Management of Malnutrition in Older Patients—Current Approaches, Evidence and Open Questions

 , , , ,
, , , ,
Abstract
:1. Malnutrition in Geriatric Patients
1.1. Prevalence
1.2. Etiology
1.3. Consequences
2. Management of Malnutrition
2.1. General Aims and Options
- Maintenance or improvement of nutritional status, which may replenish the protein and energy storage that is necessary to accommodate the needs induced by a metabolic stress;
- Maintenance or improvement of function and capacity for rehabilitation; this is mostly related to the muscle compartment including muscle mass. Activities of daily living but also community living may therefore be secondary aims;
- Maintenance or improvement of health-related quality of life, probably more important, compared to the reduction in mortality, than in younger adults; restoring food intake may play a direct role as being an important mediator of pleasure and well-being;
- Reduction of morbidity, including an improved outcome of underlying chronic diseases;
- Reduction of mortality as a consequence of morbidity reduction but also by increasing treatment tolerability of the underlying chronic disease (e.g., cancer);
- Reduction of malnutrition-associated costs (reduction of the hospital length of stay, the need for subacute care stays, reduction of nursing home admissions, the number of medical examinations and prescriptions).
2.2. Current Recommendations and Evidence: ESPEN Guidelines 2019
2.2.1. Basic Recommendations
2.2.2. Supportive Interventions
2.2.3. Nutritional Counselling
2.2.4. Food Modification
2.2.5. Oral Nutritional Supplements (ONS)
2.2.6. Enteral and Parenteral Nutrition
2.2.7. Relevance of the Refeeding Syndrome (RFS)
2.3. New Evidence after the ESPEN Guidelines
3. Knowledge Gaps
3.1. Lacking Evidence in Many Fields
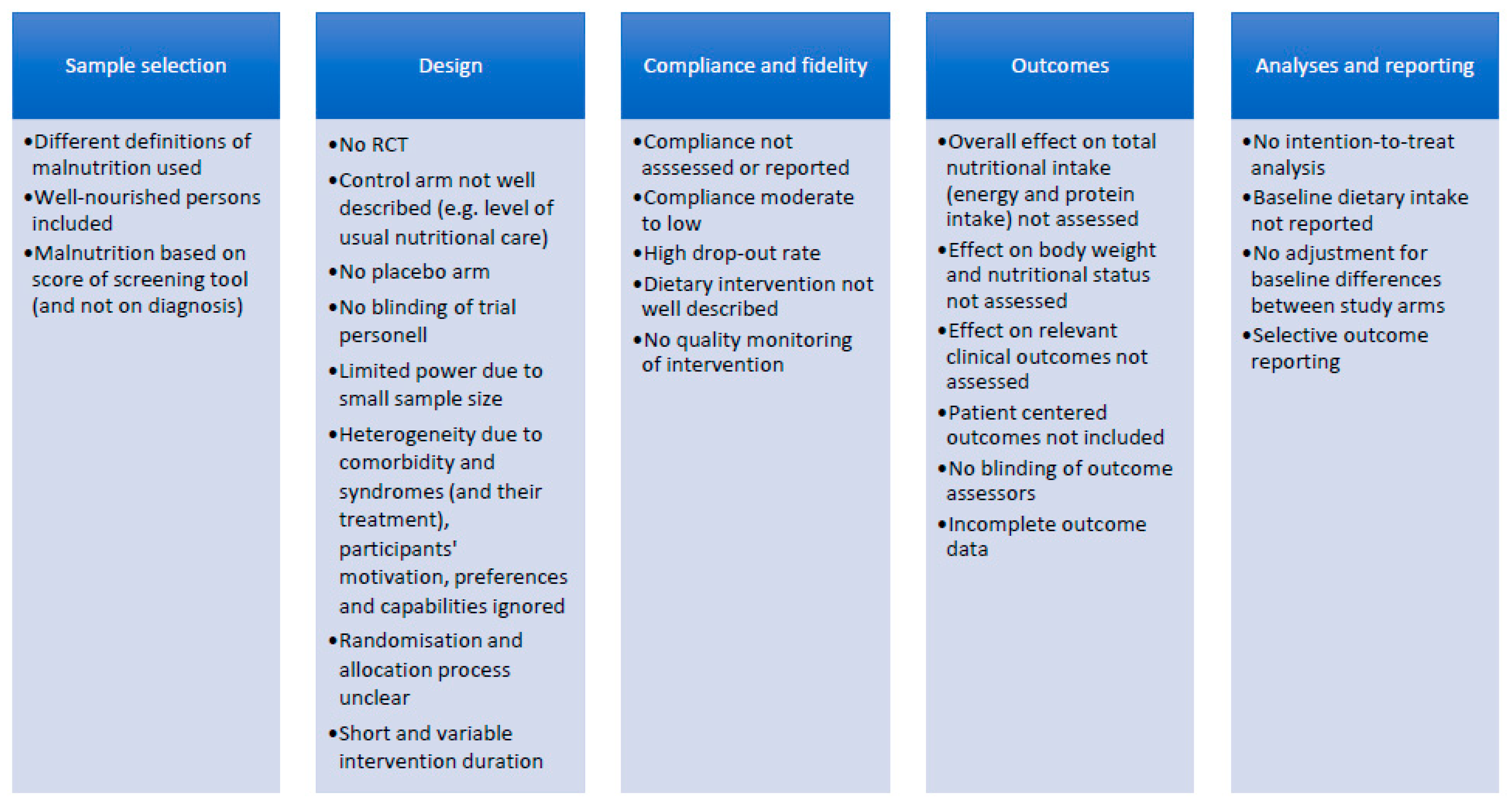
3.2. Limitations of Existing Studies
3.3. Open Questions and Research Needs
4. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Inouye, S.K.; Studenski, S.; Tinetti, M.E.; Kuchel, G.A. Geriatric Syndromes: Clinical, Research and Policy Implications of a Core Geriatric Concept. J. Am. Geriatr. Soc. 2007, 55, 780–791. [Google Scholar] [CrossRef] [PubMed]
