
Safety of Biological Therapies in Elderly Inflammatory Bowel Diseases: A Systematic Review and Meta-Analysis

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
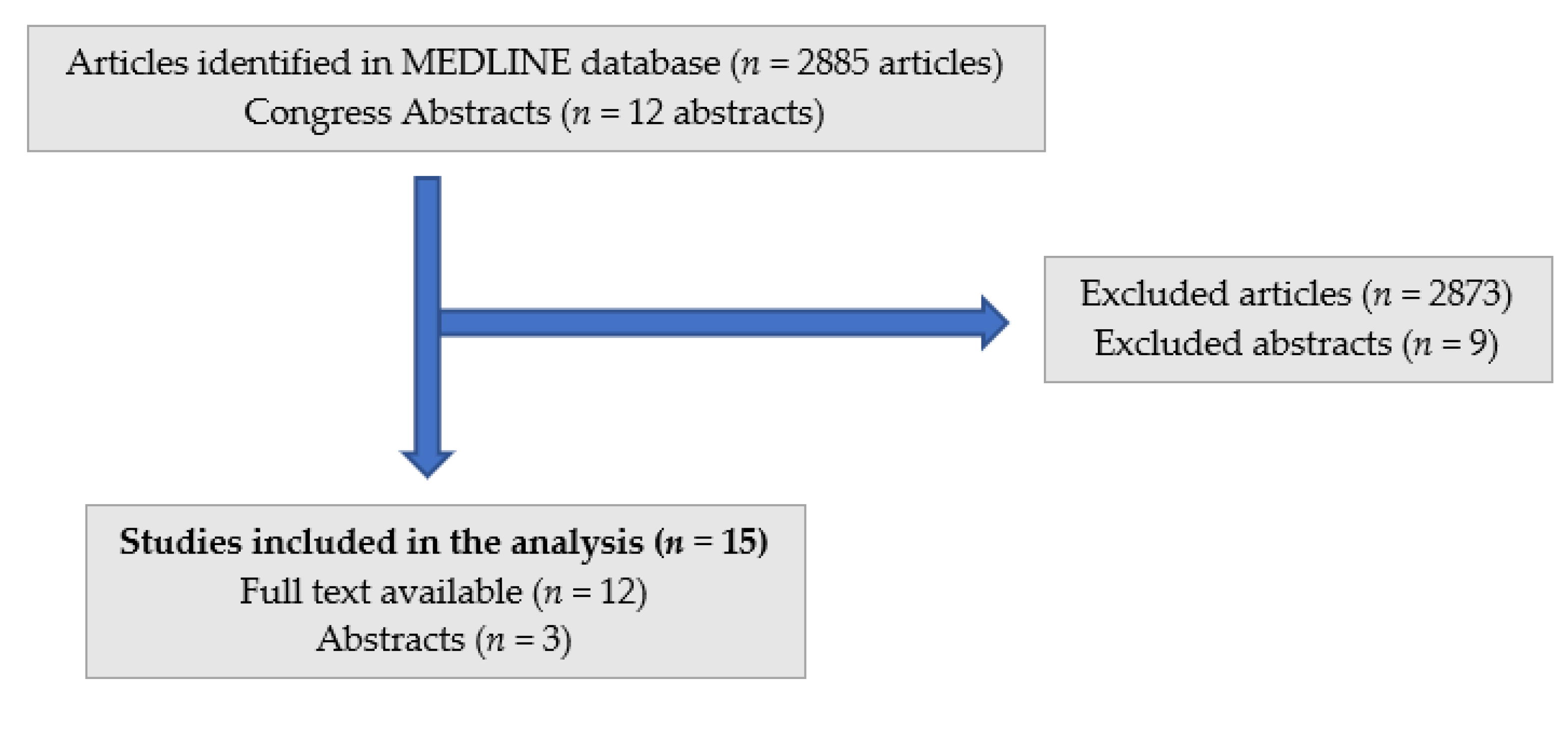
2.2. Study Selection
2.3. Data Extraction
2.4. Assessment of Study Quality
2.5. Statistical Analysis
3. Results
3.1. Study Characteristics
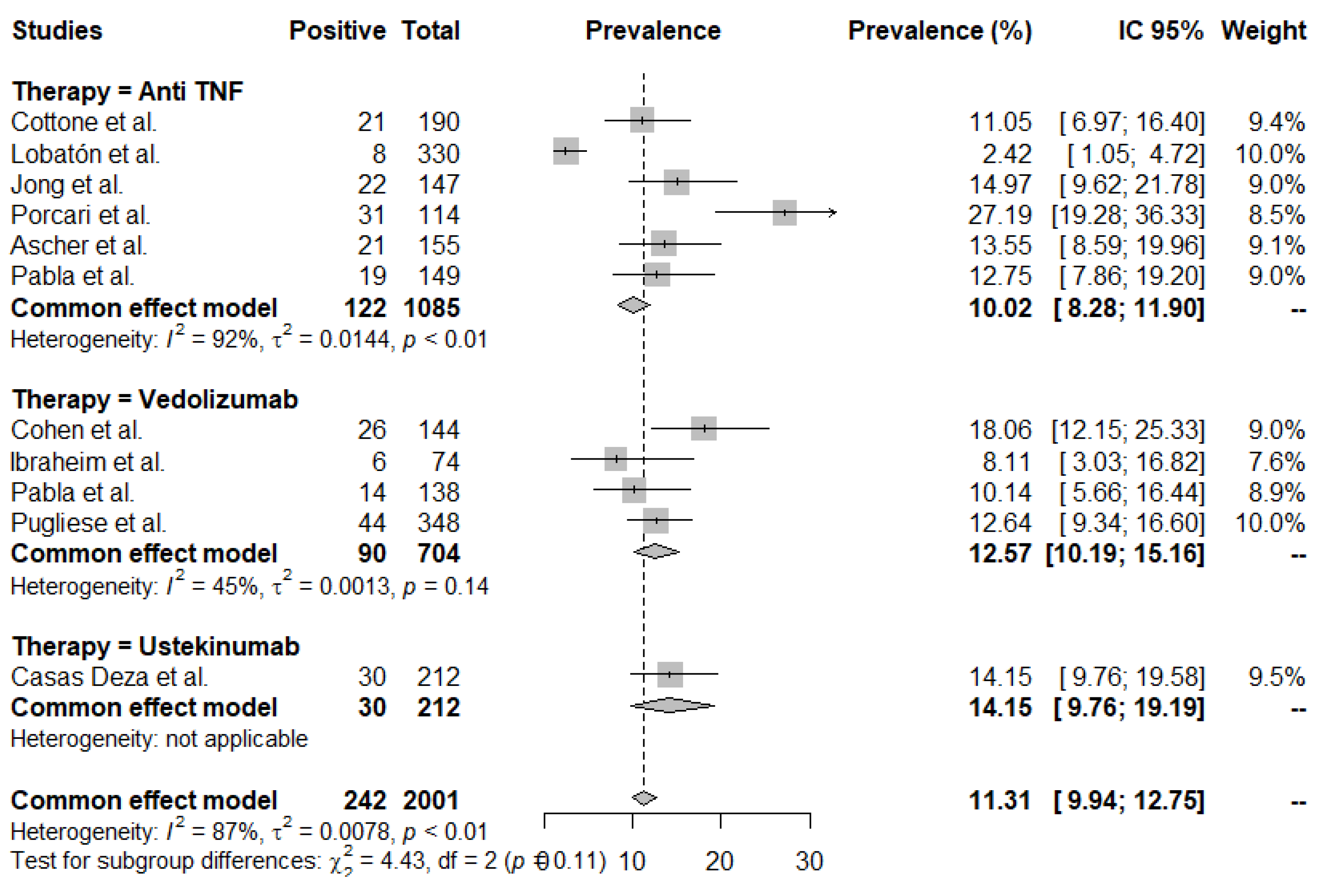
3.2. Adverse Event (AE) Rates
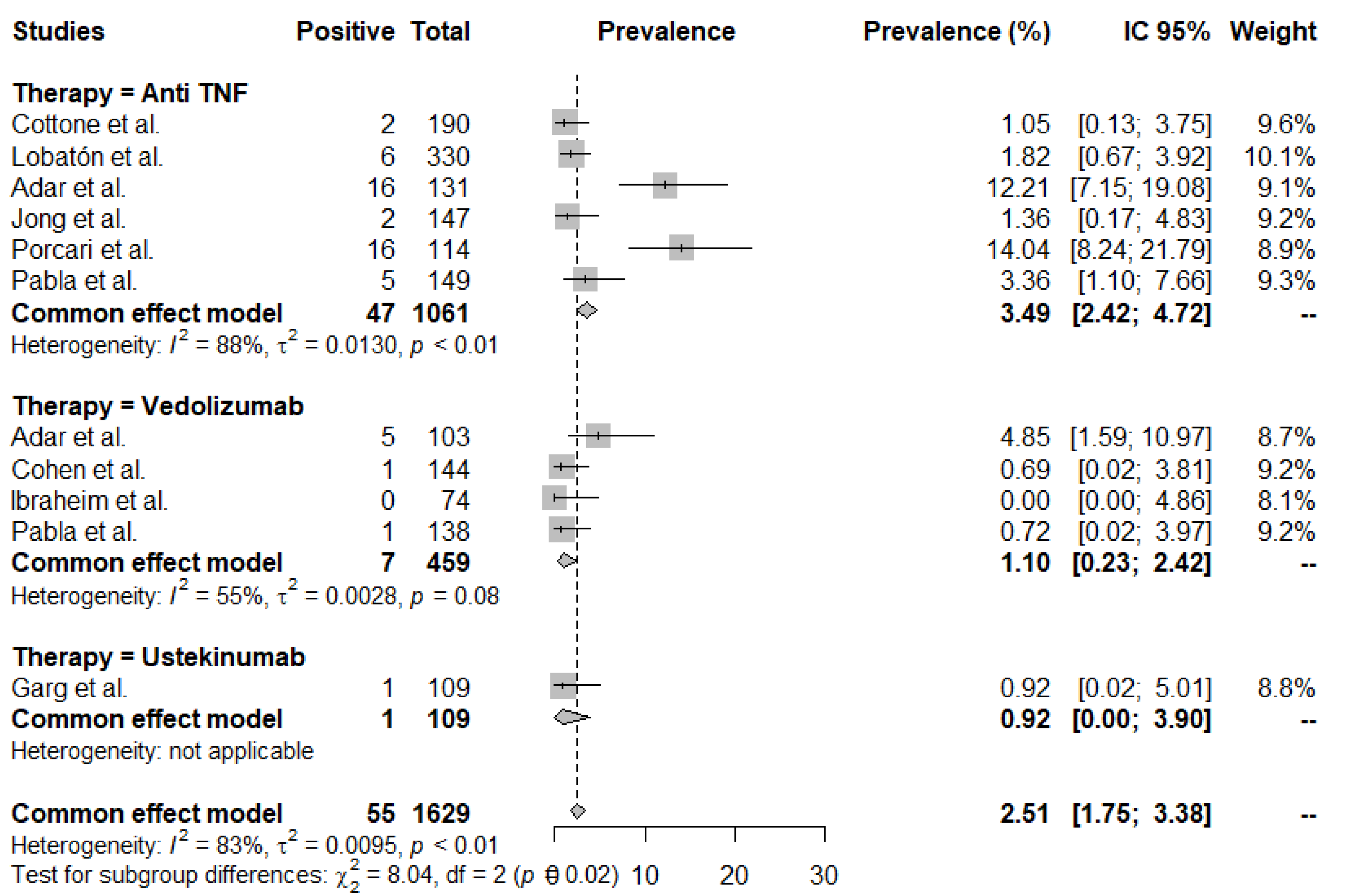
3.3. Infection Rates
3.4. Infusion/Injection Reactions
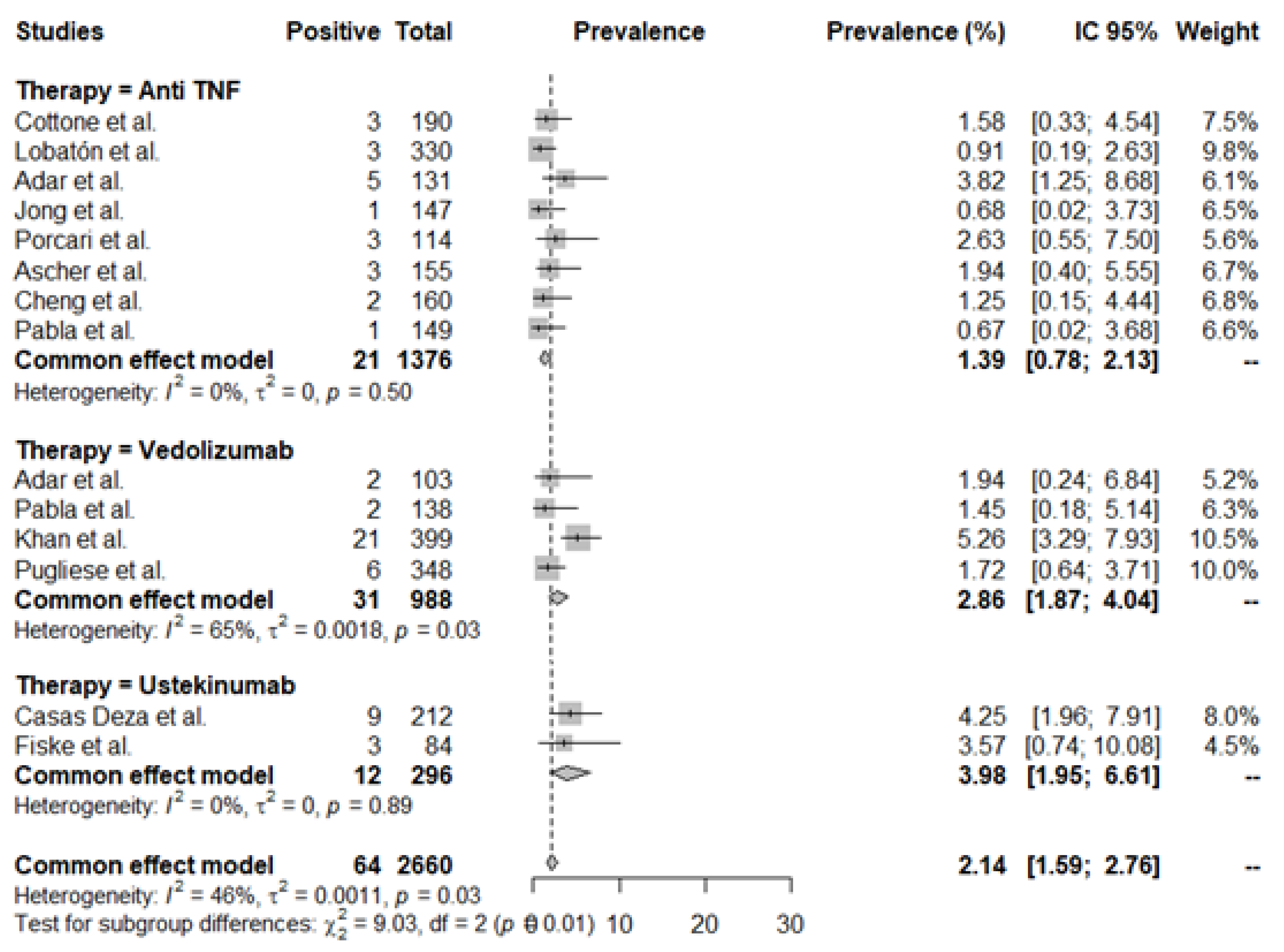
3.5. Malignancy Rates
3.6. Studies Directly Comparing Anti-TNF and VDZ Efficacy and Safety
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ng, S.C.; Shi, H.Y.; Hamidi, N.; Underwood, F.E.; Tang, W.; Benchimol, E.I.; Panaccione, R.; Ghosh, S.; Wu, J.C.Y.; Chan, F.K.L.; et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: