–836. [Google Scholar] [CrossRef]
- Schultz, C. Safety and efficacy of cyclosporine in the treatment of chronic dry eye. Ophthalmol. Eye Dis. 2014, 6, 37–42. [Google Scholar] [CrossRef]
- Othman, T.M.; Mousa, A.; Gikandi, P.W.; AbdelMabod, M.; Abdelrahman, A.M. Efficacy and safety of using topical cyclosporine A for treatment of moderate to severe dry eye disease. Saudi J. Ophthalmol. 2018, 32, 217–221. [Google Scholar] [CrossRef] [PubMed]
- Yavuz, B.; Pehlivan, S.B.; Ünlü, N. An Overview on Dry Eye Treatment: Approaches for Cyclosporin A Delivery. Sci. World J. 2012, 2012, 11. [Google Scholar] [CrossRef] [PubMed]
- Andrews, L.M.; Riva, N.; de Winter, B.C.; Hesselink, D.A.; de Wildt, S.N.; Cransberg, K.; van Gelder, T. Dosing algorithms for initiation of immunosuppressive drugs in solid organ transplant recipients. Expert Opin. Drug Metab. Toxicol. 2015, 11, 921–936. [Google Scholar] [CrossRef] [PubMed]
- Perry, H.D.; Donnenfeld, E.D. Topical 0.05% cyclosporin in the treatment of dry eye. Expert Opin. Pharmacother. 2004, 5, 2099–2107. [Google Scholar] [CrossRef] [PubMed]
- Straub, M.; Bron, A.M.; Muselier-Mathieu, A.; Creuzot-Garcher, C. Long-term outcome after topical ciclosporin in severe dry eye disease with a 10-year follow-up. Br. J. Ophthalmol. 2016, 100, 1547–1550. [Google Scholar] [CrossRef] [PubMed]
- Herrygers, L.; Noecker, R. Efficacy of cyclosporine A (Restasis) for the treatment of dry eye symptoms in the first 30 days of therapy. Investig. Ophthalmol. Vis. Sci. 2005, 46, 2026. [Google Scholar]
- Dastjerdi, M.H.; Hamrah, P.; Dana, R. High-frequency topical cyclosporine 0.05% in the treatment of severe dry eye refractory to twice-daily regimen. Cornea 2009, 28, 1091–1096. [Google Scholar] [CrossRef]
- Su, M.Y.; Perry, H.D.; Barsam, A.; Perry, A.R.; Donnenfeld, E.D.; Wittpenn, J.R.; D’Aversa, G. The effect of decreasing the dosage of cyclosporine A 0.05% on dry eye disease after 1 year of twice-daily therapy. Cornea 2011, 30, 1098–1104. [Google Scholar] [CrossRef]
- Parrilha, L.R.; Nai, G.A.; Giuffrida, R.; Barbero, R.C.; Padovani, L.D.F.; Pereira, R.H.Z.; Silva, D.A.; Silva, M.C.A.; Diniz, M.S.; Andrade, S.F. Comparison of 1% cyclosporine eye drops in olive oil and in linseed oil to treat experimentally-induced keratoconjunctivitis sicca in rabbits. Arq. Bras. De Oftalmol. 2015, 78, 295–299. [Google Scholar] [CrossRef] [Green Version]
- Demiryay, E.; Yaylali, V.; Cetin, E.N.; Yildirim, C. Effects of topical cyclosporine a plus artificial tears versus artificial tears treatment on conjunctival goblet cell density in dysfunctional tear syndrome. Eye Contact Lens 2011, 37, 312–315. [Google Scholar] [CrossRef]
- Sahli, E.; Hosal, B.M.; Zilelioglu, G.; Gulbahce, R.; Ustun, H. The effect of topical cyclosporine A on clinical findings and cytological grade of the disease in patients with dry eye. Cornea 2010, 29, 1412–1416. [Google Scholar] [CrossRef] [PubMed]