- Cereda, E.; Pedrolli, C.; Klersy, C.; Bonardi, C.; Quarleri, L.; Cappello, S.; Turri, A.; Rondanelli, M.; Caccialanza, R. Nutritional status in older persons according to healthcare setting: A systematic review and meta-analysis of prevalence data using MNA ®. Clin. Nutr. 2016, 35, 1282–1290. [Google Scholar] [CrossRef] [PubMed]
- Lacau St. Guily, J.L.S.; Bouvard, É.; Raynard, B.; Goldwasser, F.; Maget, B.; Prevost, A.; Seguy, D.; Romano, O.; Narciso, B.; Couet, C.; et al. NutriCancer: A French observational multicentre cross-sectional study of malnutrition in elderly patients with cancer. J. Geriatr. Oncol. 2018, 9, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Cereda, E.; Veronese, N.; Caccialanza, R. The final word on nutritional screening and assessment in older persons. Curr. Opin. Clin. Nutr. Metab. Care 2018, 21, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, M.J.; Bauer, J.M.; Rämsch, C.; Uter, W.; Guigoz, Y.; Cederholm, T.; Thomas, D.R.; Anthony, P.S.; Charlton, K.E.; Maggio, M.; et al. Frequency of Malnutrition in Older Adults: A Multinational Perspective Using the Mini Nutritional Assessment. J. Am. Geriatr. Soc. 2010, 58, 1734–1738. [Google Scholar] [CrossRef] [PubMed]
- Clarke, D.M.; Strauss, B.J.G.; Wahlqvist, M.L. Undereating and undernutrition in old age: Integrating bio-psychosocial aspects. Age Ageing 1998, 27, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Wolters, M.; Volkert, D.; Streicher, M.; Kiesswetter, E.; Torbahn, G.; O’Connor, E.M.; O’Keeffe, M.; Kelly, M.; O’Herlihy, E.; O’Toole, P.W.; et al. Prevalence of malnutrition using harmonized definitions in older adults from different settings—A MaNuEL study. Clin. Nutr. 2018. [Google Scholar] [CrossRef] [PubMed]
- Cederholm, T.; Jensen, G.L.; Correia, M.I.T.D.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.; et al. GLIM criteria for the diagnosis of malnutrition–A consensus report from the global clinical nutrition community. Clin. Nutr. 2019, 38, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Cederholm, T.; Bosaeus, I.; Barazzoni, R.; Bauer, J.; Van Gossum, A.; Klek, S.; Muscaritoli, M.; Nyulasi, I.; Ockenga, J.; Schneider, S.; et al. Diagnostic criteria for malnutrition–An ESPEN Consensus Statement. Clin. Nutr. 2015, 34, 335–340. [Google Scholar] [CrossRef]
- Schneider, S.M.; Al-Jaouni, R.; Pivot, X.; Braulio, V.B.; Rampal, P.; Hebuterne, X. Lack of adaptation to severe malnutrition in elderly patients. Clin. Nutr. 2002, 21, 499–504. [Google Scholar] [CrossRef]
