Recent Updates on Molecular Imaging Reporting and Data Systems (MI-RADS) for Theranostic Radiotracers—Navigating Pitfalls of SSTR- and PSMA-Targeted PET/CT

Abstract
:1. Theranostic Radiotracers for Neuroendocrine Tumors and Prostate Carcinoma
2. Common Pitfalls on SSTR- and PSMA-PET/CT
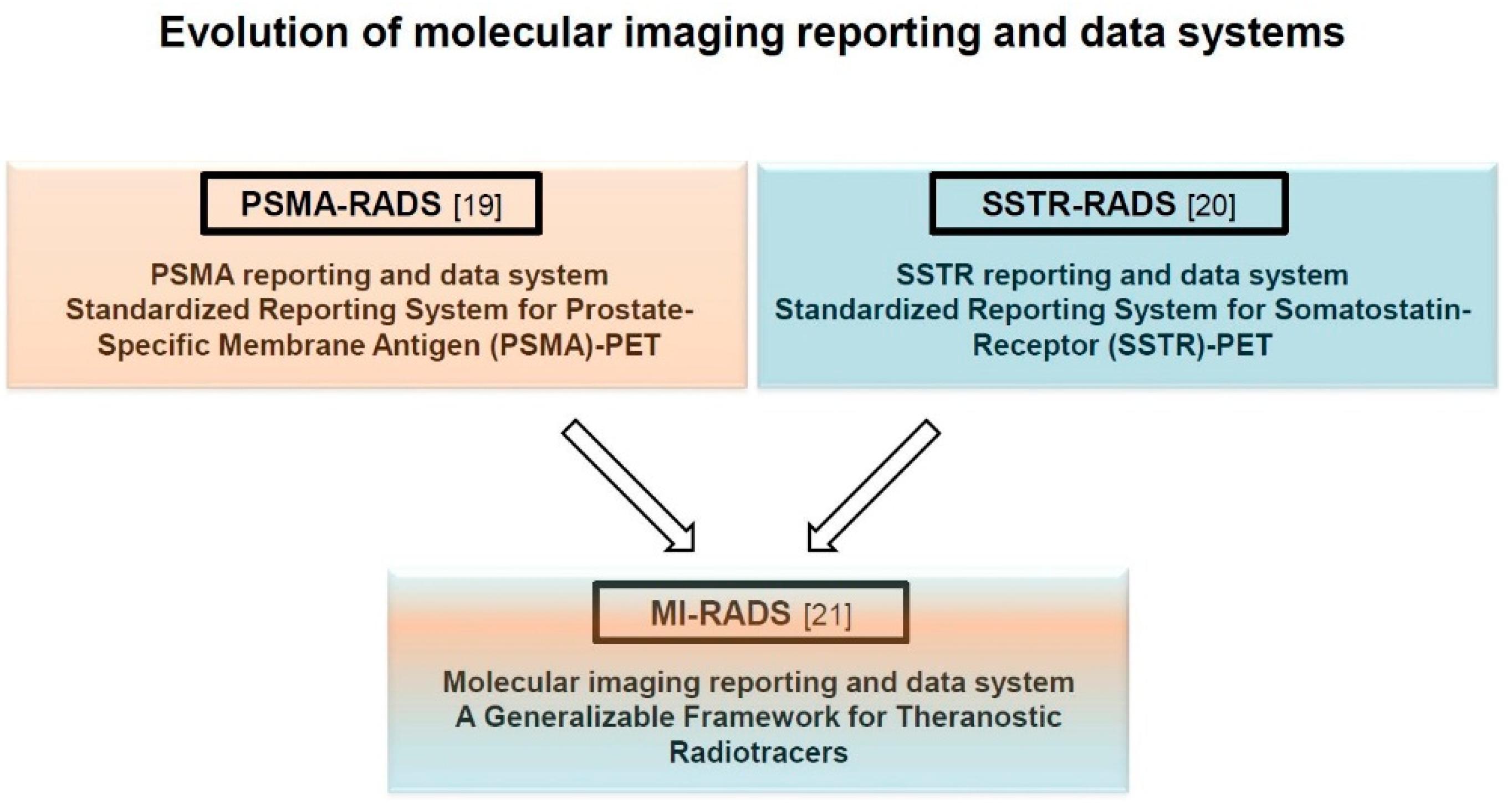
3. Structured Reporting Systems for Theranostic Radiotracers—MI-RADS
3.1. MI-RADS 1.0.
3.2. SSTR-RADS 1.0.
3.3. PSMA-RADS 1.0.
4. Conclusions
Funding
Conflicts of Interest
References
- Werner, R.A.; Bluemel, C.; Allen-Auerbach, M.S.; Higuchi, T.; Herrmann, K. 68 Gallium- and 90 Yttrium-/ 177Lutetium: “Theranostic Twins” for diagnosis and treatment of NETs. Ann. Nucl. Med. 2015, 29, 1–7. [Google Scholar] [CrossRef]
- Rahbar, K.; Ahmadzadehfar, H.; Kratochwil, C.; Haberkorn, U.; Schafers, M.; Essler, M.; Baum, R.P.; Kulkarni, H.R.; Schmidt, M.; Drzezga, A.; et al. German Multicenter study investigating 177Lu-PSMA-617 radioligand therapy in advanced prostate cancer patients. J. Nucl. Med. 2017, 58, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Eiber, M.; Maurer, T.; Souvatzoglou, M.; Beer, A.J.; Ruffani, A.; Haller, B.; Graner, F.P.; Kubler, H.; Haberkorn, U.; Eisenhut, M.; et al. Evaluation of Hybrid (6)(8)Ga-PSMA Ligand PET/CT in 248 patients with biochemical recurrence after radical prostatectomy. J. Nucl. Med. 2015, 56, 668–674. [Google Scholar] [CrossRef] [PubMed]
- Werner, R.A.; Ilhan, H.; Lehner, S.; Papp, L.; Zsoter, N.; Schatka, I.; Muegge, D.O.; Javadi, M.S.; Higuchi, T.; Buck, A.K.; et al. Pre-therapy somatostatin receptor-based heterogeneity predicts overall survival in pancreatic neuroendocrine tumor patients undergoing peptide receptor radionuclide therapy. Mol. Imaging Biol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Werner, R.A.; Weich, A.; Kircher, M.; Solnes, L.B.; Javadi, M.S.; Higuchi, T.; Buck, A.K.; Pomper, M.G.; Rowe, S.P.; Lapa, C. The theranostic promise for neuroendocrine tumors in the late 2010s-Where do we stand, where do we go? Theranostics 2018, 8, 6088–6100. [Google Scholar] [CrossRef] [PubMed]
- Strosberg, J.; El-Haddad, G.; Wolin, E.; Hendifar, A.; Yao, J.; Chasen, B.; Mittra, E.; Kunz, P.L.; Kulke, M.H.; Jacene, H.; et al. Phase 3 Trial of (177) Lu-Dotatate for Midgut Neuroendocrine Tumors. N. Engl. J. Med. 2017, 376, 125–135. [Google Scholar] [CrossRef]
- Strosberg, J.; Wolin, E.; Chasen, B.; Kulke, M.; Bushnell, D.; Caplin, M.; Baum, R.P.; Kunz, P.; Hobday, T.; Hendifar, A.; et al. Health-related quality of life in patients with progressive midgut neuroendocrine tumors treated with (177) Lu-Dotatate in the Phase III NETTER-1 trial. J. Clin. Oncol. 2018, 36, 2578–2584. [Google Scholar] [CrossRef] [PubMed]
- Rahbar, K.; Afshar-Oromieh, A.; Jadvar, H.; Ahmadzadehfar, H. PSMA theranostics: Current status and future directions. Mol. Imaging 2018, 17, 1536012118776068. [Google Scholar] [CrossRef]