- Toker, E.; Asfuroglu, E. Corneal and conjunctival sensitivity in patients with dry eye: The effect of topical cyclosporine therapy. Cornea 2010, 29, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Ogawa, Y.; Dogru, M.; Kawai, M.; Tatematsu, Y.; Uchino, M.; Okada, N.; Igarashi, A.; Kujira, A.; Fujishima, H.; et al. Ocular surface and tear functions after topical cyclosporine treatment in dry eye patients with chronic graft-versus-host disease. Bone marrow Transplant. 2008, 41, 293–302. [Google Scholar] [CrossRef] [PubMed]
- Geerling, G.; Maclennan, S.; Hartwig, D. Autologous serum eye drops for ocular surface disorders. Br. J. Ophthalmol. 2004, 88, 1467–1474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higuchi, A. Autologous Serum and Serum Components. Investig. Ophthalmol. Vis. Sci. 2018, 59, Des121–Des129. [Google Scholar] [CrossRef] [PubMed]
- Lekhanont, K.; Jongkhajornpong, P.; Choubtum, L.; Chuckpaiwong, V. Topical 100% serum eye drops for treating corneal epithelial defect after ocular surgery. BioMed Res. Int. 2013, 2013, 521315. [Google Scholar] [CrossRef]
- Quinto, G.G.; Campos, M.; Behrens, A. Autologous serum for ocular surface diseases. Arq. Bras. De Oftalmol. 2008, 71, 47–54. [Google Scholar] [CrossRef] [Green Version]
- Pan, Q.; Angelina, A.; Zambrano, A.; Marrone, M.; Stark, W.J.; Heflin, T.; Tang, L.; Akpek, E.K. Autologous serum eye drops for dry eye. Cochrane Database Syst. Rev. 2013, 8, Cd009327. [Google Scholar]
- Jehangir, N.; Bever, G.; Mahmood, S.M.J.; Moshirfar, M. Comprehensive Review of the Literature on Existing Punctal Plugs for the Management of Dry Eye Disease. J. Ophthalmol. 2016, 2016, 22. [Google Scholar] [CrossRef]
- Ervin, A.M.; Law, A.; Pucker, A.D. Punctal occlusion for dry eye syndrome: Summary of a Cochrane systematic review. Br. J. Ophthalmol. 2019, 103, 301–306. [Google Scholar] [CrossRef]
- Balaram, M.; Schaumberg, D.A.; Dana, M.R. Efficacy and tolerability outcomes after punctal occlusion with silicone plugs in dry eye syndrome. Am. J. Ophthalmol. 2001, 131, 30–36. [Google Scholar] [CrossRef]
- Tai, M.C.; Cosar, C.B.; Cohen, E.J.; Rapuano, C.J.; Laibson, P.R. The clinical efficacy of silicone punctal plug therapy. Cornea 2002, 21, 135–139. [Google Scholar] [CrossRef] [PubMed]
- Ababneh, O.H.; Msallam, M.M. Bilateral Simultaneous Pyogenic Granuloma After Perforated Punctal Plug Insertion. Ophthalmic Plast. Reconstr. Surg. 2014, 30, e113–e115. [Google Scholar] [CrossRef] [PubMed]
- Rumelt, S.; Remulla, H.; Rubin, P.A.D. Silicone Punctal Plug Migration Resulting in Dacryocystitis and Canaliculitis. Cornea 1997, 16, 377. [Google Scholar] [CrossRef] [PubMed]
- Marcet, M.M.; Shtein, R.M.; Bradley, E.A.; Deng, S.X.; Meyer, D.R.; Bilyk, J.R.; Yen, M.T.; Lee, W.B.; Mawn, L.A. Safety and Efficacy of Lacrimal Drainage System Plugs for Dry Eye Syndrome: A Report by the American Academy of Ophthalmology. Ophthalmology 2015, 122, 1681–1687. [Google Scholar] [CrossRef] [PubMed]
- Henriquez, A.S.; Korb, D.R. Meibomian glands and contact lens wear. Br. J. Ophthalmol. 1981, 65, 108–111. [Google Scholar] [CrossRef] [PubMed]