A systematic review of population-based studies. Lancet 2017, 390, 2769–2778. [Google Scholar] [CrossRef]
- Charpentier, C.; Salleron, J.; Savoye, G.; Fumery, M.; Merle, V.; Laberenne, J.E.; Vasseur, F.; Dupas, J.-L.; Cortot, A.; Dauchet, L.; et al. Natural history of elderly-onset inflammatory bowel disease: A population-based cohort study. Gut 2014, 63, 423–432. [Google Scholar] [CrossRef]
- Hruz, P.; Alain, G.K.; Schoepfer, M. Management of the Elderly Inflammatory Bowel Disease Patient. Digestion 2020, 101 (Suppl. S1), 105–119. [Google Scholar] [CrossRef] [PubMed]
- Tran, V.; Limketkai, B.N.; Sauk, J.S. IBD in the Elderly: Management Challenges and Therapeutic Considerations. Curr. Gastroenterol. Rep. 2019, 21, 60. [Google Scholar] [CrossRef] [PubMed]
- Busquets, N.; Carmona, L.; Surís, X. Systematic review: Safety and efficacy of anti-TNF in elderly patients. Reumatol. Clin. 2011, 7, 104–112. [Google Scholar] [CrossRef]
- Mangoni, A.A.; Jackson, S.H. Age-related changes in pharmacokinetics and pharmacodynamics: Basic principles and practical applications. Br. J. Clin. Pharmacol. 2004, 57, 6–14. [Google Scholar] [CrossRef]
- Juneja, M.; Baidoo, L.; Schwartz, M.B.; Barrie, A., 3rd; Regueiro, M.; Dunn, M.; Binion, D.G. Geriatric Inflammatory Bowel Disease: Phenotypic Presentation, Treatment Patterns, Nutritional Status, Outcomes, and Comorbidity. Dig. Dis. Sci. 2012, 57, 2408–2415. [Google Scholar] [CrossRef] [PubMed]