- Hofman, M.S.; Violet, J.; Hicks, R.J.; Ferdinandus, J.; Thang, S.P.; Akhurst, T.; Iravani, A.; Kong, G.; Ravi Kumar, A.; Murphy, D.G.; et al. [(177)Lu]-PSMA-617 radionuclide treatment in patients with metastatic castration-resistant prostate cancer (LuPSMA trial): A single-centre, single-arm, phase 2 study. Lancet Oncol. 2018, 19, 825–833. [Google Scholar] [CrossRef]
- Boyer, B.; Canale, S.; Arfi-Rouche, J.; Monzani, Q.; Khaled, W.; Balleyguier, C. Variability and errors when applying the BIRADS mammography classification. Eur. J. Radiol. 2013, 82, 388–397. [Google Scholar] [CrossRef]
- Balleyguier, C.; Ayadi, S.; Van Nguyen, K.; Vanel, D.; Dromain, C.; Sigal, R. BIRADS classification in mammography. Eur. J. Radiol. 2007, 61, 192–194. [Google Scholar] [CrossRef] [PubMed]
- Robinson, P.J. Radiology’s Achilles’ heel: Error and variation in the interpretation of the Rontgen image. Br. J. Radiol. 1997, 70, 1085–1098. [Google Scholar] [CrossRef] [PubMed]
- Ganeshan, D.; Duong, P.T.; Probyn, L.; Lenchik, L.; McArthur, T.A.; Retrouvey, M.; Ghobadi, E.H.; Desouches, S.L.; Pastel, D.; Francis, I.R. Structured reporting in radiology. Acad. Radiol. 2018, 25, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Young, D.S. Standardized reporting of laboratory data: The desirability of using SI units. N. Engl. J. Med. 1974, 290, 368–373. [Google Scholar] [CrossRef] [PubMed]
- D’Orsi, C.J.; Kopans, D.B. Mammography interpretation: The BI-RADS method. Am. Fam. Phys. 1997, 55, 1548–1550, 1552. [Google Scholar]
- Tessler, F.N.; Middleton, W.D.; Grant, E.G.; Hoang, J.K.; Berland, L.L.; Teefey, S.A.; Cronan, J.J.; Beland, M.D.; Desser, T.S.; Frates, M.C.; et al. ACR thyroid imaging, reporting and data system (TI-RADS): White paper of the ACR TI-RADS Committee. J. Am. Coll. Radiol. 2017, 14, 587–595. [Google Scholar] [CrossRef] [PubMed]
- Ceci, F.; Fanti, S. Standardisation of PSMA images interpretation: Why do we need it? Clin. Transl. Imaging 2018, 6, 331. [Google Scholar] [CrossRef]
- Werner, R.A.; Bundschuh, R.A.; Bundschuh, L.; Fanti, S.; Javadi, M.S.; Higuchi, T.; Weich, A.; Pienta, K.J.; Buck, A.K.; Pomper, M.G.; et al. Novel structured reporting systems for theranostic radiotracers. J. Nucl. Med. 2019, 60, 577–584. [Google Scholar] [CrossRef] [PubMed]
- Rowe, S.P.; Pienta, K.J.; Pomper, M.G.; Gorin, M.A. Proposal for a structured reporting system for prostate-specific membrane antigen-targeted PET imaging: PSMA-RADS Version 1.0. J. Nucl. Med. 2018, 59, 479–485. [Google Scholar] [CrossRef]
- Werner, R.A.; Solnes, L.B.; Javadi, M.S.; Weich, A.; Gorin, M.A.; Pienta, K.J.; Higuchi, T.; Buck, A.K.; Pomper, M.G.; Rowe, S.P.; et al. SSTR-RADS Version 1.0 as a reporting system for SSTR PET imaging and selection of potential PRRT candidates: A proposed standardization framework. J. Nucl. Med. 2018, 59, 1085–1091. [Google Scholar] [CrossRef]
- Werner, R.A.; Bundschuh, R.A.; Bundschuh, L.; Javadi, M.S.; Higuchi, T.; Weich, A.; Sheikhbahaei, S.; Pienta, K.J.; Buck, A.K.; Pomper, M.G.; et al. Molecular imaging reporting and data systems (MI-RADS): A generalizable framework for targeted radiotracers with theranostic implications. Ann. Nucl. Med. 2018, 32, 512–522. [Google Scholar] [CrossRef] [PubMed]
