K Index is a Reliable Marker of Intrathecal Synthesis, and an Alternative to IgG Index in Multiple Sclerosis Diagnostic Work-Up

 , , , and
, , , and 
Abstract
:1. Introduction
2. Experimental Section
3. Results
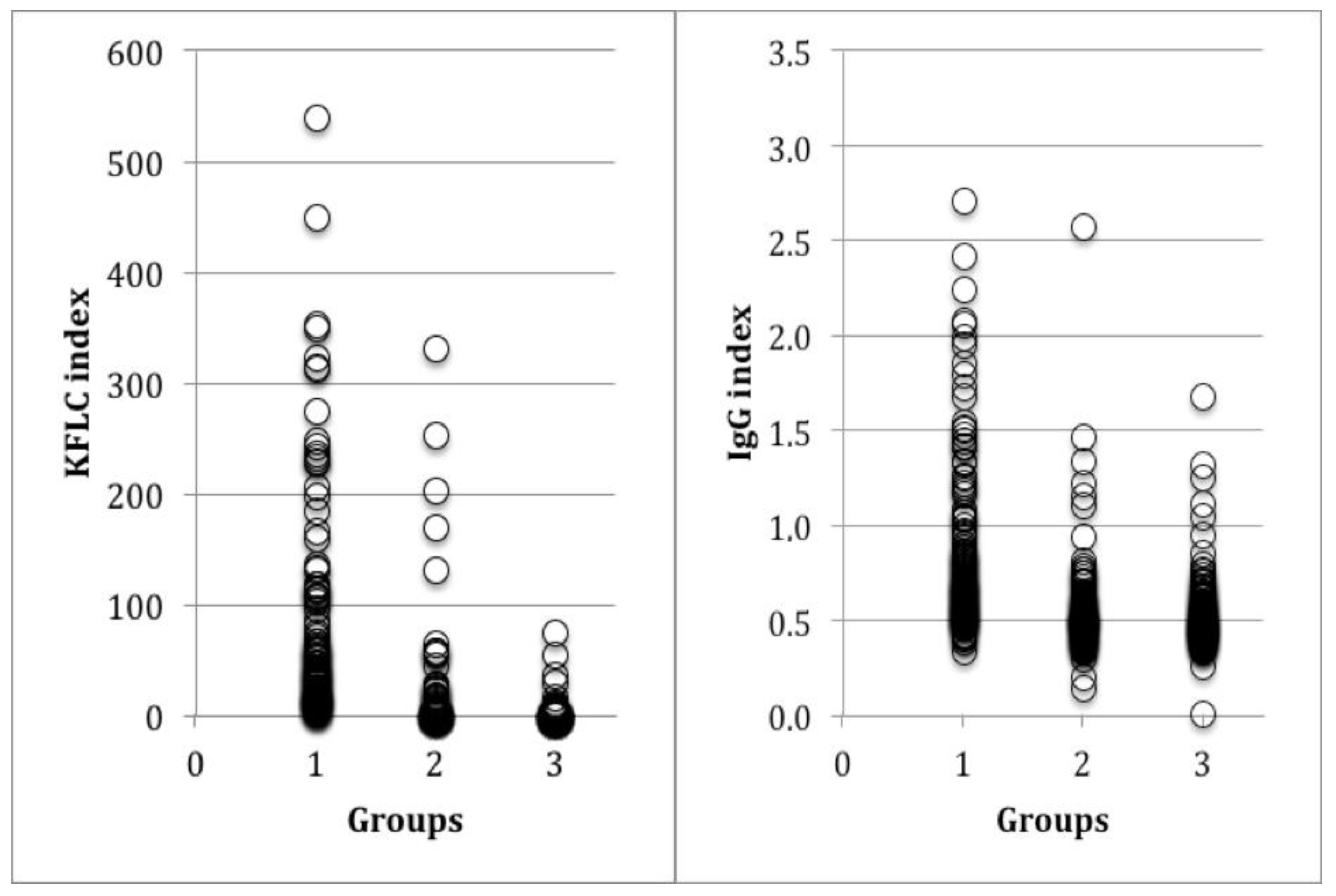
3.1. Markers of Intrathecal Synthesis in MS
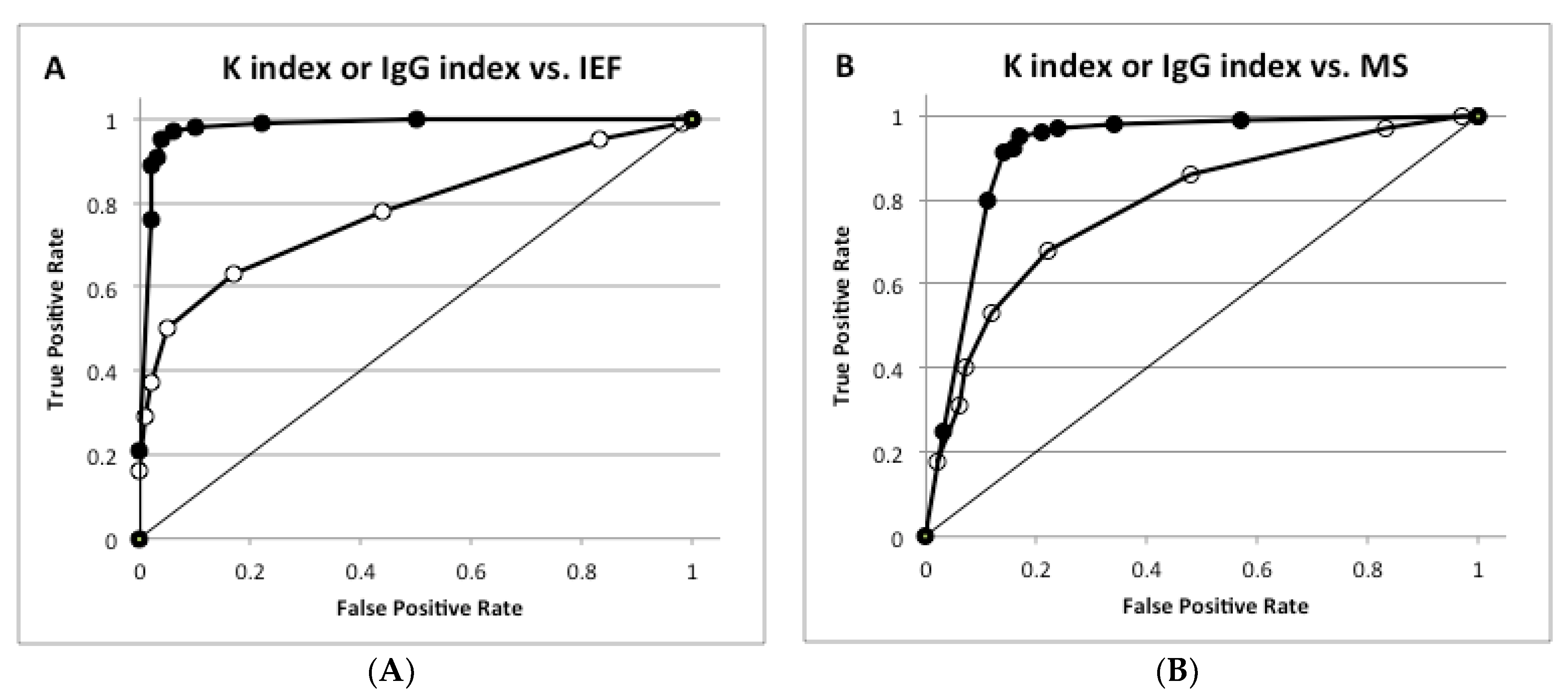
3.2. Comparisons and Diagnostic Performances of K and IgG Indexes
3.3. Confounding Effects of Blood–Brain Barrier Permeability
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- Polman, C.H.; Reingold, S.C.; Banwell, B. Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald Criteria. Ann. Neurol. 2011, 69, 292–302. [Google Scholar] [CrossRef] [PubMed]
- Poser, C.M.; Paty, D.W.; Scheinberg, L. New diagnostic criteria for multiple sclerosis: Guidelines for research protocols. Ann. Neurol. 1983, 13, 227–231. [Google Scholar] [CrossRef] [PubMed]
- Thompson, A.; Banwell, B.; Barkoff, F. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald Criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef]
- Link, H. The value of cerebrospinal fluid immunoglobulin analysis in clinical neurology. Riv. Patol. Nerv. Ment. 1976, 97, 323–340. [Google Scholar] [PubMed]