- Paugh, J.R.; Knapp, L.L.; Martinson, J.R.; Hom, M.M. Meibomian therapy in problematic contact lens wear. Optom. Vis. Sci. Off. Publ. Am. Acad. Optom. 1990, 67, 803–806. [Google Scholar] [CrossRef]
- Olson, M.C.; Korb, D.R.; Greiner, J.V. Increase in tear film lipid layer thickness following treatment with warm compresses in patients with meibomian gland dysfunction. Eye Contact Lens 2003, 29, 96–99. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.; Ho, L.; Wong, K.; La, A.; Lee, S.; Park, S.; Tran, L.; Stapleton, F. The effects of a hydrating mask compared to traditional warm compresses on tear film properties in meibomian gland dysfunction. Contact Lens Anterior Eye J. Br. Contact Lens Assoc. 2018, 41, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Arita, R.; Morishige, N.; Sakamoto, I.; Imai, N.; Shimada, Y.; Igaki, M.; Suzuki, A.; Itoh, K.; Tsubota, K. Effects of a warm compress containing menthol on the tear film in healthy subjects and dry eye patients. Sci. Rep. 2017, 7, 45848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagymihályi, A.; Dikstein, S.; Tiffany, J.M. The influence of eyelid temperature on the delivery of meibomian oil. Exp Eye Res. 2004, 78, 367–370. [Google Scholar]
- Truscott, R.J.W.; Zhu, X. Presbyopia and cataract: A question of heat and time. Prog. Retin. Eye Res. 2010, 29, 487–499. [Google Scholar] [CrossRef] [PubMed]
- Danjo, Y.; Watanabe, H.; Tisdale, A.S.; George, M.; Tsumura, T.; Abelson, M.B.; Gipson, I.K. Alteration of mucin in human conjunctival epithelia in dry eye. Investig. Ophthalmol. Vis. Sci. 1998, 39, 2602–2609. [Google Scholar]
- Gamache, D.A.; Wei, Z.Y.; Weimer, L.K.; Miller, S.T.; Spellman, J.M.; Yanni, J.M. Corneal protection by the ocular mucin secretagogue 15(S)-HETE in a rabbit model of desiccation-induced corneal defect. J. Ocul. Pharmacol. Ther. Off. J. Assoc. Ocul. Pharmacol. Ther. 2002, 18, 349–361. [Google Scholar] [CrossRef] [PubMed]
- Arakawa, T.; Higuchi, K.; Fujiwara, Y.; Watanabe, T.; Tominaga, K.; Sasaki, E.; Oshitani, N.; Yoshikawa, T.; Tarnawski, A.S. 15th anniversary of rebamipide: Looking ahead to the new mechanisms and new applications. Dig. Dis. Sci. 2005, 50, S3–s11. [Google Scholar] [CrossRef] [PubMed]
- Iijima, K.; Ichikawa, T.; Okada, S.; Ogawa, M.; Koike, T.; Ohara, S.; Shimosegawa, T. Rebamipide, a cytoprotective drug, increases gastric mucus secretion in human: Evaluations with endoscopic gastrin test. Dig. Dis. Sci. 2009, 54, 1500–1507. [Google Scholar] [CrossRef] [PubMed]
- Kashima, T.; Itakura, H.; Akiyama, H.; Kishi, S. Rebamipide ophthalmic suspension for the treatment of dry eye syndrome: A critical appraisal. Clin. Ophthalmol. 2014, 8, 1003–1010. [Google Scholar] [CrossRef] [PubMed]
- Ueda, K.; Matsumiya, W.; Otsuka, K.; Maeda, Y.; Nagai, T.; Nakamura, M. Effectiveness and relevant factors of 2% rebamipide ophthalmic suspension treatment in dry eye. BMC Ophthalmol. 2015, 15, 58. [Google Scholar] [CrossRef] [PubMed]