- Hofman, M.S.; Lau, W.F.; Hicks, R.J. Somatostatin receptor imaging with 68Ga DOTATATE PET/CT: Clinical utility, normal patterns, pearls, and pitfalls in interpretation. Radiographics 2015, 35, 500–516. [Google Scholar] [CrossRef] [PubMed]
- Werner, R.A.; Sheikhbahaei, S.; Jones, K.M.; Javadi, M.S.; Solnes, L.B.; Ross, A.E.; Allaf, M.E.; Pienta, K.J.; Lapa, C.; Buck, A.K.; et al. Patterns of uptake of prostate-specific membrane antigen (PSMA)-targeted (18)F-DCFPyL in peripheral ganglia. Ann. Nucl. Med. 2017, 31, 696–702. [Google Scholar] [CrossRef] [PubMed]
- Derlin, T.; Schmuck, S.; Juhl, C.; Teichert, S.; Zorgiebel, J.; Wester, H.J.; Schneefeld, S.M.; Walte, A.C.A.; Thackeray, J.T.; Ross, T.L.; et al. Imaging characteristics and first experience of [(68)Ga]THP-PSMA, a novel probe for rapid kit-based Ga-68 labeling and PET imaging: Comparative analysis with [(68)Ga]PSMA I&T. Mol. Imaging Biol. 2018, 20, 650–658. [Google Scholar] [CrossRef]
- Ferreira, G.; Iravani, A.; Hofman, M.S.; Hicks, R.J. Intra-individual comparison of (68)Ga-PSMA-11 and (18)F-DCFPyL normal-organ biodistribution. Cancer Imaging 2019, 19, 23. [Google Scholar] [CrossRef] [PubMed]
- Giesel, F.L.; Hadaschik, B.; Cardinale, J.; Radtke, J.; Vinsensia, M.; Lehnert, W.; Kesch, C.; Tolstov, Y.; Singer, S.; Grabe, N.; et al. F-18 labelled PSMA-1007: Biodistribution, radiation dosimetry and histopathological validation of tumor lesions in prostate cancer patients. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 678–688. [Google Scholar] [CrossRef] [PubMed]
- Sheikhbahaei, S.; Werner, R.A.; Solnes, L.B.; Pienta, K.J.; Pomper, M.G.; Gorin, M.A.; Rowe, S.P. Prostate-specific membrane antigen (PSMA)-targeted pet imaging of prostate cancer: An update on important pitfalls. Semin. Nucl. Med. 2019. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Samnick, S.; Lapa, C.; Israel, I.; Buck, A.K.; Kreissl, M.C.; Bauer, W. 68Ga-DOTATATE PET/CT for the detection of inflammation of large arteries: Correlation with 18F-FDG, calcium burden and risk factors. EJNMMI Res. 2012, 2, 52. [Google Scholar] [CrossRef] [PubMed]
- Schatka, I.; Wollenweber, T.; Haense, C.; Brunz, F.; Gratz, K.F.; Bengel, F.M. Peptide receptor-targeted radionuclide therapy alters inflammation in atherosclerotic plaques. J. Am. Coll. Cardiol. 2013, 62, 2344–2345. [Google Scholar] [CrossRef]
- Lapa, C.; Reiter, T.; Kircher, M.; Schirbel, A.; Werner, R.A.; Pelzer, T.; Pizarro, C.; Skowasch, D.; Thomas, L.; Schlesinger-Irsch, U.; et al. Somatostatin receptor based PET/CT in patients with the suspicion of cardiac sarcoidosis: An initial comparison to cardiac MRI. Oncotarget 2016, 7, 77807–77814. [Google Scholar] [CrossRef]
- Lapa, C.; Reiter, T.; Li, X.; Werner, R.A.; Samnick, S.; Jahns, R.; Buck, A.K.; Ertl, G.; Bauer, W.R. Imaging of myocardial inflammation with somatostatin receptor based PET/CT-A comparison to cardiac MRI. Int. J. Cardiol. 2015, 194, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Brogsitter, C.; Hofmockel, T.; Kotzerke, J. (68) Ga DOTATATE uptake in vertebral hemangioma. Clin. Nucl. Med. 2014, 39, 462–463. [Google Scholar] [CrossRef] [PubMed]