- Gisbert, J.P.; Chaparro, M. Systematic review with meta-analysis: Inflammatory bowel disease in the elderly. Aliment. Pharmacol. Ther. 2014, 39, 459–477. [Google Scholar] [CrossRef] [PubMed]
- Chevillotte-Maillard, H.; Ornetti, P.; Mistrih, R.; Sidot, C.; Dupuis, J.; Dellas, J.-A.; Tavernier, C.; Maillefert, J.F. Survival and safety of treatment with infliximab in the elderly population. Rheumatology 2005, 44, 695–696. [Google Scholar] [CrossRef] [PubMed]
- Schneeweiss, S.; Setoguchi, S.; Weinblatt, M.E.; Katz, J.N.; Avorn, J.; Sax, P.E.; Levin, R.; Solomon, D.H. Anti-tumor necrosis factor alpha therapy and the risk of serious bacterial infections in elderly patients with rheumatoid arthritis. Arthritis Rheum. 2007, 56, 1754–1764. [Google Scholar] [CrossRef]
- Genevay, S.; Finckh, A.; Ciurea, A.; Chamot, A.M.; Kyburz, D.; Gabay, C.; Physicians of the Swiss Clinical Quality Management Program for Rheumatoid Arthritis. Tolerance and effectiveness of anti-tumor necrosis factor alpha therapies in elderly patients with rheumatoid arthritis: A population-based cohort study. Arthritis Rheum. 2007, 57, 679–685. [Google Scholar] [CrossRef] [PubMed]
- Filippini, M.; Bazzani, C.; Favalli, E.G.; Marchesoni, A.; Atzeni, F.; Sarzi-Puttini, P.; Pallavicini, F.B.; Caporali, R.; Gorla, R. Efficacy and safety of anti-tumour necrosis factor in elderly patients with rheumatoid arthritis: An observational study. Clin. Rev. Allergy Immunol. 2010, 38, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses; Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2013; Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 27 June 2022).