- Shrivastava, S.; Patkar, P.; Ramakrishnan, R.; Kanhere, M.; Riaz, Z. Efficacy of rebamipide 2% ophthalmic solution in the treatment of dry eyes. Oman J. Ophthalmol. 2018, 11, 207–212. [Google Scholar] [CrossRef]
- Kinoshita, S.; Awamura, S.; Oshiden, K.; Nakamichi, N.; Suzuki, H.; Yokoi, N. Rebamipide (OPC-12759) in the treatment of dry eye: A randomized, double-masked, multicenter, placebo-controlled phase II study. Ophthalmology 2012, 119, 2471–2478. [Google Scholar] [CrossRef]
- Hori, Y. Secreted Mucins on the Ocular Surface. Investig. Ophthalmol. Vis. Sci. 2018, 59, Des151–Des156. [Google Scholar] [CrossRef] [PubMed]
- Keating, G.M. Diquafosol ophthalmic solution 3 %: A review of its use in dry eye. Drugs 2015, 75, 911–922. [Google Scholar] [CrossRef] [PubMed]
- Lau, O.C.F.; Samarawickrama, C.; Skalicky, S.E. P2Y2 receptor agonists for the treatment of dry eye disease: a review. Clin. Ophthalmol. (Auckl. N.Z.) 2014, 8, 327–334. [Google Scholar]
- Matsumoto, Y.; Ohashi, Y.; Watanabe, H.; Tsubota, K. Efficacy and safety of diquafosol ophthalmic solution in patients with dry eye syndrome: A Japanese phase 2 clinical trial. Ophthalmology 2012, 119, 1954–1960. [Google Scholar] [CrossRef] [PubMed]
- De Paiva, C.S.; Corrales, R.M.; Villarreal, A.L.; Farley, W.J.; Li, D.Q.; Stern, M.E.; Pflugfelder, S.C. Corticosteroid and doxycycline suppress MMP-9 and inflammatory cytokine expression, MAPK activation in the corneal epithelium in experimental dry eye. Exp. Eye Res. 2006, 83, 526–535. [Google Scholar] [CrossRef] [PubMed]
- Pleyer, U.; Ursell, P.G.; Rama, P. Intraocular pressure effects of common topical steroids for post-cataract inflammation: Are they all the same? Ophthalmol. Ther. 2013, 2, 55–72. [Google Scholar] [CrossRef] [PubMed]
- Cutolo, C.A.; Barabino, S.; Bonzano, C.; Traverso, C.E. The Use of Topical Corticosteroids for Treatment of Dry Eye Syndrome. Ocul. Immunol. Inflamm. 2019, 27, 266–275. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.Q.; Sun, W.; Gu, Y.S. A clinical study of the efficacy of topical corticosteroids on dry eye. J. Zhejiang Univ. Sci. B 2006, 7, 675–678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, H.H.; Ji, Y.S.; Sung, M.S.; Kim, K.K.; Yoon, K.C. Long-Term Outcome of Treatment with Topical Corticosteroids for Severe Dry Eye Associated with Sjogren’s Syndrome. Chonnam Med. J. 2015, 51, 26–32. [Google Scholar] [CrossRef]
- Villani, E.; Pirondini, C.; Viola, F.; Ratiglia, R. Soft steroid topical treatment for moderate to severe dry eye: Pulse vs tapered therapy. Investig. Ophthalmol. Vis. Sci. 2013, 54, 4321. [Google Scholar]
- Singla, S.; Sarkar, L.; Joshi, M. Comparison of topical cyclosporine alone and topical loteprednol with cyclosporine in moderate dry eye in Indian population: A prospective study. Taiwan J. Ophthalmol. [Epub ahead of print]. Available online: http://www.e-tjo.org/preprintarticle.asp?id=250866 (accessed on 12 August 2019).