- Thackeray, J.T.; Bankstahl, J.P.; Wang, Y.; Korf-Klingebiel, M.; Walte, A.; Wittneben, A.; Wollert, K.C.; Bengel, F.M. Targeting post-infarct inflammation by PET imaging: Comparison of (68) Ga-citrate and (68) Ga-DOTATATE with (18) F-FDG in a mouse model. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 317–327. [Google Scholar] [CrossRef] [PubMed]
- Tarkin, J.M.; Joshi, F.R.; Evans, N.R.; Chowdhury, M.M.; Figg, N.L.; Shah, A.V.; Starks, L.T.; Martin-Garrido, A.; Manavaki, R.; Yu, E.; et al. Detection of atherosclerotic inflammation by (68) Ga-DOTATATE PET compared to [(18)F]FDG PET imaging. J. Am. Coll. Cardiol. 2017, 69, 1774–1791. [Google Scholar] [CrossRef] [PubMed]
- Yamaga, L.Y.I.; Cunha, M.L.; Campos Neto, G.C.; Garcia, M.R.T.; Yang, J.H.; Camacho, C.P.; Wagner, J.; Funari, M.B.G. (68) Ga-DOTATATE PET/CT in recurrent medullary thyroid carcinoma: A lesion-by-lesion comparison with (111) In-octreotide SPECT/CT and conventional imaging. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 1695–1701. [Google Scholar] [CrossRef] [PubMed]
- Rachinger, W.; Stoecklein, V.M.; Terpolilli, N.A.; Haug, A.R.; Ertl, L.; Poschl, J.; Schuller, U.; Schichor, C.; Thon, N.; Tonn, J.C. Increased 68 Ga-DOTATATE uptake in PET imaging discriminates meningioma and tumor-free tissue. J. Nucl. Med. 2015, 56, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Elgeti, F.; Amthauer, H.; Denecke, T.; Steffen, I.; Heuck, F.; Stelter, L.; Ruf, J. Incidental detection of breast cancer by 68 Ga-DOTATOC-PET/CT in women suffering from neuroendocrine tumours. Nuklearmedizin 2008, 47, 261–265. [Google Scholar]
- Yamaga, L.Y.I.; Wagner, J.; Funari, M.B.G. 68nGa-DOTATATE PET/CT in nonneuroendocrine tumors: A pictorial essay. Clin. Nucl. Med. 2017, 42, e313–e316. [Google Scholar] [CrossRef]
- Ayati, N.; Lee, S.T.; Zakavi, R.; Pathmaraj, K.; Al-Qatawna, L.; Poon, A.; Scott, A.M. Long-acting somatostatin analog therapy differentially alters (68) Ga-DOTATATE uptake in normal tissues compared with primary tumors and metastatic lesions. J. Nucl. Med. 2018, 59, 223–227. [Google Scholar] [CrossRef]
- Cherk, M.H.; Kong, G.; Hicks, R.J.; Hofmann, M.S. Changes in biodistribution on 68 Ga-DOTA-Octreotate PET/CT after long acting somatostatin analogue therapy in neuroendocrine tumour patients may result in pseudoprogression. Cancer Imaging 2018. [Google Scholar] [CrossRef]
- Liu, Y. Super-superscan on a bone scintigraphy. Clin. Nucl. Med. 2011, 36, 227–228. [Google Scholar] [CrossRef] [PubMed]
- Beauregard, J.M.; Hofman, M.S.; Kong, G.; Hicks, R.J. The tumour sink effect on the biodistribution of 68Ga-DOTA-octreotate: Implications for peptide receptor radionuclide therapy. Eur. J. Nucl. Med. Mol. Imaging 2012, 39, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Carbonero, R.; Garcia-Figueiras, R.; Carmona-Bayonas, A.; Sevilla, I.; Teule, A.; Quindos, M.; Grande, E.; Capdevila, J.; Aller, J.; Arbizu, J.; et al. Imaging approaches to assess the therapeutic response of gastroenteropancreatic neuroendocrine tumors (GEP-NETs): Current perspectives and future trends of an exciting field in development. Cancer Metastasis Rev. 2015, 34, 823–842. [Google Scholar] [CrossRef] [PubMed]