- Cottone, M.; Kohn, A.; Daperno, M.; Armuzzi, A.; Guidi, L.; D’Inca, R.; Bossa, F.; Angelucci, E.; Biancone, L.; Gionchetti, P.; et al. Advanced age is an independent risk factor for severe infections and mortality in patients given anti-tumor necrosis factor therapy for inflammatory bowel disease. Clin. Gastroenterol. Hepatol. 2011, 9, 30–35. [Google Scholar] [CrossRef]
- Lobatón, T.; Ferrante, M.; Rutgeerts, P.; Ballet, V.; Van Assche, G.; Vermeire, S. Efficacy and safety of anti-TNF therapy in elderly patients with inflammatory bowel disease. Aliment. Pharmacol. Ther. 2015, 42, 441–451. [Google Scholar] [CrossRef]
- Adar, T.; Faleck, D.; Sasidharan, S.; Cushing, K.; Borren, N.Z.; Nalagatla, N.; Ungaro, R.; Sy, W.; Owen, S.C.; Patel, A.; et al. Comparative safety and effectiveness of tumor necrosis factor α antagonists and vedolizumab in elderly IBD patients: A multicentre study. Aliment. Pharmacol. Ther. 2019, 49, 873–879. [Google Scholar] [CrossRef]
- de Jong, M.E.; Smits, L.J.T.; van Ruijven, B.; den Broeder, N.; Russel, M.G.V.M.; Römkens, T.E.H.; West, R.L.; Jansen, J.M.; Hoentjen, F.; on behalf of IBDREAM. Increased Discontinuation Rates of Anti-TNF Therapy in Elderly Inflammatory Bowel Disease Patients. J. Crohn’s Colitis 2020, 14, 888–895. [Google Scholar] [CrossRef]
- Porcari, S.; Viola, A.; Orlando, A.; Privitera, A.C.; Ferracane, C.; Cappello, M.; Vitello, A.; Siringo, S.; Inserra, G.; Fries, W.; et al. Persistence on Anti-Tumour Necrosis Factor Therapy in Older Patients with Inflammatory Bowel Disease Compared with Younger Patients: Data from the Sicilian Network for Inflammatory Bowel Diseases (SN-IBD). Drugs Aging 2020, 37, 383–392. [Google Scholar] [CrossRef]
- Asscher, V.E.; van der Vliet, Q.; van der Aalst, K.; van der Aalst, A.; Brand, E.C.; van der Meulen-de Jong, A.; Oldenburg, B.; Pierik, M.J.; van Tuyl, B.; Fidder, H.H.; et al. Anti-tumor necrosis factor therapy in patients with inflammatory bowel disease; comorbidity, not patient age, is a predictor of severe adverse events. Int. J. Colorectal. Dis. 2020, 35, 2331–2338. [Google Scholar] [CrossRef]
- Cheng, D.; Cushing, K.C.; Cai, T.; Ananthakrishnan, A.N. Safety and Efficacy of Tumor Necrosis Factor Antagonists in Older Patients With Ulcerative Colitis: Patient-Level Pooled Analysis of Data From Randomized Trials. Clin. Gastroenterol. Hepatol. 2021, 19, 939–946.e4. [Google Scholar] [CrossRef]
- Pabla, B.S.; Wiles, C.A.; Slaughter, J.C.; Scoville, E.A.; Dalal, R.L.; Beaulieu, D.B.; Schwartz, D.A.; Horst, S.N. Safety and Efficacy of Vedolizumab versus Tumor Necrosis Factor α Antagonists in an Elderly IBD Population: A Single Institution Retrospective Experience. Dig. Dis. Sci. 2021, 67, 3129–3137. [Google Scholar] [CrossRef]
- Cohen, N.A.; Plevris, N.; Kopylov, U.; Grinman, A.; Ungar, B.; Yanai, H.; Leibovitzh, H.; Isakov, N.F.; Hirsch, A.; Ritter, E.; et al. Vedolizumab is effective and safe in elderly inflammatory bowel disease patients: A binational, multicenter, retrospective cohort study. United Eur. Gastroenterol. J. 2020, 8, 1076–1085. [Google Scholar] [CrossRef]
- Ibraheim, H.; Samaan, M.A.; Srinivasan, A.; Brain, O.; Digby-Bell, J.; Irving, P.M.; Norman, I.; Jawad, I.; Biedermann, J.; Ibarra, A.; et al. Effectiveness and safety of vedolizumab in inflammatory bowel disease patients aged 60 and over: An observational multicenter UK experience. Ann. Gastroenterol. 2020, 33, 170–177. [Google Scholar] [CrossRef] [PubMed]