- Chinnery, H.R.; Naranjo Golborne, C.; Downie, L.E. Omega-3 supplementation is neuroprotective to corneal nerves in dry eye disease: A pilot study. Ophthalmic Physiol. Opt. J. Br. Coll. Ophthalmic Opt. (Optom.) 2017, 37, 473–481. [Google Scholar] [CrossRef] [PubMed]
- Schmidl, D.; Werkmeister, R.; Kaya, S.; Unterhuber, A.; Witkowska, K.J.; Baumgartner, R.; Holler, S.; O’Rourke, M.; Peterson, W.; Wolter, A.; et al. A Controlled, Randomized Double-Blind Study to Evaluate the Safety and Efficacy of Chitosan-N-Acetylcysteine for the Treatment of Dry Eye Syndrome. J. Ocul. Pharmacol. Ther. Off. J. Assoc. Ocul. Pharmacol. Ther. 2017, 33, 375–382. [Google Scholar] [CrossRef] [PubMed]
- Steven, P.; Augustin, A.J.; Geerling, G.; Kaercher, T.; Kretz, F.; Kunert, K.; Menzel-Severing, J.; Schrage, N.; Schrems, W.; Krosser, S.; et al. Semifluorinated Alkane Eye Drops for Treatment of Dry Eye Disease Due to Meibomian Gland Disease. J. Ocul. Pharmacol. Ther. Off. J. Assoc. Ocul. Pharmacol. Ther. 2017, 33, 67–685. [Google Scholar] [CrossRef] [PubMed]
- Toshida, H.; Funaki, T.; Ono, K.; Tabuchi, N.; Watanabe, S.; Seki, T.; Otake, H.; Kato, T.; Ebihara, N.; Murakami, A. Efficacy and safety of retinol palmitate ophthalmic solution in the treatment of dry eye: A Japanese Phase II clinical trial. Drug Des. Dev. Ther. 2017, 11, 1871–1879. [Google Scholar] [CrossRef]
- Wang, D.H.; Liu, X.Q.; Hao, X.J.; Zhang, Y.J.; Zhu, H.Y.; Dong, Z.G. Effect of the Meibomian Gland Squeezer for Treatment of Meibomian Gland Dysfunction. Cornea 2018, 37, 1270–1278. [Google Scholar] [CrossRef] [PubMed]
- Chi, S.C.; Tuan, H.I.; Kang, Y.N. Effects of Polyunsaturated Fatty Acids on Nonspecific Typical Dry Eye Disease: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Nutrients 2019, 11, 5. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Kam, W.R.; Sullivan, D.A. Influence of Omega 3 and 6 Fatty Acids on Human Meibomian Gland Epithelial Cells. Cornea 2016, 35, 1122–1126. [Google Scholar] [CrossRef] [Green Version]
- Oleñik, A.; Mahillo-Fernández, I.; Alejandre-Alba, N.; Fernández-Sanz, G.; Pérez, M.A.; Luxan, S.; Quintana, S.; Martínez de Carneros Llorente, A.; García-Sandoval, B.; Jiménez-Alfaro, I. Benefits of omega-3 fatty acid dietary supplementation on health-related quality of life in patients with meibomian gland dysfunction. Clin. Ophthalmol. (Auckl. N.Z.) 2014, 8, 831–836. [Google Scholar] [CrossRef] [Green Version]
- Asbell, P.A.; Maguire, M.G.; Pistilli, M.; Ying, G.S.; Szczotka-Flynn, L.B.; Hardten, D.R.; Lin, M.C.; Shtein, R.M. n-3 Fatty Acid Supplementation for the Treatment of Dry Eye Disease. New Engl. J. Med. 2018, 378, 1681–1690. [Google Scholar]
- Hongyok, T.; Chae, J.J.; Shin, Y.J.; Na, D.; Li, L.; Chuck, R.S. Effect of chitosan-N-acetylcysteine conjugate in a mouse model of botulinum toxin B-induced dry eye. Arch. Ophthalmol. (Chic. Ill. 1960) 2009, 127, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Fischak, C.; Klaus, R.; Werkmeister, R.M.; Hohenadl, C.; Prinz, M.; Schmetterer, L.; Garhofer, G. Effect of Topically Administered Chitosan-N-acetylcysteine on Corneal Wound Healing in a Rabbit Model. J. Ophthalmol. 2017, 2017, 5192924. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.C.; Kim, T.K.; Park, S.H.; Kim, M.S. The wound healing effects of vitamin A eye drops after a corneal alkali burn in rats. Acta Ophthalmol. 2012, 90, e540–e546. [Google Scholar] [CrossRef] [PubMed]