- Werner, R.A.; Hanscheid, H.; Leal, J.P.; Javadi, M.S.; Higuchi, T.; Lodge, M.A.; Buck, A.K.; Pomper, M.G.; Lapa, C.; Rowe, S.P. Impact of tumor burden on quantitative [(68)Ga] DOTATOC biodistribution. Mol. Imaging Biol. 2018. [Google Scholar] [CrossRef]
- Rowe, S.P.; Deville, C.; Paller, C.; Cho, S.Y.; Fishman, E.K.; Pomper, M.G.; Ross, A.E.; Gorin, M.A. Uptake of (18)F-DCFPyL in Paget’s disease of bone, an important potential pitfall in clinical interpretation of PSMA PET studies. Tomography 2015, 1, 81–84. [Google Scholar] [CrossRef] [PubMed]
- Vamadevan, S.; Le, K.; Bui, C.; Mansberg, R. Incidental PSMA uptake in an undisplaced fracture of a vertebral body. Clin. Nucl. Med. 2017, 42, 465–466. [Google Scholar] [CrossRef] [PubMed]
- Derlin, T.; Weiberg, D.; Sohns, J.M. Multitracer molecular imaging of paget disease targeting bone remodeling, fatty acid metabolism, and PSMA expression on PET/CT. Clin. Nucl. Med. 2016, 41, 991–992. [Google Scholar] [CrossRef] [PubMed]
- Rischpler, C.; Maurer, T.; Schwaiger, M.; Eiber, M. Intense PSMA-expression using (68) Ga-PSMA PET/CT in a paravertebral schwannoma mimicking prostate cancer metastasis. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 193–194. [Google Scholar] [CrossRef] [PubMed]
- Parihar, A.S.; Vadi, S.K.; Mittal, B.R.; Kumar, R.; Bal, A.; Singh, S.K. 68 Ga-PSMA-HBED-CC-Avid synchronous urinary bladder paraganglioma in a patient with metastatic prostate carcinoma. Clin. Nucl. Med. 2018, 43, e329–e330. [Google Scholar] [CrossRef]
- Gulhane, B.; Ramsay, S.; Fong, W. 68 Ga-PSMA uptake in neurofibromas demonstrated on PET/CT in a Patient with neurofibromatosis Type 1. Clin. Nucl. Med. 2017, 42, 776–778. [Google Scholar] [CrossRef]
- Bhardwaj, H.; Stephens, M.; Bhatt, M.; Thomas, P.A. Prostate-specific membrane antigen PET/CT findings for hepatic hemangioma. Clin. Nucl. Med. 2016, 41, 968–969. [Google Scholar] [CrossRef] [PubMed]
- Derlin, T.; Kreipe, H.H.; Schumacher, U.; Soudah, B. PSMA expression in tumor neovasculature endothelial cells of follicular thyroid adenoma as identified by molecular imaging using 68 Ga-PSMA Ligand PET/CT. Clin. Nucl. Med. 2017, 42, e173–e174. [Google Scholar] [CrossRef] [PubMed]
- Sasikumar, A.; Joy, A.; Nair, B.P.; Pillai, M.R.A.; Madhavan, J. False positive uptake in bilateral gynecomastia on 68 Ga-PSMA PET/CT scan. Clin. Nucl. Med. 2017, 42, e412–e414. [Google Scholar] [CrossRef] [PubMed]
- Kanthan, G.L.; Hsiao, E.; Kneebone, A.; Eade, T.; Schembri, G.P. Desmoid tumor showing intense uptake on 68Ga PSMA-HBED-CC PET/CT. Clin. Nucl. Med. 2016, 41, 508–509. [Google Scholar] [CrossRef] [PubMed]
- Zacho, H.D.; Nielsen, J.B.; Dettmann, K.; Hjulskov, S.H.; Petersen, L.J. 68 Ga-PSMA PET/CT uptake in intramuscular myxoma imitates prostate cancer metastasis. Clin. Nucl. Med. 2017, 42, 487–488. [Google Scholar] [CrossRef] [PubMed]