- Bayart, J.L.; Muls, N.; van Pesch, V. Free kappa light chains in neuroinflammatory disorders: Complement rather than substitute? Acta Neurol. Scand. 2018, 138, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Ramsden, D.B. Multiple sclerosis: Assay of free immunoglobulin light chains. Ann. Clin. Biochem. 2017, 54, 5–13. [Google Scholar] [CrossRef]
- Zeman, D.; Kušnierová, P.; Švagera, Z.; Všianský, F.; Byrtusová, M.; Hradílek, P.; Kurková, B.; Zapletalová, O.; Bartoš, V. Assessment of intrathecal free light chain synthesis: Comparison of different quantitative methods with the detection of oligoclonal free light chains by isoelectric focusing and affinity-mediated immunoblotting. PLoS ONE 2016, 15, 11. [Google Scholar] [CrossRef] [PubMed]
- Crespi, I.; Sulas, M.G.; Mora, R.; Naldi, P.; Vecchio, D.; Comi, C.; Cantello, R.; Bellomo, G. Combined use of kappa free light chain index and isoelectrofocusing of cerebro-spinal fluid in diagnosing multiple sclerosis: Performances and costs. Clin. Lab. 2017, 63, 551–559. [Google Scholar] [CrossRef]
- Caldarelli, G.; Troiano, G.; Rosadini, D.; Nante, N. Adoption of TSH Reflex algorithm in an Italian clinical laboratory. Ann. Igy. 2017, 29, 317–322. [Google Scholar]