- Agarwal, E.; Miller, M.; Yaxley, A.; Isenring, E. Malnutrition in the elderly: A narrative review. Maturitas 2013, 76, 296–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malafarina, V.; Uriz-Otano, F.; Gil-Guerrero, L.; Iniesta, R. The anorexia of ageing: Physiopathology, prevalence, associated comorbidity and mortality. A systematic review. Maturitas 2013, 74, 293–302. [Google Scholar] [CrossRef] [PubMed]
- Landi, F.; Picca, A.; Calvani, R.; Marzetti, E. Anorexia of Aging: Assessment and Management. Clin. Geriatr. Med. 2017, 33, 315–323. [Google Scholar] [CrossRef] [PubMed]
- O’Keeffe, M.; Kelly, M.; O’Herlihy, E.; O’Toole, P.W.; Kearney, P.M.; Timmons, S.; O’Shea, E.; Stanton, C.; Hickson, M.; Rolland, Y.; et al. Potentially Modifiable Determinants of Malnutrition in Older Adults: A systematic review. Available online: https://www.sciencedirect.com/science/article/pii/S0261561418325755 (accessed on 28 June 219).
- Van Der Pols-Vijlbrief, R.; Wijnhoven, H.A.; Schaap, L.A.; Terwee, C.B.; Visser, M. Determinants of protein–energy malnutrition in community-dwelling older adults: A systematic review of observational studies. Ageing Res. Rev. 2014, 18, 112–131. [Google Scholar] [CrossRef] [PubMed]
- Volkert, D.; Kiesswetter, E.; Cederholm, T.; Donini, L.M.; Eglseer, D.; Norman, K.; Schneider, S.M.; Ströbele-Benschop, N.; Torbahn, G.; Rainer Wirth, R.; et al. Development of a model on Determinants of Malnutrition in Aged Persons (DoMAP) – a MaNuEL project. Gerontol. Geriatr. Med. 2019, 5, 1–8. [Google Scholar] [CrossRef]
- Norman, K.; Pichard, C.; Lochs, H.; Pirlich, M. Prognostic impact of disease-related malnutrition. Clin. Nutr. 2008, 27, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Deutz, N.E.; Ashurst, I.; Ballesteros, M.D.; Bear, D.E.; Cruz-Jentoft, A.J.; Genton, L.; Landi, F.; Laviano, A.; Norman, K.; Prado, C.M. The Underappreciated Role of Low Muscle Mass in the Management of Malnutrition. J. Am. Med Dir. Assoc. 2019, 20, 22–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abizanda, P.; Sinclair, A.; Barcons, N.; Lizan, L.; Rodriguez-Manas, L. Costs of Malnutrition in Institutionalized and Community-Dwelling Older Adults: A Systematic Review. J. Am. Med. Dir. Assoc. 2016, 17, 17–23. [Google Scholar] [CrossRef]