- Malik, D.; Basher, R.K.; Mittal, B.R.; Jain, T.K.; Bal, A.; Singh, S.K. 68 Ga-PSMA Expression in pseudoangiomatous stromal hyperplasia of the breast. Clin. Nucl. Med. 2017, 42, 58–60. [Google Scholar] [CrossRef] [PubMed]
- Dias, A.H.; Holm Vendelbo, M.; Bouchelouche, K. Prostate-specific membrane antigen PET/CT: Uptake in lymph nodes with active sarcoidosis. Clin. Nucl. Med. 2017, 42, e175–e176. [Google Scholar] [CrossRef] [PubMed]
- Pyka, T.; Weirich, G.; Einspieler, I.; Maurer, T.; Theisen, J.; Hatzichristodoulou, G.; Schwamborn, K.; Schwaiger, M.; Eiber, M. 68 Ga-PSMA-HBED-CC PET for differential diagnosis of suggestive lung lesions in patients with prostate cancer. J. Nucl. Med. 2016, 57, 367–371. [Google Scholar] [CrossRef] [PubMed]
- McGuiness, M.; Sounness, B. 68 Ga-PSMA-Ligand PET/CT uptake in anthracosilicosis. Clin. Nucl. Med. 2017, 42, e431–e432. [Google Scholar] [CrossRef]
- Huang, K.; Baur, A.D.; Furth, C. Prostate-Specific Membrane Antigen-Positive Manifestations of Chronic Beryllium Lung Disease. Clin. Nucl. Med. 2019, 44, 64–65. [Google Scholar] [CrossRef]
- Arora, S.; Prabhu, M.; Damle, N.A.; Bal, C.; Kumar, P.; Nalla, H.; Arun Raj, S.T. Prostate-specific membrane antigen imaging in recurrent medullary thyroid cancer: A New Theranostic Tracer in the Offing? Indian J. Nucl. Med. 2018, 33, 261–263. [Google Scholar] [CrossRef] [PubMed]
- Passah, A.; Arora, S.; Damle, N.A.; Tripathi, M.; Bal, C.; Subudhi, T.K.; Arora, G. 68 Ga-prostate-specific membrane antigen PET/CT in Triple-negative breast cancer. Clin. Nucl. Med. 2018, 43, 460–461. [Google Scholar] [CrossRef] [PubMed]
- Yin, Y.; Campbell, S.P.; Markowski, M.C.; Pierorazio, P.M.; Pomper, M.G.; Allaf, M.E.; Rowe, S.P.; Gorin, M.A. Inconsistent detection of sites of metastatic non-clear cell renal cell carcinoma with PSMA-targeted [(18)F]DCFPyL PET/CT. Mol. Imaging Biol. 2019, 21, 567–573. [Google Scholar] [CrossRef] [PubMed]
- Jochumsen, M.R.; Gormsen, L.C.; Nielsen, G.L. 68 Ga-PSMA avid primary adenocarcinoma of the lung with complementary low 18F-FDG uptake. Clin. Nucl. Med. 2018, 43, 117–119. [Google Scholar] [CrossRef] [PubMed]
- Gaertner, F.C.; Halabi, K.; Ahmadzadehfar, H.; Kurpig, S.; Eppard, E.; Kotsikopoulos, C.; Liakos, N.; Bundschuh, R.A.; Strunk, H.; Essler, M. Uptake of PSMA-ligands in normal tissues is dependent on tumor load in patients with prostate cancer. Oncotarget 2017, 8, 55094–55103. [Google Scholar] [CrossRef] [PubMed]
- Werner, R.A.; Bundschuh, R.A.; Bundschuh, L.; Lapa, C.; Yin, Y.; Javadi, M.S.; Buck, A.K.; Higuchi, T.; Pienta, K.J.; Pomper, M.G.; et al. Semiquantitative parameters in PSMA-targeted PET imaging with 18F-DCFPyL: Impact of tumor burden on normal organ uptake. Mol. Imaging Biol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Rowe, S.P.; Pienta, K.J.; Pomper, M.G.; Gorin, M.A. PSMA-RADS Version 1.0: A step towards standardizing the interpretation and reporting of PSMA-targeted PET imaging studies. Eur. Urol. 2018, 73, 485–487. [Google Scholar] [CrossRef] [PubMed]