- Gurtner, K.M.; Shosha, E.; Bryant, S.C.; Andreguetto, D.; Murray, D.L.; Pittock, S.J.; Willrich, M.A.V. CSF free light chain identification of demyelinating disease: Comparison with oligoclonal bands and other CSF indexes. Clin. Chem. Lab. Med. 2018, 56, 1071–1080. [Google Scholar] [CrossRef]
- Schwenkenbecher, P.; Konen, F.F.; Wurster, U.; Jendretzky, K.F.; Gingele, S.; Sühs, K.W.; Pul, R.; Witte, T.; Stangel, M.; Skripuletz, T. The persisting significance of oligoclonal bands in the dawning era of kappa free light chains for the diagnosis of multiple sclerosis. Int. J. Mol. Sci. 2018, 19. [Google Scholar] [CrossRef]
- Deisenhammer, F.; Bartos, A.; Egg, R.; Gilhus, N.E.; Giovannoni, G.; Rauer, S.; Sellebjerg, F. Guidelines on routine cerebrospinal fluid analysis. Report from an EFNS task force. Eur. J. Neurol. 2006, 13, 913–922. [Google Scholar] [CrossRef]
- Presslauer, S.; Milosavljevic, D.; Huebl, W.; Aboulenein-Djamshidian, F.; Krugluger, W.; Deisenhammer, F.; Senel, M.; Tumani, H.; Hegen, H. Validation of kappa free light chains as a diagnostic biomarker in multiple sclerosis and clinically isolated syndrome. A multicenter study. Mult. Scler. 2016, 22, 502–510. [Google Scholar] [CrossRef]
- Available online: https://www.sipmel.it/it/risorse/strumenti (accessed on 29 March 2019).
- Available online: http://vassarstats.net/ (accessed on 29 March 2019).