- Martínez-Reig, M.; Aranda-Reneo, I.; Peña-Longobardo, L.M.; Oliva-Moreno, J.; Barcons-Vilardell, N.; Hoogendijk, E.O.; Abizanda, P. Use of health resources and healthcare costs associated with nutritional risk: The FRADEA study. Clin. Nutr. 2018, 37, 1299–1305. [Google Scholar] [CrossRef]
- Volkert, D.; Beck, A.M.; Cederholm, T.; Cruz-Jentoft, A.; Goisser, S.; Hooper, L.; Kiesswetter, E.; Maggio, M.; Raynaud-Simon, A.; Sieber, C.C.; et al. ESPEN guideline on clinical nutrition and hydration in geriatrics. Clin. Nutr. 2019, 38, 10–47. [Google Scholar] [CrossRef]
- Volkert, D.; Berner, Y.N.; Berry, E.; Cederholm, T.; Coti Bertrand, P.; Milne, A.; Palmblad, J.; Schneider, S.; Sobotka, L.; Stanga, Z.; et al. ESPEN Guidelines on Enteral Nutrition: Geriatrics. Clin. Nutr. 2006, 25, 330–360. [Google Scholar] [CrossRef] [PubMed]
- Sobotka, L.; Schneider, S.; Berner, Y.; Cederholm, T.; Krznaric, Z.; Shenkin, A.; Stanga, Z.; Toigo, G.; Vandewoude, M.; Volkert, D.; et al. ESPEN Guidelines on Parenteral Nutrition: Geriatrics. Clin. Nutr. 2009, 28, 461–466. [Google Scholar] [CrossRef] [PubMed]
- Eglseer, D.; Halfens, R.J.; Lohrmann, C. Is the presence of a validated malnutrition screening tool associated with better nutritional care in hospitalized patients? Nutrition. 2017, 37, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, M.J.; Bauer, J.M.; Uter, W.; Donini, L.M.; Stange, I.; Volkert, D.; Diekmann, R.; Drey, M.; Bollwein, J.; Tempera, S.; et al. Prospective Validation of the Modified Mini Nutritional Assessment Short-Forms in the Community, Nursing Home, and Rehabilitation Setting. J. Am. Geriatr. Soc. 2011, 59, 2124–2128. [Google Scholar] [CrossRef] [PubMed]
- Power, L.; de van der Schueren, M.A.E.; Leij-Halfwerk, S.; Bauer, J.; Clarke, M.; Visser, M.; Volkert, D.; Bardon, L.; Gibney, E.; Corish, C.A. Development and application of a scoring system to rate malnutrition screening tools used in older adults in community and healthcare settings—A MaNuEL study. Clin. Nutr. 2018. [Google Scholar] [CrossRef] [PubMed]
- Council of Europe, Committee of ministers. Resolution ResAP(2003)3 on Food and Nutritional Care in Hospitals. Available online: https://www.nutritionday.org/cms/upload/pdf/11.resolution/Resolution_of_the_Council_of_Europe.pdf (accessed on 1 July 2019).