- Odaka, A.; Toshida, H.; Ohta, T.; Tabuchi, N.; Koike, D.; Suto, C.; Murakami, A. Efficacy of retinol palmitate eye drops for dry eye in rabbits with lacrimal gland resection. Clin. Ophthalmol. (Auckl. N.Z.) 2012, 6, 1585–1593. [Google Scholar] [Green Version]
- Kobayashi, T.K.; Tsubota, K.; Takamura, E.; Sawa, M.; Ohashi, Y.; Usui, M. Effect of retinol palmitate as a treatment for dry eye: A cytological evaluation. Ophthalmol. J. Int. D’ophtalmologie Int. J. Ophthalmol. Z. fur Augenheilkd. 1997, 211, 358–361. [Google Scholar] [CrossRef]
- Fan, N.W.; Ho, T.C.; Lin, E.H.; Wu, C.W.; Chien, H.Y.; Tsao, Y.P. Pigment epithelium-derived factor peptide reverses mouse age-related meibomian gland atrophy. Exp. Eye Res. 2019, 185, 107678. [Google Scholar] [CrossRef]
- Hu, W.L.; Wu, P.C.; Pan, L.Y.; Yu, H.J.; Pan, C.C.; Hung, Y.C. Effect of laser acupuncture on dry eye: A study protocol for a 2-center randomized controlled trial. Medicine 2018, 97, e10875. [Google Scholar] [CrossRef]
- Wang, C.; Ding, W.; Yu, Y.; Zhang, B.; Xu, D.; Zhang, C. Comparison effects of acupuncture at distal acupoints and local acupoints on treatment of xerophthalmia. Zhongguo Zhen Jiu Chin. Acupunct. Moxibustion 2017, 37, 1069–1072. [Google Scholar]
- Zhang, X.; Liu, Z.; Ding, W.; Zhang, J.; Shi, H.; Zhu, W. Efficacy and safety of acupuncture at a single BL1 acupoint in the treatment of moderate to severe dry eye disease: Protocol for a randomized, controlled trial. Medicine 2018, 97, e10924. [Google Scholar] [CrossRef]
- Benitez-Del-Castillo, J.M.; Moreno-Montanes, J.; Jimenez-Alfaro, I.; Munoz-Negrete, F.J.; Turman, K.; Palumaa, K.; Sadaba, B.; Gonzalez, M.V.; Ruz, V.; Vargas, B.; et al. Safety and Efficacy Clinical Trials for SYL1001, a Novel Short Interfering RNA for the Treatment of Dry Eye Disease. Investig. Ophthalmol. Vis. Sci. 2016, 57, 6447–6454. [Google Scholar] [CrossRef] [Green Version]
- Szallasi, A.; Cortright, D.N.; Blum, C.A.; Eid, S.R. The vanilloid receptor TRPV1: 10 years from channel cloning to antagonist proof-of-concept. Nat. Rev. Drug Discov. 2007, 6, 357–372. [Google Scholar] [CrossRef] [PubMed]
- Chang, R.; Wang, P.Y.; Tseng, C.L. New Combination/Application of Polymer-Based Nanoparticles for Biomedical Engineering. Adv. Exp. Med. Biol. 2018, 1078, 271–290. [Google Scholar] [PubMed]
- Huang, H.Y.; Wang, M.C.; Chen, Z.Y.; Chiu, W.Y.; Chen, K.H.; Lin, I.C.; Yang, W.V.; Wu, C.C.; Tseng, C.L. Gelatin-epigallocatechin gallate nanoparticles with hyaluronic acid decoration as eye drops can treat rabbit dry-eye syndrome effectively via inflammatory relief. Int. J. Nanomed. 2018, 13, 7251–7273. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Chang, C.N.; Verma, M.S.; Hileeto, D.; Muntz, A.; Stahl, U.; Woods, J.; Jones, L.W.; Gu, F.X. Phenylboronic acid modified mucoadhesive nanoparticle drug carriers facilitate weekly treatment of experimentallyinduced dry eye syndrome. Nano Res. 2015, 8, 621–635. [Google Scholar] [CrossRef]