- Gastaldi, M.; Zardini, E.; Leante, R.; Ruggieri, M.; Costa, G.; Cocco, E.; De Luca, G.; Cataldo, I.; Biagioli, T.; Ballerini, C.; et al. Cerebrospinal fluid analysis and the determination of oligoclonal bands. Neurol. Sci. 2017, 38, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Emersic, A.; Anadolli, V.; Krsnik, M.; Rot, U. Intrathecal immunoglocbulin synthesis: The potential value of an adjunct test. Clin. Chim. Acta 2019, 489, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Vecchio, D.; Crespi, I.; Virgilio, E.; Naldi, P.; Campisi, M.P.; Serino, R.; Dianzani, U.; Bellomo, G.; Cantello, R.; Comi, C. Kappa free light chains could predict early disease course in multiple sclerosis. Mult. Scler. Relat. Disord. 2019, 30, 81–84. [Google Scholar] [CrossRef]
- Solaro, C.; Ponzio, M.; Moran, E.; Tanganelli, P.; Pizio, R.; Ribizzi, G.; Venturi, S.; Mancardi, G.L.; Battaglia, M.A. The changing face of multiple sclerosis: Prevalence and incidence in an aging population. Mult. Scler. 2015, 10, 1244–1250. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Parameters | MS (n: 127) | Non-MS (n: 258) | ID (n: 117) | NID (n: 141) |
|---|---|---|---|---|
| IgG index > 0.7 (n, %) | 75/127 (59.1%) | 39/258 (15.1%) | 21/117 (17.9%) | 18/141 (12.8%) |
| K index > 5 (n, %) | 122/127 (96.1%) | 50/258 (19.4%) | 39/117 (33.3%) | 11/141 (7.8%) |
| OB (n, %) | 123/127 (96.8%) | 44/258 (17%) | 35/117 (29.9%) | 9/141 (6.4%) |
| OB Detection | ||||
|---|---|---|---|---|
| IgG Index | IgG loc | K Index | K loc | |
| Sensitivity (%) | 48.0 (41.2–54.9) | 47.6 (40.6–54.7) | 96.5 (93.0–98.3) | 95.8 (91.8–97.8) |
| Specificity (%) | 93.8 (90.3–96.1) | 95.5 (92.0–97.4) | 89.8 (85.7–92.9) | 93.3 (89.4–95.8) |
| Likelihood ratio for a positive test | 7.8 (4.8–12.6) | 10.5 (5.8–19.0) | 9.48 (6.7–13.5) | 14.2 (8.8–22.9) |
| Likelihood ratio for a negative test | 0.6 (0.5–0.6) | 0.6 (0.5–0.6) | 0.04 (0.02–0.08) | 0.04 (0.02–0.09) |
| Positive predictive value (%) | 85.1 (77.4–90.5) | 89.1 (81.5–93.8) | 87.4 (82.5–91.2) | 91.9 (87.2–94.9) |
| Negative predictive value (%) | 71.1 (66.2–75.5) | 70.0 (64.8–74.7) | 97.2 (94.4–98.7) | 96.5 (93.3–98.2) |
| Efficiency (%) | 74.4 (70.3–78.1) | 74.5 (70.2–78.4) | 92.7 (89.9–94.7) | 94.4 (91.8–96.2) |
| Pre-test probability (prevalence) (%) | 42.3 (37.9–46.8) | 43.8 (39.2–48.6) | 42.3 (37.9–48.8) | 44.3 (39.6–49.0) |
| Pre-test odds | 0.7 (0.6–0.9) | 0.8 (0.7–0.9) | 0.7 (0.6–0.9) | 0.8 (0.7–0.96) |
| Post-test odds | 5.7 (2.9–11.1) | 8.2 (3.7–17.9) | 6.9 (4.1–11.9) | 11.3 (5.8–22.0) |