- Keller, H.; Carrier, N.; Duizer, L.; Lengyel, C.; Slaughter, S.; Steele, C. Making the Most of Mealtimes (M3): Grounding mealtime interventions with a conceptual model. J. Am. Med Dir. Assoc. 2014, 15, 158–161. [Google Scholar] [CrossRef] [PubMed]
- Roberts, H.C.; Lim, S.E.R.; Cox, N.J.; Ibrahim, K. The challenge of managing undernutrition in older people with Frailty. Nutrition 2019, 11, 808. [Google Scholar] [CrossRef] [PubMed]
- Marx, W.; Kelly, J.T.; Crichton, M.; Craven, D.; Collins, J.; Mackay, H.; Isenring, E.; Marshall, S. Is telehealth effective in managing malnutrition in community—dwelling older adults? A systematic review and meta–analysis. Maturitas 2018, 111, 31–46. [Google Scholar] [CrossRef]
- Marshall, S.; Agarwal, E.; Young, A.; Isenring, E. Role of domiciliary and family carers in individualised nutrition support for older adults living in the community. Maturitas 2017, 98, 20–29. [Google Scholar] [CrossRef] [Green Version]
- Cederholm, T.; Barazzoni, R.; Austin, P.; Ballmer, P.; Biolo, G.; Bischoff, S.C.; Compher, C.; Correia, I.; Higashiguchi, T.; Holst, M.; et al. ESPEN guidelines on definitions and terminology of clinical nutrition. Clin. Nutr. 2017, 36, 49–64. [Google Scholar] [CrossRef]
- Wirth, R.; Dziewas, R.; Beck, A.M.; Clave, P.; Hamdy, S.; Heppner, H.J.; Langmore, S.; Leischker, A.H.; Martino, R.; Pluschinski, P.; et al. Oropharyngeal dysphagia in older persons— from pathophysiology to adequate intervention: A review and summary of an international expert meeting. Clin. Interv. Aging. 2016, 11, 189–208. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.M.; Kjaersgaard, A.; Hansen, T.; Poulsen, I. Systematic review and evidence based recommendations on texture modified foods and thickened liquids for adults (above 17 years) with oropharyngeal dysphagia–An updated clinical guideline. Clin. Nutr. 2018, 37, 1980–1991. [Google Scholar] [CrossRef] [PubMed]
- Friedli, N.; Stanga, Z.; Sobotka, L.; Culkin, A.; Kondrup, J.; Laviano, A.; Mueller, B.; Schuetz, P. Revisiting the refeeding syndrome: Results of a systematic review. Nutrition 2017, 35, 151–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedli, N.; Stanga, Z.; Culkin, A.; Crook, M.; Laviano, A.; Sobotka, L.; Kressig, R.W.; Kondrup, J.; Mueller, B.; Schuetz, P. Management and prevention of refeeding syndrome in medical inpatients: An evidence-based and consensus—supported algorithm. Nutrition 2018, 47, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Janssen, G.; Pourhassan, M.; Lenzen-Großimlinghaus, R.; Jäger, M.; Schäfer, R.; Spamer, C.; Cuvelier, I.; Volkert, D.; Wirth, R.; on Behalf of the Working Group on Nutrition and Metabolism of the German Geriatric Society (DGG). The Refeeding Syndrome Revisited: You can only Diagnose What You Know. Available online: https://www.nature.com/articles/s41430-019-0441-x (accessed on 29 June 2019).
- Aubry, E.; Friedli, N.; Schuetz, P.; Stanga, Z. Refeeding syndrome in the frail elderly population: Prevention, diagnosis and management. Clin. Exp. Gastroenterol. 2018, 11, 255–264. [Google Scholar] [CrossRef] [PubMed]
- Pourhassan, M.; Cuvelier, I.; Gehrke, I.; Marburger, C.; Modreker, M.K.; Volkert, D.; Willschrei, H.P.; Wirth, R. Risk factors of refeeding syndrome in malnourished older hospitalized patients. Clin. Nutr. 2018, 37, 1354–1359. [Google Scholar] [CrossRef] [PubMed]
- Doig, G.S.; Simpson, F.; Heighes, P.T.; Bellomo, R.; Chesher, D.; Caterson, I.D.; Reade, M.C.; Harrigan, P.W.J. Restricted versus continued standard caloric intake during the management of refeeding syndrome in critically ill adults: A randomised, parallel-group, multicentre, single-blind controlled trial. Lancet Respir. Med. 2015, 3, 943–952. [Google Scholar] [CrossRef]