- Bodei, L.; Mueller-Brand, J.; Baum, R.P.; Pavel, M.E.; Horsch, D.; O’Dorisio, M.S.; O’Dorisio, T.M.; Howe, J.R.; Cremonesi, M.; Kwekkeboom, D.J.; et al. The joint IAEA, EANM, and SNMMI practical guidance on peptide receptor radionuclide therapy (PRRNT) in neuroendocrine tumours. Eur. J. Nucl. Med. Mol. Imaging 2013, 40, 800–816. [Google Scholar] [CrossRef]
- Fendler, W.P.; Rahbar, K.; Herrmann, K.; Kratochwil, C.; Eiber, M. (177) Lu-PSMA radioligand therapy for prostate cancer. J. Nucl. Med. 2017, 58, 1196–1200. [Google Scholar] [CrossRef]
- Werner, R.A.; Bundschuh, R.A.; Bundschuh, L.; Javadi, M.S.; Leal, J.P.; Higuchi, T.; Pienta, K.J.; Buck, A.K.; Pomper, M.G.; Gorin, M.A.; et al. Interobserver agreement for the standardized reporting system PSMA-RADS 1.0 on (18) F-DCFPyL PET/CT imaging. J. Nucl. Med. 2018, 59, 1857–1864. [Google Scholar] [CrossRef]
- Yin, Y.; Werner, R.A.; Higuchi, T.; Lapa, C.; Pienta, K.J.; Pomper, M.G.; Gorin, M.A.; Rowe, S.P. Follow-up of lesions with equivocal radiotracer uptake on PSMA-targeted PET in patients with prostate cancer: Predictive values of the PSMA-RADS-3A and PSMA-RADS-3B categories. J. Nucl. Med. 2019, 60, 511–516. [Google Scholar] [CrossRef] [PubMed]
- Reyes, D.K.; Demehri, S.; Werner, R.A.; Pomper, M.G.; Gorin, M.A.; Rowe, S.P.; Pienta, K.J. PSMA-targeted [(18)F]DCFPyL PET/CT-avid lesions in a patient with prostate cancer: Clinical decision-making informed by the PSMA-RADS interpretive framework. Urol. Case Rep. 2019, 23, 72–74. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MI-RADS | PSMA- and SSTR-RADS | Workup | Uptake Level # | PRRT/RLT? | |
|---|---|---|---|---|---|
| 1 | 1A | Benign lesion, characterized by biopsy or anatomic imaging without abnormal uptake | n/a | 1 | N |
| 1B | Benign lesion, characterized by biopsy or anatomic imaging with abnormal uptake | n/a | 2–3 | N | |
| 2 | Soft tissue site or bone lesion atypical for metastatic PC or NET | n/a | 1 | N | |
| 3 | 3A | Equivocal uptake in soft tissue lesion typical of PC or NET | B, F/U | 1–2 | N |
| 3B | Equivocal uptake in bone lesion not atypical of PC or NET | B, F/U | 1–2 | N | |
| 3C | Intense uptake in site highly atypical of all but advanced stages of PC or NET (i.e., high likelihood of nonprostatic/non-NET malignancy or other benign tumor) | B | 3 | N | |
| 3D | Lesion suggestive of malignancy on anatomic imaging but lacking uptake. For SSTR-RADS: 18F-FDG is recommended to rule out potential dedifferentiation | B, F/U | not available | N | |
| 4 | Intense uptake in site typical of PC or NET but lacking definitive findings on conventional imaging | n/a | 3 | Y | |
| 5 | Intense uptake in site typical of PC or NET and with definitive findings on conventional imaging | n/a | 3 | Y | |
| MI-RADS | Examples on SSTR-PET/CT | Examples on PSMA-PET/CT | |
|---|---|---|---|
| 1 | 1A | Normal physiologic biodistribution of an SSTR imaging agent [20] | Normal physiologic biodistribution of a PSMA imaging agent [19] |