- Contreras-Ruiz, L.; Zorzi, G.K.; Hileeto, D.; López-García, A.; Calonge, M.; Seijo, B.; Sánchez, A.; Diebold, Y. A nanomedicine to treat ocular surface inflammation: Performance on an experimental dry eye murine model. Gene Ther. 2012, 20, 467. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.J.; Luo, L.J.; G Harroun, S.; Wei, S.C.; Unnikrishnan, B.; Chang, H.T.; Huang, Y.F.; Lai, J.Y.; Huang, C.C. Synergistically dual-functional nano eye-drops for simultaneous anti-inflammatory and anti-oxidative treatment of dry eye disease. Nanoscale 2019, 11, 5580–5594. [Google Scholar] [CrossRef] [PubMed]
- Vickers, L.A.; Gupta, P.K. The Future of Dry Eye Treatment: A Glance into the Therapeutic Pipeline. Ophthalmol. Ther. 2015, 4, 69–78. [Google Scholar] [CrossRef]
- Luo, L.J.; Lai, J.Y. Epigallocatechin Gallate-Loaded Gelatin-g-Poly(N-Isopropylacrylamide) as a New Ophthalmic Pharmaceutical Formulation for Topical Use in the Treatment of Dry Eye Syndrome. Sci. Rep. 2017, 7, 9380. [Google Scholar] [CrossRef]
- Wagh, V.D.; Apar, D.U. Cyclosporine A Loaded PLGA Nanoparticles for Dry Eye Disease: In Vitro Characterization Studies. J. Nanotechnol. 2014, 2014, 10. [Google Scholar] [CrossRef]
- Yu, Y.; Chen, D.; Li, Y.; Yang, W.; Tu, J.; Shen, Y. Improving the topical ocular pharmacokinetics of lyophilized cyclosporine A-loaded micelles: Formulation, in vitro and in vivo studies. Drug Deliv. 2018, 25, 888–899. [Google Scholar] [CrossRef]
- Di Tommaso, C.; Valamanesh, F.; Miller, F.; Furrer, P.; Rodriguez-Aller, M.; Behar-Cohen, F.; Gurny, R.; Moller, M. A novel cyclosporin a aqueous formulation for dry eye treatment: In vitro and in vivo evaluation. Investig. Ophthalmol. Vis. Sci. 2012, 53, 2292–2299. [Google Scholar] [CrossRef] [PubMed]
- Acar, D.; Molina-Martinez, I.T.; Gomez-Ballesteros, M.; Guzman-Navarro, M.; Benitez-Del-Castillo, J.M.; Herrero-Vanrell, R. Novel liposome-based and in situ gelling artificial tear formulation for dry eye disease treatment. Contact Lens Anterior Eye J. Br. Contact Lens Assoc. 2018, 41, 93–96. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Assessment Tool | Evaluation | Ref. |
|---|---|---|
| Corneal fluorescein staining | Corneal and conjunctival vital dye staining (fluorescein/rose Bengal) to identify and track ocular-surface changes at the cellular level. | [5] |
| Schirmer test | Measurement of tear volume by placing a paper test strip in the lateral third of the lower eyelid after drying the inferior fornix, then measuring the length of the moistened portion of the strip after 5 min. | [9] |
| Tear osmolarity | Measurement of solutes of tear film (e.g., TearLab™ osmolarity system) | [10] |
| Tear film stability | Fluorescein tear break-up time widely used to assess tear film stability and reflect different pathophysiologies by break-up pattern. | [11,12] |
| Tear film interferometry | Assessment of the thickness of the superficial lipid layer that floats upon the tear film and of the fluid layer that covers the anterior surface of contact lenses (to reflect clinical tear dynamics of DED | [13,14] |