- Khan, N.; Pernes, T.; Weiss, A.; Trivedi, C.; Patel, M.; Xie, D.; Yang, Y.X. Incidence of Infections and Malignancy among Elderly Male Patients with IBD Exposed to Vedolizumab, Prednisone, and 5-ASA Medications: A Nationwide Retrospective Cohort Study. Adv. Ther. 2021, 38, 2586–2598. [Google Scholar] [CrossRef] [PubMed]
- Pugliese, D.; Privitera, G.; Armuzzi, A. P477 Italian real-life study evaluating the long-term effectiveness of vedolizumab for the treatment of inflammatory bowel disease: The elderly cohort. J. Crohn’s Colitis 2020, 14 (Suppl. S1), S419–S422. [Google Scholar] [CrossRef]
- Garg, R.; Aggarwal, M.; Butler, R.; Achkar, J.P.; Lashner, B.; Philpott, J.; Cohen, B.; Qazi, T.; Rieder, F.; Regueiro, M.; et al. Real-World Effectiveness and Safety of Ustekinumab in Elderly Crohn’s Disease Patients. Dig. Dis. Sci. 2022, 67, 3138–3147. [Google Scholar] [CrossRef] [PubMed]
- Deza, D.C.; Calvo, L.J.L.; Mainar, J.M.A.; Ricart, E.; Gisbert, J.P.; Tirado, M.R.; Rodríguez, E.S.; Sicilia, B.; Casbas, A.G.; Ochoa, O.M.; et al. P262 Effectiveness and safety of ustekinumab in elderly patients: Real world evidence from ENEIDA registry. J. Crohn’s Colitis 2021, 15 (Suppl. S1), S298–S299. [Google Scholar] [CrossRef]
- Fiske, J.; Liu, E.; Limdi, J.; Conley, T.E.; Townsend, T.; Davies, M.; Brockwell, R.; Baig, D.; Abdelbadiee, S.; Uney, A.; et al. P482 Safety and efficacy of ustekinumab for Crohn’s disease in the elderly population. J. Crohn’s Colitis 2021, 15 (Suppl. S1), S471. [Google Scholar] [CrossRef]
- Peyrin-Biroulet, L.; Deltenre, P.; de Suray, N.; Branche, J.; Sandborn, W.J.; Colombel, J.F. Efficacy and safety of tumor necrosis factor antagonists in Crohn’s disease: Meta-analysis of placebo-controlled trials. Clin. Gastroenterol. Hepatol. 2008, 6, 644–653. [Google Scholar] [CrossRef]
- Wheat, C.L.; Ko, C.W.; Clark-Snustad, K.; Grembowski, D.; Thornton, T.A.; Devine, B. Inflammatory Bowel Disease (IBD) pharmacotherapy and the risk of serious infection: A systematic review and network meta-analysis. BMC Gastroenterol. 2017, 17, 52. [Google Scholar] [CrossRef]
- Lichtenstein, G.R.; Feagan, B.G.; Cohen, R.D.; Salzberg, B.A.; Diamond, R.H.; Price, S.; Langholff, W.; Londhe, A.; Sandborn, W.J. Serious infection and mortality in patients with Crohn’s disease: More than 5 years of follow-up in the TREAT™ registry. Am. J. Gastroenterol. 2012, 107, 1409–1422. [Google Scholar] [CrossRef] [PubMed]
- Calafat, M.; Mañosa, M.; Ricart, E.; Nos, P.; Iglesias-Flores, E.; Vera, I.; López-Sanromán, A.; Guardiola, J.; Taxonera, C.; Mínguez, M.; et al. Risk of immunomediated adverse events and loss of response to infliximab in elderly patients with inflammatory bowel disease. A cohort study of the ENEIDA registry. J. Crohn’s Colitis 2021, 16, 946–953. [Google Scholar] [CrossRef]
- Piovani, D.; Danese, S.; Peyrin-Biroulet, L.; Nikolopoulos, G.K.; Bonovas, S. Systematic review with meta-analysis: Biologics and risk of infection or cancer in elderly patients with inflammatory bowel disease. Aliment. Pharmacol. Ther. 2020, 51, 820–830. [Google Scholar] [CrossRef] [PubMed]
- Sands, B.E.; Peyrin-Biroulet, L.; Loftus, E.V., Jr.; Danese, S.; Colombel, J.F.; Törüner, M.; Jonaitis, L.; Abhyankar, B.; Chen, J.; Rogers, R.; et al. Vedolizumab versus Adalimumab for Moderate-to-Severe Ulcerative Colitis. N. Engl. J. Med. 2019, 381, 1215–1226. [Google Scholar] [CrossRef] [PubMed]