| 1B | - Prostatitis [20] - Benign prostatic hyperplasia [20] - Radiotracer-avid liver lesion, with magnetic resonance imaging findings compatible with hemangioma [20] | - Thyroid nodules with uptake that have been previously biopsied and found to be benign [19] - Liver hemangioma with focal uptake that have been characterized with liver protocol CT or MRI [19] - Adrenal adenoma with radiotracer uptake with characteristic conventional imaging findings [19] | |
| 2 | - Axillary lymph nodes [20] - Schmorl’s node in a vertebral body [20] | - Isolated mediastinal or axillary lymph nodes with minimal uptake, healing fractures [19] - Focal splenic uptake [21] | |
| 3 | 3A | - Regional lymph nodes, e.g. low-level uptake in mesenteric lymph node in midabdomen [20] - Mild radiotracer uptake in a supraclavicular lymph node [5] | - Pelvic lymph node involvement with low-level uptake [19] |
| 3B | - Low-level uptake in a rib with lack of anatomic correlate [20] | - Low level-uptake in the iliac bone with lack of anatomic correlate [19] | |
| 3C | - Intense breast uptake on SSTR-PET [20,21] - Intense uptake in the Musculus vastus lateralis [18] | - High level of radiotracer uptake in a lung nodule in a patient with low level of serum prostate-specific antigen [19] - Substernal thyroid nodule with radiotracer uptake (and without further work-up) [21,72] | |
| 3D | - Single liver lesion without SSTR expression but finding on conventional imaging [20] - Modest/No radiotracer uptake in the primary of the lung, with intense radiotracer uptake on 2-deoxy-2-18F-fluoro-d-glucose PET two weeks later [18] | - Prostate cancer (PC) of neuroendocrine origin [19] - Non-radiotracer-avid lung nodule in a patient with biochemically recurrent PC [19] | |
| 4 | - Intense uptake in a liver lesion without definitive findings on conventional imaging [20] | - Intense radiotracer uptake in a lymph node without definitive findings on conventional imaging [19] | |
| 5 | - Intense uptake in a liver lesion with definitive findings on conventional imaging [20] | - Extensive metastatic PC with diffuse osseous metastatic disease and intense radiotracer uptake (“superscan“ on PSMA-PET/CT) [19] | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Werner, R.A.; Thackeray, J.T.; Pomper, M.G.; Bengel, F.M.; Gorin, M.A.; Derlin, T.; Rowe, S.P. Recent Updates on Molecular Imaging Reporting and Data Systems (MI-RADS) for Theranostic Radiotracers—Navigating Pitfalls of SSTR- and PSMA-Targeted PET/CT. J. Clin. Med. 2019, 8, 1060. https://doi.org/10.3390/jcm8071060
Werner RA, Thackeray JT, Pomper MG, Bengel FM, Gorin MA, Derlin T, Rowe SP. Recent Updates on Molecular Imaging Reporting and Data Systems (MI-RADS) for Theranostic Radiotracers—Navigating Pitfalls of SSTR- and PSMA-Targeted PET/CT. Journal of Clinical Medicine. 2019; 8(7):1060. https://doi.org/10.3390/jcm8071060
Chicago/Turabian StyleWerner, Rudolf A., James T. Thackeray, Martin G. Pomper, Frank M. Bengel, Michael A. Gorin, Thorsten Derlin, and Steven P. Rowe. 2019. "Recent Updates on Molecular Imaging Reporting and Data Systems (MI-RADS) for Theranostic Radiotracers—Navigating Pitfalls of SSTR- and PSMA-Targeted PET/CT" Journal of Clinical Medicine 8, no. 7: 1060. https://doi.org/10.3390/jcm8071060