| Meibomian gland grading | Grading of Meibomian gland dysfunction according to clinical features and gland expression | [15] |
| Inflammation examination | Measurement of matrix metalloproteinase 9 (MMP9) level in the tear film to identify patients with ocular surface inflammation and autoimmune disease (levels >40 ng/mL indicate ocular surface inflammation) | [16,17] |
| Questionnaires to check patient’s lifestyle or suffering history | Questionnaires assessing patient’s subjective experience of DED in order to get more objective and reproducible data as reference to diagnosis:, model questionnaire can be acquired from: - National Eye Institute Visual Function Questionnaire-25 (NEI-VFQ25) - Ocular Surface Disease Index (OSDI) - Subject Global Assessment scale - Standard Patient Evaluation of Eye Dryness Questionnaire (SPEED) - Canadian Dry Eye Epidemiology Study (CANDEES) - Dry Eye Screening for Dry Eye Epidemiology Projects (DEEP) - Dry Eye Questionnaire (DEQ) - Contact Lens Dry Eye Questionnaire (CLDEQ) - Impact of Dry Eye in Everyday Life (IDEEL) - McCarty Symptom Questionnaire - McMonnies Questionnaire - Ocular Comfort Index (OCI) - Symptom Assessment In Dry Eye (SANDE) - Schein Questionnaire - Texas Eye Research and Technology Center Dry Eye Questionnaire (TERTC-DEQ) | [7,18,19,20] |
| Polymer/Material | Drug | Treatment Effects | Ref. |
|---|---|---|---|
| Gelatin | MUC5AC protein (pMUC5AC) |
| [191] |
| Gelatin, hyaluronic acid (HA) | Epigallocatechin gallate (EGCG) |
| [207] |
| Gelatin-g-Poly(N-isopropylacrylamide) (GN) | Epigallocatechin gallate (EGCG) |
| [212] |
| Poly (d,l-lactide), Dextran and 3-aminophenylboronic acid monohydrate (PLA-b-Dex-g-PBA) | Cyclosporine A (CsA) |
| [190] |
| Poly(d,l-lactide-co-glycolide) (PLGA) | CsA |
| [213] |
| (ethylene glycol)-poly (lactide) polymer (mPEG-PLA) | CsA |
| [214] |
| Methoxy-poly(ethylene glycol), hexyl-substituted poly(lactides) (MPEG-hexPLA) | CsA |
| [215] |
| Poly(catechin) capped- gold nanoparticles (Au@Poly-CH NPs) | Amfenac [AF; a nonsteroidal antiinflammatory drug (NSAID)] |
| [192] |
| Phosphatidylcholine, cholesterol/gellan gum, hydroxypropyl methylcellulose, levocarnitine | Vitamins A and E |
| [216] |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuo, Y.-K.; Lin, I.-C.; Chien, L.-N.; Lin, T.-Y.; How, Y.-T.; Chen, K.-H.; Dusting, G.J.; Tseng, C.-L. Dry Eye Disease: A Review of Epidemiology in Taiwan, and its Clinical Treatment and Merits. J. Clin. Med. 2019, 8, 1227. https://doi.org/10.3390/jcm8081227
Kuo Y-K, Lin I-C, Chien L-N, Lin T-Y, How Y-T, Chen K-H, Dusting GJ, Tseng C-L. Dry Eye Disease: A Review of Epidemiology in Taiwan, and its Clinical Treatment and Merits. Journal of Clinical Medicine. 2019; 8(8):1227. https://doi.org/10.3390/jcm8081227
Chicago/Turabian StyleKuo, Yu-Kai, I-Chan Lin, Li-Nien Chien, Tzu-Yu Lin, Ying-Ting How, Ko-Hua Chen, Gregory J. Dusting, and Ching-Li Tseng. 2019. "Dry Eye Disease: A Review of Epidemiology in Taiwan, and its Clinical Treatment and Merits" Journal of Clinical Medicine 8, no. 8: 1227. https://doi.org/10.3390/jcm8081227