- Irving, P.M.; Sands, B.E.; Hoops, T.; Izanec, J.L.; Gao, L.-L.; Gasink, C.; Greenspan, A.; Allez, M.; Danese, S.; Hanauer, S.B.; et al. Ustekinumab versus adalimumab for induction and maintenance therapy in biologic-naïve patients with moderately to severely active Crohn’s disease: A multicentre, randomised, double-blind, parallel-group, phase 3b trial. Lancet 2022, 399, 2200–2211. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Biologic | Year | Author | Age Cutoff | Study Design | Number of Elderly Patients | Median Disease Duration (Years) | Median Treatment Duration (Years) | Previous Biologic Exposure (%) |
|---|---|---|---|---|---|---|---|---|
| Anti-TNF | 2011 | Cottone et al. [15] | >65 y | Cohort—Prospective | 95 | NA | 1.4 | NA |
| 2015 | Lobatón et al. [16] | >65 y | Case Control—Retrospective | 66 | 6 | 1 | NA | |
| 2019 | Adar et al. [17] | >60 y | Case Control—Retrospective | 131 | 13 | 1 | 14 (Anti-TNF) 6 (VDZ) | |
| 2020 | Jong et al. [18] | >60 y | Cohort—Prospective | 81 | 7.5 | 1.7 | NA | |
| 2020 | Porcari et al. [19] | >60 y | Cohort—Retrospective | 114 | >5 | 1 | NA | |
| 2020 | Asscher et al. [20] | >60 y | Cohort—Retrospective | 90 | 16.7 | 1.7 | NA | |
| 2021 | Cheng et al. [21] | >60 y | Cohort—Retrospective | 160 | 5.5 | 1 | NA | |
| 2021 | Pabla et al. [22] | >60 y | Cohort—Retrospective | 104 | 10 | 1.43 | 17.3 (Anti-TNF) | |
| Vedolizumab | 2019 | Adar et al. [17] | >60 y | Case Control—Retrospective | 103 | 16 | 1 | 60 (Anti-TNF) |
| 2020 | Cohen et al. [23] | >60 y | Cohort—Retrospective | 144 | 10 | 1 | 46. | |
| 2020 | Ibraheim et al. [24] | >60 y | Cohort—Retrospective | 74 | 9 | 1 | 27 | |
| 2021 | Pabla et al. [22] | >60 y | Cohort—Retrospective | 108 | 15.5 | 1.27 | 73.2 (Anti-TNF) | |
| 2021 | Khan et al. [25] | >65 y | Cohort—Retrospective | 213 | NA | 1 | NA | |
| 2021 | Pugliese et al. [26] | >65 y | Cohort—Prospective | 174 | 10.9 | 2 | 55 | |
| Ustekinumab | 2021 | Garg et al. [27] | >65 y | Cohort—Retrospective | 39 | 20.6 | 1.3 | 95 |
| 2021 | Casas Deza et al. [28] | >60 y | Cohort—Prospective/ Retrospective | 212 | NA | 1 | 85 | |
| 2021 | Fiske et al. [29] | >60 y | Cohort—Retrospective | 70 | NA | 1 | 84.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hahn, G.D.; Golovics, P.A.; Wetwittayakhlang, P.; Santa Maria, D.M.; Britto, U.; Wild, G.E.; Afif, W.; Bitton, A.; Bessissow, T.; Lakatos, P.L. Safety of Biological Therapies in Elderly Inflammatory Bowel Diseases: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 4422. https://doi.org/10.3390/jcm11154422
Hahn GD, Golovics PA, Wetwittayakhlang P, Santa Maria DM, Britto U, Wild GE, Afif W, Bitton A, Bessissow T, Lakatos PL. Safety of Biological Therapies in Elderly Inflammatory Bowel Diseases: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2022; 11(15):4422. https://doi.org/10.3390/jcm11154422
Chicago/Turabian StyleHahn, Gustavo Drügg, Petra Anna Golovics, Panu Wetwittayakhlang, Dirlene Melo Santa Maria, Usiara Britto, Gary Edward Wild, Waqqas Afif, Alain Bitton, Talat Bessissow, and Peter Laszlo Lakatos. 2022. "Safety of Biological Therapies in Elderly Inflammatory Bowel Diseases: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 11, no. 15: 4422. https://doi.org/10.3390/jcm11154422