- Correa-Perez, A.; Abraha, I.; Cherubini, A.; Collinson, A.; Dardevet, D.; de Groot, L.; de van der Schueren, M.A.E.; Hebestreit, A.; Hickson, M.; Jaramillo-Hidalgo, J.; et al. Efficacy of non-pharmacological interventions to treat malnutrition in older persons: A systematic review and meta-analysis. The SENATOR project ONTOP series and MaNuEL knowledge hub project. Ageing Res. Rev. 2019, 49, 27–48. [Google Scholar] [CrossRef] [PubMed]
- Wright, J.; Baldwin, C. Oral nutritional support with or without exercise in the management of malnutrition in nutritionally vulnerable older people: A systematic review and meta-analysis. Clin. Nutr. 2018, 37, 1879–1891. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, N.M.; Belqaid, K.; Lugnet, K.; Nielsen, A.L.; Rasmussen, H.H.; Beck, A.M. Effectiveness of multidisciplinary nutritional support in older hospitalised patients: A systematic review and meta-analyses. Clin. Nutr. ESPEN 2018, 27, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Tsuboi, M.; Momosaki, R.; Vakili, M.; Abo, M. Nutritional supplementation for activities of daily living and functional ability of older people in residential facilities: A systematic review. Geriatr. Gerontol. Int. 2018, 18, 197–210. [Google Scholar] [CrossRef] [PubMed]
- Perna, S.; Rondanelli, M.; Spadaccini, D.; Lenzi, A.; Donini, L.M.; Poggiogalle, E. Are the therapeutic strategies in anorexia of ageing effective on nutritional status? A systematic review with meta-analysis. J. Hum. Nutr. Diet. 2019, 32, 128–138. [Google Scholar] [CrossRef] [PubMed]
- Reinders, I.; Volkert, D.; de Groot, L.C.P.G.M.; Beck, A.M.; Feldblum, I.; Jobse, I.; Neelemaat, F.; de van der Schueren, M.A.E.; Shahar, D.R.; Smeets, E.T.H.C.; et al. Effectiveness of nutritional interventions in older adults at risk of malnutrition across different health care settings: Pooled analyses of individual participant data from nine randomized controlled trials. Clin. Nutr. 2018. [Google Scholar] [CrossRef] [PubMed]
- van Zwienen-Pot, J.I.; Reinders, I.; de Groot, L.C.P.G.M.; Beck, A.M.; Feldblum, I.; Jobse, I.; Neelemaat, F.; de van der Schueren, M.A.E.; Shahar, D.R.; Smeets, E.T.H.C.; et al. The effect of nutritional intervention in older adults at risk of malnutrition on handgrip strength and mortality: Results from 9 pooled RCTs. Clin. Nutr. 2018, 37, S177. [Google Scholar]
- Schuetz, P.; Fehr, R.; Baechli, V.; Geiser, M.; Deiss, M.; Gomes, F.; Kutz, A.; Tribolet, P.; Bregenzer, T.; Braun, N.; et al. Individualised nutritional support in medical inpatients at nutritional risk: A randomised clinical trial. Lancet 2019, 393, 2312–2321. [Google Scholar] [CrossRef]
- Bischoff, S.C.; Singer, P.; Koller, M.; Barazzoni, R.; Cederholm, T.; Van Gossum, A. Standard operating procedures for ESPEN guidelines and consensus papers. Clin. Nutr. 2015, 34, 1043–1051. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hubbard, G.P.; Elia, M.; Holdoway, A.; Stratton, R.J. A systematic review of compliance to oral nutritional supplements. Clin. Nutr. 2012, 31, 293–312. [Google Scholar] [CrossRef] [PubMed]
- Baldwin, C.; Weekes, C.E. Dietary advice with or without oral nutritional supplements for disease-related malnutrition in adults. Cochrane Database Syst. Rev. 2011. [Google Scholar] [CrossRef] [PubMed]
- Abbott, R.A.; Whear, R.; Thompson-Coon, J.; Ukoumunne, O.C.; Rogers, M.; Bethel, A.; Hemsley, A.; Stein, K. Effectiveness of mealtime interventions on nutritional outcomes for the elderly living in residential care: A systematic review and meta-analysis. Ageing Res. Rev. 2013, 12, 967–981. [Google Scholar] [CrossRef]