| Post-test probability (%) | 85.1 (74.6–91.7) | 89.1 (78.8–94.7) | 87.4 (80.3–92.2) | 91.9 (85.3–95.7) |
| Number needed to diagnose (NND) | 2.4 (3.2–2.0) | 2.3 (3.2–1.9) | 1.2 (1.3–1.1) | 1.1 (1.2–1.1) |
| MS Diagnosis | ||||
|---|---|---|---|---|
| IgG Index | IgG loc | K Index | KFLC loc | |
| Sensitivity (%) | 49.6 (42.5–56.7) | 51.3 (42.4–60.1) | 96.1 (90.8–98.5) | 95.8 (90.5–98.2) |
| Specificity (%) | 88.5 (84.2–92.7) | 90.7 (86.6–93.7) | 77.9 (72.0–83.7) | 80.7 (75.5–85.0) |
| Likelihood ratio for a positive test | 4.3 (3.1–7.0) | 5.5 (3.6–8.4) | 4.4 (3.1–5.9) | 5.0 (3.9–6.4) |
| Likelihood ratio for a negative test | 0.6 (0.5–0.7) | 0.5 (0.4–0.7) | 0.05 (0.02–0.11) | 0.05 (0.02–0.12) |
| Positive predictive value (%) | 67.7 (58.2–76.9) | 71.8 (61.4–80.2) | 68.2 (60.9–75.4) | 69.5 (62.1–76.0) |
| Negative predictive value (%) | 78.4 (73.3–82.9) | 80.2 (75.3–84.4) | 97.6 (94.5–98.8) | 97.6 (94.6–98.9) |
| Efficiency (%) | 75.8 (70.1–80.7) | 78.3 (73.9–82.2) | 83.9 (80.7–87.5) | 85.4 (81.5–88.6) |
| Pre-test probability (prevalence) (%) | 32.6 (28.0–37.2) | 31.5 (27.0–36.3) | 33.0 (28.5–38.3) | 31.5 (27.0–36.3) |
| Pre-test odds | 0.5 (0.4–0.6) | 0.5 (0.4–0.6) | 0.5 (0.4–0.6) | 0.5 (0.4–0.6) |
| Post-test odds | 2.1 (1.2–3.4) | 2.5 (1.4–4.8) | 2.1 (1.5–3.7) | 2.1 (1.5–3.6) |
| Post-test probability (%) | 67.7 (57.9–76.8) | 71.8 (57.4–82.8) | 68.2 (58.0–67.3) | 69.5 (58.8–78.5) |
| Number needed to diagnose (NND) | 2.6 (3.8–2.1) | 2.4 (3.5–1.9) | 1.5 (1.5–1.2) | 1.5 (1.5–1.2) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Crespi, I.; Vecchio, D.; Serino, R.; Saliva, E.; Virgilio, E.; Sulas, M.G.; Bellomo, G.; Dianzani, U.; Cantello, R.; Comi, C. K Index is a Reliable Marker of Intrathecal Synthesis, and an Alternative to IgG Index in Multiple Sclerosis Diagnostic Work-Up. J. Clin. Med. 2019, 8, 446. https://doi.org/10.3390/jcm8040446
Crespi I, Vecchio D, Serino R, Saliva E, Virgilio E, Sulas MG, Bellomo G, Dianzani U, Cantello R, Comi C. K Index is a Reliable Marker of Intrathecal Synthesis, and an Alternative to IgG Index in Multiple Sclerosis Diagnostic Work-Up. Journal of Clinical Medicine. 2019; 8(4):446. https://doi.org/10.3390/jcm8040446
Chicago/Turabian StyleCrespi, Ilaria, Domizia Vecchio, Roberto Serino, Elena Saliva, Eleonora Virgilio, Maria Giovanna Sulas, Giorgio Bellomo, Umberto Dianzani, Roberto Cantello, and Cristoforo Comi. 2019. "K Index is a Reliable Marker of Intrathecal Synthesis, and an Alternative to IgG Index in Multiple Sclerosis Diagnostic Work-Up" Journal of Clinical Medicine 8, no. 4: 446. https://doi.org/10.3390/jcm8040446