- Collins, J.; Porter, J. The effect of interventions to prevent and treat malnutrition in patients admitted for rehabilitation: A systematic review with meta-analysis. J. Hum. Nutr. Diet. 2015, 28, 1–15. [Google Scholar] [CrossRef]
- Poscia, A.; Milovanovic, S.; La Milia, D.I.; Duplaga, M.; Grysztar, M.; Landi, F.; Moscato, U.; Magnavita, N.; Collamati, A.; Ricciardi, W. Effectiveness of nutritional interventions addressed to elderly persons: Umbrella systematic review with meta-analysis. Eur. J. Public Health 2018, 28, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Milne, A.C.; Potter, J.; Vivanti, A.; Avenell, A. Protein and energy supplementation in elderly people at risk from malnutrition. Cochrane Database Syst. Rev. 2009. [Google Scholar] [CrossRef] [PubMed]
- Baldwin, C.; Weekes, C.E. Dietary counselling with or without oral nutritional supplements in the management of malnourished patients: A systematic review and meta-analysis of randomised controlled trials. J. Hum. Nutr. Diet. 2012, 25, 411–426. [Google Scholar] [CrossRef] [PubMed]
- Correa-Pérez, A.; Lozano-Montoya, I.; Volkert, D.; Visser, M.; Cruz-Jentoft, A.J. Relevant outcomes for nutrition interventions to treat and prevent malnutrition in older people: A collaborative senator-ontop and manuel delphi study. Eur. Geriatr. Med. 2018, 9, 243–248. [Google Scholar] [CrossRef]
- Power, L.; Mullally, D.; Gibney, E.R.; Clarke, M.; Visser, M.; Volkert, D.; Bardon, L.; De Van Der Schueren, M.A.; Corish, C.A. A review of the validity of malnutrition screening tools used in older adults in community and healthcare settings–A MaNuEL study. Clin. Nutr. ESPEN 2018, 24, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.; Huen, S.C.; Luan, H.H.; Yu, S.; Zhang, C.; Gallezot, J.-D.; Booth, C.J.; Medzhitov, R. Opposing Effects of Fasting Metabolism on Tissue Tolerance in Bacterial and Viral Inflammation. Cell 2016, 166, 1512–1525.e12. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
Basic recommendations
|
Supportive interventions
|
Nutritional counselling
|
Food modification
|
| Oral nutritional supplements (ONS) (3 A, 3 GPP) |
| Enteral/parenteral nutrition (12 GPP) |
Prevalence, screening and diagnosis
|
Determinants and multifactorial etiology of malnutrition
|
Effectiveness and safety of interventions
|
Natural recovery
|
Role of protein and other specific nutrients
|
Dehydration
|
Knowledge transfer into clinical practice
|
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Volkert, D.; Beck, A.M.; Cederholm, T.; Cereda, E.; Cruz-Jentoft, A.; Goisser, S.; de Groot, L.; Großhauser, F.; Kiesswetter, E.; Norman, K.; et al. Management of Malnutrition in Older Patients—Current Approaches, Evidence and Open Questions. J. Clin. Med. 2019, 8, 974. https://doi.org/10.3390/jcm8070974
Volkert D, Beck AM, Cederholm T, Cereda E, Cruz-Jentoft A, Goisser S, de Groot L, Großhauser F, Kiesswetter E, Norman K, et al. Management of Malnutrition in Older Patients—Current Approaches, Evidence and Open Questions. Journal of Clinical Medicine. 2019; 8(7):974. https://doi.org/10.3390/jcm8070974
Chicago/Turabian StyleVolkert, Dorothee, Anne Marie Beck, Tommy Cederholm, Emanuele Cereda, Alfonso Cruz-Jentoft, Sabine Goisser, Lisette de Groot, Franz Großhauser, Eva Kiesswetter, Kristina Norman, and et al. 2019. "Management of Malnutrition in Older Patients—Current Approaches, Evidence and Open Questions" Journal of Clinical Medicine 8, no. 7: 974. https://doi.org/10.3390/jcm8070974